
Abstract
Objective
To evaluate the feasibility and perceived helpfulness of Single Session Therapy (SST) as a counselling waitlist management strategy in an Australian public health service.
Method
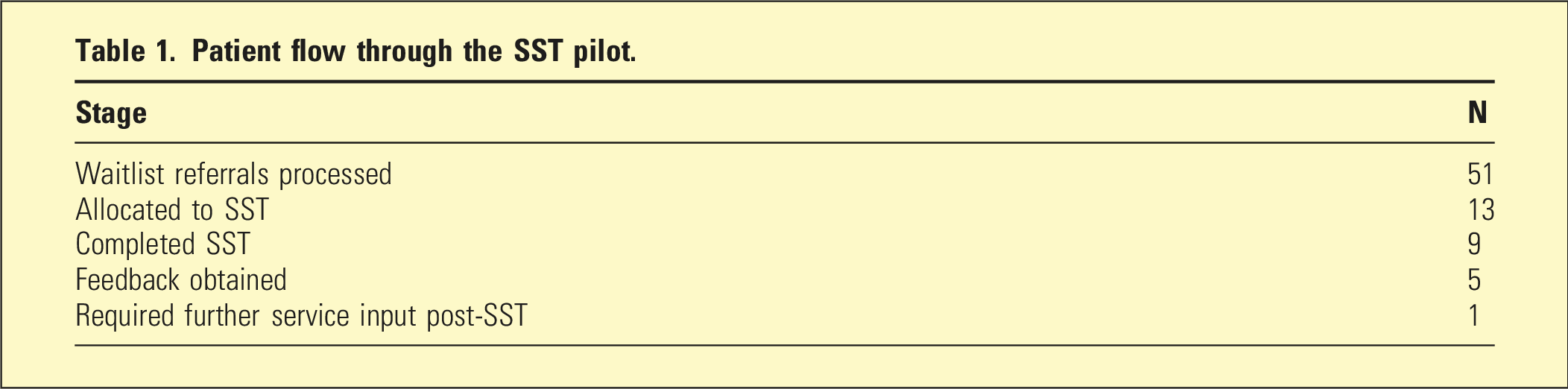
This quality improvement project used a single-group post-intervention design, drawing on routine service data and brief patient feedback from a small SST pilot embedded within a counselling waitlist management initiative at a community health counselling service within Monash Health, Victoria, Australia, between October 2024 and January 2025. Of 51 referrals processed, 13 patients were allocated to SST and 9 completed the intervention. Follow-up feedback was obtained from 5 patients.
Results
Patient-reported helpfulness ratings were positive, with a mean rating of 4.4/5, and all five respondents reported some perceived benefit. Of the nine patients who completed SST, only one required further counselling input from the service. Qualitative feedback suggested that SST was perceived as helpful in increasing awareness, providing practical strategies, and offering an opportunity to speak with a psychologist.
Conclusion
SST may be a feasible and acceptable brief intervention within counselling waitlist management in an Australian public health setting. Findings should be interpreted within the limits of a small local quality improvement evaluation and warrant further service-level investigation.
Keywords
Introduction
Long waitlists for counselling and psychological services are a persistent challenge in mental health care. When demand exceeds service capacity, waiting lists are commonly used, but they raise clinical, administrative, and ethical concerns and may delay timely access to care. 1 Timely access matters because prolonged waits may be associated with worsening distress, unmet need during the waiting period, and increased desire for additional support while awaiting treatment. 2
In this context, brief intervention models may offer a pragmatic way of improving service responsiveness. Single-session therapy (SST), and related single-session intervention models, aim to provide a meaningful therapeutic contact within a limited timeframe and may help bridge treatment gaps when longer-term care is delayed or unavailable. Evidence syntheses suggest that single-session interventions can produce positive effects for at least some mental health outcomes and may have value as low-intensity, scalable, and service-responsive options.3,4 Single-session models have also been examined in real-world service settings, including as routine practice within an acute mental health assessment service, 5 within community addiction and mental health centres, 6 and as a structured single-session intervention in acute and crisis psychology that explicitly incorporates collaborative formulation. 7
Within the Australian context, single-session work has a relatively well-established history in child and adolescent mental health services and in family therapy contexts, including agency-wide implementations and follow-up studies. 8 By comparison, there is limited published evaluation of SST as a waitlist management strategy specifically within Australian adult community-based public health counselling services. The present project contributes preliminary local evidence to that comparatively under-reported area.
