
Abstract
Horse racing has faced increased scrutiny because of concerns about equine welfare and the safety of both equine and human participants. Sudden death (SD) in racehorses is relatively uncommon, and its causes are still unclear. Little information and considerable confusion exist regarding the clinical significance of microscopic lesions in the hearts of horses with SD. We examined the hearts of 29 horses that suffered exercise-associated sudden cardiac death (EASCD) and 29 clinically healthy control horses that were euthanized because of catastrophic musculoskeletal injuries. Acute cardiomyocyte injury (ACI) was found at a significantly higher overall prevalence and with a significantly higher severity score in the left atrial appendage in horses with EASCD than in control horses. ACI may be a very early stage of cardiomyocyte degeneration, perhaps driven by myocardial ischemia during high-intensity exercise. We found no significant differences in the prevalence, severity, and distribution of inflammation, fibrosis, or miscellaneous lesions between the 2 groups. Inflammation, fibrosis, and miscellaneous lesions in the heart may have clinical significance in individual cases, but they can also be confounding background lesions. Postmortem confirmation of sudden cardiac death (SCD) remains difficult, given that fatal arrhythmias can occur with no associated microscopic cardiac lesions. Elevated hepatic cobalt concentrations were overrepresented in SCD horses. Toxicology results for other performance-enhancing drugs or xenobiotics were negative or inconclusive.
Keywords
In recent years, horse racing has faced increased scrutiny regarding equine welfare and safety concerns for both equine and human participants. Sudden death (
SD of horses is usually defined as the death of a closely observed, apparently healthy animal, in which clinical signs have not been observed previously.25,26 Exercise-associated sudden death (
Several authors have investigated the possible causes of SD, EASD, and EASCD in horses.1,9,11,12,23,25,29 Studies of postmortem evaluations in horses with SD have revealed significant lesions in 30–53% of cases.23,25 Some causes of SD, EASD, or EASCD—such as major internal hemorrhages that result from a ruptured artery (including cardiac tamponade caused by aortic rupture and hemoperitoneum with severe mesenteric hemorrhage), and severe trauma to the skull or cervical vertebrae following a fall during exercise or a stable accident—are generally widely accepted as definitive causes.4,6,12,21 However, other causes, such as cardiac and/or respiratory failure or collapse, circulatory collapse, and exercise-associated pulmonary hemorrhages, are less definitive, reflect a degree of uncertainty, and have significant interinstitutional and interpersonal variability in the interpretation of gross and histologic findings.12,14,21,25,27
Depending on the study, 20–60% of cases of EASD are unexplained or presumptively attributed to SCD or EASCD, given that no significant lesions support a definitive cause of death.1,6,22,25 The consensus is that, for these “autopsy-negative” EASCD cases, a detailed standardized gross and histologic cardiac examination is essential. A postmortem examination protocol in horses with SD has been published 7 and serves as a reference to standardize postmortem examination procedures. However, published data are limited 25 regarding the prevalence and type of histologic lesions in EASCD cases and how they compare with lesions that may be present in the hearts of control horses euthanized because of severe musculoskeletal injuries. This scarcity of published scientific information poses a significant challenge for pathologists attempting to interpret microscopic lesions in the hearts of horses that have presumably died of SCD. This lack of data is an important reason for the potentially significant interinstitutional and interpersonal variability in cardiac lesion interpretation and their possible association (or lack thereof) with SCD.
Performance-enhancing drugs are associated with SCD in human athletes and are a concern in the racehorse industry. Cobalt (
The 2 main goals of our study were 1) to identify and compare microscopic lesions in the heart of horses with EASCD and horses that were euthanized because of catastrophic musculoskeletal injuries (control group); and 2) to look for performance-enhancing drugs and other xenobiotics, including Co, that may be risk factors for SCD in horses.
Materials and methods
Case selection
Cases of racehorses with EASCD (n = 29) were identified prospectively based on clinical history through submissions to the California Horse Racing Board (
Comparison of breed, age, and sex distribution of the 29 horses in each of the exercise-associated sudden cardiac death (EASCD) and control groups.
