
Abstract
Objective
To evaluate changes in mental health symptoms, wellbeing, recovery, and emotion regulation among young people receiving care in a recovery-oriented inpatient unit and day programme.
Methods
This is a prospective observational longitudinal cohort study of young adults aged 16–25 years assessed at baseline, 3 months, and 6 months. Measures included the Depression Anxiety Stress Scales–21 item version, Difficulties in Emotion Regulation Scale, Interpersonal Emotion Regulation Questionnaire, Recovery Assessment Scale–20 item version, and WHO-5 Wellbeing Index. Lifestyle and psychosocial factors were assessed.
Results
Seventy participants were enrolled; 71.4% were female and 52.9% aged 17–19 years. Significant reductions in depressive symptoms were observed, with DASS-21 Depression scores decreasing from 26.3 at baseline to 20.5 at 6 months (p = .04). Emotion regulation difficulties improved significantly, with DERS-16 scores decreasing from 58.9 to 53.5 (p = .02). Recovery scores and wellbeing showed positive but non-significant trends. Positive changes were observed in outdoor activity, physical activity, diet quality, and perceived social support.
Conclusions
This study provides preliminary evidence that a tailored, recovery-oriented inpatient and day programme model is associated with reduced depressive symptoms and improved emotion regulation among young adults with mental health concerns. These findings support further evaluation of youth-specific, recovery-oriented mental health services.
Keywords
Mental health disorders among adolescents and young adults are increasing in prevalence both in Australia and internationally, with emerging evidence suggesting further exacerbation following the COVID-19 pandemic.1,2 This age group represents a critical developmental period characterised by ongoing neurobiological, psychological, and social change, during which the onset or exacerbation of mental illness can have enduring impacts on functioning, identity formation, and life trajectory. Despite the growing burden of mental health concerns among young people, there remains a relative paucity of developmentally appropriate inpatient and intensive day-treatment services specifically designed for individuals aged 16–25 years.
Young people with mental health concerns have distinct developmental and psychosocial needs that differ from those of both younger adolescents and older adults. Evidence suggests that youth-specific mental health services that cohort young people with peers and are grounded in recovery-oriented principles are more likely to promote engagement, autonomy, and sustained wellbeing. 3 However, much of the existing literature on recovery-oriented mental health care has focused on adult community settings, with limited empirical evaluation of inpatient or combined inpatient–day programme models tailored specifically to young adults. 4
Recovery-oriented practice conceptualises recovery as a personal and holistic process involving hope, identity, meaning, and empowerment, rather than symptom reduction alone. 5 Within youth mental health, recovery frameworks emphasise the importance of skill development, social connection, and participation in meaningful activities alongside clinical treatment. Emotion regulation has been identified as a key mechanism underpinning recovery and functional improvement in young people experiencing mental illness, particularly given its association with mood disorders, anxiety, and interpersonal functioning.6,7
The Amanda Flynn Clinic is a private, recovery-focused mental health service located within the Mater Young Adult Health Centre in Brisbane, Queensland. The service comprises a 12-bed inpatient ward and an associated outpatient day programme known as the Recovery College. Established in 2019, the Unit delivers multidisciplinary, developmentally appropriate care for young people aged 16–25 years experiencing significant mental health concerns. There is limited published evidence describing outcomes from private youth-specific inpatient services in Australia. Evaluating outcomes from this model of care is therefore important to inform service development and contribute to the emerging evidence base for youth-focused recovery-oriented mental health services.
This observational longitudinal cohort study aimed to evaluate changes in mental health symptoms, wellbeing, recovery, and emotion regulation among young people admitted to the Amanda Flynn Clinic inpatient service and/or attending the Recovery College day programme. Secondary aims were to explore behavioural and psychosocial factors associated with recovery, including sleep, physical activity, diet, social engagement, and perceived social support.
Methods
This study employed a prospective observational longitudinal cohort design.
