
Abstract
Cholangiocarcinoma (CCA) affects a range of veterinary species, but its heterogeneous morphology complicates diagnosis, particularly when features overlap with benign biliary lesions, congenital anomalies, and other neoplasms. To identify common diagnostic pitfalls and define practical diagnostic criteria, we retrospectively reviewed 24 suspected CCA cases across 16 species submitted to Johns Hopkins University between 1986 and 2024. Twelve cases were confirmed as CCA, 2 were unclassified, and 10 were reclassified as biliary adenoma, biliary hamartoma, polycystic liver disease, primary neuroendocrine tumor, or metastatic adenocarcinoma based on histology and immunohistochemistry (cytokeratin, synaptophysin). From recurring diagnostic patterns, we developed a diagnostic flowchart emphasizing mass effect, growth pattern, architectural pattern (cystic vs. solid), features of malignancy, and immunohistochemical criteria to aid in stepwise interpretation of proliferative ductular lesions. Furthermore, confirmed CCA cases aligned with large- and small-duct subtypes described in human pathology. Collectively, our cases underscore both the diagnostic challenges and shared histomorphologic and immunohistochemical characteristics across species within the spectrum of biliary proliferative disorders.
Keywords
Cholangiocarcinoma (
In human pathology, intrahepatic CCA is subclassified into large-duct and small-duct CCA based on histomorphology, with differences in pathogenesis and prognosis. 2 Comparable subtypes have not been systematically described in veterinary species, nor has the histomorphologic spectrum of biliary neoplasia been evaluated across taxa.
We retrospectively reviewed 24 cases of suspected CCA submitted between 1986 and 2024 to the Department of Molecular and Comparative Pathobiology (MCP) at Johns Hopkins University (Baltimore, MD, USA) using the following keyword terms: “cholangio-”, “cholangiocarcinoma”, “biliary”, “bile duct”, “gallbladder”, “ductular”, “adenocarcinoma”, “hepatic mass”, “hepatic carcinoma”, “carcinoid”, and “neuroendocrine”. Inclusion criteria consisted of cases with suspected primary biliary or ductular hepatic lesions and available histologic material (archived paraffin blocks and/or H&E-stained slides) for review. Cases were included regardless of species, completeness of clinical data, or availability of immunohistochemistry (IHC). Exclusion criteria included severe autolysis precluding histologic interpretation or insufficient tissue for diagnostic reassessment.
