
Abstract
Background
Intergenerational conflicts (IGCs) are a common feature of family life and are particularly salient in migrant families. Contributory cultural stressors include the acculturation gap.
Aims
This qualitative study explored perceived psychological impacts of IGCs, contexts in which conflicts were experienced and responses to them, by individuals from immigrant New Zealand Chinese families receiving specialist mental healthcare.
Method
Ten adult participants, from both child and parent generations, took part in semi-structured interviews, which were transcribed, coded, and analysed using reflexive thematic analysis.
Results
Three core themes were identified: (1) Types of IGCs and perceived associations with mental illness; (2) Family cultural factors associated with conflicts; and (3) Navigating IGCs and building resilience amid mental illness.
Conclusion
Narratives from this clinical sample of immigrant Chinese-New Zealand mental health service users suggest links between mental illness and intergenerational conflicts within specific personal contexts. Participants associated parenting practices that emphasise achievement, alongside cultural stressors such as the acculturation gap, with parent–child tensions and psychological distress. Biculturalism, faith, social support, and professional assistance are resources that may support resilience and intergenerational reconciliation.
Intergenerational conflicts (IGCs) occur in most families and refer to tension, disagreements, or misunderstandings between family members of different generations, typically parents and children. 1 Conflicts may ensue from differing values and priorities between family members; or be underpinned by contrasting communication styles. 2
Cultural stress theory 3 highlights the cultural and psychological stresses experienced by minority immigrant families. Adapting to a new cultural environment may be associated with impaired psychological adjustment,3,4 which is mediated by family functioning, including conflict between generations. 3 One particular cultural stressor associated with IGCs 5 is the acculturation gap, whereby family members adapt to the host culture at different rates and in different ways. 6
Ethnic Chinese comprise around 5.6% of the New Zealand population, with most (71.1%) being overseas born. 7 Chinese immigrants are likely to experience a cultural distance 8 between Chinese and New Zealand cultures, multiple cultural stressors, 9 and other intersecting disadvantage(s) based on their gender or position in the family hierarchy. 10 Previous research has identified significant yet underreported psychiatric morbidity in immigrant Chinese New Zealanders. 9 Factors associated with under-utilisation of mental health services include language barriers, lack of awareness, and stigma of mental disorders and poor cultural support. 11
Conflicts between generations of Chinese migrant families are well-reported in international literature 2 and associated with symptoms of anxiety, depression,12,13 and psychosis. 14 Resilience factors identified as helpful for individuals’ psychological wellbeing include adjusted expectations, 15 bicultural self-efficacy, 16 harnessing social resources, 12 and faith-based or philosophical worldviews that help to create meaning out of adversity. 17
Rationale for the present study: International literature, primarily focused on young people, suggest IGCs are relevant to the experiences of immigrant Chinese with mental illnesses. Despite the growing Chinese presence in Australasia, there is a paucity of research on the intersection between IGCs and mental illness in this population. This exploratory study aimed to examine subjective experiences of IGCs by adult New Zealand Chinese mental health service users, including conflict-resolution and psychological coping strategies.
Methods
Setting and participants
The research team are first- and second-generation Chinese medical practitioners working in New Zealand. Two members are fluent in the Chinese (Mandarin) language. Interpretive description research methodology was used to scaffold the study, as it explicitly employs a clinician-researcher lens, acknowledges the role of the researchers in all steps of the research process, and returns discipline-relevant knowledge to the field of practice. 18
Participants were recruited from three community mental health and primary care clinics in Auckland Tamaki Makaurau, a region with a diverse population, of whom 11.74% identify as ethnic Chinese. 19 Advertisements displayed at recruitment sites allowed for service users to initiate contact independently. In addition, the treating clinicians at each site were invited to refer eligible service users.
Inclusion criteria were: aged between 18 and 60 years, a Diagnostic and Statistical Manual of Mental Disorders (DSM-5) diagnosed mental illness, self-identification as Chinese, and either first- or second-generation migrants. Exclusion criteria were inability to provide informed consent and acute psychiatric symptoms limiting participants’ ability to participate. Participants for whom any of the researchers had been the treating clinician were also excluded.
