
Abstract
Six 11-wk-old, commercial, Broad-Breasted White, meat turkeys were submitted to the Turlock branch of the California Animal Health & Food Safety (CAHFS) laboratory for autopsy and diagnostic work-up. Clinical signs in the turkeys of the affected flock included depression, ruffled feathers, swollen periorbital areas, rales, and sneezing. A mortality of 50% (5,000 of 10,000) was reported at the time of case submission. Flock morbidity was 100% by 12 wk of age, and mortality eventually exceeded 90%. Fibrinous pleuropneumonia, airsacculitis, increased luminal mucoid exudate in the nasal cavities and tracheas, mottled and enlarged spleens, and hepatomegaly were the most remarkable gross findings. Microscopically, fibrinoheterophilic pneumonia and epicarditis with intralesional bacterial colonies, and necrotizing hepatitis and splenitis, were noted. Mycoplasmoides (Mycoplasma) gallisepticum (MG) was detected in tracheal and sinus pools by quantitative real-time PCR. Multilocus sequence analysis of the mgc2 gene and IGSR segment of MG differentiated our strain from MG vaccine strains, but were similar to MG isolates detected previously in other commercial turkey operations in California. Pasteurella multocida was isolated from air sacs, lungs, tracheas, hearts, and livers, and classified as profile HhaI 0001, strain X-73, by restriction enzyme analysis DNA fingerprinting. Coinfection with P. multocida and MG in a susceptible flock resulted in rapid elevation of mortality and significant economic losses in this commercial meat turkey operation.
High mortality events in commercial poultry due to infection with one or more pathogens can have severe impacts on intensive poultry production. Development of infectious diseases in poultry flocks can result in animal welfare issues and economic challenges associated with high morbidity and mortality, and increased condemnations. In addition, there are added economic costs and labor associated with diagnostic procedures, intervention strategies, and extended downtime periods between grow-out flocks.2 −4,9,10
Epornitics of acute fowl cholera caused by Pasteurella multocida are occasionally reported in wild bird species, such as pheasants and waterfowl.3,6 In commercial turkeys, mortality induced by P. multocida varies widely, and mortality as high as 68% has been described. 3 Mycoplasmoides (Mycoplasma) gallisepticum (MG) is the causative agent of infectious sinusitis in turkeys. MG strains vary widely in pathogenicity, and mortality and morbidity rates are highly variable.1,2 Flock morbidity is usually higher than mortality, and morbidity is usually low or moderate but can progress to 90% in turkey flocks exposed to environmental stressors and opportunistic pathogens.2,7 MG infection mortality in commercial turkeys is infrequently reported, but mortality rates of 4–25% have been reported. 1
Although coinfection of commercial turkeys with P. multocida and MG is occasionally reported, simultaneous flock infection with both pathogens leading to high mortality is rarely reported in modern, commercial poultry systems. The pathology of this combined infection has not been described in detail.
Five dead, and 1 live, 11-wk-old, Broad-Breasted White, commercial meat turkeys originating from 1 barn with 10,000 turkeys were submitted to the Turlock Branch of the California Animal Health & Food Safety (CAHFS; University of California−Davis, Davis, CA, USA) diagnostic laboratory, for postmortem examination and diagnostic work-up. Turkeys were reared on a commercial broiler premises in the Central Valley of California in curtain-sided barns with outdoor access pens. Birds were submitted due to increased flock morbidity and mortality increasing from 1.0% to 50% within 1 wk, in 1 of the 3 barns on the affected premises. Mortality and morbidity continued to increase and surpassed 90% by 1 wk post submission. Clinical signs included depression, ruffled feathers, swollen periorbital areas, and rales. Turkeys had been vaccinated at 5 wk of age against hemorrhagic enteritis virus (HEV; family Adenoviridae, taxon species Siadenovirus gallopavotertii) using a live avirulent avian adenovirus. When mortality increased, all of the birds in the flock were medicated with oxytetracycline hydrochloride powder in drinking water, but mortality rebounded on cessation of treatment.
