
Abstract
Objectives
This study aimed to explore the associations of pain status with long-term depressive symptoms, cognition, and the trajectories of both.
Methods
A total of 10,683 and 4644 individuals were included in this study. The generalized estimation equation and multinomial logistic regression was applied to explore the association of pain status with long-term depressive symptoms, cognition, and the trajectories of them.
Results
Compared to individuals without pain, those with pain were positively related to depressive symptoms (adjusted β = 0.479, 95% CI: 0.449, 0.508), and were negatively related to cognitive function (adjusted β = −0.166, 95%CI: −0.212, −0.119). Both four depressive and cognitive trajectories were identified. Participants with pain were associated with significantly increased risk of moderate-stable (Traj 2, OR = 2.78, 95% CI 2.49-3.09), extra-stable (Traj 3, OR = 6.14, 95% CI 5.36-7.03) and high-stable depressive symptoms trajectory (Traj 4, OR = 12.55, 95% CI 9.70-16.24). Participants with pain were also associated with significantly decreased risk of moderate-stable (Traj 2, OR = 0.71, 95% CI 0.50-0.99), extra-stable (Traj 3, OR = 0.52, 95% CI 0.36-0.74) and high-stable (Traj 4, OR = 0.35, 95% CI 0.22-0.55) cognition trajectory.
Conclusion
Individuals with pain were more likely to suffer more depressive symptoms, and were associated with lower scores for cognition function.
Keywords
Chronic pain, defined as pain lasting over 3 months, is a complex and heterogeneous condition, 1 and has been linked to restrictions in mobility and daily activities, dependence on opioids, anxiety and depression, and poor perceived health or reduced quality of life.2–4 It was estimated that about 30% of people suffer from chronic pain globally,5,6 and data from the Global burden of disease (GBD) study 2019 indicated that the global burden of chronic pain increased significantly from 1990 to 2019, with projections indicating a continued rise in headache burden over the next 15 years. 7 Now, chronic pain is recognized as a separate disease entity rather than a concomitant symptom of the underlying disease, which will bring more challenges to global human health, under condition of the increasing life expectancy and growing aging population. 8
With the progression of population aging, the aging of the population has led to a high prevalence of chronic diseases such as depressive symptoms, cognitive function impairment and dementia.9–11 It was estimated that over 300 million people suffered from depression, and depressive disorders were ranked as the largest contributor to non-fatal health loss (7.5% of all global Years Lived with Disability). 12 It was estimated that approximately 15.6% of individuals aged 50 years or older have mild cognitive impairment, and more than 55 million people worldwide suffer from dementia currently, over 60% of whom live in low- and middle-income countries.13,14 An emerging number of studies had reported the association of pain with depression and cognitive impairment. Evidence from the cross-sectional, longitudinal and meta-analysis studies had reported that chronic pain (single-site, multisite; across distinct body sites) was related to higher risk of depression.15–17 Furthermore, numerous studies also had found chronic pain has a major effect on cognitive functions, encompassing processing and psychomotor speed, memory and learning, attention, and executive functions.18–20 Taking together, all those findings had proved the significant associations between chronic pain with depression and cognitive function. Actually, both depressive symptoms and cognitive function are not static. All of them are dynamic, time-varying indicator.21,22 However, whether the chronic pain affect the long-term trend of individuals’ depressive symptoms and cognitive function in middle-aged and elderly adults are still unknown.
Therefore, in current study, we used a large, multinational cohorts derived from the China Health and Retirement Longitudinal Study (CHARLS) to explore the associations of chronic pain status with long-term depressive symptoms and cognitive function, and the relationship between chronic pain status and the trajectories of depressive symptoms and cognition function.
Methods
Study population
The CHARLS is an ongoing nationally representative and population-based study, that uses a multistage clustering sample method to select participants and conducted to collect a series of data regarding demographics, economic status, social networks, physical and psychological health in China. 23 The first visit was accomplished in 2011-2012 (Wave 1) of 17,708 patients, subsequently third follow-up visits carried out after that, each nearly 2 years apart among survivors (2013–2014: Wave 2, 2015–2016: Wave 3;2017–2018: Wave 4; 2019-2020: Wave 5). The ethics application for collecting data on human subjects in CHARLS was approved by the Biomedical Ethics Review Committee of Peking University (IRB00001052-11,015), and all CHARLS participants provided written informed consent. The details of the CHARLS data are available at its website (https://charls.pku.edu.cn/en).
