
Abstract
Objective
To examine longitudinal changes in depressive symptoms during a 30-session course of repetitive transcranial magnetic stimulation (rTMS) in routine clinical practice, with particular attention to symptom change by mid-treatment.
Methods
In this single-center, naturalistic, retrospective observational study, 24 patients with unipolar depressive disorder diagnosed in routine clinical practice according to the International Classification of Diseases, 10th or 11th revision, were included. The primary outcome was change in 17-item Hamilton Depression Rating Scale (HAMD-17) total score at baseline, after 15 sessions, and after 30 sessions, analyzed using a linear mixed-effects model. Secondary analyses examined the 6-item Hamilton Depression Rating Scale (HAMD-6) and the insomnia 3-item score.
Results
HAMD-17 total scores decreased significantly over time. Estimated reductions from baseline were 8.58 points at mid-treatment and 12.99 points at end-of-treatment, corresponding to reductions of 37.9% and 57.4%, respectively. A further 4.41-point reduction was observed from mid-treatment to end-of-treatment. HAMD-6 also decreased significantly across treatment, whereas the insomnia 3-item score improved mainly between baseline and mid-treatment.
Conclusions
In this small real-world cohort, depressive symptom scores decreased during rTMS, with substantial reduction already evident by 15 sessions. Mid-treatment assessment may provide clinically useful information during treatment, although these findings should be interpreted as hypothesis-generating.
Introduction
Depression that does not improve sufficiently with antidepressant pharmacotherapy remains a major clinical challenge. Repetitive transcranial magnetic stimulation (rTMS) is an established treatment option for patients with depression who do not respond adequately to standard pharmacological approaches, and it is increasingly used in routine clinical practice. 1 In Japan, rTMS has been incorporated into clinical care under defined practice guidance and institutional eligibility frameworks, creating a need for real-world data on its clinical course and outcomes. 2
Although the antidepressant effects of rTMS have been examined in randomized and naturalistic studies, many reports have focused on overall change in total depression severity scores, response rates, and remission rates. These outcomes are important, but they do not fully address how symptoms evolve during the treatment course. In routine practice, this issue becomes especially relevant around the middle of a standard treatment course, when clinicians and patients often need to judge whether continuing treatment is reasonable. 3 Prior work has suggested that early symptom change during rTMS may help predict later response or non-response.4,5
The 17-item Hamilton Depression Rating Scale (HAMD-17) remains one of the most widely used clinician-rated measures of depressive symptom severity, but its factorial structure is not fully consistent across studies. Because of this psychometric heterogeneity, supplementary analyses based on previously established abbreviated components may be preferable to post hoc use of an internally defined domain structure.6,7 The 6-item Hamilton Depression Rating Scale (HAMD-6), consisting of depressed mood, guilt, work and activities, psychomotor retardation, psychic anxiety, and general somatic symptoms, was developed to capture core depressive symptoms and has shown favorable clinimetric properties. In comparative analyses, HAMD-6 has also been reported to be more sensitive to change than HAMD-17 in some treatment studies.8,9
In addition to core depressive symptoms, sleep disturbance is clinically relevant during rTMS treatment. The three insomnia items of the HAMD-17 directly assess initial, middle, and late insomnia and can be examined without relying on a broader and potentially unstable factor model. This approach allows a clinically interpretable assessment of whether sleep-related symptoms improve earlier than core depressive symptoms during treatment.
Thus, the present study was designed as a descriptive real-world repeated-measures study focusing on whether significant symptom change can already be detected by the midpoint of a standard 30-session rTMS course. Specifically, we examined longitudinal changes in HAMD-17 total score at baseline, mid-treatment, and end-of-treatment, and conducted secondary analyses of HAMD-6 and the HAMD-17 insomnia items. We additionally evaluated response and remission at the final available time point and performed sensitivity analyses to examine whether the overall temporal pattern differed according to antidepressant medication-change status during treatment.