The one live bird submitted was euthanized with CO2, according to standard operating procedures of CAHFS and following AVMA guidelines. Blood was collected immediately after death for ELISA for antibody detection against avian influenza A virus (avian IAV; Orthomyxoviridae, Alphainfluenzavirus influenzae), MG, Mycoplasmopsis (Mycoplasma) synoviae (MS), Newcastle disease virus (NDV; Paramyxoviridae, Orthoavulavirus javaense), P. multocida (Idexx), and HEV (ProFlock; Zoetis). Serum samples were negative for antibodies to AIV, MG, MS, NDV, and P. multocida. The HEV ELISA was positive, and a titer of 14,252 (titer group 12) was detected.
An autopsy was performed on all 6 birds submitted. Grossly, there was hyperemia of the nasal cavity, skeletal muscles, and the skin of the head and neck (6 of 6). Clear exudate was in the medial canthus of the eyes (3), and tracheal lumen (2), and large quantities of clear mucus and off-white to pale-yellow caseous exudate were in the nasal cavity and infraorbital sinuses (3). There was moderate accumulation of fibrinous exudate in the thoracic and abdominal air sacs (3), severely enlarged, mottled, and friable livers (4), congested livers (2), mildly enlarged, congested kidneys (6), and severely enlarged, mottled spleens (6; Fig. 1A). The lungs were consolidated, and there was exudate on the surface of the lungs (6; Fig. 1B).
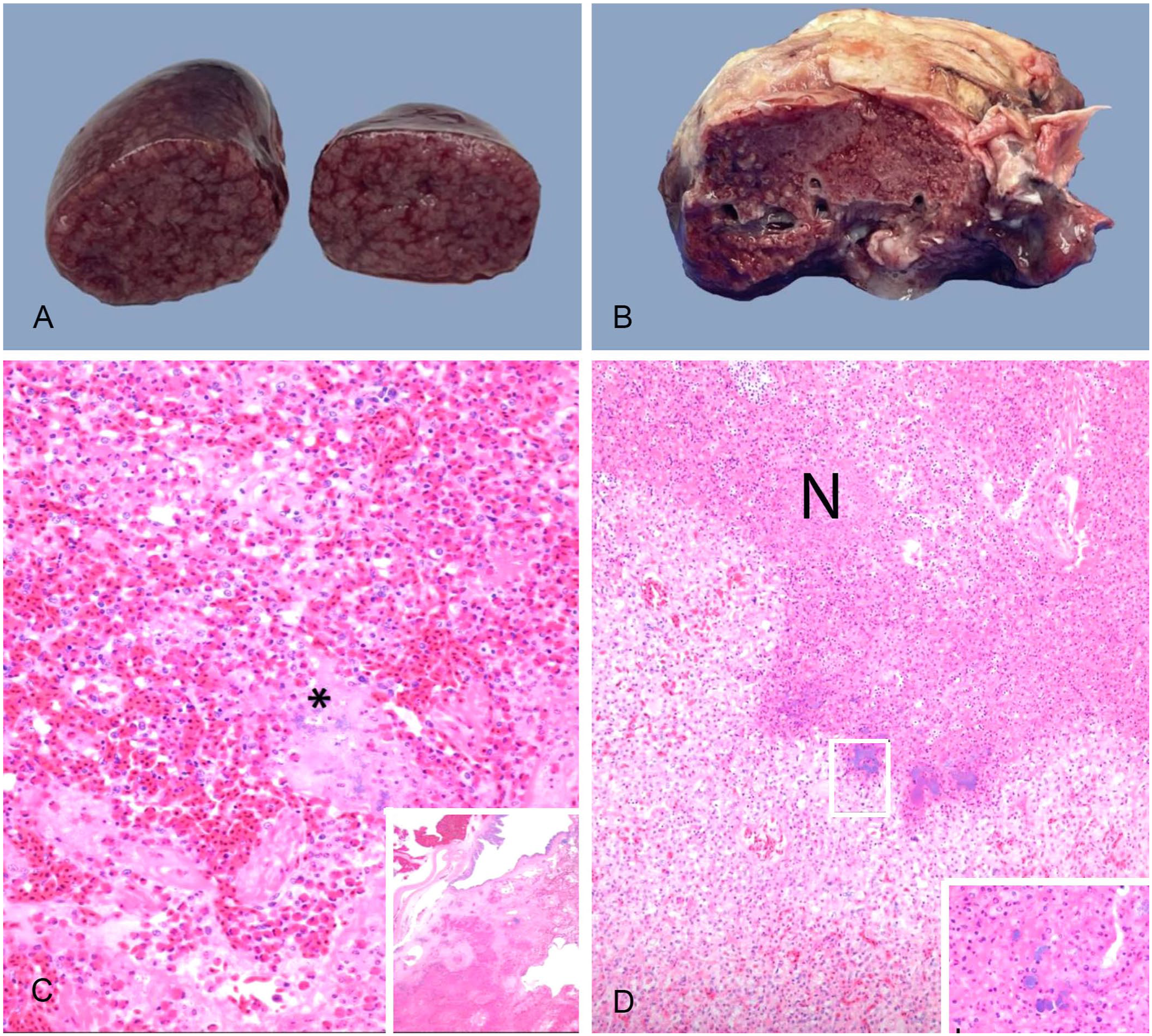
Gross and microscopic findings in an 11-wk-old commercial turkey with Pasteurella multocida and Mycoplasmoides (Mycoplasma) gallisepticum coinfection.
Samples of nasal cavity, eyelids, heart, trachea, lung, air sac, spleen, liver, and small and large intestine were collected and fixed in 10% neutral-buffered formalin for 72 h. All tissues were processed to produce 4-µm thick, H&E-stained sections. Microscopically, there was lymphocytic rhinitis, eyelid conjunctivitis, tracheitis, infraorbital lymphocytic sinusitis, and congestion of nasal mucosa with accumulation of