In current study, we conducted a longitudinal analysis using data from the four waves of CHARLS (Wave 1 to Wave 4, from 2011 to 2018). We included participants according to the following criteria
1
: individuals ≥45 years old,
2
individuals with complete information about chronic pain in 2011
3
individuals who were successfully followed-up, and with complete four-times information about depressive symptoms and cognition. Finally, a total of 10,683 and 5351 individuals were eligible for subsequent analysis (Figure 1). Flowchart for selecting study participants in this study.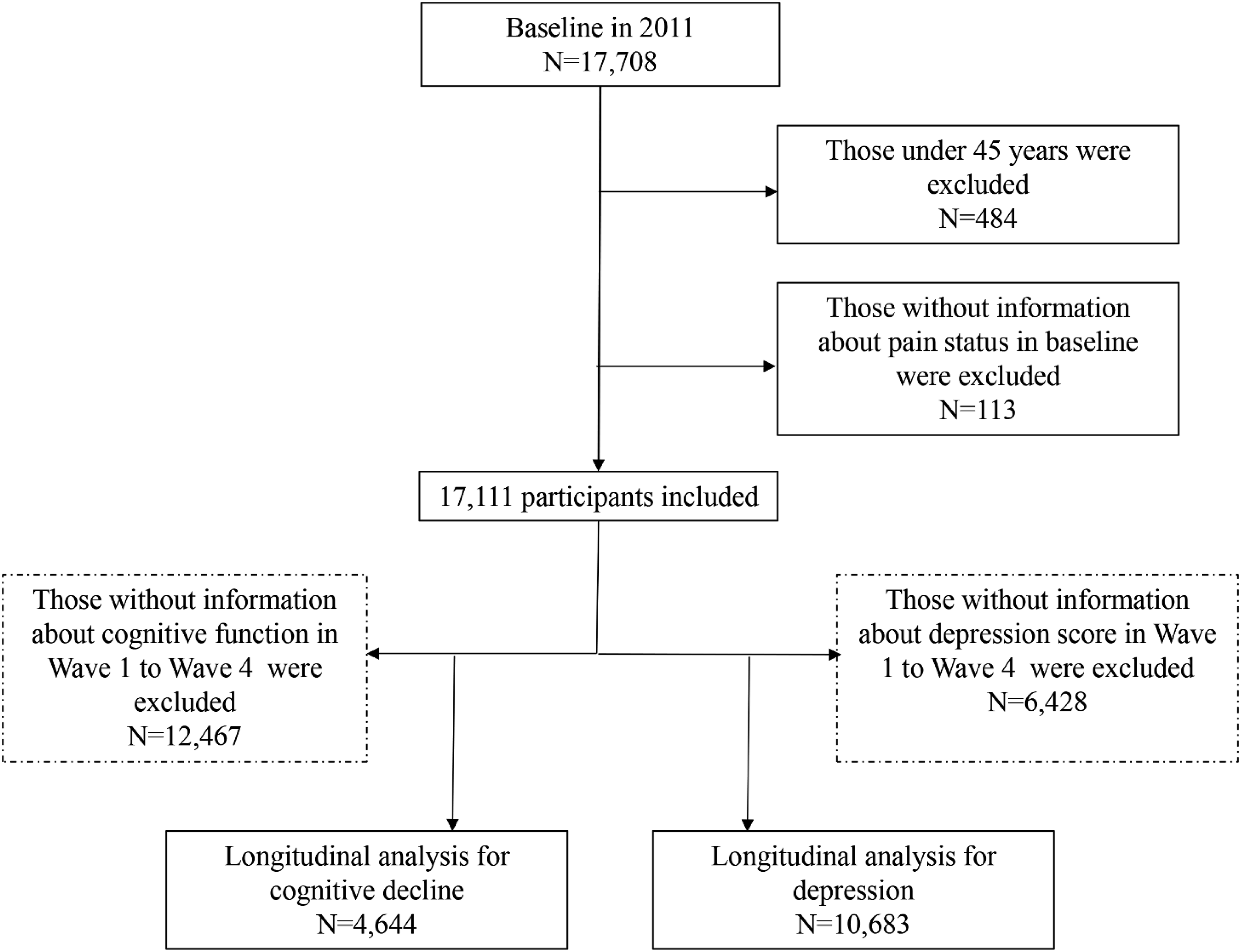
Assessment of pain characteristics
Pain characteristics in CHARLS were assessed based on the following self-reported questions: “Are you often troubled with anybody pains (‘no’ or ‘yes’)? On what part of your body do you feel pain? Please list all parts of your body where you are currently feeling pain (head, neck, chest, stomach, shoulder, back, waist, buttocks, arm, leg, knees, wrist, fingers, ankle, toes). 24 ” According to the pain characteristics assessment report, we divided the pain status into no pain and pain. In addition, we calculated the total pain score according to the score for each site (score 1 for each site with the total score range 0 to 15), and divided the pain distribution into no pain, single-site pain, and more than one site of pain (multisite pain).