Ethical considerations
Ethics approval was obtained from the New Zealand Health and Disability Ethics Committees (HDEC) (Ethics reference: 2023 EXP 15582) and locality approval gained from Health New Zealand Te Whatu Ora Te Toka Tumai. The conduct of this study adhered to the New Zealand National Ethical Standards for Health and Disability Research and Quality Improvement. All participants provided written informed consent using a bilingual consent form, with explanations given in their preferred language by RY. To ensure confidentiality, we replaced the names of the participants with participants’ codes and all identifying information was removed from the transcripts.
Data collection
Interview schedules for participants
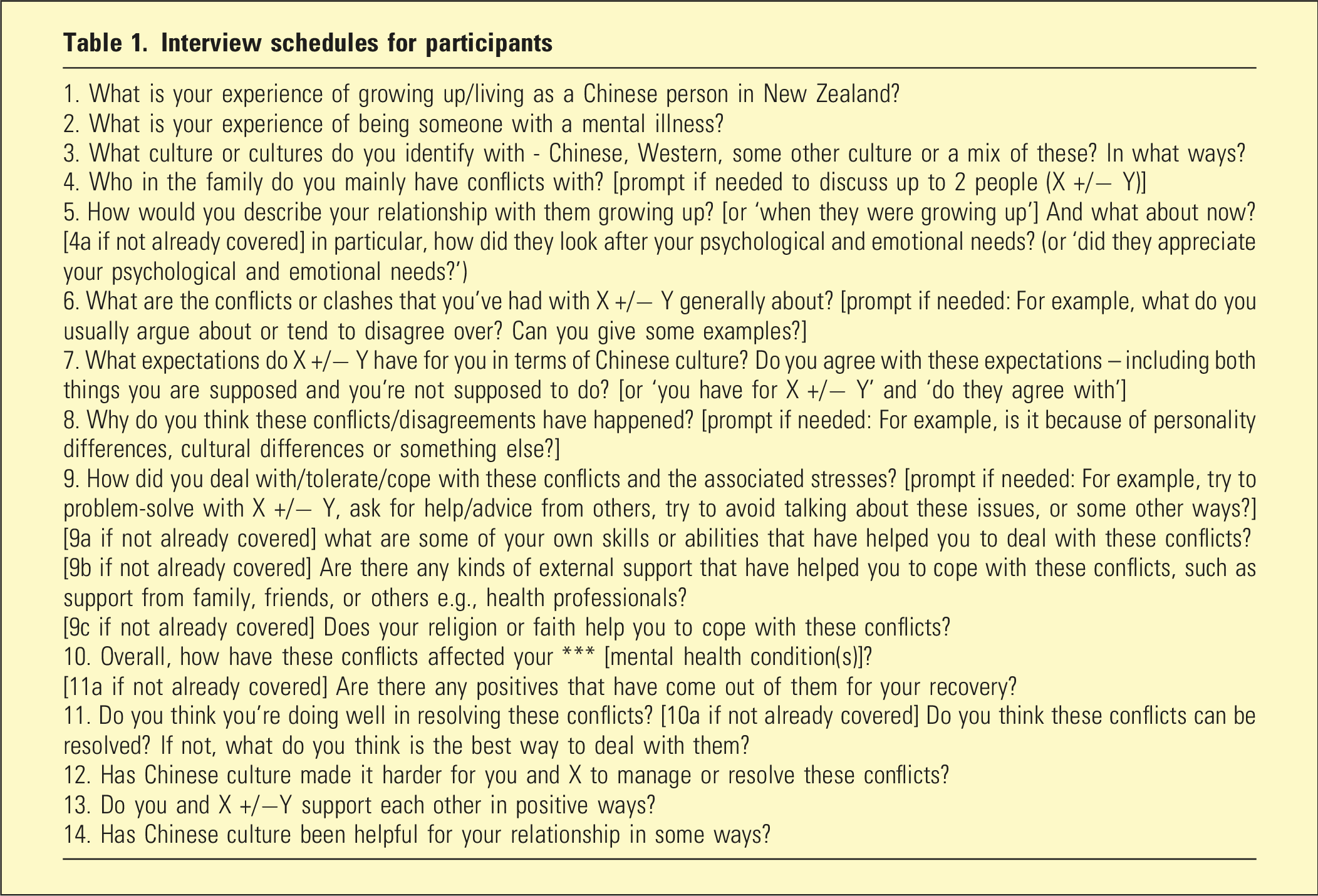
Interviews were conducted in the participant’s preferred language, either in person or online, after completing a demographic questionnaire. Details of psychiatric diagnoses were obtained from referring clinicians and verified with participants. All interviews were audio-recorded and transcribed verbatim.