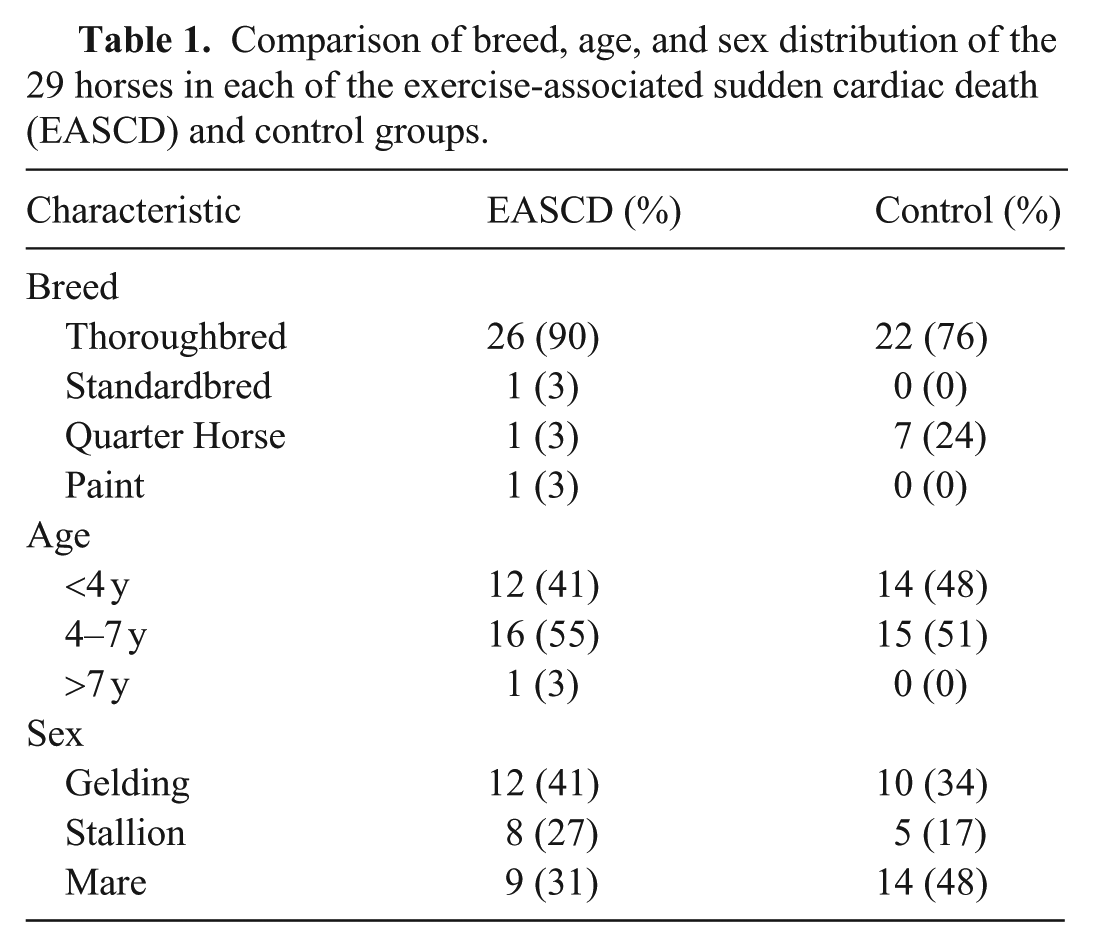
Control horses (n = 29) were prospectively selected from the same postmortem program and study period as EASCD cases (Table 1). Controls were reportedly clinically healthy horses actively training or racing that were euthanized because of catastrophic musculoskeletal injuries. This group was chosen to represent a population exposed to similar exercise intensity, management practices, and regulatory oversight as EASCD cases, while providing a definitive non-cardiac cause of death. Cases and controls were matched by total number to allow balanced comparisons; demographic variables were not used as matching criteria. All 29 control horses underwent complete gross and histologic cardiac examination using the same standardized postmortem and cardiac histology protocol applied to the EASCD group.
General postmortem and cardiac histopathology protocol
An EASD standardized postmortem and cardiac examination protocol 7 was followed in both the EASCD and control groups. Briefly, an autopsy was performed, and samples from lungs, liver, kidneys, spleen, adrenal gland, gastrointestinal tract, and brain, along with 11 standardized sections of the heart ( Table 2 ), were collected and fixed by immersion in 10% buffered formalin (pH 7) for at least 24 h for histopathology.