Depressive symptoms and cognitive function assessment
The CES-D was administrated to measure depressive symptoms at baseline and each follow-up visit of the CHARLS (25), which has been proved to be a reliable and valid approach to detect depressive symptoms in Chinese adults.25,26 The CES-D short form consists of 10 items assessing the frequency of symptoms or behaviors experienced during the past week: I was bothered by little things/had trouble concentrating/felt depressed/felt everything I did was an effort/felt hopeful about the future/felt fearful/my sleep was restless/was happy/felt lonely/could not get going. Each item scores 0 (rarely or none of the time) to 3 points (most or all of the time), with the highest score indicating the greatest symptom burden. The total CES-D score ranges from 0 to 30 (positive items were reverse coded), with higher scores representing greater severity of depressive symptoms. 27 Cognitive function was measured using questionnaires that were adapted from the Telephone Interview for Cognitive Status. 28 According to the recommendations by the Health and Retirement Study and CHARLS, 29 2 dimensions of cognitive function were captured: episodic memory and executive function. Episodic memory was measured by immediate recall and delayed recall (score range, 0–10 points, with higher scores indicating better function). Executive function was evaluated by orientation, calculation, and visuospatial ability (score range, 0–11 points, with higher scores indicating better function). Global cognition was defined as the total score of these 2 components with a scale ranging from 0 to 21 points, with higher scores indicating better function.
Covariates
The following potential confounders were selected in our analyses: age, sex (male or female), living place (urban or rural), marital status (not married or married), education level (primary school, middle school or high school), dyslipidemia (no or yes), diabetes (no or yes), hypertension (no or yes), stroke (no or yes), heart attack (no or yes).
Statistical analysis
Descriptive analyses were conducted according to the classification of nighttime sleep subgroups. Data were displayed as mean with standard deviation for continuous variables or as frequency with column percentage for categorical factors. The Chi-square test and one-way analysis of variance were used to compare the difference between inter group of three pain status subgroups for quantitative or qualitative data.
The Group-based Trajectory Model (GBTM) was performed to identify the trajectories of depressive symptoms and cognitive function based on two-step method. 30 Determining the most suitable trajectory number was the first exploring step. The cubic form was fitted to each trajectory when GBTMs were conducted sequentially from one to five or more trajectory groups. The lowest absolute value of the Bayesian information criterion (BIC) combined with actual reasonable situation could be utilized to decide the final trajectory number. The second process was to confirm the final shapes of each trajectory fitted the most optimal polynomial order, which was linear, quadratic, and cubic. The following principles were used to estimate the ultimate trajectories if eligible: the average posterior probability of assignments (APPA) values should be greater than 70%; the odds of correct classification (OCC) ought to be more than 5.0; the estimated group proportions (EGP) should be approximate to the corresponding assigned group proportions (AGP). The generalized estimation equation (GEE) was performed to plumb the relationship between chronic pain status (without pain vs with pain; without pain vs single-site pain vs multisite pain) and per score increase with depressive symptoms or cognitive function. The quasi-likelihood under the independence model criterion (QIC) value was used for model selection in GEE analyses to choose the optimal working correlation structures. Cured models with chronic pain status and per score increase, and adjusted models that were controlled age, sex, living place, marital status, education level, dyslipidemia, diabetes, hypertension, stroke, heart attack were applied to GEEs. Multivariable multinomial logistic regression models were used to determine if chronic pain subgroups and per score increase was associated with long-term depressive symptoms and cognitive function trajectory. Two tailed P < .05 was considered to be statistically significant. All statistical analyses were conducted using SAS statistical software (version 9.4, Cary, NC).
Results
Baseline characteristics
A total of 10,683 (5066 men and 5617 women, with an average age of 57.52 ± 8.33 years) and 4644 (2589 men and 2055 women, with an average age of 56.25 ± 7.84 years) participants were included in present study. Baseline characteristics of the participants across the three pain subgroups (without pain vs single-site pain vs multisite pain) are provided in Supplement Tables 1 and 2
Association of pain status with long-term depressive symptoms and cognitive function
Associations of combined pain status with long-term depression and cognition.