Materials and methods
Study design and setting
This was a single-center, naturalistic, single-arm retrospective observational study conducted at Nagano Prefectural Mental Wellness Center Komagane, a regional psychiatric hospital in Nagano Prefecture, Japan. The analysis used routinely collected clinical data obtained in routine practice between July 2022 and January 2026. Diagnosis of unipolar depressive disorder was established in routine clinical practice according to the International Classification of Diseases, 10th or 11th revision (ICD-10/ICD-11).
During the study period, 31 patients requested rTMS treatment at our center. Of these, four patients were not treated because they did not meet the Japanese Society of Psychiatry and Neurology guidance criteria, and 3 withdrew consent before treatment initiation. The remaining 24 patients underwent an acute course of rTMS and were all included in the present analysis. Each participant contributed only one acute rTMS treatment course; repeated acute courses in the same patient were not included.
Patients were considered eligible for rTMS under the institutional framework based on Japanese clinical guidance. Eligible patients were adults aged 18 years or older with unipolar depressive disorder, a baseline HAMD-17 total score of 13 or higher as an operational threshold for clinically significant depressive symptom severity, and insufficient improvement despite treatment with at least one antidepressant at an adequate dose and duration. Patients with psychotic symptoms, bipolar depression, or other conditions outside the Japanese clinical indication for rTMS were not eligible. All patients underwent rTMS as part of routine clinical care and elected to receive the treatment after clinical explanation.
rTMS procedure
All patients were treated using a standard NeuroStar rTMS protocol. Stimulation was delivered to the left dorsolateral prefrontal cortex at 10 Hz, 120% of motor threshold, with 3000 pulses per session. Target localization was performed using the 5.5-cm method. Resting motor threshold was determined according to the standard NeuroStar procedure as the minimum stimulation intensity required to elicit visible movement of the right thumb at rest during stimulation of the motor cortex. Treatment was delivered five sessions per week on weekdays, with a planned total of 30 sessions. Symptom severity was assessed at three clinically defined time points: before treatment initiation (baseline), after 15 sessions (mid-treatment), and after 30 sessions (end-of-treatment). Patients who did not complete the full course contributed data up to their final available assessment.
Clinical measures
Depressive symptom severity was assessed using the 17-item Hamilton Depression Rating Scale (HAMD-17), rated by the attending psychiatrist. The primary outcome was longitudinal change in HAMD-17 total score across the three time points.
Secondary analyses examined two clinically interpretable symptom groupings derived from prior literature. First, we analyzed the 6-item Hamilton Depression Rating Scale (HAMD-6), which was designed to capture core depressive symptom severity and has been reported to show favorable clinimetric properties and sensitivity to change. The HAMD-6 consisted of depressed mood, guilt, work and activities, psychomotor retardation, psychic anxiety, and general somatic symptoms.8,9 Second, we analyzed the three insomnia items of the HAMD-17, namely initial insomnia, middle insomnia, and late insomnia, as a clinically straightforward measure of sleep-related symptom change during treatment. HAMD-6 and the insomnia 3-item score were not used as eligibility criteria.
Item-level analyses of the 17 HAMD items were conducted as supplementary exploratory analyses only. Response was defined as a reduction of at least 50% in HAMD-17 total score relative to baseline. Remission was defined as a HAMD-17 total score of 7 or less at the final available time point.10,11
Concomitant treatment and additional clinical variables
Pharmacotherapy at treatment initiation was generally maintained during the rTMS course, but antidepressant medication changes were permitted when clinically indicated, such as for insufficient response, adverse effects, or other clinical necessity. Antidepressant medication-change status, type of change, and timing relative to the mid-treatment assessment were recorded. We also recorded history of electroconvulsive therapy (ECT), number of completed rTMS sessions, treatment completion status, reasons for discontinuation, adverse events, and the number of prior antidepressant trials.
Statistical analysis
Descriptive statistics were calculated for baseline demographic and clinical characteristics. Continuous variables are presented as means and standard deviations, and categorical variables as counts and percentages. Raw descriptive statistics by time point were also calculated for HAMD-17 total score, HAMD-6, and the insomnia 3-item score.