Setting and participants
Participants were recruited from the Amanda Flynn Clinic inpatient service and the Recovery College day programme at the Mater Young Adult Health Centre, Brisbane. There was no randomisation, and all participants received usual clinical care consistent with the Centre’s recovery-focused multidisciplinary model. All new admissions to the service were eligible to participate, provided they were aged between 16 and 25 years, able to communicate in English, and able to provide informed consent, including assessment of Gillick competence where applicable. Written informed consent was obtained from all participants prior to participation. Participants who were unable to commit to follow-up or did not have access to an internet-enabled device were excluded.
Procedure
Participants completed assessments at baseline, defined as admission to the inpatient ward or commencement of the day programme, and were followed up at 3 months and 6 months post-baseline. A total of 70 participants were included in demographic and diagnostic analyses. Of these, 48 attended the Amanda Flynn Clinic inpatient service, 12 attended the Recovery College day programme, and 10 engaged in both services. Baseline survey data were available for 52 participants, with 38 completing the three-month follow-up and 41 completing the six-month follow-up.
Measures
The primary outcome was negative emotional states measured using the Depression Anxiety Stress Scales–21 item version (DASS-21). 8 Secondary outcomes included the Difficulties in Emotion Regulation Scale (DERS-16), 9 the Interpersonal Emotion Regulation Questionnaire (IERQ), 10 the Recovery Assessment Scale–20 item version (RAS-20),11,12 and the WHO-5 Wellbeing Index. 13 Additional self-report measures assessed lifestyle and psychosocial factors including sleep adequacy, time spent outdoors, physical activity, diet quality, family meal frequency, social participation, digital technology impact on sleep, group membership, and perceived support from friends. Clinical diagnoses were obtained from hospital records.
Statistical analysis