Data analysis
English interviews were transcribed verbatim by a professional transcriber. Chinese-language interviews were transcribed in Chinese and translated into English by an experienced Chinese translator and second independent contractor. Back translations were undertaken for all Chinese-language interviews in full by the first author (RY), who is fluent in both Chinese and English, with the assistance of deepL translation tool, to check for consistency of thematic representation between the English translation and original texts. Where there were concerns regarding conceptual non-equivalence/semantic drift (less than 10% of text) the translation was discussed with the transcriber and co-authors to agree on an alternative translation, in consideration of broader contexts of the interview. When this occurred, changes primarily related to nuances of meaning, culturally embedded expressions, and the interpretation of emotionally laden terms rather than substantive differences in content.
Interview data were analysed using reflexive thematic analysis, 20 supported by NVivo software for data management, using the following process: familiarisation and intensive data engagement, independent data coding by three authors [RY, RL, and LN] on an iterative basis with generation of initial themes, discussion and refinement of themes based on key organising concepts, and final consensus on themes among all authors after checking against data. Additionally Chinese-language interviews were coded in the original Chinese transcript [GC] and by an independent coder (a Chinese psychiatrist). These codes were considered alongside those generated from the English translations during thematic development. Differences in coding or interpretation were discussed with reference to both the Chinese and English texts until a shared understanding of the underlying meaning was reached. With the research team’s Chinese cultural backgrounds, the interpretation of data was also facilitated by our combined clinical and personal experiences, and independent coding by different coders in both languages facilitated reflexivity and deeper interpretive analysis.
Results
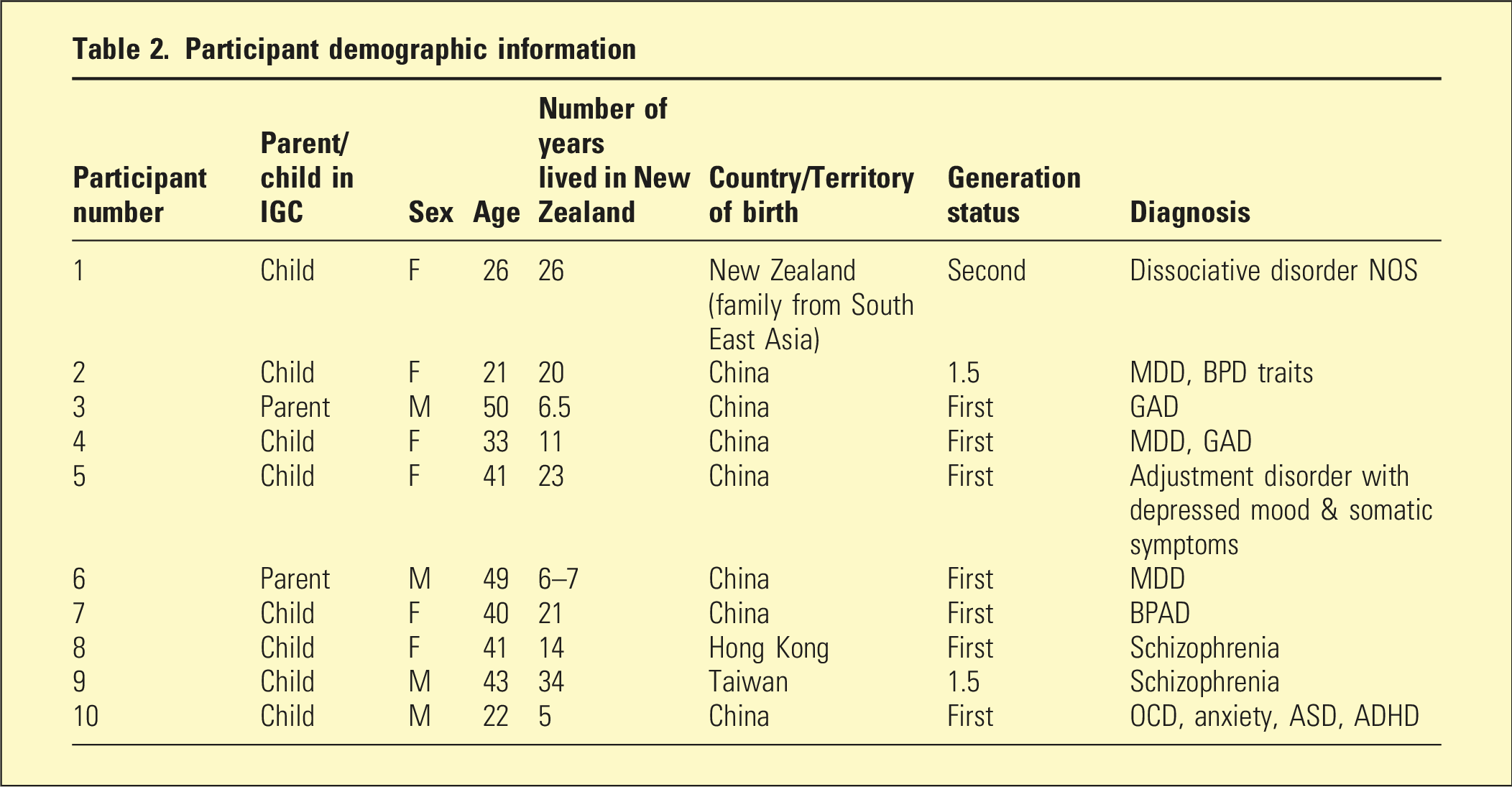
Participant demographic information
Themes
There were three main themes: (1) Types of IGCs and perceived associations with mental illness; (2) Family cultural factors associated with conflicts; and (3) Navigating IGCs and building resilience amid mental illness.
Data to support themes
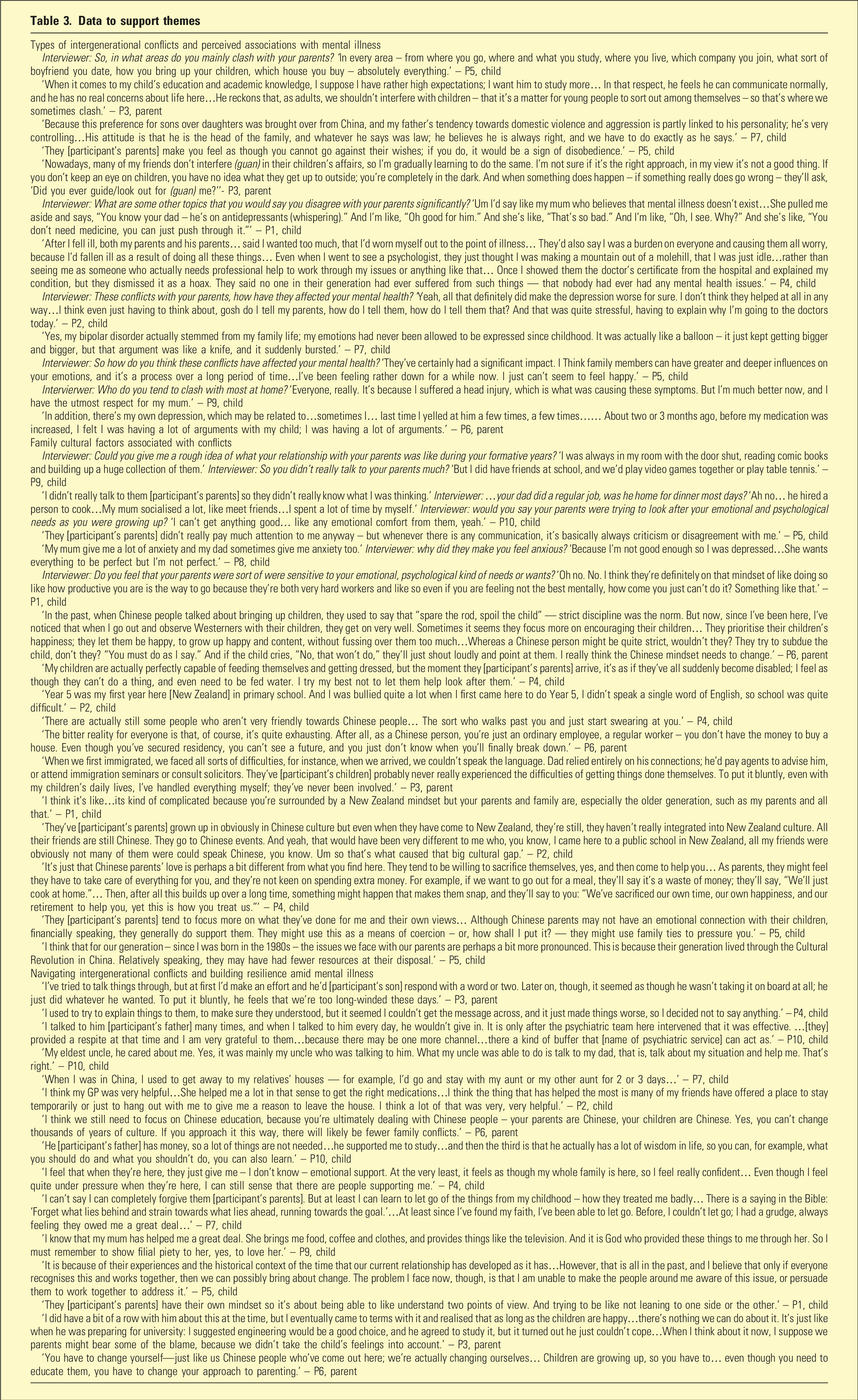
Theme 1: Types of IGCs and perceived associations with mental illness
IGCs were most commonly attributed to clashes over a variety of topics and values, including filial piety (孝顺), patriarchy, paternalism, educational/occupational achievements, accommodation, marriage/childbearing, friendships, parenting of the third generation, substance use, and gender identity. Indeed, there was a common perception that parents sought to impose their own values globally over a child’s life choices under the guise of benign paternalism. While parent-generation participants expressed helpful intentions to guide/supervise (管, guan) their children’s behaviours, child-generation participants sometimes interpreted these as interferences that were poorly suited to their own circumstances. These differing interpretations were frequently associated with experiences of conflict and psychological stress.
Some participants described IGCs arising from mismatched mental health-related beliefs. They recounted experiences in which parents appeared to dismiss medical explanations for distress or questioned the need for treatment. One participant described feeling blamed by her parents for her illness and for causing family disharmony as a result, moralised through traditional gender norms. Another participant described experiencing stigma and emotional distancing from parents following a diagnosis of schizophrenia.
Several participants perceived relationships between particular personality traits of family members and conflict frequency and intensity. Regardless of how those arose, participants generally endorsed negative impacts of these conflicts on their psychological wellbeing and mental illnesses. Conversely, some participants reflected that symptoms of mental illness had shaped their behaviours and interactions in ways that intensified family conflicts.
