
Abstract
Objective
To assess the effectiveness of Western Australia’s first public, voluntary, inpatient eating disorder program in improving client weight, BMI, eating disorder cognitions and behaviours, and depression, anxiety and stress levels, and to identify factors associated with self-discharge, over the first 12 months of operation.
Methods
Clients participated in a multidisciplinary team eating disorder program comprised of meal support, group education sessions, and one-on-one clinician reviews. Weight, BMI, Global EDE-Q, and DASS-21 scores were compared at admission and discharge. An analysis was completed to identify variables predicting self-discharge from the program.
Results
There were 81 admissions over a 12-month period. Weight and BMI were significantly higher at discharge compared to admission, and Global EDE-Q, depression, anxiety, and stress scores were significantly lower. The self-discharge rate was 21%. Older age was associated with lower chance of self-discharge, while admission BMI, referral source, and diagnosis demonstrated no association with self-discharge.
Conclusions
These results broadly support the effectiveness of the program in increasing client weight and BMI, reducing eating disorder cognitions and behaviours, and improving depression, anxiety and stress levels. The high self-discharge rate should prompt further investigation and reflection on strategies to improve client retention and engagement.
Background
Eating disorders are a group of complex mental health conditions associated with significant negative physical and mental health outcomes.1,2 Standardised mortality rates are significantly higher in those with eating disorders compared to the general public, particularly anorexia nervosa which confers a five-fold increased risk of death. 3 Concerningly, the prevalence of eating disorders is increasing in Australia.4,5 Approximately 1.1 million Australians (∼4.5% of the population) were living with an eating disorder in 2023, a 21% increase since 2012. 5 Multiple ‘stepped’ levels of intervention are utilised in the provision of care to those with eating disorders, including community teams, day programs, residential programs, and inpatient admissions. 6 Intensive eating disorder management, including inpatient admission, has been demonstrated to significantly improve Body Mass Index (BMI), disordered eating, and levels of depression. 7 Additionally, 24/7 care produces a higher rate of weight gain in those with low BMI, compared to non-24/7 care. 8 Residential programs have been demonstrated to improve eating disorder psychopathology, weight, and affective symptoms, 9 and when compared with day programs are associated with greater outcomes. 10 Previous research calls for further investigation and comparison of the differences in treatment outcomes between varying levels of care.9,10 The effectiveness of inpatient treatment is relevant in this context given the significantly higher healthcare systems costs of inpatient management compared to outpatient options.
Relapses of anorexia nervosa following inpatient admission are common, with estimated rates of approximately 50% at 12 months post-discharge. 11 Low BMI at discharge following weight-restoring treatment is associated with relapse, with relevant literature recommending a treatment goal BMI above 20. 11 Current local guidelines recommend medical admission for physiological stabilisation at BMI <14 for adults, 12 and anecdotal feedback indicates that those admitted to medical wards are frequently discharged back into community at BMI <18.5, resulting in a proportion of individuals who chronically remain in a BMI range 14–18. General practitioners are often too under-resourced in time, education, and specialist team support to adequately treat eating disorders, 13 creating a gap in intensive public services between medical admission and community supports. This precludes the opportunity to further weight-restore clients in an inpatient setting and lower their risk of relapse.
In October 2024, Western Australia’s first public, voluntary psychiatric inpatient eating disorder program commenced. The seven-bed unit accepts clients state-wide, acting as either a ‘step-down’ service from inpatient medical and psychiatric wards, or a ‘step-up’ service from community mental health or eating disorder teams, GPs, or psychologists. The program’s aim is to provide an effective service for individuals who are medically stable and would benefit from a voluntary, inpatient admission for weight restoration and MDT eating disorder management. The first 12 months of operation provided an opportunity to appraise the program’s ability to achieve this goal.
Aims
Data were collected during the first 12 months of the program’s operation to: (1) Assess the effectiveness of the program in increasing weight and BMI, reducing eating disorder cognitions and behaviours, and improving depression, anxiety, and stress levels, and (2) Identify demographic or presentation factors which predict self-discharge from the program.