Response and remission rates were summarized at the final available HAMD-17 assessment. Response was defined as a reduction of at least 50% in HAMD-17 total score relative to baseline, and remission was defined as a final available HAMD-17 total score of 7 or less. When end-of-treatment data were unavailable, the mid-treatment assessment was used as the final available time point. Corresponding rates among patients who completed the planned 30-session course were also calculated descriptively.
Longitudinal changes in HAMD-17 total score were analyzed using a linear mixed-effects model with time point (baseline, mid-treatment, and end-of-treatment) as a fixed effect and participant as a random intercept. Models were fitted by maximum likelihood, and degrees of freedom were estimated using Satterthwaite’s method. Estimated marginal means with 95% confidence intervals were calculated for each time point, and pairwise comparisons between time points were performed with Bonferroni adjustment. All available repeated observations were included in the likelihood-based analyses; therefore, patients without end-of-treatment data contributed baseline and mid-treatment observations. No imputation was performed. Because treatment discontinuation was related to clinical status in some cases, missingness may not have been completely at random, and this was considered when interpreting the results.
The same modeling strategy was applied to HAMD-6 and the insomnia 3-item score as secondary analyses. Item-level analyses of the 17 HAMD items were conducted as supplementary exploratory analyses only, and false discovery rate correction was applied to item-level p values.
Sensitivity analyses were performed in two ways. First, the primary model was repeated in the subgroup without antidepressant medication changes during treatment. Second, an interaction model including time point, antidepressant medication-change status, and their interaction was fitted to examine whether the temporal pattern of change differed according to medication-change status. Descriptive trajectories stratified by antidepressant medication-change status were also summarized.
Percentage reductions from baseline were calculated using estimated marginal means. Standardized response means were calculated as supplementary effect-size indices.
All analyses were conducted using R ver. 4.5.2. Statistical significance was set at a two-sided p value of less than 0.05.
Ethics statements
This study was approved by the institutional review board (approval number: No.2025-7). As this was a retrospective observational study using routinely collected clinical data, information about the study was made available to patients, and they were given the opportunity to decline participation through an opt-out procedure, in accordance with local regulations and ethics committee requirements.
Results
Participant characteristics