caseous exudate and cellular debris in nasal cavities. In the lung, there was extensive fibrinoheterophilic exudate in the alveoli, parabronchi, and interstitium (Fig. 1C). Large numbers of intralesional bacterial colonies (IBCs) were also noted within parabronchi. Air sacs were extensively expanded by fibrinoheterophilic exudate with scattered IBC. Multifocal-to-coalescing necrosis, mononuclear and granulomatous hepatitis with IBC, and congestion were observed in the liver (Fig. 1D). The epicardium had extensive fibrinoheterophilic exudate with scattered IBC. Randomly distributed, variably sized, necrotic foci with or without heterophil infiltrates and IBC were observed in spleens. Spleens also had extensive and severe lymphocyte depletion. No other microscopic abnormalities were observed.
No parasites or parasite eggs were observed on microscopic examination of small and large intestinal scrapings and fecal flotations.
Swabs from infraorbital sinuses, hearts, tracheas, lungs, air sacs, and livers were inoculated onto chocolate agar (Thermo Scientific), 5% sheep blood agar (Thermo), and MacConkey agar (Thermo) plates and incubated with 7% CO2 at 37°C for 48 h. Pure cultures of P. multocida were isolated from liver, air sac, heart, and lung cultures. P. multocida and Escherichia coli were isolated from tracheas.
Quantitative real-time PCR (qPCR) tests were performed on the liver tissue pool for P. multocida, on the trachea swab pool and sinus swab pool for MG and MS, and on the spleen tissue pool for HEV. Reverse-transcription qPCR (RT-qPCR) tests were performed on the oropharyngeal swab pool for avian IAV and NDV and on the sinus swab pool for avian metapneumovirus (AMPV; Pneumoviridae, Metapneumovirus avis) types A–C. P. multocida was detected in the liver, and HEV was detected in the spleen pool by molecular tests. MG was detected in both sinus and trachea swab pools by qPCR. Molecular detection tests were negative for MS, avian IAV, NDV, and AMPV types A–C.