Methods
To meet admission criteria, clients were required to be female, voluntary, ≥18 years old, with BMI >14, and have either an established eating disorder diagnosis (anorexia nervosa, atypical anorexia nervosa, bulimia nervosa, Avoidant Restrictive Food Intake Disorder (ARFID), binge eating disorder, or Other Specified Feeding or Eating Disorder (OSFED)) or strong clinical suspicion for an eating disorder. Common reasons for decline of referral included the inability to manage the person’s current medical or psychiatric risk on an open psychiatric ward, and a principal presenting diagnosis other than an eating disorder. Admitted clients participated in an MDT program comprised of input from nurses, dietitians, clinical psychologists, psychiatrists, junior doctors, social workers, occupational therapists, exercise physiologists, and a peer support worker. The program was composed of six supervised meal support sessions per day, two one-hour group sessions per day on weekdays, and one-on-one reviews with MDT members determined by individual need. Group sessions were presented by MDT members and covered topics including sensory modulation strategies, approaching relationships, nutrition education, emotions, food preparation, relaxation, and craft. Individualised meal plans were created for each client following assessment by a dietitian, with changes made to meet energy intake requirements as the admission progressed. Collaboration and trust with clients were prioritised through the program’s voluntary structure and provision of personal en-suite bathrooms, despite associated purging risk. Repeated meal plan non-adherence triggered discussions of facilitating increased supports for the client, with consideration of clinician-led discharge only occurring after other options were explored. Discharge from the program was either organised collaboratively between the treating team and client, or self-initiated by the client, each with concurrent appraisal of psychiatric and medical risk. Clients who self-discharged from the program were identified for subsequent analysis of demographic and presentation variables. If the same client was admitted more than once over the data collection period, the data from each of their individual admissions were included separately.
Weight, BMI, Global Eating Disorder Questionnaire (EDE-Q) scores, and Depression, Anxiety and Stress Scale 21 Items (DASS-21) scores were collected at admission and discharge for clients admitted between 21st October 2024 and 20th October 2025. Client age, principal diagnosis, referral source (inpatient vs community), and length of stay were recorded.
The EDE-Q is a widely used, validated, self-reported, 28-item questionnaire. 14 It quantifies eating disorder psychopathology over the preceding 28-day period by measuring intake restriction, eating concern, weight concern, shape concern, and related behavioural symptoms including frequency of binge eating, vomiting, use of laxatives or diuretics, and overexercising. Global EDE-Q is derived from points in these subscales, with higher scores indicating higher severity of eating disorder cognitions and behaviours. The possible range of scores is 0–6, with scores >2.5 suggesting clinically significant symptoms.
The DASS-21 is a validated and widely administered 21-item self-reported questionnaire used to assess psychological distress. 15 It is comprised of three seven-question subscales for depression, anxiety, and stress, and uses a four-point frequency scale (0 = Did not apply to me at all, 1 = Applied to me to some degree, or some of the time, 2 = Applied to me to a considerable degree, or a good part of the time, 3 = Applied to me very much, or most of the time), with higher scores indicating higher levels of psychological distress. The range of possible scores for each subscale is 0–21, with a maximum total DASS-21 score of 63.
Statistical analysis
Scores for the depression, anxiety, and stress subscales comprising the DASS-21 were analysed independently. Using Cronbach Alpha testing, internal consistency of the DASS-21 and EDE-Q in the sample were 0.85 and 0.92, respectively. Assessment of normality was completed on admission and discharge weight, BMI, Global EDE-Q, depression, anxiety, and stress scores. Depression scores were found to be distributed normally, with weight, BMI, Global EDE-Q, anxiety and stress scores distributed non-normally.