During the study period, 31 patients requested rTMS treatment. Four patients were not treated because they did not meet the Japanese Society of Psychiatry and Neurology guidance criteria, and 3 withdrew consent before treatment initiation. The remaining 24 patients underwent an acute rTMS course and were all included in the analysis. No patient was represented more than once in the dataset.
Demographic, clinical, and treatment course characteristics.
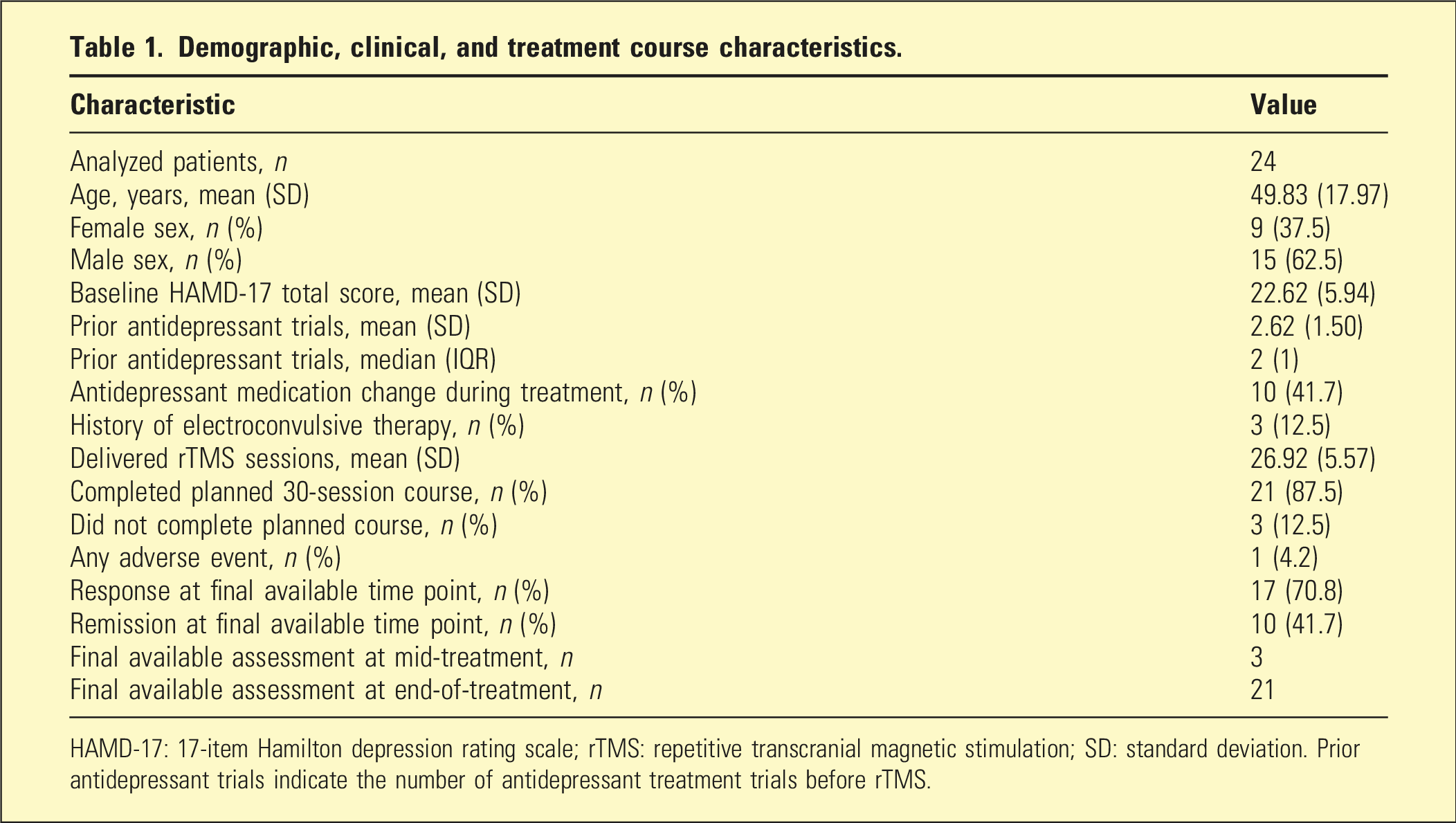
HAMD-17: 17-item Hamilton depression rating scale; rTMS: repetitive transcranial magnetic stimulation; SD: standard deviation. Prior antidepressant trials indicate the number of antidepressant treatment trials before rTMS.
The numbers of evaluable patients were 24 at baseline, 24 at mid-treatment, and 21 at end-of-treatment. A participant flow summary is shown in Supplemental Figure 2.
Longitudinal change in HAMD-17 total score
Estimated mean scores, overall effect of time, and pairwise comparisons.
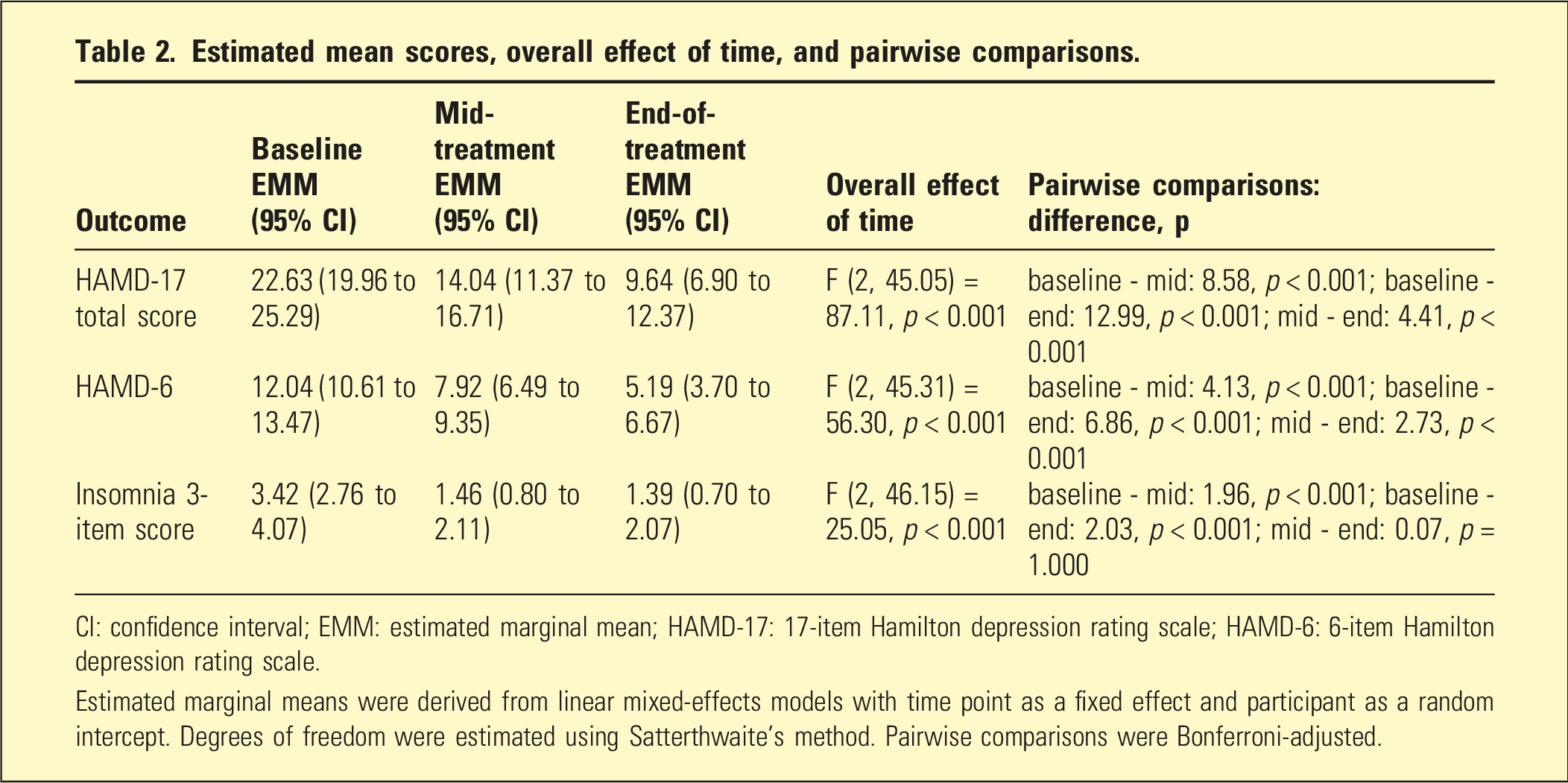
CI: confidence interval; EMM: estimated marginal mean; HAMD-17: 17-item Hamilton depression rating scale; HAMD-6: 6-item Hamilton depression rating scale.
Estimated marginal means were derived from linear mixed-effects models with time point as a fixed effect and participant as a random intercept. Degrees of freedom were estimated using Satterthwaite’s method. Pairwise comparisons were Bonferroni-adjusted.