Descriptive statistics were calculated using frequencies and percentages for categorical variables and means for continuous variables. Changes over time were examined using repeated-measures ANOVA. Statistical significance was set at p < .05. Ethics approval was obtained from the Mater Misericordiae Ltd Human Research Ethics Committee (HREC/MML/76981).
Results
Participant characteristics
Demographic characteristics of participants by clinic
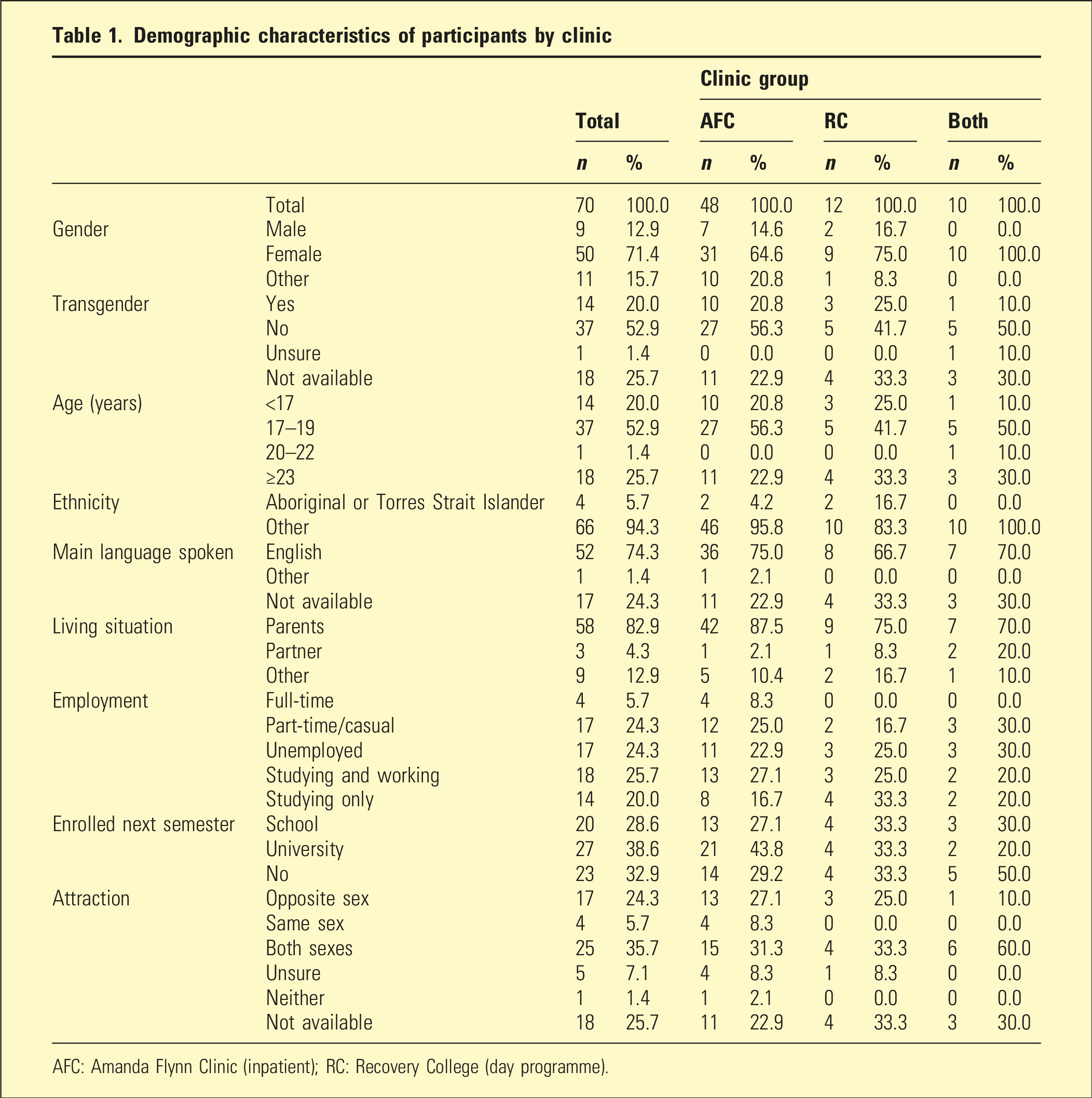
AFC: Amanda Flynn Clinic (inpatient); RC: Recovery College (day programme).
Diagnoses
Cohort diagnoses
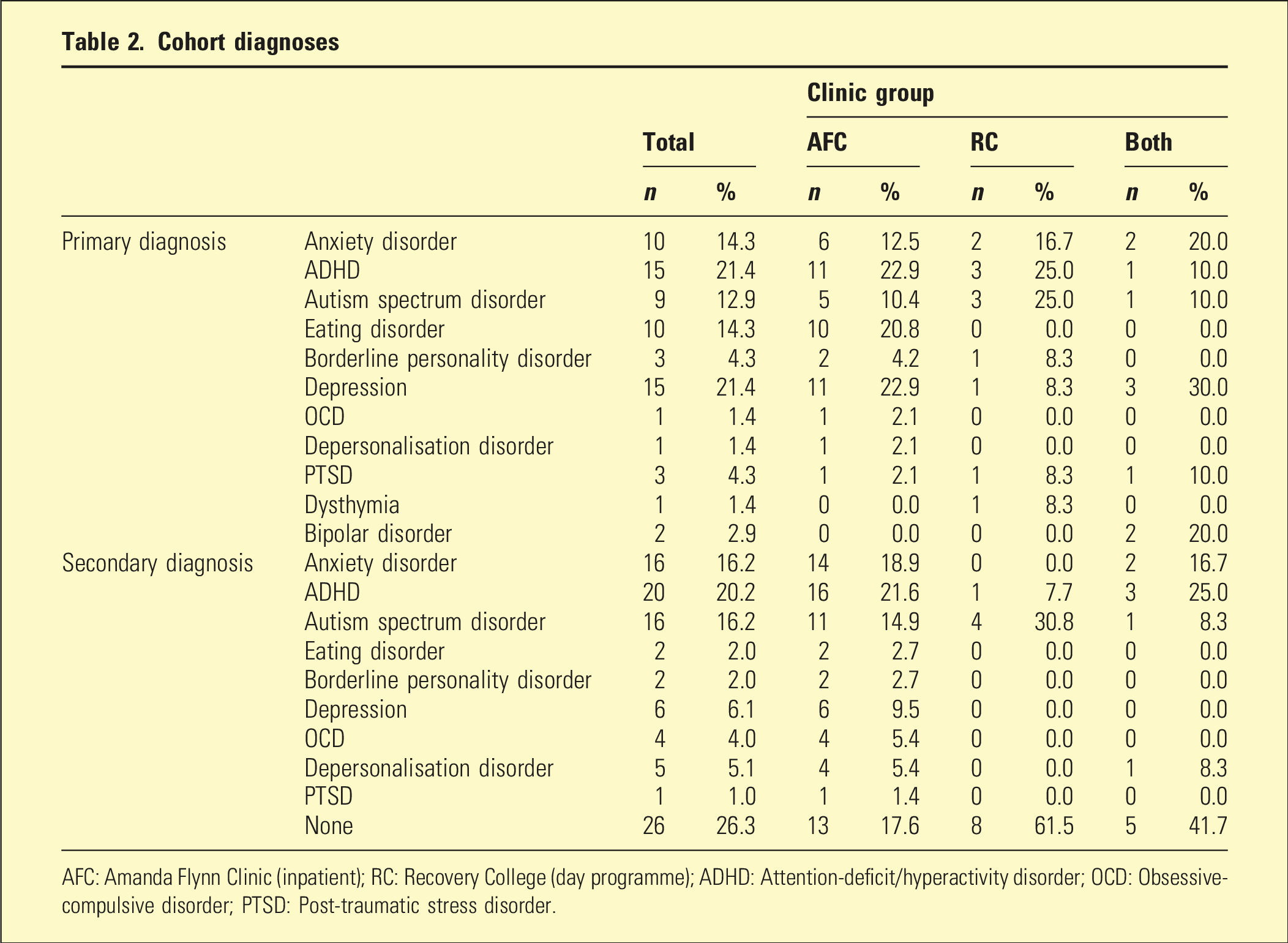
AFC: Amanda Flynn Clinic (inpatient); RC: Recovery College (day programme); ADHD: Attention-deficit/hyperactivity disorder; OCD: Obsessive-compulsive disorder; PTSD: Post-traumatic stress disorder.
Outcome measures
Survey outcome scores at baseline, 3 months, and 6 months
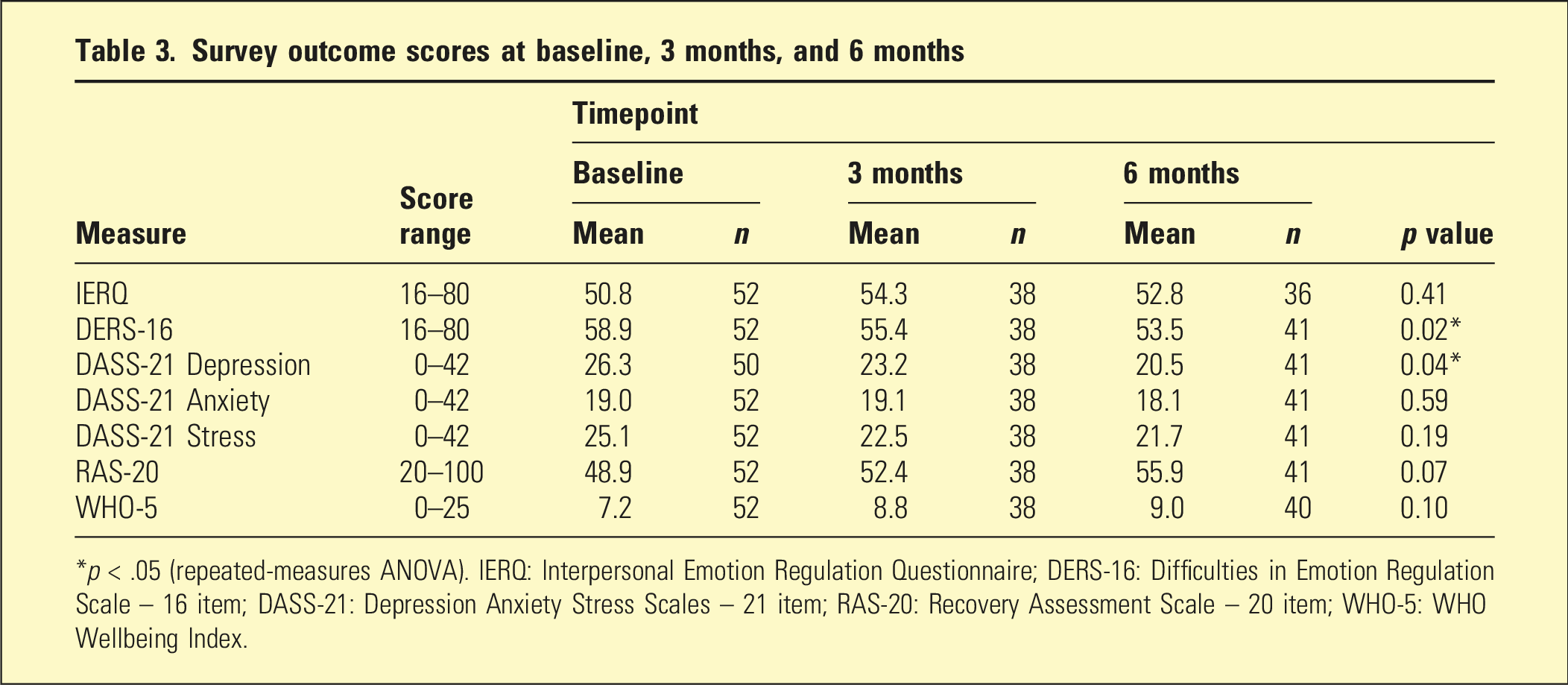