Our aims were to 1) define the histologic spectrum of CCA in veterinary medicine and 2) develop a diagnostic flowchart to aid in the classification of ductular liver lesions across species. We characterized each lesion using gross, histologic, and immunohistochemical features; identified common diagnostic pitfalls; and documented the range of lesions that mimicked CCA. We then synthesized the recurrent diagnostic decision points observed across cases, including mass effect, presence of cystic morphology, features of malignancy, and immunohistochemical profile, into a practical diagnostic flowchart (
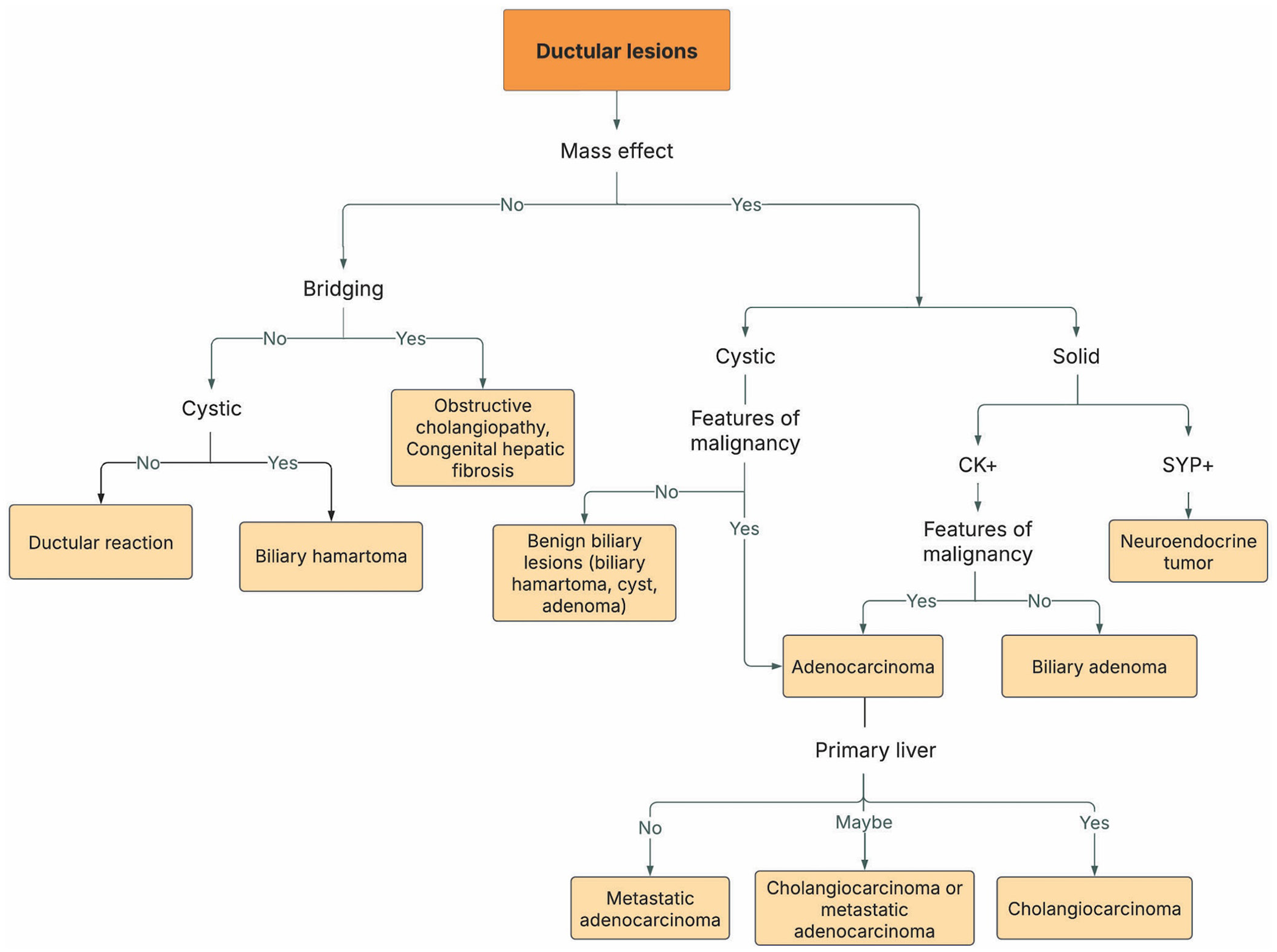
Diagnostic flowchart for ductular liver lesions, with key histologic and immunologic features used to differentiate cholangiocarcinoma (CCA) from other mimics. Malignant features include high mitotic index, nuclear atypia, cell piling, lymphovascular invasion, and metastasis. CK = cytokeratin (cytokeratin 7, 19, or pan-cytokeratin); SYP = synaptophysin.
Application of the diagnostic flowchart
Step 1: determine presence or absence of mass effect (gross or histologic)
Mass effect, defined as an expansile nodule, served as the initial branching point. Lesions without mass effect typically were ductal plate malformations (
Step 2: evaluate histomorphologic pattern (cystic vs. solid)
Among mass-forming lesions, cystic, non-invasive patterns favored benign entities, such as polycystic liver disease, hamartomas, or adenomas; solid masses required further distinction between epithelial and neuroendocrine tumors.
Step 3: immunohistochemical confirmation
IHC was essential for lineage determination of solid masses. Epithelial neoplasms had positivity for pan-cytokeratin (pan-CK), CK7, or CK19, whereas neuroendocrine tumors were synaptophysin-positive and CK-negative, allowing resolution of cases with pseudoglandular morphology. Although we evaluated only synaptophysin, additional neuroendocrine markers may be used depending on laboratory validation and availability. When lesions do not meet morphologic and/or immunohistochemical criteria for a defined entity, cases should exit the flowchart and be designated descriptively (e.g., “unclassified” or “indeterminate biliary carcinoma”) with documentation of differential diagnoses.
Step 4: evaluate features of malignancy
Epithelial lesions were assessed for malignancy using cytologic atypia, stromal response, and invasive growth, including parenchymal, lymphovascular, or perineural invasion.
