
Abstract
Objectives
The nosological status of burnout has been a topic of critical debate since its inception as a psychological phenomenon in the 1970s. It was sought here to narratively review current literature regarding burnout’s definition, differentiation from depression, and diagnostic status, including Parker’s contribution to this field.
Conclusion
Burnout was originally defined as being comprised of emotional exhaustion, empathy loss, and reduced professional accomplishment. More recent research suggests other symptoms, such as cognitive dysfunction and emotional withdrawal/distancing, may also be important components of the syndrome. There are mixed findings regarding the degree of overlap between burnout and depression. However, research by Parker and others provides preliminary evidence that the overlap is stronger when considering non-melancholic compared to melancholic depression. Finally, while its current diagnostic status is ambiguous, diagnostic criteria covering (paid or unpaid) work-based causes, multiple key symptoms, and consideration of other confounding conditions, have been proposed. Such criteria may allow for the clinical distress caused by burnout to be acknowledged, while reducing the chance of over-diagnosis.
Interest in burnout as an occupational phenomenon ignited in the 1970s, with early research focusing on emotional exhaustion and compassion fatigue experienced by those working in the service industry.1,2 Since then, researchers and clinicians have debated how best to define burnout, whether and how it can be differentiated from other mental health conditions, particularly depression, and its relevant diagnostic criteria should it be considered diagnosable. 3 As both an active clinician and researcher, it was this latter question that sparked Gordon Parker’s initial investigation into burnout. He observed that many of his patients referred for assessment and treatment of depression did not appear to fit the clinical picture, with burnout seeming the likely culprit for many such patients. From this initial interest, a broader research program was established, with Parker and the current author working to determine how to best define, differentiate and diagnose burnout. The aim of this paper was to review Parker’s research and proposed research translation amongst the broader context of the burnout literature, highlighting the current status of the debate regarding burnout as a distinct clinical condition.
Defining and measuring burnout
Early conceptualisations of burnout positioned it as an occupational phenomenon affecting those in the service professions, occurring as a result of the emotional toll of their jobs.1,2 Burnout was defined by seminal researchers Christina Maslach and colleagues as a syndrome comprising emotional exhaustion, empathy loss or ‘depersonalization’, and a reduced sense of professional accomplishment. 2 This definition, developed in the early 1970s, remains the most prominent definition of burnout today and underpins the most widely used measure of burnout, the Maslach Burnout Inventory (MBI).2,4
Despite such dominance, the MBI and its conceptualisation of burnout have been subject to ongoing discussion. Firstly, regarding its scope, the MBI was initially restricted for use in the service industry and then adapted for use in other professions, 4 with workplace factors such as workload, rewards, control/autonomy and fairness all proposed to impact workers’ susceptibility to burnout. 5 However, some have argued for expanding this context even further to acknowledge that those outside of the workforce, but with demanding home and caring responsibilities, may also be vulnerable to burnout.6,7 Furthermore, burnout was once thought to be a Western phenomenon; however, it is now becoming recognised as a more universal experience affecting diverse ethnic groups. 8
A second key issue concerns the symptoms included for assessment in developing the MBI burnout definition. The MBI was derived through factor analysing a relatively small set of 47 items compiled through earlier qualitative interviews and a review of the existing burnout literature.2,4 Questions have since arisen regarding whether the three-factor MBI burnout definition might have differed had a more exhaustive list of items been initially examined. 9 Of particular interest is whether symptoms of other psychological states, particularly depression, are relevant to a comprehensive definition of burnout. 9
Considering such questions, Parker and colleagues conducted several studies to evaluate the key symptoms of burnout as experienced by the lay population.7,10,11 137 total symptoms derived from an exhaustive review of the burnout literature and previous burnout measures were evaluated across the studies. Bifactor analyses – a strategy which loads all items onto a general factor while also specifying additional factors uncorrelated with the general factor – led to a new definition and associated measure of burnout (later labelled the Sydney Burnout Measure or SBM). 11 Bifactor modelling helped to reconcile competing unidimensional and multidimensional perspectives (e.g. the MBI definition) on burnout by including a general underlying burnout factor alongside multiple distinct but related symptom constructs, with the SBM bifactor burnout model incorporating exhaustion, cognitive dysfunction, depressed mood, empathy loss, reduced work performance, and insularity/social withdrawal. 11 Overall, the results suggested a new model that defined burnout as having more key symptom constructs than captured by the MBI triadic model.