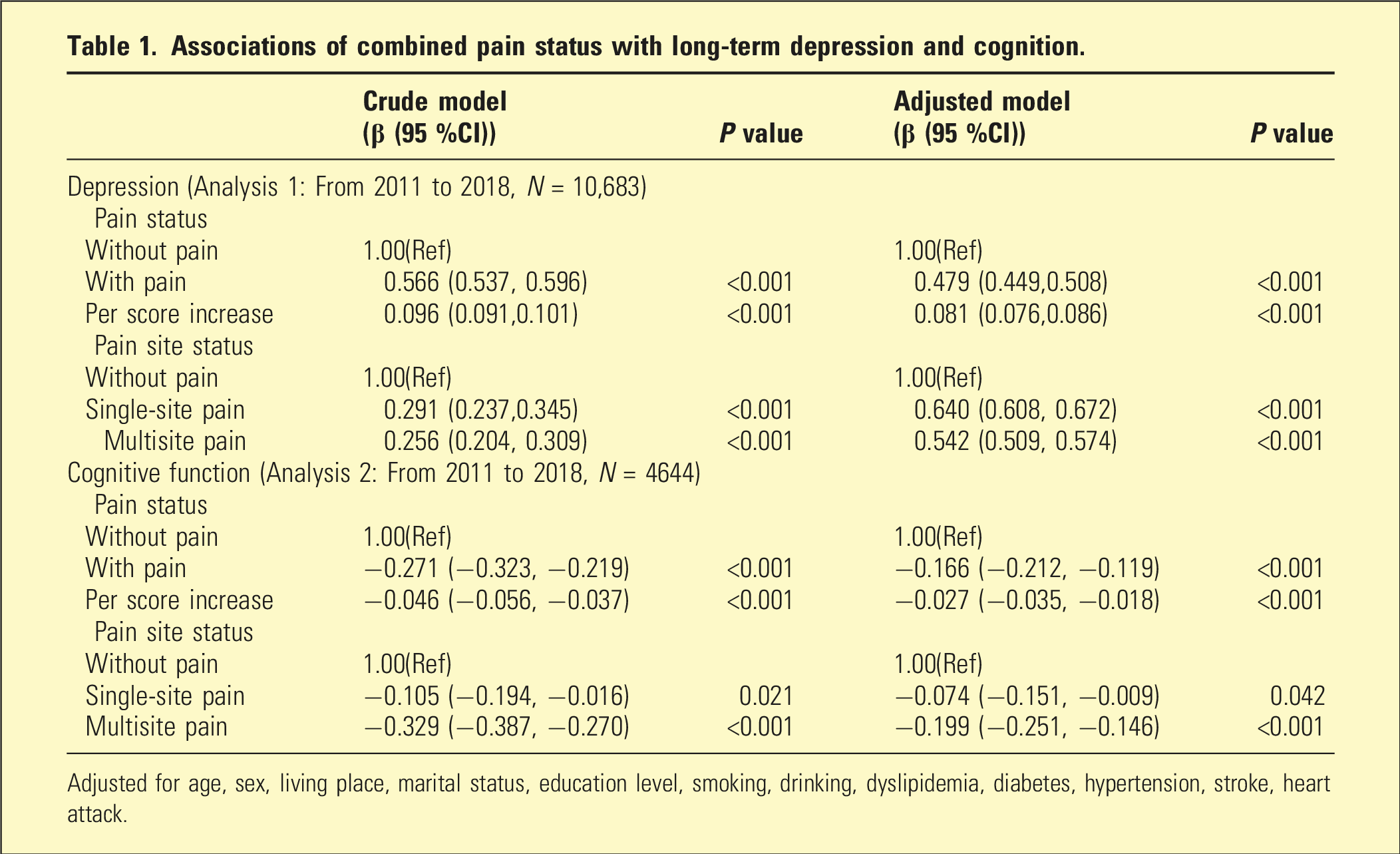
Adjusted for age, sex, living place, marital status, education level, smoking, drinking, dyslipidemia, diabetes, hypertension, stroke, heart attack.