A comparison of means at admission and discharge was completed using paired T-testing for the normally distributed variables (Depression scores), and Wilcoxon signed-rank testing for the non-normally distributed variables (Weight, BMI, Global EDE-Q, anxiety, and stress scores). A two-sided p-value of <0.05 was considered significant. If admission or discharge paired data were missing for a given variable for a client, that client’s data was excluded from the comparison of means testing for that variable.
Univariate and multivariate logistic regression analyses were completed using client age, admission weight, admission BMI, referral source, and diagnosis to assess for significant predictors of self-discharge. The univariate logistic regressions used pairwise NA handling per predictor to handle missing data. Admission weight was excluded from the multivariate analyses to avoid collinearity with admission BMI, and multivariate results were based on complete cases across included predictors.
Results
Over the 12-month data collection period, the program received 147 referrals and accepted 104. Referrals were accepted for 23 people who subsequently declined admission.
Eighty-one referrals were admitted to the program, with 20 (25%) admitted from inpatient referrals, and 61 (75%) referred from community. Mean age of admitted clients was 29.5 years (Range 18–65 years) and mean length of stay 23.7 days (1–70 days). Most clients (61.7%) had a principal presenting diagnosis of anorexia nervosa, followed by atypical anorexia nervosa (30.9%), ARFID (3.7%), bulimia nervosa (2.5%), and OSFED (1.2%). Over the sample period, 18 clients were admitted to the program more than once, with 14 admitted twice, three admitted three times, and one admitted four times.
Self-discharge was initiated by 17 clients, 21% of those admitted. The mean admission length of stay of these clients was 6.3 days (1–21 days), with 11 (14% of admitted clients) self-discharging