The SBM corresponds with another contemporary burnout measure, the Burnout Assessment Tool (BAT). 3 The BAT conceptualises burnout as comprised of exhaustion, mental distance, emotional impairment, and cognitive dysfunction, as well as secondary symptoms of psychological complaints and psychosomatic complaints. The BAT was developed through a top-down approach, in which items were derived through interviews with general practitioners, psychologists and other mental health professionals. In contrast, the SBM was created using a bottom-up method, examining the experiences and symptoms of those who self-identified as suffering from burnout. The overlap in symptoms identified through both approaches supports the validity of such symptoms in being definitional to the burnout experience. Validation of the SBM in new samples has commenced, 12 and it is hoped the measure will become more widely used to measure burnout in the future.
Differentiating burnout
Questions regarding how to best define burnout are further complicated by the syndrome’s apparent overlap with several formally recognised somatic (e.g. chronic fatigue syndrome) and psychiatric conditions. As an example of the latter, burnout has been considered by some as an adjustment disorder that results from a work-related stressor. 13 However, while an adjustment disorder should emerge within one to three months after experiencing a stressor, and typically resolves within six months, burnout is generally accepted as developing slowly over time (i.e. several months to more than a year), 14 thus whether the conditions are redundant remains contentious.
Depression is believed to be the condition that shares the greatest overlap with burnout. Some have argued that burnout encompasses most symptoms of Major Depressive Disorder (MDD), and therefore, burnout should not be considered a distinct syndrome. 15 In contrast, meta-analyses have concluded that the correlation between burnout and depression reported across studies is not large enough to suggest syndrome equivalence. 16
Tavella and Parker sought to clarify such mixed findings by examining the burnout/depression overlap using both quantitative and qualitative data. First, in their study in which the SBM was developed, the 137 possible symptom list included 37 items that had been adapted from validated measures of depression, so to assess whether the symptoms represented by these items might be integral to burnout’s definition. 11 Seven of the 37 were found to contribute to the final bifactor solution, including ones capturing low mood, reduced self-worth, anhedonia, social withdrawal, low energy and compromised cognition. These items were interpreted as indicating depressed mood rather than clinical depression per se, as other key MDD symptoms (e.g. psychomotor disturbance, suicidal ideation) were not represented. Second, a qualitative study indicated that the lay population differentiated burnout from depression based on several phenomenological features. 17 Namely, the former was identified as usually having a more identifiable cause and being associated with (compared to depression) relatively preserved functioning, greater anger than sadness, feelings of helplessness rather than hopelessness, and heightened anxiety and emotionality. Taken together, these studies were interpreted as suggesting some key indicators of clinical depression are not core components of burnout.
Both Parker and Tavella 18 and Bianchi et al. 9 have argued that previous inconclusive findings regarding the degree of burnout’s overlap with depression may be partly due to such research ignoring the impact of depressive subtypes on results. Bianchi et al. identified that a large proportion of their participants who scored highly on both burnout and depression measures exhibited symptoms of atypical rather than melancholic depression. 19 Tavella et al. compared participants with self-diagnosed burnout and clinically diagnosed depression on the SBM and other measures, splitting the latter group into melancholic and non-melancholic depression subgroups for subsequent analyses. 20 Results indicated that comparatively few study variables distinguished the burnout group from the non-melancholic depression group. Substantially more differences were observed between the burnout group and the melancholic depression group, with the latter being more likely to report biological and/or relationship causal factors, depressed mood, trouble getting started with everyday tasks, passive suicidal ideation and oversleeping, and less likely to report middle insomnia, feeling angry, and work-related causal factors. Overall, the findings indicated that burnout corresponded to a greater degree with non-melancholic as opposed to melancholic depression. A theoretical differentiation template put forward by Parker and Tavella 18 highlights the identified points of convergence and divergence between burnout and each of the key depressive subtypes.