Theme 2: Family cultural factors associated with conflicts
Most child-generation participants described family cultures where parents appeared to lack interest, capacity, or skills to respond to their emotional needs since childhood. Participants frequently associated this perceived lack of emotional understanding and support, along with high parental criticality, with detrimental effects on their mental wellbeing. Multiple participants commented on the continuing sense of emotional distance between themselves and their parents/children. Conversely, two participants associated parental emotional overinvolvement with psychological stress, one in relation to herself and the other in relation to her own children.
Participants, particularly those from the parent-generation, made links between cultural stress factors arising through migration and increased IGCs. These ranged from economic hardship, unemployment, to language barriers and discrimination, leading to downward social drift, that is, downward movement in socioeconomic position. Participants linked these experiences to psychological distress and described how unacknowledged parental sacrifices and aspirations for children could result in intergeneration friction. The acculturation gap as a cultural stressor was commonly discussed by participants as an important contextual factor for both IGCs and mental distress. These were underpinned by divergent values, beliefs and behavioural choices between generations that created misunderstandings and disagreements. Some participants interpreted these differences as reflecting broader generational differences in social environments and experiences, rather than migration alone.
Theme 3: Navigating IGCs and building resilience amid mental illness
While some participants found open communication with their family members helpful, a majority described difficulties in resolving conflicts through direction communication, which often instead led to withdrawal, avoidance and further emotional suppression. Multiple participants cited intervention and support from others, including spouses, relatives, and mental health professionals as beneficial. Other helpful factors were maintaining resilience while navigating conflicts, psychotropic medications, individual psychotherapy, creative art, and support from friends. While professional supports were mostly positively received, one participant noted limited therapeutic resonance with psychotherapy due to their perceived mismatch between Western therapy models emphasising individual autonomy and their own Chinese family’s value system.
When reflecting on possibilities for intergenerational reconciliation, participants from both generations acknowledged the need for and endorsed observed efforts in mutual understanding and self-reflection, which included children learning about and respecting aspects of Chinese culture, and parents appreciating and adopting aspects of Western-style parenting. Some participants wanted to spend more time together as a family. Several participants positive aspects of the intergenerational relationship, particularly caring supports. Four participants highlighted religious faith as important for individual emotional healing and intergenerational reconciliation. Others described difficulties translating intentions for reconciliation into effective practical actions, due to lack of knowledge and skills, and reported difficulties in locating resources to help them resolve IGCs.
Discussion
This exploratory study sought to understand immigrant Chinese mental health service users’ experiences of IGCs. Participants’ narratives identified salient recurring themes and lent insights into meanings attached to distress, interpretations of family dynamics and stressors, and reflections on coping, resilience, and reconciliation. These findings can be understood as context-bound accounts constructed within the intersecting clinical, cultural, relational, and personal circumstances of this sample; rather than implying representation of Chinese parenting or intergenerational family relationships more broadly.
Our findings align with previous research suggesting bidirectional associations between family conflicts and mental distress. This literature indicates that mental illness can predispose family systems to stress and intrafamilial conflicts, 21 as emotions are suppressed and communication difficulties maintained. 22 Conversely, IGCs, linked to high expressed emotion 23 and unmet filial expectations, 24 are associated with increased psychological symptoms and distress.