within the first 72 hours of admission. Three cases (4% of admitted clients) required transfer to other hospitals due to medical or psychiatric risk of a severity unmanageable in an open psychiatry ward. Referral, admission, discharge, self-discharge, and transfer proportions are described in Figure 1. Pictorial proportional representation of client disposition over admission course.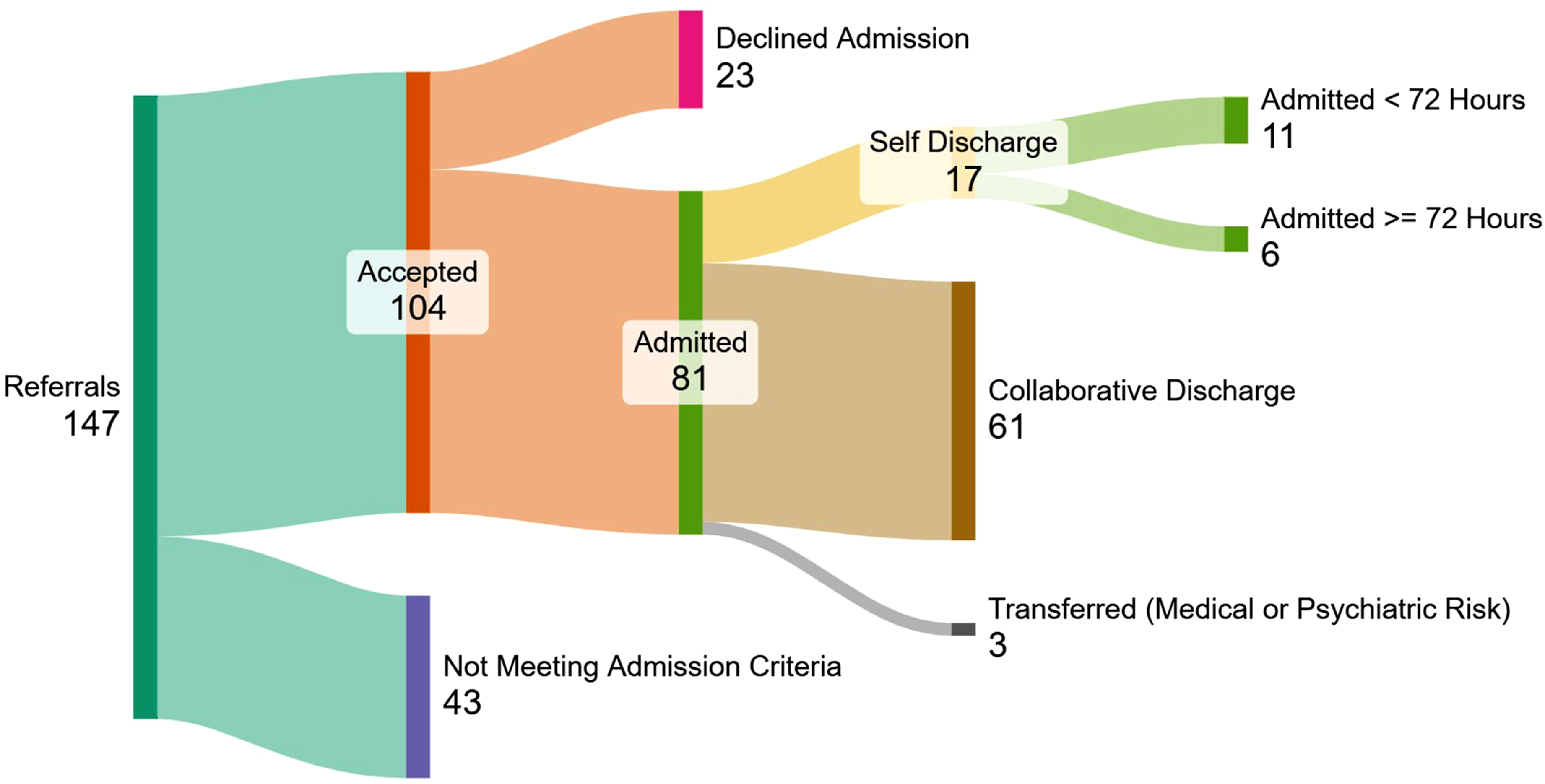
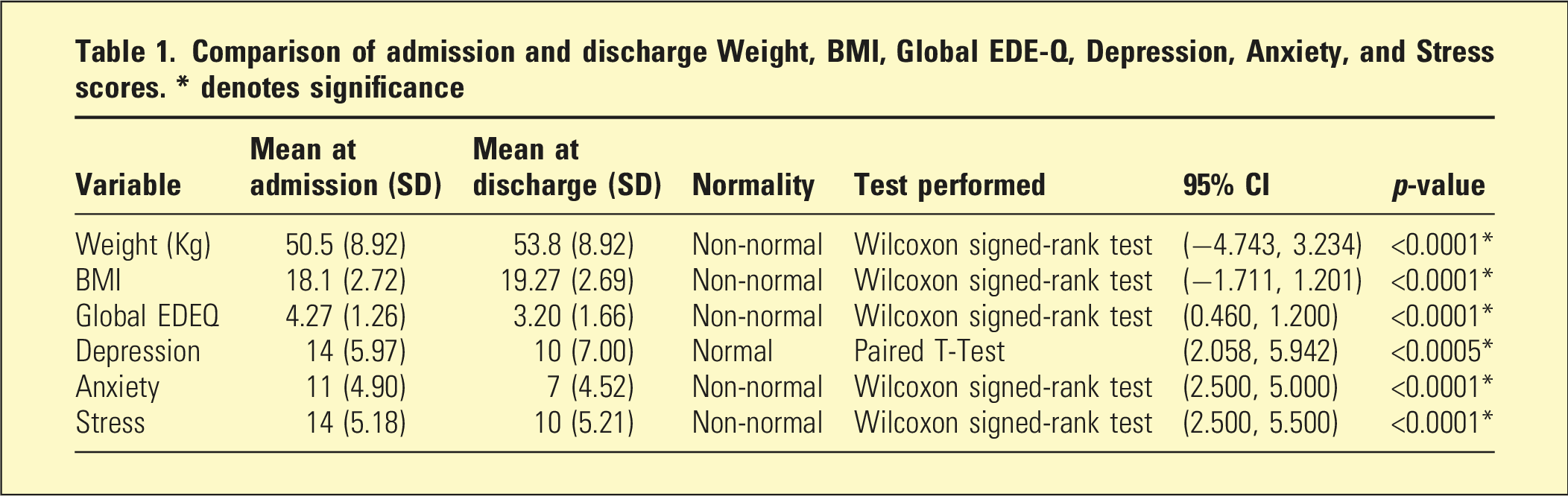
Comparison of admission and discharge weight, BMI, Global EDE-Q, depression, anxiety, and stress scores
Comparison of admission and discharge Weight, BMI, Global EDE-Q, Depression, Anxiety, and Stress scores. * denotes significance
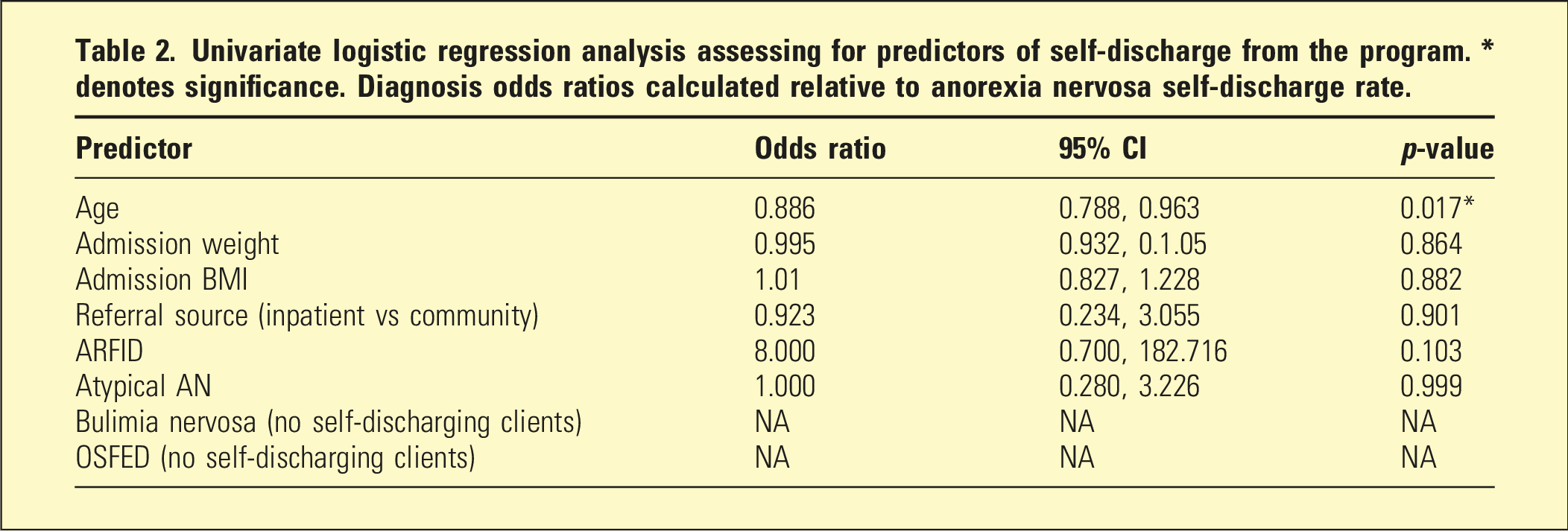
Predictors of self-discharge
Univariate logistic regression analysis assessing for predictors of self-discharge from the program. * denotes significance. Diagnosis odds ratios calculated relative to anorexia nervosa self-discharge rate.