*p < .05 (repeated-measures ANOVA). IERQ: Interpersonal Emotion Regulation Questionnaire; DERS-16: Difficulties in Emotion Regulation Scale – 16 item; DASS-21: Depression Anxiety Stress Scales – 21 item; RAS-20: Recovery Assessment Scale – 20 item; WHO-5: WHO Wellbeing Index.
Mean recovery scores on the RAS-20 increased from 48.9 at baseline to 55.9 at 6 months, and mean WHO-5 wellbeing scores increased from 7.2 to 9.0 over the same period. Although these findings indicate improvements in perceived recovery and subjective wellbeing, the observed changes were not statistically significant.
Figure 1 shows the changes in outcome measures over time. Survey outcome scores at baseline, 3 months, and 6 months.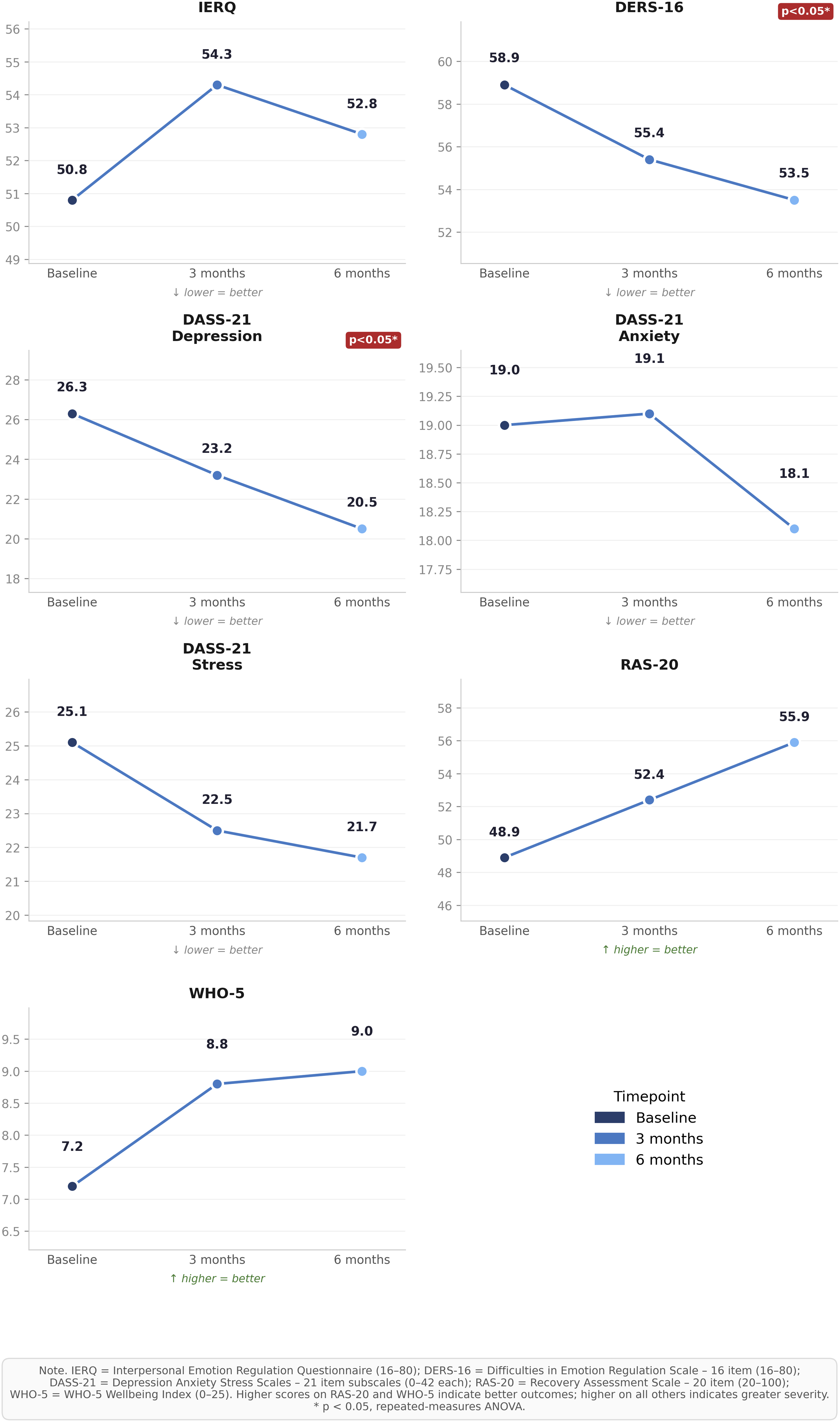
Lifestyle and behavioural measures
Positive trends were evident across lifestyle and behavioural measures over time. At baseline, 69.2% of participants reported spending less than 1 hour outdoors per week; this proportion decreased to 16.2% at 3 months and 19.5% at 6 months. The proportion reporting no days of at least 30 minutes of physical activity decreased from 36.5% at baseline to 18.4% at 3 months and 21.9% at 6 months. Self-rated diet quality improved at 3 months, with 65.8% rating their diet as good compared to 46.2% at baseline. Engagement in enjoyable activities increased over time. Perceived support from friends improved at 3 months, with 68.4% reporting adequate support compared to 53.9% at baseline, though this was less sustained at 6 months.
Discussion
This observational cohort study evaluated clinical, behavioural, and psychosocial outcomes among young adults receiving care in a private, recovery-oriented inpatient mental health unit and its associated outpatient Recovery College day programme. Over 6 months of follow-up, participants demonstrated significant improvements in depressive symptoms and emotion regulation, alongside positive trends in recovery and wellbeing scores and health-related behaviours. These findings provide preliminary evidence supporting the effectiveness of a developmentally tailored, recovery-focused inpatient and day programme model for young people experiencing significant mental health concerns.