The P. multocida isolate was submitted to the National Veterinary Services Laboratories (NVSL; USDA, Ames, IA, USA) for restriction endonuclease analysis DNA fingerprinting using enzyme HhaI 11 (NVSL) and was genotyped as profile HhaI 0001. The DNA profile of the isolate was identical to the profile of somatic strain X-73. Less than 0.1% of NVSL diagnostic submissions from domestic poultry have been genotyped as profile HhaI, strain X-73; >95% of isolates from wild migratory waterfowl submitted to the NVSL have been characterized as strain X-73 (NVSL diagnostic report). The plausibility of wild bird introduction of fowl cholera into the affected turkey flock is supported by the detection of the X-73 strain, which is identified most often in migratory waterfowl. Other risk factors for the introduction and rapid spread of fowl cholera in this commercial turkey flock include having outdoor access, which can facilitate contact with mammalian vectors and rodents, infrequent collection of dead turkeys, and environmental stressors.3,4 Virulence-associated genotypic and phenotypic factors of P. multocida strains were not assessed in our case, but these factors can play a role in increasing the severity of disease. In addition, coinfection with primary pathogens such as MG or opportunistic poultry pathogens can also play a role in exacerbating flock morbidity and mortality. 2
The MG isolate was subsequently characterized by multilocus sequence analysis of both the mgc2 gene (Fig. 2A) and the intergenic spacer region (IGSR; Fig. 2B) of MG.5,8 Phylogenetic analyses of both loci were performed, and our isolate was compared to other MG field isolates from prior CAHFS poultry submissions and the vaccine strains Mycovac-L (Merck), ts-11 (Zoetis), and F VAX (Merck). Comparison across the mgc2 gene and IGSR segment indicated that the MG isolated from our cases was genetically distinct from the 3 vaccine strains but similar to MG isolates detected in commercial turkey operations in the Central Valley in 2013, 2015, and 2017 (isolate IDs: 2013A, 2015C, 2017A, respectively). The source of the MG identified in our case remains unclear, but MG can be transmitted vertically and horizontally in flocks. 