Step 5: exclude metastatic disease, if possible
In hepatic tumors with atypical or mixed features, further evaluation of lesion distribution and IHC profiling was used to exclude metastatic adenocarcinoma, particularly from the pancreaticobiliary system, gastrointestinal tract, or other extrahepatic sites. Cases with widespread involvement or discordant primary-site morphology were classified as metastatic disease.
Of the 24 cases, 12 were confirmed as CCA, 10 were reclassified following histologic and immunohistochemical evaluation, and 2 remained unclassified ( Table 1 ). Relevant clinical data were recorded when available and cases are referenced by species and case number ( Suppl. Table 1 ).
Distribution of cholangiocarcinoma (CCA) subtypes and histologic mimics across taxonomic groups including morphologic subtypes and documented metastasis. Cases were retrospectively reviewed and reclassified based on histomorphology and immunohistochemistry.
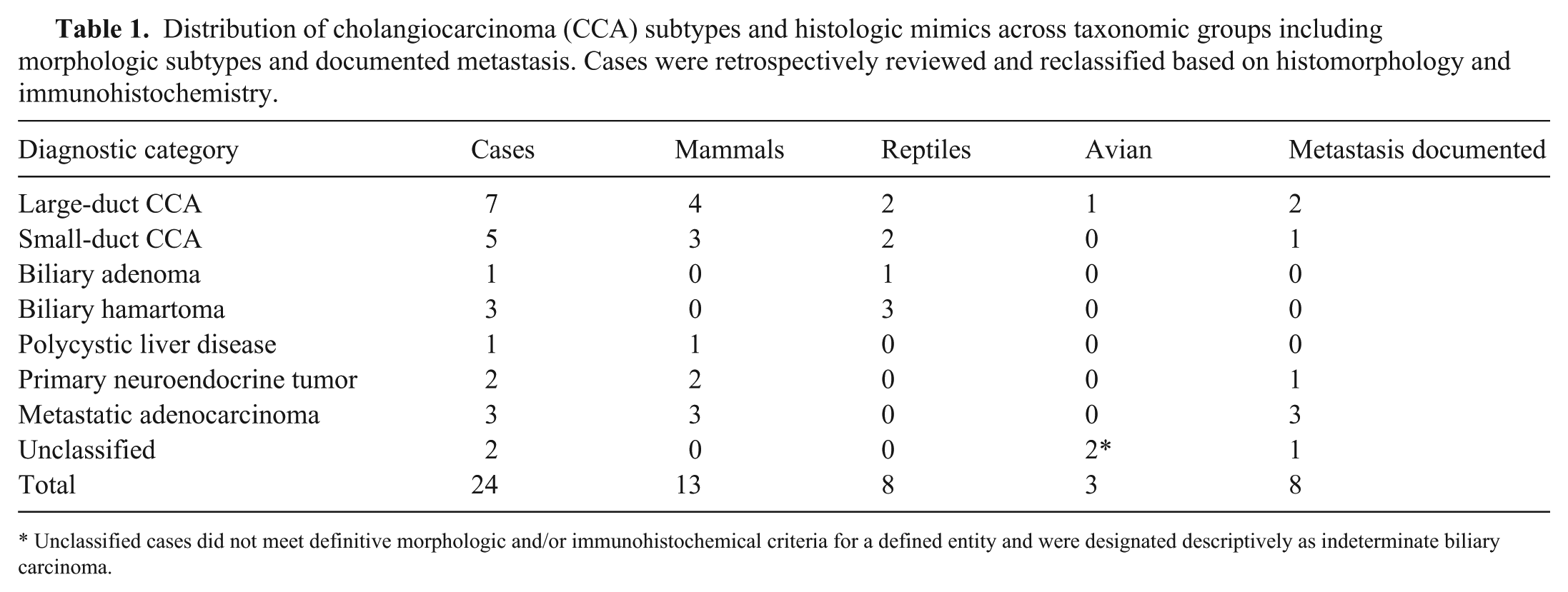
Unclassified cases did not meet definitive morphologic and/or immunohistochemical criteria for a defined entity and were designated descriptively as indeterminate biliary carcinoma.