Association of pain status with depressive symptoms and cognition trajectories
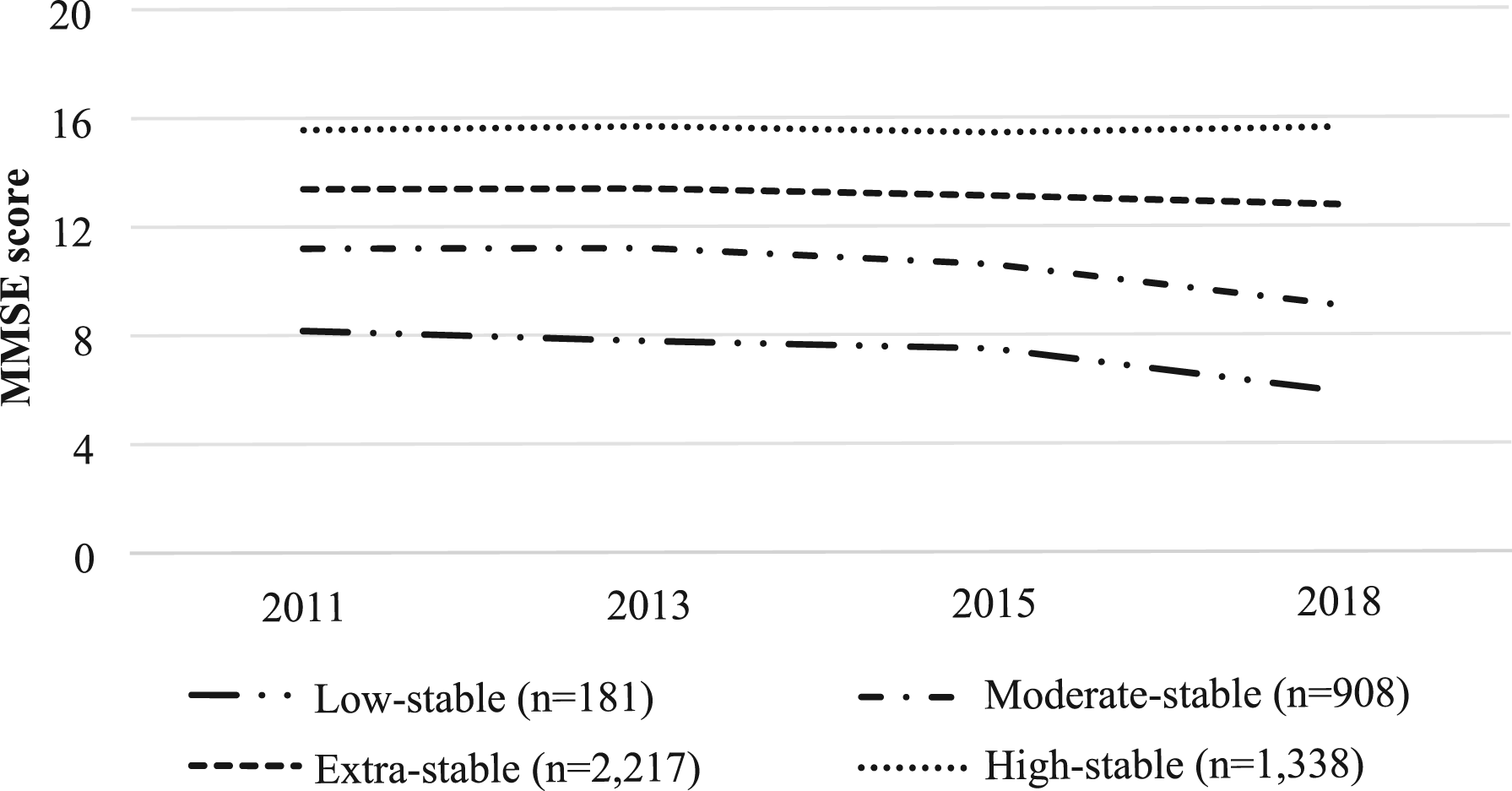
Figures 2 and 3 and Supplement Table 3 showed the overall trajectory of depressive symptoms and cognition in follow-up. Based on BIC value and reasonable actual situation, both four depressive and cognitive trajectories were found, and Figures 2 and 3 showed the overall trajectory of depressive symptoms and cognition. Same number of depressive trajectories but with slight shape difference were identified, namely persistently low-stable trajectory (Traj 1, n = 4,555, 42.64%), constantly moderate-stable trajectory (Traj 2, n = 4,053, 37.94%), extra-stable trajectory (Traj 3, n = 1,669, 15.62%) and continuously high-stable trajectory (Traj 4, n = 406, 3.80%) (Figure 2). Homoplastically, persistently low-stable trajectory (Traj 1, n = 181, 3.90%), moderate-stable trajectory (Traj 2, n = 908, 19.55%), extra-stable trajectory (Traj 3, n = 2,217, 47.74%), persistently high-stable cognition trajectory (Traj 4, n = 1,338, 28.81 %) were also identified (Figure 3). Trajectories of CES-D among the CHARLS study participants. Trajectories of MMSE among the CHARLS study participants.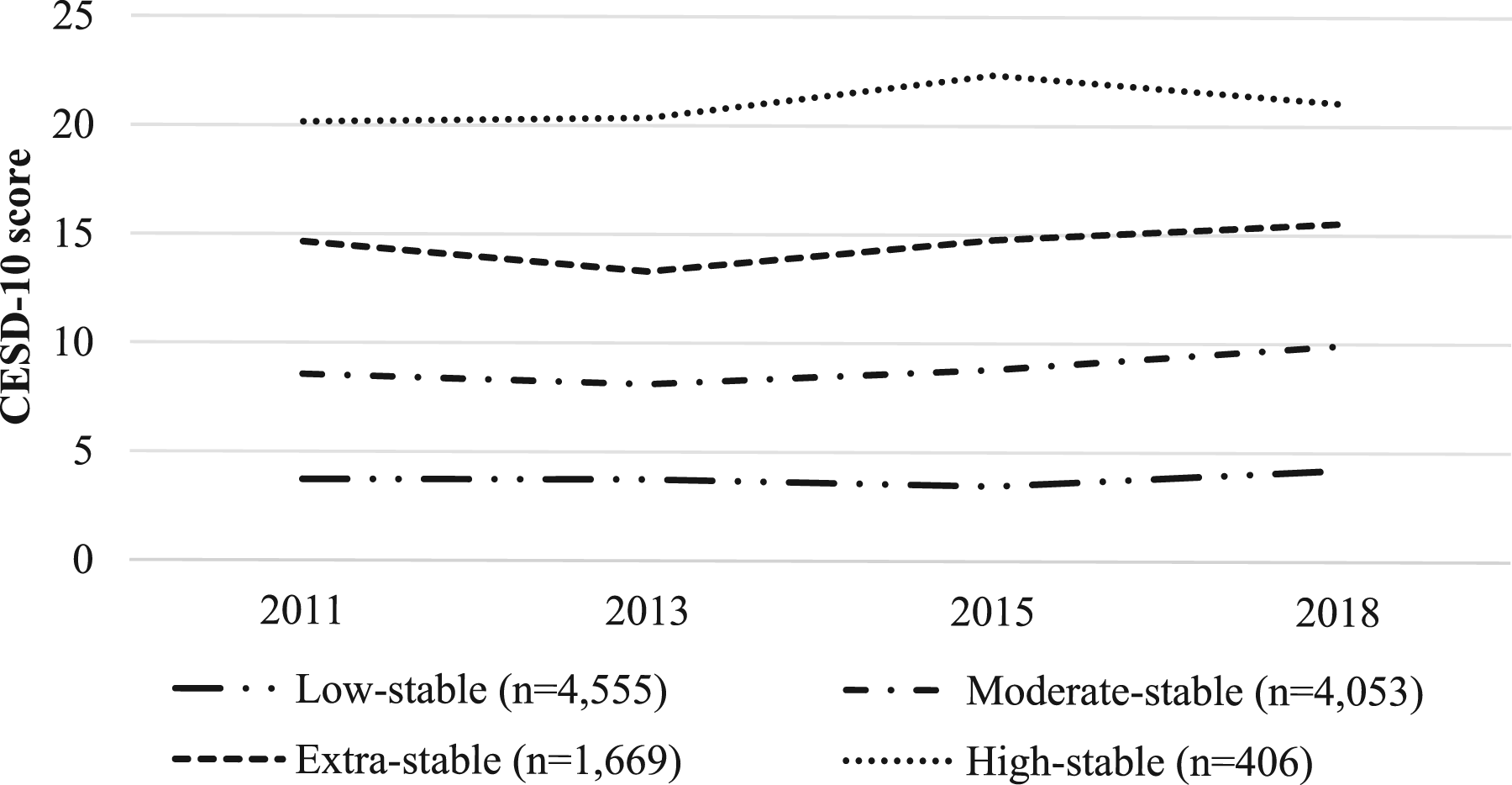
Association between with depression and cognition trajectories.
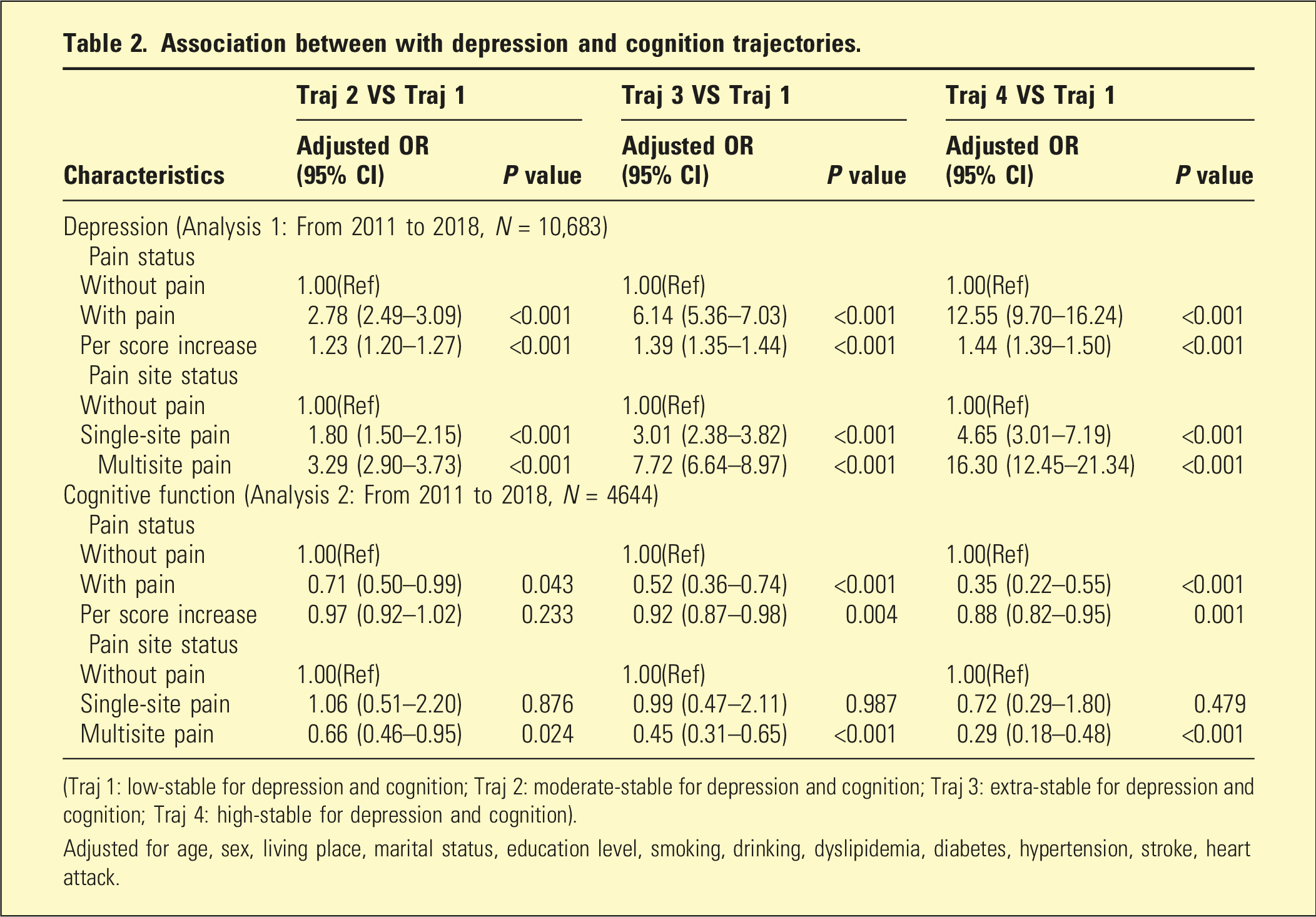