2 Introduction of MG infection can occur by wild birds or, alternatively, latently infected carrier poultry species can remain MG carriers for prolonged periods. Introduction of MG onto premises can also occur indirectly via fomites and by movement of humans. 2 Stringent biosecurity measures are critical in limiting the introduction and spread of P. multocida and MG in poultry flocks.
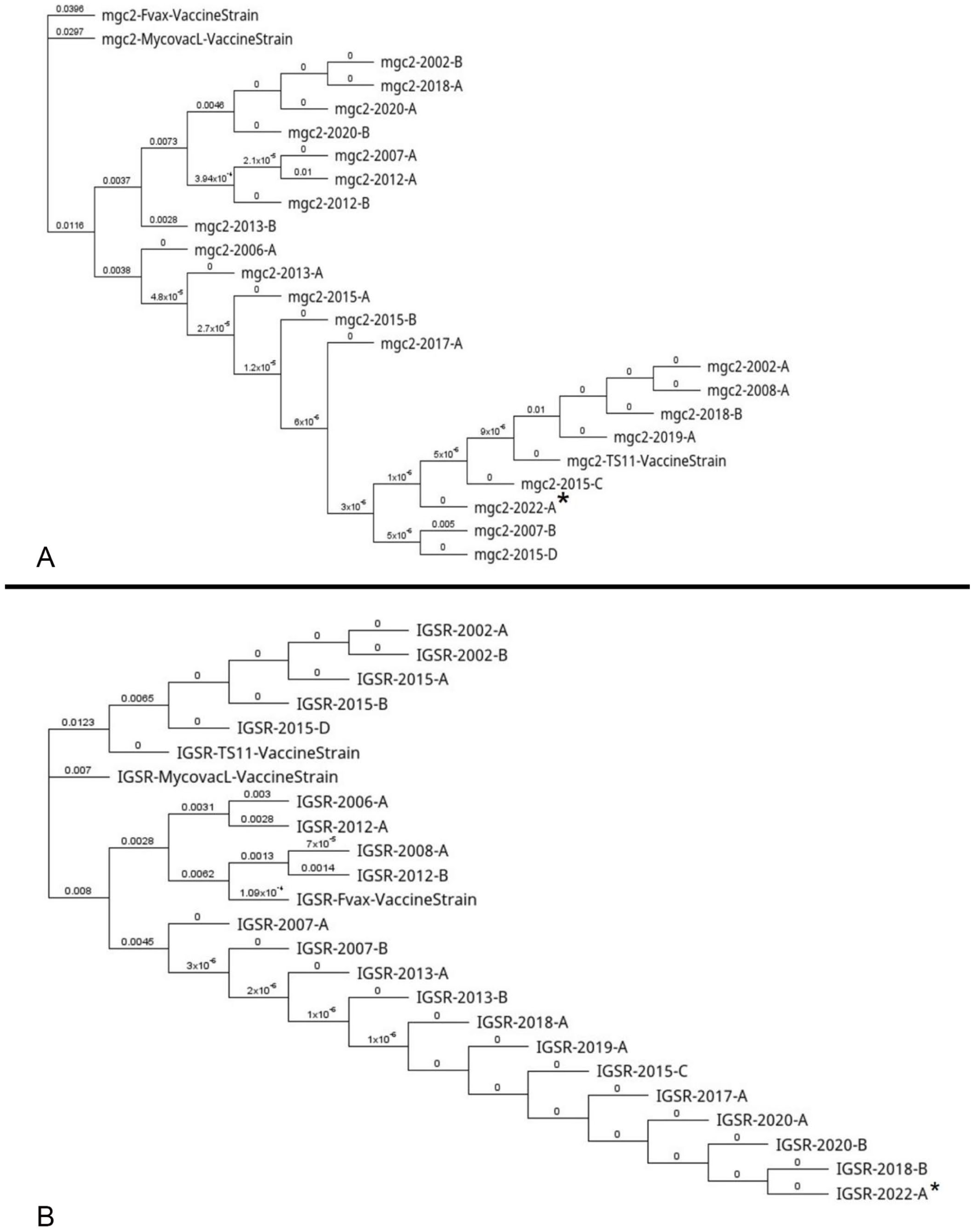
Multilocus sequence analysis of Mycoplasmoides (Mycoplasma) gallisepticum (MG).
The HEV detected by qPCR and serology may be associated with the vaccination of the flock at 5 wk of age with a live avirulent HEV vaccine. No intranuclear inclusion bodies or lesions compatible with HEV infection were detected in the sections of spleen and intestine examined microscopically in our case. Despite the detection of both P. multocida and MG by molecular tests, the ELISAs were negative for antibodies against these 2 pathogens, which indicates that the birds submitted had not yet seroconverted post exposure and supports the acute nature of infection with both pathogens at the time of diagnostic submission.
The catastrophic mortality in our case, caused by coinfection with P. multocida and MG in commercial turkeys, was significantly higher than the previously reported H5N8 highly pathogenic avian influenza (HPAI) outbreak affecting turkeys in 2016 in California. 9 Although HPAI and virulent Newcastle disease are often associated with acute spikes in mortality,9,10 other causes of high economic losses can occur in poultry. The conjunctivitis, sinusitis, tracheitis, and airsacculitis observed are consistent with those noted in MG infections in turkeys. 1 Fibrinous pneumonia, necrotizing hepatitis, and splenitis were observed in our case and are often noted in cases of acute fowl cholera.3,4
Footnotes
Acknowledgements
We thank the technical staff of the CAHFS Turlock branch for their excellent assistance in ancillary tests.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.