This quality improvement project evaluates a small SST pilot implemented within a counselling waitlist management initiative in an Australian public health service. The aim was to examine the feasibility and perceived helpfulness of SST as a brief intervention within routine care, rather than to test treatment efficacy.
Method
Project design and setting
This was a single-group post-intervention quality improvement evaluation using routine service data and brief patient feedback collected as part of usual care. The project was conducted within a community health counselling service at Monash Health, a large public health network in Victoria, Australia. The service receives referrals from general practitioners and from other internal allied health services (e.g. physiotherapy and exercise physiology) and operates as a secondary-care community counselling service. The project ran between October 2024 and January 2025 as part of a broader waitlist management initiative developed in response to substantial waitlist demand.
Participants and allocation
Patients were drawn from the counselling waitlist. Across the project period, 51 waitlist referrals were processed; of these, 13 were allocated to SST and 9 completed the intervention. The number allocated to SST was determined pragmatically by the placement capacity of two provisional psychologists delivering the intervention, rather than by predefined sample size considerations.
Formal inclusion and exclusion criteria were not predefined for this pilot. Patients were allocated to SST pragmatically through the waitlist management process, with consideration of clinical suitability for a brief intervention delivered by provisional psychologists with senior psychologist supervision. In general, patients with mild-to-moderate symptom severity were considered more suitable for SST, while those with more severe, acute, or complex presentations were more likely to be directed to standard service pathways or alternative care planning. The absence of predefined eligibility criteria is acknowledged as a limitation.
Intervention
The intervention consisted of SST delivered primarily via telehealth, with telephone delivery used where patients reported information technology difficulties. SST was offered as a brief, goal-focused intervention informed by established single-session frameworks, which conceptualise the therapeutic encounter as potentially complete in itself while remaining open to additional contact if required.
Within the SST framework, clinicians retained flexibility to select therapeutic approaches based on the presenting concern and the patient’s preferences. This could include collaborative case formulation where the clinician and patient considered it useful, alongside cognitive-behavioural, acceptance and commitment, and solution-focused techniques. The framework does not prescribe a single therapeutic content; rather, it shapes the structure and intent of the contact. In some sessions this involved collaborative exploration of contributing factors, while in others the work was more strategy-focused, reflecting clinician and patient judgement about what would be most useful within the available time.
The session structure included orientation to the clinician’s role and the purpose of the session, discussion of confidentiality and its limits, verbal consent to proceed, identification of the presenting concern, delivery of an SST-informed intervention, collaborative development of an action plan, and clinical documentation (see Supplementary Material 1). Patients were informed that another clinician might contact them approximately 1 week later to ask whether the session had been helpful, and verbal consent for this follow-up call was obtained and documented in the electronic medical record.
Clinicians, training, supervision, and escalation
The intervention was delivered by two provisional psychologists on placement, with supervision from senior clinical psychologists within the service. One supervising senior psychologist had completed formal external SST training; the others drew on broader clinical experience and the internal training materials developed for this project. The provisional psychologists did not undertake formal external SST certification. Internal training was provided through senior psychologist-developed materials, structured role plays, and supervision before and during clinical delivery.
Supervision was provided primarily through routine placement supervision, supplemented by ad hoc consultation as required. The additional senior clinician time associated with the project was directed largely toward developing training materials, conducting role plays, and providing in-session and post-session consultation. Provisional psychologists were instructed to escalate to acute services if acute imminent risk was identified at any point during the intervention, and senior clinician consultation was available throughout the project for complex or rapidly changing presentations.