(Traj 1: low-stable for depression and cognition; Traj 2: moderate-stable for depression and cognition; Traj 3: extra-stable for depression and cognition; Traj 4: high-stable for depression and cognition).
Adjusted for age, sex, living place, marital status, education level, smoking, drinking, dyslipidemia, diabetes, hypertension, stroke, heart attack.
Discussion
Several major findings have been documented among this population-based longitudinal study of the middle-aged and elderly population in China. First, individuals with pain (both single-site and multisite pain) were more likely to suffer depressive symptoms, and were associated with lower scores for cognition function. Second, we identified four distinct depressive symptoms and cognition trajectories, and for the first time explored the association of pain status with depressive symptoms and cognition trajectories. Third, individuals with pain were significantly associated with elevated odds for the adverse depressive symptoms trajectories and tended to be less likely to belong to high cognitive trajectory. Furthermore, all of those findings were almost consistent in sex and age subgroups.
Pain, depression and cognitive decline are common in the population and co-morbid with each other. Both cross-sectional and longitudinal had reported the relationship between pain with depression and cognitive decline. Data from a systematic review and meta-analysis of 376 studies from 50 countries comprising 347,468 individuals indicated that clinical symptoms of depression were present in 39.3% (95% CI, 37.3%-41.1%) among adults with chronic pain. 31 Another systematic review and meta-analysis of 273,952 individuals from 47 low- and middle-income countries also found a linear increase in the prevalence of all types of depression was observed with increasing pain scores. 17 Similarly, evidence from a meta-analysis of 37 studies with a total of 52,373 patients with chronic pain and 80,434 healthy control participants suggested that chronic pain was associated with cognitive decline when the short-form 36 health survey questionnaire mental component summary (SMD = −1.50, 95% CI = −2.19 to −0.81), the Montreal cognitive assessment (SMD = −1.11, 95% CI = −1.60 to −0.61), performance validity testing (SMD = 3.05, 95% CI = 1.74 to 4.37), or operation span (SMD = −1.83, 95% CI = −2.98 to −0.68) were used. 32 Based on the four-wave information of CHARLS (from 2011 to 2018), our findings suggested pain (regardless of single-site or multisite pain) associated with longitudinal increases in depressive symptoms, and decrease in cognitive function after 7-year follow-up. Taking together, our findings combined with previous reported studies supported the hypothesis that individuals with pain was associated with long-term depressive symptoms and cognitive impairment during a long-period follow-up.