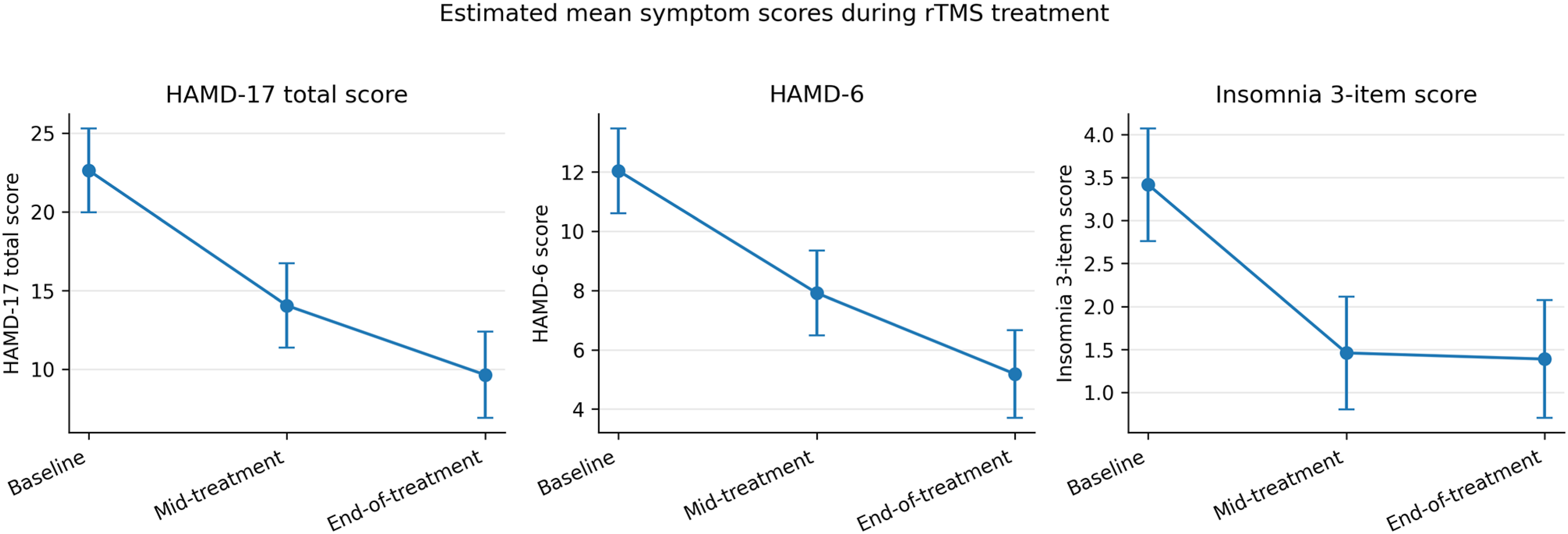
Estimated mean HAMD-17 total score, HAMD-6, and insomnia 3-item score during the rTMS treatment course. Points indicate estimated marginal means and error bars indicate 95% confidence intervals from linear mixed-effects models. HAMD-17: 17-item Hamilton depression rating scale; HAMD-6: 6-item Hamilton depression rating scale; rTMS: repetitive transcranial magnetic stimulation.
Secondary analyses: HAMD-6 and insomnia
HAMD-6 scores also decreased significantly over time. The overall effect of time point was significant, F(2, 45.31) = 56.30, p < 0.001. Estimated mean HAMD-6 score was 12.04 at baseline, 7.92 at mid-treatment, and 5.19 at end-of-treatment. Pairwise comparisons showed significant reductions from baseline to mid-treatment, from baseline to end-of-treatment, and from mid-treatment to end-of-treatment, indicating continued reduction in core depressive symptom scores during the later phase of treatment.
The insomnia 3-item score also improved significantly over time. The overall effect of time point was significant, F(2, 46.15) = 25.05, p < 0.001. Estimated mean values were 3.42 at baseline, 1.46 at mid-treatment, and 1.39 at end-of-treatment. Pairwise comparisons showed significant reductions from baseline to mid-treatment and from baseline to end-of-treatment, whereas the difference between mid-treatment and end-of-treatment was minimal and not significant (p = 1.000). These findings indicate that insomnia-related symptom scores improved mainly during the earlier phase of treatment. Detailed results for HAMD-17 total score, HAMD-6, and the insomnia 3-item score are summarized in Table 2 and illustrated in Figure 1. Raw descriptive statistics by time point are provided in Supplemental Table 1.
Response and remission
At the final available time point, 17 of 24 patients (70.8%) met the response criterion and 10 of 24 (41.7%) met the remission criterion. Because 3 patients did not complete the full 30-session course, these proportions were calculated using the final available HAMD-17 score. Among the 21 patients who completed the planned 30-session course, 16 (76.2%) met the response criterion and 9 (42.9%) met the remission criterion. The completer-based proportions were therefore similar to those obtained using the final available time point.