Eleven histologic sections of the heart obtained routinely as part of the cardiac histology protocol in exercise-associated sudden cardiac death and control groups. 7
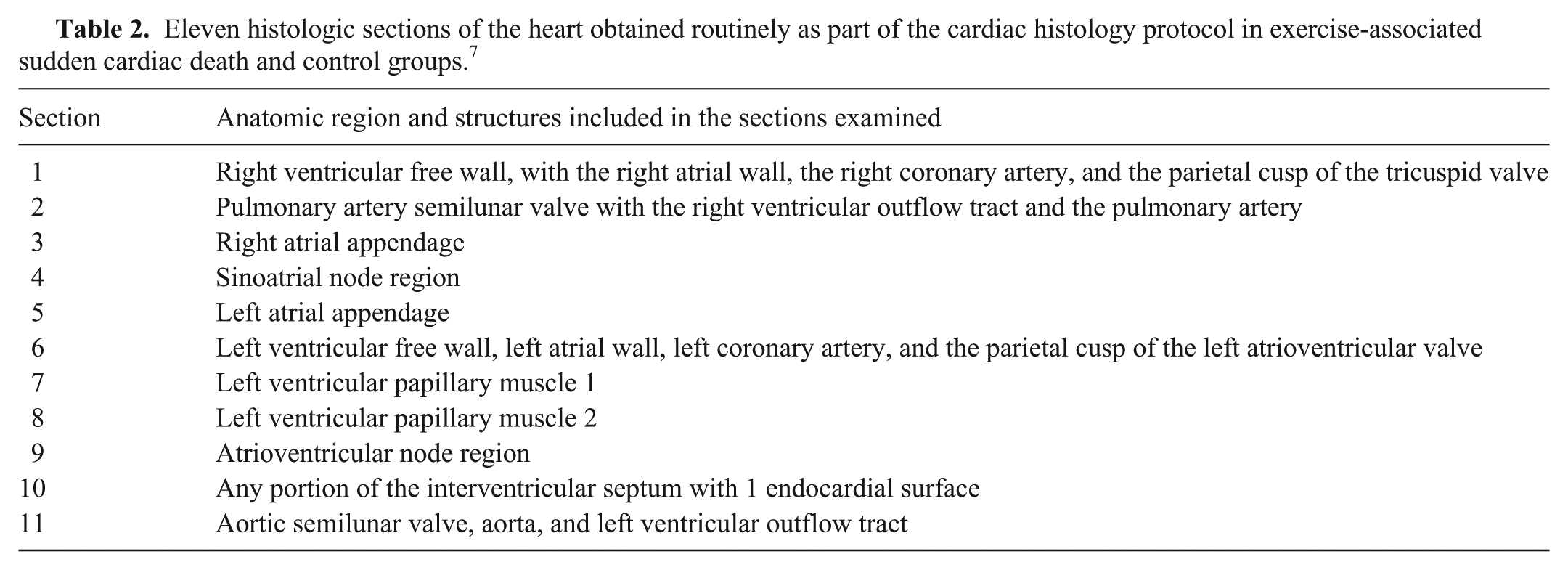
Myocardium from the right and left ventricular walls and interventricular septum, right and left atrial appendages, part of the conduction system (atrioventricular [AV] and sinoatrial [SA] nodes), the origins of the aorta and pulmonary artery, the tricuspid, aortic, and pulmonic valves were examined.
Histology of the heart, lesion classification, and severity scoring
The 11 histologic sections from the heart of each of the 29 horses in the EASCD group and the 29 horses in the control group were reviewed by 2 independent veterinary pathologists (pathologists 1 and 2) for the presence or absence of lesions in the myocardium, endocardium, epicardium, valves, AV and SA node regions, and blood vessels, and lesions were classified and severity scored. Pathologists 1 (F Giannitti) and 2 (S Diab) reviewed all of the heart slides (n = 638) from both groups individually, and each pathologist recorded the lesion category and severity (when present) for all the slides. The results from both pathologists were then compared, and discrepancies—primarily reflecting lesions recorded by one pathologist and not identified by the other—were reviewed again on the original glass slides by pathologist 2 using the same predefined morphologic criteria. Following re-examination, the recorded results were updated to confirm lesion presence or absence. This process was intended to ensure consistent lesion documentation rather than to assess interobserver agreement or assign clinical significance.
The lesions were classified into 4 major categories: 1) acute cardiomyocyte injury (
Lesion histologic scoring was determined as follows. A score of 0 was given to a slide if no lesion was present. A severity grade of 1–3 was assigned to each slide with ACI, inflammation, and fibrosis. A score of 1 (mild) indicated lesions that were small, either focal or multifocal, but infrequent; a score of 2 (moderate) indicated lesions that were small, multifocal, and frequent, or larger, focal or multifocal, but not frequent; a score of 3 (severe) indicated lesions that were large and focal, or small-to-mid-size, but very frequent. A total severity score for ACI, inflammation, and fibrosis in each horse was obtained by adding the individual slide severity score from all slides with that lesion. The miscellaneous lesion subcategories were recorded, but a severity score was not assigned using a standardized grading scheme for each slide because this category included infrequent, heterogeneous lesions with differing and often unclear biological significance. These lesions were recorded for descriptive completeness and were not used for hypothesis testing, summed severity analyses, or to infer clinical significance. Instead, the presence of a miscellaneous lesion was scored as 1 if the lesion was subjectively recorded as mild, as 2 if it was scored as moderate, and as 3 if it was recorded as severe.