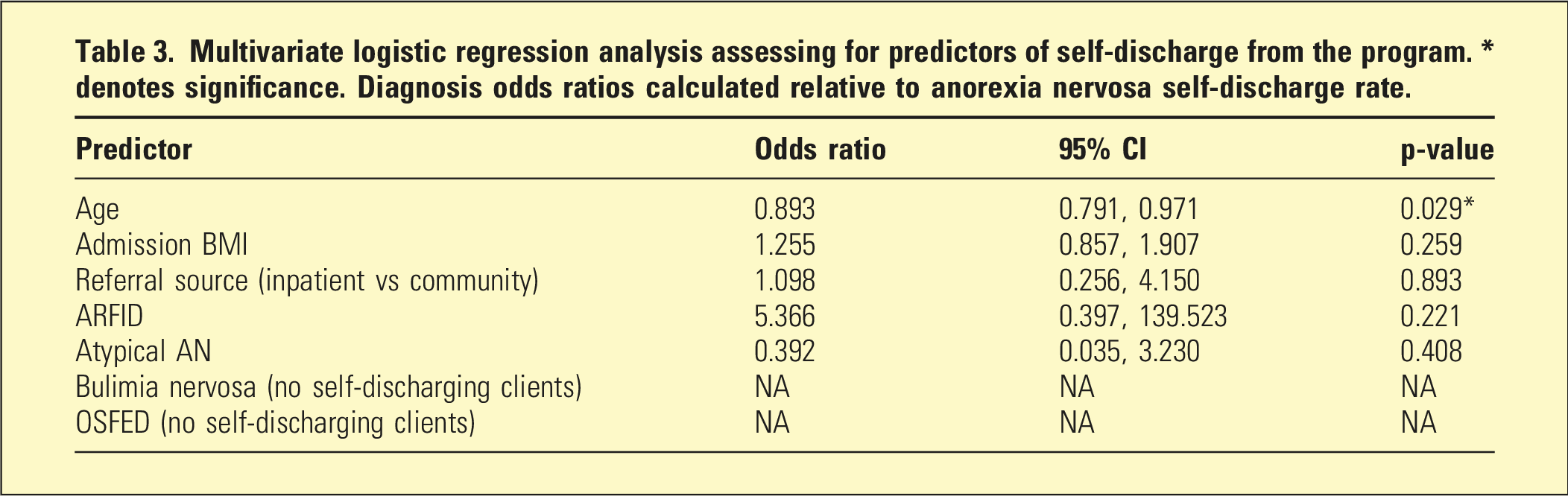
Multivariate logistic regression analysis assessing for predictors of self-discharge from the program. * denotes significance. Diagnosis odds ratios calculated relative to anorexia nervosa self-discharge rate.
Discussion
Statistically significant increases in weight and BMI at discharge compared to admission provide support for the effectiveness of the program at achieving weight restoration for clients. Changes in weight and BMI were not analysed relative to admission length, so this result can only speak to absolute change over the course of admission, not rates of weight and BMI change. This is a limitation of the study design, and further data collection and analysis could provide valuable insight into rates of weight and BMI change over the course of admission.
Significant decreases in Global EDE-Q during admission indicate the program facilitated improvements in eating disorder cognitions and behaviours for clients. Depression, anxiety, and stress scores fell significantly between admission and discharge, supporting the program’s effectiveness in reducing the severity of psychological distress.
These results are in keeping with previous literature which demonstrates intensive eating disorder management reduces eating disorder behaviours and depression levels while increasing BMI. 7 While they broadly support the effectiveness of the program there are several significant limitations and potential areas for further investigation.
The exclusion of those with missing admission or discharge data from the comparison of means testing represents a significant limitation. The fifteen excluded clients represent ∼18% of the sample. The high proportion of these clients who self-discharged (93%) is relevant, as the circumstances leading to self-discharge likely affected clients’ willingness to complete discharge questionnaires, contributing to missing data. As clients who self-discharge are likely to be those who struggled most, their exclusion likely falsely inflates the effectiveness of the program. The self-discharge rate of 21% represents a significant proportion of clients. The majority (65%) of self-discharges occurred within 72 hours of admission, indicating a rapid decision to leave the program. Previous literature has demonstrated higher levels of emotional dysregulation, and more severe depressive symptoms and eating disorder cognitions at admission are associated with earlier termination of inpatient admissions, 16 and these factors may have contributed to early self-discharge rates in this sample. Collection of further quantitative and qualitative data from self-discharging clients at admission and discharge could inform understanding of factors contributing to self-discharge from the program and subsequently direct strategies to increase client retention and engagement.