Feedback procedure and data
Approximately 1 week after the SST session, a clinician other than the treating provisional psychologist contacted patients by telephone. Patients were asked to rate how helpful the session had been on a scale from 1 (not helpful at all) to 5 (very helpful) and to describe how the session had been helpful for them (see Supplementary Material 2). Responses were documented and later summarised for this evaluation. Routine service-level data extracted for the evaluation included the number of waitlist referrals processed, the number allocated to and completing SST, the number subsequently requiring further service input, as well as helpfulness ratings and qualitative feedback where obtained. Quantitative data were analysed descriptively. Qualitative feedback was reviewed and summarised narratively to describe recurring areas of perceived helpfulness.
Ethics and governance
This project was conducted as a Quality Improvement activity within routine service delivery at Monash Health and was reviewed and approved as negligible-risk Quality Assurance by the Monash Health Research Office (ERM Ref: 127303). The project used de-identified service data and patient feedback collected as part of usual care. No additional data collection beyond routine service processes was undertaken. Findings are reported in de-identified summary form only.
Results
Patient flow
Patient flow through the SST pilot.
Helpfulness ratings and qualitative feedback
Among the five patients who provided feedback, the mean helpfulness rating was 4.4/5, and all five reported some perceived benefit. Ratings comprised three responses of 5/5 (very helpful), one of 4/5 (helpful), and one of 3/5 (somewhat helpful). No respondent rated the session as unhelpful, although patients were not explicitly asked about aspects that were unhelpful or could have been improved, which is acknowledged as a limitation.
Qualitative feedback suggested several recurring areas of perceived benefit, including increased awareness of personal issues or thought processes, development of effective strategies, receiving helpful advice or guidance, and having space to speak with a clinician and feel heard. Illustrative responses included: “I now have strategies to better communicate with my partner. It made me more aware of my own thoughts/processing.” “I had someone to discuss my issues with, someone who listened to me carefully, asked questions and explained things to me, and has given me useful advice. That’s what I needed.” “Brought a lot of things to light that I had no knowledge of (e.g. being under coercive control, etc.). I wish I would still have this support.” “Getting things off my chest that I wasn’t able to tell my wife. I could talk with the psychologist.” “I got out of it all that I wanted.”
Service outcomes
Of the 9 patients who completed SST, 8 (89%) did not require further counselling input from the service following SST. One patient was identified as requiring additional psychological support and was escalated directly to longer-term counselling within the service to ensure continuity of care without disruption, rather than being returned to the waitlist.
Discussion
This quality improvement evaluation suggests that SST may be a feasible and acceptable component of counselling waitlist management within an Australian community public health service. Patient feedback was positive overall, and qualitative responses suggested perceived benefit through increased awareness, practical strategies, advice, and an opportunity to speak with a clinician. These findings are broadly consistent with the wider SST literature, which suggests that single-session interventions can be clinically useful across a range of presentations and service contexts.3,4
Although based on a small sample, the service-level outcome data offer a tentatively encouraging signal: the majority of SST completers did not require further counselling input from the service, while the appropriate escalation of the one patient who did demonstrates the operation of the stepped-care pathway. For selected patients, one or two goal-focused session(s) within an SST framework may be sufficient to address the presenting concern, while the broader care pathway remains available for those who need more.
The flexible nature of the SST framework is also relevant to interpretation. Within the model used here, collaborative case formulation was one of the approaches available to clinicians, alongside cognitive-behavioural, acceptance and commitment, and solution-focused techniques. The framework shapes the structure and intent of the contact rather than mandating a specific therapeutic content. This aligns with broader work in single-session and brief intervention settings, including structured single-session models such as Comprehend, Cope, and Connect, which explicitly integrate formulation within an acute and crisis context. 7
The project also speaks to broader service-level efforts to improve access and responsiveness. Waitlist-management literature has highlighted the need to explore alternative pathways when demand exceeds capacity, rather than relying only on passive waiting. 9 Likewise, implementation work in mental health settings suggests that brief one-at-a-time or single-session models may support more rapid access when embedded thoughtfully into service systems. 6 In the Australian context, single-session work is well established in child, adolescent and family therapy settings 8 , but has been less commonly evaluated as a waitlist management strategy in adult community public health counselling. The present project seeks to address this gap.