Cholangiocarcinoma
Most CCA cases were intrahepatic, with one extrahepatic case identified in the perihilar region of an olive baboon (Papio anubis; case 1). Grossly, intrahepatic CCAs were commonly well-demarcated, yellow-tan masses with umbilicate or fluid-filled centers, extending into adjacent liver parenchyma. In contrast to human cases, which are typically solitary and solid, 5 veterinary cases often had numerous lesions, likely reflecting delayed detection and secondary spread. In our cases, we classified CCA in animals using the 2 major subtypes recognized in humans: large-duct and small-duct.
Large-duct CCAs (cases 1–4, 8, 11, 12)
In large-duct CCAs, mucin-producing (PAS-positive) columnar epithelial cells formed lakes of intraluminal mucin (

Histologic features of cholangiocarcinoma (CCA) and histologic mimics. H&E, unless otherwise noted.
Small-duct CCAs (cases 5–7, 9, 10)
In small-duct CCA, well-differentiated, non–mucin-producing (PAS-negative) cuboidal epithelial cells were within a hyalinized or desmoplastic stroma, causing a mass effect and irregular invasion into adjacent liver parenchyma (
Histologic mimics and differential diagnoses
Among the 10 reclassified cases, 5 major histologic mimics were identified: biliary adenoma, biliary hamartoma, polycystic liver disease (DPM), primary neuroendocrine tumor, and metastatic adenocarcinoma.
Biliary adenoma (cholangiocellular adenoma, case 19)
The case of biliary adenoma was a mass-forming lesion of cystic or solid, non-invasive bile ducts. A western hognose snake (Heterodon nasicus) had 2 discrete adenomas in subcapsular and intrahepatic locations. These were benign, well-circumscribed masses of uniform bile ducts with a fibrotic stroma (
Biliary hamartoma (cases 20–22)
Also known as von Meyenburg complex, biliary hamartoma is generally a small, non–mass-forming, and solitary malformation of abnormally formed ducts embedded in a fibrous mass, isolated from the biliary tree. When found in later stages, lesions may have a mass effect. In the diagnostic flowchart, these lesions are defined by cystic ductular profiles without features of malignancy. A solitary biliary hamartoma is typically considered an incidental lesion, whereas multiple biliary hamartomas can be compatible with a DPM. The prevalence of this lesion in veterinary species is unknown, but they have been reported in cats and reptiles.12,14 Our cases included a blotched blue-tongued skink (Tiliqua nigrolutea), Mexican milk snake (Lampropeltis annulata), and green vine snake (Oxybelis fulgidus). Lesions were microscopic, well-demarcated, frequently subcapsular, variably cystic, irregularly formed ducts lined by attenuated cuboidal epithelium and supported by moderately hyalinized collagenous trabeculae (
Polycystic liver disease (case 13)
In polycystic liver disease (PCLD), mass-forming, multiloculated cystic lesions arise from aberrant ductal plate remodeling. PCLD follows the non-neoplastic, cystic branch but is distinguished from biliary hamartomas by the size, expansile nature, and marked mass effect of the lesions. Our case was in a Ragdoll cat (Felis catus), with large, fluid-filled cystic biliary masses that had a pronounced mass effect on adjacent liver parenchyma. Histologically, cysts were lined by flattened, monomorphic biliary epithelium and supported by thin, collagenous trabeculae with notable compression and atrophy of adjacent hepatocytes (
Primary neuroendocrine tumor (carcinoid, cases 14, 15)
Primary neuroendocrine tumors of the liver can closely mimic CCA, given the pseudoglandular or acini-like architecture, creating significant overlap on routine H&E evaluation. In the diagnostic flowchart, these lesions follow a mass-forming, solid architecture, but diverge at the immunohistochemical decision point. Our cases involved a DSH cat and a mixed-breed dog with hepatic neuroendocrine tumors that closely mimicked CCA with pseudoglandular architecture and malignant histologic features (
Metastatic adenocarcinoma (cases 16–18)
Metastatic adenocarcinomas involving the liver can be morphologically and immunohistochemically indistinguishable from primary CCA, particularly when lesions are identified in the pancreaticobiliary system, major duodenal papilla, ampulla, or gastrointestinal tract. In the diagnostic flowchart, these lesions follow the mass-forming, epithelial branch with features of malignancy, but diverge based on lesion distribution in extrahepatic sites. Metastatic lesions were identified in an olive baboon, a rhesus macaque (Macaca mulatta), and a DSH cat. All 3 cases had invasive tubular or gland-forming architecture, mass effect, and IHC CK positivity, closely resembling CCA (
Unclassified cases
Two avian cases remained unclassified (cases 23, 24) because of CK negativity and equivocal synaptophysin expression. Interpretation in these species is complicated by variable cross-reactivity of commonly used mammalian antibodies, the lack of species-validated markers limiting further classification, and the limitations of using a restricted number of markers. Morphologic findings were insufficient to support a definitive diagnosis without additional IHC confirmation, and the results were therefore interpreted with caution.