For clients who completed multiple admissions, including paired data from each admission separately in the statistical analysis strictly violates the assumption of independence in paired t-testing and Wilcoxon signed rank testing. Following consideration, this was deemed preferable to retain the resolution of data from separate admissions, as each admission represents a different stage of recovery for clients and warrants independent measurement. It is acknowledged that this may decrease the validity of the comparison of means results.
Another significant limitation of this study is the lack of long-term follow-up. In the context of anorexia nervosa’s high relapse rate, assessing if improvements in weight, BMI, eating disorder cognitions and behaviours, and psychological distress levels are sustained following discharge is integral to accurately appraise the program’s effectiveness. This would also improve the interpretation of EDE-Q outcomes, as changes in eating disorder-related behaviours during admission may represent superficial adherence to program structure, rather than genuine changes in eating disorder cognitions. Further research with long-term follow-up is required to address these shortcomings. While Global EDE-Q scores decreased between admission and discharge, the mean score of 3.2 at discharge remains in a range suggestive of significant symptoms. This highlights a need for continued care following discharge with an aim to further reduce symptomatology.
The significantly decreased odds of self-discharge associated with older age, with most self-discharges occurring early in admission, is out of keeping with previous literature demonstrating longer durations of stay for adolescent clients in residential eating disorder programs compared to adults. 17 This difference may reflect the relative tolerability of residential versus inpatient program environments or be a product of the increased decision-making autonomy of young adults compared to adolescents who require guardian consent for treatment decisions.
Principal admission diagnosis was found to have no significant ability to predict self-discharge from the program. Low numbers of participants with ARFID (3), bulimia nervosa (2), or OSFED (1) likely preclude meaningful analyses for these diagnoses. Previous literature has demonstrated inpatient anorexia nervosa patients who terminate treatment early are more likely to have a binge-eating/purging subtype diagnosis over restricting subtype. 16 This study did not differentiate between anorexia nervosa subtypes precluding their assessment as separate predictors of self-discharge. The program’s relatively low rate (4%) of transfer to medical or higher-support psychiatric units may indicate the admission criteria are effectively filtering for clients within an appropriate range of medical and psychiatric risk.
An additional notable limitation is the restriction of subjects to female adults. Approximately 33% of reported eating disorder cases in Australia are male, 5 and there is consensus available prevalence data for men likely underestimate case numbers due to gender differences in presentation phenotypes, and male marginalisation in eating disorder research. 18 Further research in male populations is required to assess the efficacy of treatments in this cohort. Furthermore, eating disorders commonly develop in childhood and adolescence, with both anorexia nervosa and bulimia nervosa having a mean onset age of approximately 18 years. 19 Concern has been raised recently regarding increasing prevalence of eating disorders in younger age groups, with the proportion of eating disorder cases aged 10-19 in Australia doubling since 2012. 5 The mean age of participants in this study (29.5 years) is higher than the estimated population mean age of those suffering from eating disorders, reflecting the selected adult population. Combination and comparison of data with research from child and adolescent services could better represent the true population of those with eating disorders.
These results broadly support the effectiveness of the program in increasing weight and BMI while decreasing eating disorder cognitions and behaviours, and improving depression, anxiety, and stress levels. This provides promising evidence that the program is effective in treating medically stable individuals who would benefit from inpatient weight restoration and MDT care. Further research, particularly focussed on long-term follow-up outcomes and factors driving self-discharge and early discharge from the program, would be beneficial to more accurately appraise the effects of the program and improve client retention and engagement.
Footnotes
Ethical considerations
Ethical approval not required as per internal quality improvement committee.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.