Stigmatised attitudes towards mental illness are still held by many Chinese people.25,26 When such attitudes are expressed by family members, can create perceptions of being blamed, criticised, or emotionally unsupported during periods of psychological difficulty. Conflicts in cultural values including patriarchal preferences and filial piety noted by the study participants have been reported in other research. 27
Traditional Chinese culture emphasises parents’ role in guiding and regulating children’s behaviours to enable children to succeed academically and socially.28,29 Within cultural concepts of parenting such as ‘guan’ (管, guidance/discipline), parental control and criticism can function as care – aimed at improvement rather than rejection, with parental authority used to protect the child’s best interests. 28 Love and warmth may be conveyed instrumentally rather than verbally, through investing in education and providing practical support. 30 When experienced within the broader socio-cultural context of the host country however, children can experience such practices as pressure to achieve, emotionally distant or overinvolved, censorious, and authoritarian, 31 and associated with psychological distress. 29
Consistent with cultural stress theory, participants frequently endorsed the presence of cultural stresses, including the acculturation gap, as important contexts within which IGCs were experienced. Migration brings challenges including discrimination, financial strain, and loss of social networks. 32 These difficulties may contribute to economic precarity or downward social mobility experience by parent-generation participants. This may further elevate implicit pressure on children to succeed 29 and to reciprocate parental sacrifice through filial obligations. Other cultural stressors, such as a need to work long hours or bicultural identity tensions, may render parents emotionally less available or overprotective, while sensitising children to perceived parental criticism. 3
In adaptively responding to IGCs, many participants’ described conflict avoidance as their default strategy. This can reduce short-term tension but increase risks of further emotional distancing 21 in family systems already strained by poor communication and trust; for some, the associated emotional suppression can lead to mental distress. 33
Conversely, mutual perspective-taking and behavioural changes effected by both generations have been reported to foster intergenerational understanding.12,34 The concept of biculturalism, that is, the integration of knowledge, behaviours, and identity from both heritage and host cultures, 35 can be gainfully embraced by both generations. Specifically, children could balance desire for autonomy with respect for filial piety 36 and engage with Chinese cultural customs and knowledge15,37; while parents might espouse more emotionally attuned communication styles 38 and allow for greater autonomy of children according to their developmental stage.12,16 Participants’ narratives support the argument for parenting styles within immigrant Chinese families to combine strong limit setting and high expectations with both emotional and practical supports, for pursuits aligned with a child’s strengths and own aspirations.
Professionals and family members with authority may serve positive functions in alleviating IGCs, given an inclination to defer to authority in Chinese culture. 39 Informal family and community supports may be particularly useful for immigrant Chinese where cultural stigma could limit helping-seeking from mental health services, 40
Taken together, participants’ narratives suggest that filial piety, guan, and related beliefs and practices regulating parent–child relationships form part of the meaning-making framework through which IGCs, in relation to mental wellbeing, were individually interpreted and understood. Such frameworks are also created through other psychological and social determinants of mental health at the structural, relational and individual levels, 41 for example, minority stress, socioeconomic constraints, personality factors, and spiritual beliefs. Effective support for conflict reduction in these families means intervenes on multiple factors. Our findings suggest the potential value of approaches that create opportunities for family members to discuss important matters in an emotionally contained and safe setting. Topics of interest include host-vs-heritage and generational cultural gaps; individual circumstances, experiences and meaning-making; and, the impact on differing assumptions, experiences and interpretations of shared event.
Considerations for practice
This study revealed associations between cultural stressors, intergenerational conflicts, and experiences of mental illnesses in immigrant Chinese-New Zealanders utilising mental health services. Current psychiatric interventions for adults are typically individual-focused, overlooking the family system’s role in illness and recovery. Community-based education to reduce cultural stigma and family-based interventions that target the nexus of culture values, health beliefs, and communication patterns may be valuable. International educational programs enhancing bicultural awareness, emotional attunement, and communication30,42 have shown benefits in improving parent–child relationships. Alleviating cultural stressors experienced by patients and family members is also relevant.
In other studies, problem-solving 16 and peer support26,40 in relation to IGCs have achieved improved psychological outcomes. Peer-led support groups, facilitated by local Asian mental health teams or non-governmental organisations such as Asian Family Services, could foster shared learning and growth within each generation. In the context of New Zealand’s growing Asian population, enhanced government investment in family-inclusive mental health services could improve outcomes for Chinese immigrants experiencing mental illness and family conflicts.