Diagnosing burnout
The nosological status of burnout remains enigmatic, not helped by the lack of consensus regarding how to best define, measure, and differentiate the condition. As such, burnout has never been listed in the Diagnostic and Statistical Manual of Mental Disorders (DSM). It has been listed in the two most recent revisions of the World Health Organization’s (WHO) International Classification of Diseases (i.e. the ICD-10 and ICD-11), with its three listed diagnostic criteria (i.e. exhaustion, mental distancing, and a sense of reduced accomplishment) aligning with the MBI’s triadic burnout definition. Importantly, burnout has been characterised in the ICD as a factor that may influence an individual’s health status but ‘is not in itself a current illness or injury’. This stance has been judged as ambivalent and confusing, 3 as WHO has both included burnout in its list of diseases while also explicitly stating it should not be considered as one.
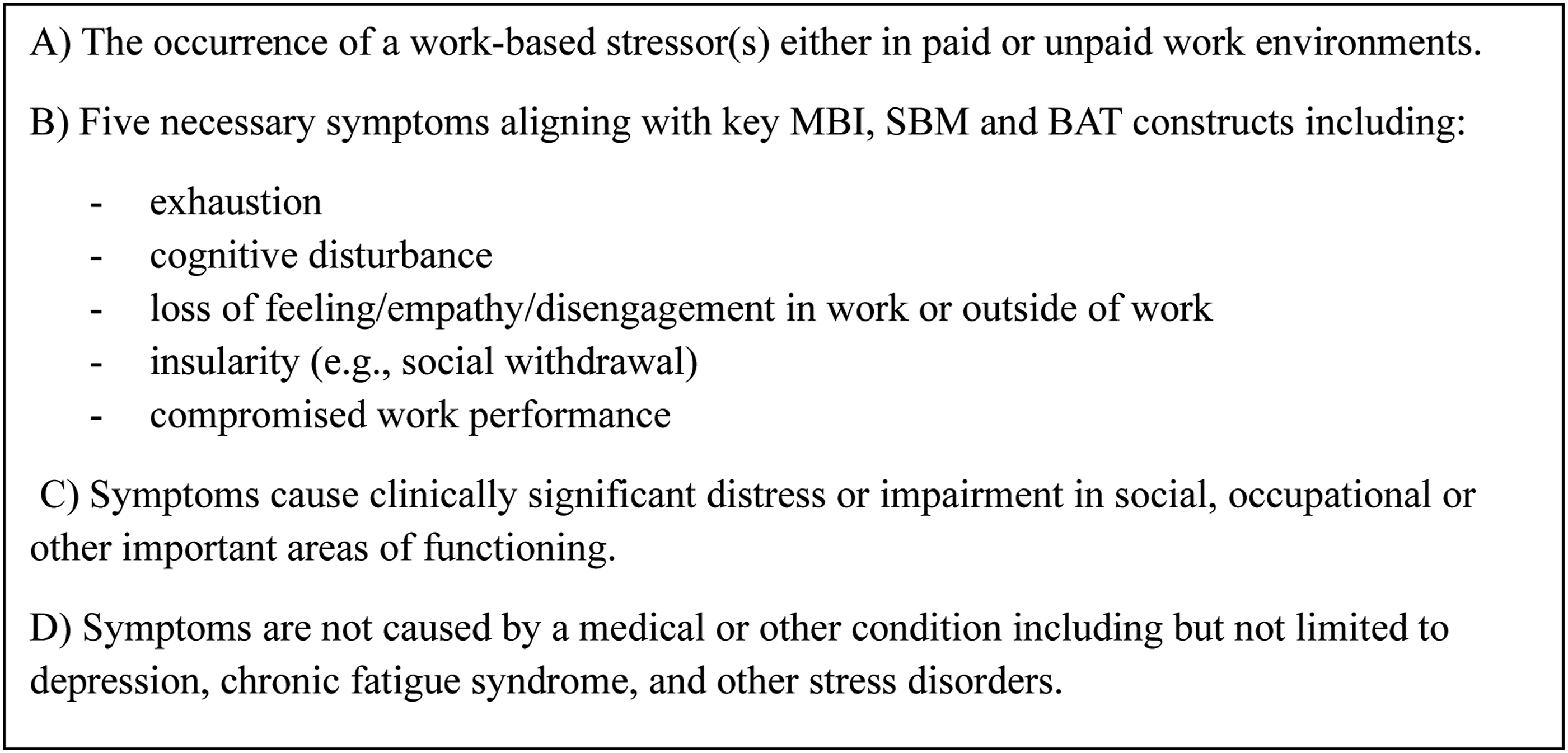
Parker holds the position that burnout could be considered a nosological entity if issues regarding its definition, measurement and differentiation could be resolved. Based on theirs and others’ research into burnout, Parker and Tavella put forward a set of diagnostic criteria that could be considered for burnout if it was to be included as a mental health condition in the DSM, as demonstrated in Figure 1.
21
Such criteria would arguably allow for recognition of illness for patients with burnout symptoms who are experiencing clinical distress, while helping to limit over-diagnosis of burnout in cases where there is some other underlying or primary cause (e.g. depression). Symptom criteria for burnout proposed by Parker and Tavella.
21
Limitations and implications
This narrative review was limited in its scope, primarily centred on the work of Parker, which may restrict the extent to which alternative perspectives and approaches within the field are fully represented. It is clear, however, that since the inception of the MBI, research by Parker, Schaufeli, 3 and many others suggests that burnout may incorporate several additional symptom constructs that are not included in the MBI-based ICD-11 burnout definition. Such research argues for re-evaluation of the diagnostic criteria in the ICD-11 and consideration for the appropriateness of inclusion of burnout in the DSM.