In general, previous studies have shown that depressive symptoms and cognitive function in the elderly develop dynamically with age, and individuals may show different change patterns at different times. Better than measuring depression/cognitive function at a single time point, establishing depression/cognitive function trajectories based on multiple measurements over a longer time period may capture the dynamic and heterogeneous nature of depression/cognitive function. In French GAZEL study of 12,650 individuals participating, Melchior et al. identified four depression trajectory (no depression, increasing depression, decreasing depression and persistent depression) groups after 13 years of follow-up. 33 You et al. using data from the CHARLS in 2011, 2013, 2015, and 2018 also identified four depression symptom trajectories throughout the follow-up process: “low depressive symptom group,” “worsening depressive symptom group,” “relieved depressive symptom group,” and “high depressive symptom group.” 34 In addition, findings from the Irish Longitudinal Study on Ageing of 2327 participants with repeated neuropsychological tests (8.08 ± 0.3-year follow-up) identified three cognitive function trajectory groups: high-stable, mid-stable, and low-declining cognitive function trajectories. 35 Furthermore, Mose et al. found three cognitive function trajectory groups: low-decline group, medium-decline group and high-stable group using data from CHARLS 2013–2018. 36 In somewhat contrast to previous studies, we identified four distinct depressive symptoms and cognition trajectories using trajectory modeling method. We found individuals with pain were significantly associated with elevated odds for the adverse depressive symptoms trajectories and tended to be less likely to belong to high cognitive trajectory. Further studies are needed to confirmed our findings that whether the association between pain status with depressive symptoms and cognition trajectory was valid.
The current findings provide a strong rationale for improving health services and interventions to better meet the mental health needs of older adults with pain. The current approach to treating chronic pain emphasizes a personalized, multimodal, and multidisciplinary strategy, including pharmacological interventions and non-pharmacological methods, and has been proved to make a modest improvement to the burden of pain symptoms. 37 In the context of aging and with the growing number of patients with depression or cognitive impairment, even modest positive effects related to greater adherence to an overall chronic pain management could yield significant public health benefits if they can be cost-effectively delivered on a large scale. Therefore, we call for increased emphasis on offering more tailored and effective approaches to alleviate the burden of chronic pain.
The present study was based on the data from the CHARLS study, which is a large nationally representative cohort study with a high response rate, and potential confounders were collected and controlled in the multivariable models. However, several potential limitations of present study need to be mentioned. First, the present study used observational data from CHARLS. Although, we had adjusted a series of confounders. This observational analysis could be influenced by potential biases and confounding factors. Second, our exposures were measured by self-reported, random measurement error may have biased results toward the null, and thereby underestimating the true magnitude of the associations. Third, some of the participants were excluded from analysis due to incomplete baseline information or outcome data, and there was a large discrepancy between the sample size for depressive symptoms and cognitive function, which may cause selection bias. Fourth, the cumulative score of pain based on number of places in the body may also cause bias.
In conclusion, the present study indicated that individuals with pain were more likely to suffer more depressive symptoms, and were associated with lower scores for cognition function. Furthermore, those with pain were also significantly associated with higher odds for the adverse depressive symptoms trajectories, and lower likely to belong to high cognitive trajectory.
Supplemental material
Supplemental Material - Longitudinal relationship between pain with long-term depressive symptoms, cognitive function and its trajectory among middle-aged and older adults in China
Supplemental Material for Longitudinal relationship between pain with long-term depressive symptoms, cognitive function and its trajectory among middle-aged and older adults in China by Xinyue Zhang, Wenyang Han, Yiqun Li, Xiaowei Zheng in Australasian Psychiatry.
Footnotes
Acknowledgments
This analysis uses data or information from the Harmonized CHARLS dataset and Codebook, Version C as of April 2018 developed by the Gateway to Global Aging Data. The development of the Harmonized CHARLS was funded by the National Institute on Ageing (R01 AG030153, RC2 AG036619, R03 AG043052). For more information, please refer to ![]() .
.
Ethics approval
The ethics application for collecting data on human subjects in CHARLS was approved by the Biomedical Ethics Review Committee of Peking University (IRB00001052-11,015).
Consent to participate
All CHARLS participants provided written informed consent.
Authors’ contributions
Xiaowei Zheng conceived and designed the research; Xinyue Zhang and Wenyang Han wrote the manuscript; Wenyang Han and Yiqun Li performed the data analysis. All authors reviewed the manuscript.
Funding
The study was supported by Jiangsu Province Young Science and Technology Talent Support Program (JSTJ-2025-474).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
This analysis uses data or information from the Harmonized CHARLS dataset and Codebook, Version C as of April 2018 developed by the Gateway to Global Aging Data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.