Our study offers a descriptive, multispecies overview of CCA and its major histologic mimics, highlighting both the diagnostic challenges and conserved morphologic patterns that emerge across taxa. Despite the broad species range, CCAs consistently had recognizable histomorphology, including division into large-duct and small-duct subtypes, characteristic stromal responses, and shared features of malignancy.
The recognition of large-duct and small-duct CCA morphologies in our cohort parallels subclassification schemes described in human medicine. In humans, cholangiocarcinogenesis is a multistep process shaped by various genetic, epigenetic, environmental, and inflammatory influences, with the cell of origin further contributing to morphologic heterogeneity. 2 Large-duct tumors arise from biliary epithelial cells and peribiliary glands, whereas small-duct tumors arise from hepatic progenitor or cholangiolar cells. 10 Although metastatic disease was observed across both morphologic subtypes in our cohort, the small number of cases within each group and limited clinical data precluded meaningful conclusions regarding prognostic differences. Larger species-specific studies will be required to determine whether subclassification in veterinary species has prognostic significance comparable to that described in humans.
Across species, non-cystic tubular neoplasms posed the greatest diagnostic difficulty, overlapping with benign biliary proliferations, DPMs, and neuroendocrine tumors. Neuroendocrine tumors frequently had pseudoglandular patterns that were indistinguishable from well-differentiated CCA, underscoring the necessity of synaptophysin or other neuroendocrine markers to resolve cellular lineage. Metastatic adenocarcinomas from pancreaticobiliary or gastrointestinal tracts had tubular and infiltrative features nearly identical to primary hepatic CCA, reinforcing the importance of lesion distribution in classification.
The recurring decision points highlighted in our diagnostic flowchart, such as mass effect, cystic vs. solid architecture, and immunohistochemical markers (cytokeratin, synaptophysin), formed the basis for a structured diagnostic flowchart. The flowchart is intended as a structured interpretive aid rather than a definitive classification algorithm. Although descriptive, this framework is intended to promote a more consistent interpretation of proliferative biliary lesions across species.
Several limitations warrant consideration. Our small, taxonomically diverse caseload limits species-specific conclusions regarding behavior, prognosis, or grading schemes. IHC interpretation was also constrained in non-mammalian species because of variable antibody cross-reactivity. Ancillary testing, such as expanded IHC panels or ultrastructure evaluation, may be considered, if available, to further evaluate lineage differentiation. Moreover, we did not assess interobserver agreement nor formally validate the diagnostic flowchart, both of which will require larger, more homogeneous datasets.
Within these constraints, we identified shared diagnostic features and pitfalls that complicate interpretation of biliary proliferations. Together, our findings emphasize the comparative value of biliary tumors, particularly given the rarity of CCA in most veterinary species. By organizing recurring decision points into a structured approach, we offer a practical foundation upon which future comparative and species-focused investigations may build.
Supplemental Material
sj-pdf-1-vdi-10.1177_10406387261450615 – Supplemental material for Interspecies comparative features of cholangiocarcinoma and histologic mimics
Supplemental material, sj-pdf-1-vdi-10.1177_10406387261450615 for Interspecies comparative features of cholangiocarcinoma and histologic mimics by Katti R. Crakes, Hannah M. Stephen, Kiyoko Oshima, John G. Trupkiewicz, Eunju April Choi and Cory Brayton in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank the Molecular & Comparative Pathobiology (MCP) post-doctoral fellows and Research Animal Resources (RAR) at Johns Hopkins University, as well as the Maryland Zoo in Baltimore, for their invaluable contributions to the pathology cases included in our study. Special thanks to Shana Lee (JHU) for the preparation of histologic samples, and the Cornell Animal Health Diagnostic Center and UC Davis Veterinary Medical Teaching Hospital Histology Laboratory for contributions to the IHC stains integral to the diagnostic workup.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.