These findings should be interpreted within the context of service-level implementation rather than clinical efficacy. The project reflects a pragmatic response to demand pressures, where the goal is not to replace standard therapy but to provide timely, meaningful intervention for selected patients. SST in this model functions as a complement to existing care pathways rather than a substitute.
Implications for service delivery
The findings suggest that SST may support improved access and responsiveness within counselling services experiencing high demand. Implementation requires consideration of workforce capacity, supervision arrangements, and training. Although routine placement supervision absorbed most of the supervisory load, the project required additional senior clinician time for the development of training materials, role plays, and ad hoc consultation. Services considering SST models should plan for these implementation costs and ensure appropriate governance, clinical oversight, clear escalation pathways for risk, and well-defined patient selection processes.
Limitations
Several limitations should be considered. This was a small local quality improvement evaluation with a single-group post-intervention design and no comparison group, randomisation, or longer-term follow-up. Feedback was obtained from only 5 of the 9 patients who completed SST, and the evaluation used a brief locally developed feedback process rather than validated outcome measures. Patients were not explicitly asked about aspects of the intervention that were unhelpful or that could be improved, which limits interpretation of the helpfulness ratings.
Allocation to SST was pragmatic rather than guided by predefined inclusion and exclusion criteria. While this reflected real-world implementation conditions, more clearly specified eligibility criteria would have strengthened the evaluation and supported clearer interpretation of feasibility findings. Future implementation work should define eligibility criteria a priori, for example, by symptom severity threshold, presenting concern, or risk profile.
The intervention was delivered by provisional psychologists who had not undertaken formal external SST training; internal training and supervision were provided by senior psychologists, only one of whom had completed formal external SST training. This reflects real-world service constraints but limits conclusions regarding intervention fidelity and broader implementation. Formal feedback was not obtained from the provisional psychologists themselves; future evaluations should include clinician-reported data on sufficiency of single contact, perceived complexity of allocated cases, and supervision needs.
Finally, the project was conducted in a single Australian community health counselling service, and findings may not generalise to other adult public health contexts. A larger, more methodologically rigorous evaluation, with prospectively defined eligibility criteria, validated outcome measures, longer-term follow-up, and capacity for clinician feedback, would be a logical next step.
Conclusion
This brief quality improvement evaluation suggests that SST may be a feasible and acceptable strategy within counselling waitlist management in an Australian community public health service. Patient feedback was positive overall, and most SST completers were able to be discharged without requiring further service input. Although preliminary and limited by small sample size, the findings support further service-level evaluation of SST as a brief intervention option in adult public health counselling contexts, an area where the Australian peer-reviewed literature remains comparatively under-developed.
Supplemental material
Suppplemental Material—Single-session therapy as a counselling waitlist management strategy in a public health service: A brief quality improvement evaluation
Suppplemental Material for Single-session therapy as a counselling waitlist management strategy in a public health service: A brief quality improvement evaluation by Aliz Ovlachi in Australasian Psychiatry
Footnotes
Acknowledgements
Sincere thanks are extended to the patients whose participation and feedback informed this project. The author also gratefully acknowledges the provisional psychologists who contributed to the delivery of the intervention, as well as colleagues whose practical and collegial support assisted the project. Appreciation is also extended for the clinical and operational support provided within Monash Health, which contributed to the successful development and completion of this quality assurance work.
Generative AI was used to assist with language editing and formatting. The author reviewed, revised and takes full responsibility for all content.
Ethical considerations
This project was conducted as a Quality Improvement (QI) activity within routine service delivery at Monash Health and was reviewed and approved as negligible-risk Quality Assurance by the Monash Health Research Office (ERM Ref:127303).
Consent to participate
The project used de-identified service data and patient feedback collected as part of usual care. No additional data collection beyond routine service processes was undertaken. Verbal consent for follow-up contact was obtained from patients during the SST session and documented in the electronic medical record.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this quality improvement project are not publicly available due to their containing information that could compromise patient privacy. De-identified summary data are presented in the manuscript.
Additional information
This quality improvement project was conducted within Monash Health and is independent of the author’s doctoral research program at Federation University Australia.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.