This study contributes to a limited but growing evidence base examining youth-specific recovery-oriented mental health services, particularly within inpatient and combined inpatient–day programme contexts. A systematic review of adolescent and youth inpatient admissions demonstrated a general tendency toward improved outcomes across course of admission. 15 This is consistent with findings from Hayes et al., 16 who reported that most adolescents admitted to a private inpatient unit improved by discharge, with notable reductions in emotional symptoms and self-injury. Previous research has highlighted the challenges of implementing recovery-oriented practice within private inpatient settings. 4 The present findings suggest that such models can be associated with meaningful improvements when services are developmentally tailored and integrated across inpatient and outpatient care.
The observed reductions in depressive symptoms and improvements in emotional regulation are consistent with emerging evidence highlighting the central role of emotional regulation in youth mental health recovery. 17 Difficulties in emotion regulation are strongly associated with mood and anxiety disorders and are increasingly recognised as a key transdiagnostic mechanism underpinning psychological distress in young people.6,18 The significant improvements observed in DERS-16 scores suggest that the therapeutic components of the programme—likely including skill-based interventions, group therapy, and multidisciplinary input—may effectively target these underlying processes.
Improvements in recovery (RAS-20) and wellbeing (WHO-5) scores, although not statistically significant, are consistent with a recovery-oriented framework that extends beyond symptom reduction. Recovery-oriented mental health care conceptualises recovery as a multidimensional process encompassing hope, agency, social connection, and quality of life. 5 The Recovery Assessment Scale has demonstrated sensitivity to change in clinical populations. 19 Our findings do not allow firm conclusions to be drawn, but they may indicate meaningful trends toward improved personal recovery and subjective wellbeing among participants.
Positive changes in lifestyle and social behaviours, including increased outdoor activity, physical activity, engagement in enjoyable activities, and perceived social support, are consistent with broader evidence linking behavioural activation and social participation to improved mental health outcomes in young people. 3 These changes may reflect both direct effects of structured therapeutic programming and indirect effects of improved mental health and functioning. The Recovery College model, which emphasises skill-building, participation, and peer engagement, may be particularly well suited to supporting these broader psychosocial gains.
These findings should be interpreted within the broader context of known barriers to mental health service access among young people. Previous research indicates that a substantial proportion of young adults with mental health needs do not access care, often due to structural, financial, and attitudinal barriers. 20 Qualitative research in Australian contexts further highlights systemic challenges faced by young people, including fragmented care pathways, long wait times, limited service integration, and difficulties establishing therapeutic rapport. 21 The present findings suggest that youth-specific, recovery-oriented services may help address some of these barriers by enhancing engagement and perceived relevance of care, albeit within a private health service context.
Several limitations should be acknowledged. The study utilised an observational design without a control group, limiting causal inference. The sample size was relatively small, and attrition at follow-up may have introduced bias. Additionally, the cohort was drawn from a single private service, which may limit generalizability to public or more diverse populations. The predominance of female participants is consistent with patterns of help-seeking in youth mental health but may also limit applicability to male or gender-diverse populations. Future research employing controlled designs, larger samples, and longer follow-up periods is needed to further evaluate the effectiveness and scalability of this model.
Conclusions
This study provides preliminary evidence that a private, recovery-oriented inpatient and outpatient day programme model is associated with reductions in depressive symptoms, improvements in emotion regulation, and positive trends in recovery and wellbeing among young adults. These findings support the continued development and rigorous evaluation of youth-specific, recovery-oriented mental health services within contemporary mental health systems.
Footnotes
Ethical considerations
This study was approved by the Mater Misericordiae Ltd Human Research Ethics Committee (HREC/MML/76981).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Several authors receive research salary support through Mater Research, which is supported by the Mater Foundation. The Mater Foundation had no role in the design, conduct, analysis, interpretation, or reporting of this study.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors are employed by the organisation that operates the Amanda Flynn Clinic evaluated in this study. Their involvement in the service formed part of their usual salaried roles, and no author received any additional payment, bonus, consultancy fee, or other financial benefit in relation to the evaluation or publication of this work. The authors declare no other conflicts of interest.