Sensitivity and exploratory analyses
In the subgroup without antidepressant medication changes, HAMD-17 total scores also decreased significantly over time, F(2, 27.16) = 57.95, p < 0.001. In the interaction model including time point and antidepressant medication-change status, the main effect of time point remained significant, whereas the time point-by-medication-change interaction was not statistically significant, F(2, 45.34) = 0.94, p = 0.400. Because antidepressant medication changes were not randomized and differed in type and timing, this null interaction should be interpreted cautiously. Descriptive trajectories stratified by antidepressant medication-change status are provided in Supplemental Table 3.
Exploratory item-level analyses are presented in Supplemental Table 4. In these analyses, most individual HAMD-17 item changes were observed between baseline and mid-treatment, whereas no individual item showed significant additional change from mid-treatment to end-of-treatment after false discovery rate correction. Individual trajectories of HAMD-17 total score are shown in Supplemental Figure 1.
Discussion
In this naturalistic study of patients with unipolar depressive disorder meeting Japanese clinical eligibility criteria for rTMS, depressive symptom scores decreased over the course of a standard 30-session treatment. A marked reduction was already evident at the mid-course assessment after 15 sessions and was followed by further reduction by the end of treatment. At the final available time point, approximately 71% of patients met the response criterion and 42% met the remission criterion. Because this was a single-arm observational study, these findings should be interpreted as descriptive evidence of symptom trajectories during routine rTMS rather than as evidence of causal treatment efficacy.
One clinically relevant finding was that substantial symptom reduction was already detectable at the mid-course assessment. In routine practice, clinicians often face the question of whether improvement should be expected by the middle of the treatment course and whether continuation is justified when early changes are modest. Our findings indicate that, in this cohort, a large proportion of HAMD-17 total-score reduction occurred within the first 15 sessions, while additional reduction in HAMD-17 total score and HAMD-6 was observed through treatment completion.4,5 However, this pattern should be interpreted alongside the exploratory item-level findings, which suggested that many individual symptom changes were front-loaded.
Our results should be interpreted in the context of prior Japanese real-world data. In a recent multisite observational study, HAMD-17 scores improved from 18.9 to 9.7, with response and remission rates of 53.5% and 42.8%, respectively. 3 In our cohort, baseline HAMD-17 severity was somewhat higher, whereas the final estimated mean score was similar. Response rates were numerically higher in our sample, while remission rates were broadly comparable. Direct comparison is limited by differences in sample size, clinical characteristics, and study design, but the overall pattern of improvement was generally consistent with that previous Japanese real-world report.
Secondary analyses suggested that symptom change was not entirely uniform across clinically relevant measures. HAMD-6, reflecting core depressive symptoms, decreased significantly not only from baseline to mid-treatment but also from mid-treatment to end-of-treatment. By contrast, the insomnia 3-item score improved mainly during the first half of treatment, with little additional change thereafter. Exploratory item-level analyses provided further nuance: most individual HAMD-17 items improved between baseline and mid-treatment, whereas no individual item showed significant additional improvement from mid-treatment to end-of-treatment after false discovery rate correction.
These findings suggest a predominantly front-loaded pattern of symptom change at the item level, even though total and HAMD-6 scores continued to decrease from mid-treatment to end-of-treatment. Because the HAMD-17 includes insomnia and other somatic items, early improvement in these components may contribute to the apparent magnitude of early total-score reduction. In contrast, HAMD-6 may provide a more focused index of core depressive symptoms. Nevertheless, these secondary and item-level findings remain exploratory and should not be interpreted as evidence for distinct mechanistic response profiles. Improvement in sleep-related symptoms during TMS treatment has also been reported in prior naturalistic data. 12
We selected HAMD-6 and the insomnia items as supplementary measures because the factorial structure of the HAMD-17 is not fully consistent across studies, whereas HAMD-6 has been proposed as a concise measure of core depressive symptoms with favorable clinimetric properties and sensitivity to change.7–9 These secondary analyses were therefore intended to provide clinically interpretable complementary information rather than to establish a novel symptom-domain structure.