Clarification of burnout’s definition and whether and how it should be diagnosed is imperative before rigorous treatment efficacy studies can be undertaken. Conclusions that can be drawn from meta-analyses evaluating treatment efficacy studies for burnout have been limited due to lack of consistency in how burnout is defined and measured across studies. 22 The preliminary evidence of burnout’s overlap with non-melancholic (including atypical) depression allows an argument that treatment for non-melancholic (rather than melancholic) depression could be beneficial in treating burnout, namely, prioritising psychotherapy above antidepressant medication. 23 There are reports of burnout cases being treated with antidepressants, 24 despite there being no clinical trials published that have evaluated antidepressant efficacy for treating burnout, and some evidence that antidepressant use can lead to a worsening of burnout symptoms. 25 Further research is clearly needed to examine the degree of overlap between burnout and non-melancholic versus melancholic depression, as well as to determine whether workplace interventions and/or individualised depression (e.g. pharmacotherapy versus psychotherapy) or other treatments are most effective in treating burnout. Neurobiological measures (e.g. cerebral MRI) and other novel approaches may help to answer these questions by identifying differential biological markers and treatment effects across burnout and depressive subtypes.
Conclusion
Burnout is a term that resonates with many but its merit as a nosological entity remains contentious. While questions remain regarding its definition, differentiation, and diagnosis, Parker has worked to uncover additional symptoms not previously recognised, nuances (e.g. depressive subtyping) which may explain its differing points of overlap and distinction from depression, and ways to conceptualise the condition if it is to become diagnosable. As the lay population continues to steadily endorse experiencing burnout and seek treatment, the contributions by Parker and others reviewed here provide a foundation upon which future assessment, diagnostic considerations, and further research can be built, with such studies likely to have an enduring impact on clinical practice.
Footnotes
Ethical considerations
There are no human or animal participants in this article and informed consent is not required.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.