Strengths and limitations
This exploratory study involved a purposive sample of immigrant Chinese mental health service users, an underrepresented cultural group in mental health research in Australasia. The use of an interpretive description methodology 18 through a dual clinician–researcher lens, by researchers of Chinese cultural backgrounds, fostered rapport and open communication with participants during data collection and enriched the analysis through strong reflexive engagement. Consistent with this methodological framework, information power, that is, that data collected provides relevant and rich information to support practice-useful interpretations, rather than data saturation, is a key concept in determining data adequacy. 43 Thus, despite the modest sample size, results provided novel and meaningful insights which are of high clinical relevance for this population, notably with respect to meaning-making of family dynamics and conflicts, as well as experiences in seeking conflict resolution and mental resilience, supporting the information power of this study in relation to its aims.
Our study, however, have inherent limitations of the sampling method 44 and in the transferability of findings, particularly to Chinese immigrants not presenting to health professionals. The paucity of self-referred participation may reflect persisting stigmatised attitudes towards help-seeking for mental illness, 45 desire to keep family conflicts private, 13 and to avoid controversial discussion, as seen in the phenomenon of courtesy bias, 46 all issues that need addressing to improve service engagement and outcomes for all immigrant Chinese with mental illnesses. Participants’ accounts represent context-bound understandings of Chinese family relationships in specific clinical settings, cannot be generalised to Chinese culture or families generally, especially in considering intersecting factors such as family roles and socioeconomic positions.
The research team’s Chinese cultural background served as a resource for interpretation of data, for example, with implied meanings of expressions used and identification of clinically salient narratives. Nevertheless, there was a risk of cultural assumptions being taken for granted, and this was addressed through reflexive discussions where data was reviewed to confirm interpretations.
Directions of future research
We suggest future research to explore second-generation migrants’ perspectives of acculturative/bicultural stress and mental illness, who have a higher mental illness burden than first generation migrants. 47 Perspectives of family members on family conflicts and supporting a family member with mental illness would also be invaluable. It may be useful to compare IGCs with host and other migrant groups, which was beyond the scope of this study, to gain additional insights on their culture-specific dimensions.
Conclusion
Narratives from this clinical sample of immigrant Chinese-New Zealand mental health service users, best understood within each participant’s specific clinical, cultural, migration, and relational contexts, suggested perceived interconnection and mutual influence between mental illness and intergenerational conflicts. Participants also described parenting practices characterised by guidance, high expectations, and a stronger emphasis on achievement than emotional expression, that within the context of cultural stressors, are experienced as authoritarian, controlling, or critical, and associated with feelings of limited parental support, heightened parent–child tensions, and emotional distress for both generations. Participants identified a range of resources that support resilience and intergenerational reconciliation, including biculturalism, religious faith, social support, and assistance from trusted others, including professionals. Culturally responsive, family-oriented interventions may help support bicultural adaptation, mutual understanding, and constructive communication across generations.
Footnotes
Acknowledgements
The authors would like to thank all the participants who engaged in this research, contributed their data and shared their stories; as well as colleagues who provided valuable feedback and support for the study, including the work done by the data translator and transcribers.
Ethical considerations
Approvald were obtained from the Health and Disability Ethics Committees (HDEC) (Ethics reference: 2023 EXP 15582) and Health New Zealand Te Whatu Ora Te Toka Tumai. The conduct of this study adhered to the New Zealand National Ethical Standards for Health and Disability Research and Quality Improvement.
Consent to participate
Written informed consent was obtained from all participants at time of entry into study for participation and publication of research results.
Author contributions
Dr Richard Yu - Principal researcher, study design, recruitment of participants, conduct of interviews, data interpretation and analysis, and report writing. Dr Gary Cheung – Co-supervisor, study design and report writing. Dr Rosie Luo – Associate researcher, data interpretation and analysis. Dr Lillian Ng – Primary supervisor, study design, data interpretation and analysis, and report writing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author received the RANZCP (Royal Australian & New Zealand College of Psychiatrists) Foundation Beverley Raphael New Investigator Grant to cover the costs of the research and publication of this article. The authors did not receive any financial reward personally.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The anonymised data that support the findings of this study are available from the corresponding author upon reasonable request.