Medication changes during treatment are an important potential confounder in this naturalistic cohort. Antidepressant medication changes occurred in 10 patients and consisted mainly of dose increases, with most changes occurring before the mid-treatment assessment. In sensitivity analyses, HAMD-17 total scores decreased significantly in the subgroup without antidepressant medication changes, and the time point-by-medication-change interaction was not statistically significant. However, this null interaction should be interpreted cautiously because medication changes were clinically determined, not randomized, and were coded using limited categories. Patients who required medication changes may also have represented a clinically more severe or less stable subgroup.
Several limitations should be considered. First, this was a single-arm naturalistic study without a control condition, and therefore the observed improvement cannot be interpreted as evidence of causal treatment efficacy. Second, the sample size was small, which limited statistical precision and the stability of subgroup and supplementary analyses. Confidence intervals and subgroup results should therefore be interpreted cautiously, and the findings should be regarded as hypothesis-generating rather than confirmatory. Third, clinical characterization was limited by the retrospective design. Although the number of prior antidepressant trials was available, information on illness duration, current episode duration, psychiatric comorbidities, and formal treatment-resistance staging was not consistently available in the records and could not be uniformly analyzed. Fourth, antidepressant medication changes were permitted when clinically indicated. Although sensitivity analyses were conducted, medication change was not randomized and was heterogeneous in type and timing; residual confounding by medication adjustment, illness severity, and clinical instability therefore remains possible. Fifth, three patients did not complete the full 30-session course, and response/remission estimates were therefore based on the final available assessment rather than a uniform endpoint for all participants. Because treatment discontinuation was related to clinical status in some cases, missingness may not have been completely at random. However, response and remission rates calculated among completers were broadly similar to those based on the final available time point, which partially reduces concern that this analytic choice materially distorted the overall clinical interpretation. Sixth, although HAMD-6 and the insomnia items were selected on the basis of prior literature and clinical interpretability, these secondary analyses remain supplementary and should not be overinterpreted as evidence for distinct mechanistic response profiles. Finally, depressive symptoms were rated by the attending psychiatrist in routine clinical practice, and ratings were therefore not blinded to treatment status. In addition, target localization was performed using the 5.5-cm method rather than individualized targeting; therefore, anatomical variability of the stimulated site cannot be excluded.13,14
Despite these limitations, the present study has several strengths. All patients were treated using a standardized NeuroStar protocol under a consistent institutional treatment framework, and depressive symptoms were repeatedly assessed at clinically meaningful time points. This allowed us to describe symptom trajectories across baseline, mid-treatment, and end-of-treatment rather than relying only on a simple pre-post comparison. The inclusion of HAMD-6, insomnia items, and exploratory item-level analyses also provided complementary information on how different symptom measures changed during the treatment course, although these findings remain exploratory.
In conclusion, in this small naturalistic cohort, depressive symptom scores decreased over the course of a standard 30-session rTMS treatment, with substantial reduction already observable by 15 sessions. Secondary analyses suggested continued reduction in HAMD-6 scores through treatment completion, whereas insomnia-related symptom scores improved mainly earlier in the course of treatment. These findings support the potential clinical usefulness of repeated symptom assessment during rTMS treatment, but should be interpreted as hypothesis-generating given the small sample size, single-arm design, and naturalistic treatment context.
Supplemental material
Supplemental Material - Depressive symptom trajectories during a 30-session course of repetitive transcranial magnetic stimulation in routine clinical practice: A single-center naturalistic study
Supplemental Material for Depressive symptom trajectories during a 30-session course of repetitive transcranial magnetic stimulation in routine clinical practice: A single-center naturalistic study by Masahiro Uzawa in Australasian Psychiatry
Footnotes
Acknowledgments
The author has no acknowledgements to declare.
Ethical considerations
The study protocol was approved by the institutional ethics committee of Nagano Prefectural Mental Wellness Center Komagane (approval number: No.2025-7). As this was a retrospective observational study using routinely collected clinical data, information about the study was made available to patients, and they were given the opportunity to decline participation through an opt-out procedure, in accordance with local regulations and ethics committee requirements.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to privacy and ethical restrictions related to patient data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.