Toxicology screening
Samples from horses with EASCD and from control horses were collected and submitted to test for performance-enhancing drugs, other potential toxicants, and to screen for Co to evaluate a possible association between high levels of performance-enhancing drugs, Co, and EASCD. All horses included in toxicology testing were drawn from the same California racehorse population and met the same case or control definitions as those used for the pathology examination cohort. The toxicology cohort partially overlapped with the pathology cohort, in that some horses underwent both pathology and toxicology evaluation, whereas others were included only in the toxicology analysis. In the EASCD group, 7 of 29 horses with lesions had one or more toxicology assays performed, whereas in the control group, 6 of 29 horses with lesions had one or more toxicology assays performed. For each toxicology assay, ~12–13 additional horses per group were included exclusively in the toxicology analysis without corresponding pathology evaluation. Unless otherwise noted, all testing was performed at the California Animal Health and Food Safety Laboratory, Toxicology Section (Davis, CA, USA), following standard operating procedures.
Frozen (−20°C) liver samples from 19 EASCD and 10 control horses were submitted for element testing by inductively coupled plasma–optical emission spectroscopy (ICP-OES). These elements included lead (Pb), manganese (Mn), iron (Fe), mercury (Hg), molybdenum (Mo), zinc (Zn), copper (Cu), and cadmium (Cd). Inductively coupled plasma–mass spectrometry (ICP-MS) was used to test arsenic (As) and selenium (Se). Co was tested in 18 EASCD and 10 control horses. The RI for Co was adapted by dividing the published RI, 34 expressed in mg/kg of dry weight, by 3.3 to obtain an estimated RI expressed in mg/kg of wet weight, assuming a liver moisture content of 70%. The reporting limits of detection for each element were: Pb (1 ppm), Mn (0.1 ppm), Fe (1 ppm), Hg (1 ppm), Mo (0.4 ppm), Zn (0.3 ppm), Cu (0.3 ppm), Cd (0.3 ppm), Se (0.020 ppm), As (0.050 ppm), and Co (0.010 ppm).
Frozen (−20°C) liver samples from 17 EASCD and 10 control horses were submitted for non-targeted testing by gas chromatography–mass spectrometry (GC-MS) and liquid chromatography–mass spectrometry (LC-MS), designed to detect a large number of organic compounds of diverse chemical classes (pesticides, environmental contaminants, drugs, and natural products). Frozen (−20°C) liver samples from 19 EASCD and 10 control horses were screened by LC-MS for anticoagulants, including brodifacoum, bromadiolone, chlorophacinone, coumachlor, difethialone, diphacinone, warfarin, and difenacoum.
Statistical analysis
The presence (prevalence) of each cardiac lesion (ACI, myocarditis, endocarditis, epicarditis, valvulitis, myocardial fibrosis) was compared between the EASCD (n = 29) and control (n = 29) groups using chi-squared testing (or Fisher exact testing for cell counts <5). Total severity scores (sum of ACI, inflammation, and fibrosis severity scores across all cardiac sections) and lesion-specific severity scores were compared between groups using the Kruskal–Wallis rank test (Stata SE v.17.0; StataCorp). For any cardiac lesion in which the global presence and/or severity score differed significantly between EASCD and control groups, lesion-specific severity scores were compared between groups for each cardiac slide using Wilcoxon rank-sum testing. Within each group (EASCD and control), the distribution (presence or absence) of each cardiac lesion (ACI, myocarditis, endocarditis, epicarditis, valvulitis, myocardial fibrosis) across the 11 cardiac slides examined was assessed using Fisher exact testing. The type of inflammatory infiltrate (lymphocytes, lymphocytes + plasma cells, lymphocytes + macrophages, lymphocytes + plasma cells + macrophages, macrophages, lymphocytes + neutrophils, lymphocytes + macrophages + eosinophils, lymphocytes + macrophages + neutrophils, neutrophils) was compared using chi-squared testing (or Fisher exact test) between the EASCD and control groups. Type of inflammatory cell population was included to provide contextual information regarding lesion chronicity and potential pathogenesis; however, interpretation was limited by the unknown interval between any inciting event and tissue examination, the largely nonspecific nature of these infiltrates, and the absence of clinical or postmortem findings supporting an alternative underlying or predisposing, clinically significant disease process. Similarly, the prevalence of combinations of cardiac lesion categories (more than one of the following lesion categories: ACI, inflammation, fibrosis, and miscellaneous) was compared using chi-squared (or Fisher exact test) between EASCD and control groups.
Results
Histology of the heart, lesion classification, and severity scoring
Acute cardiomyocyte injury was the only lesion that was significantly (p = 0.04) more prevalent in EASCD horses (18 of 29; 62%) than in control horses (10 of 29, 34%;
Total scores for each major cardiac lesion category, added scores for major lesion categories, and presence and severity of miscellaneous lesions in the 29 exercise-associated sudden cardiac death horses.
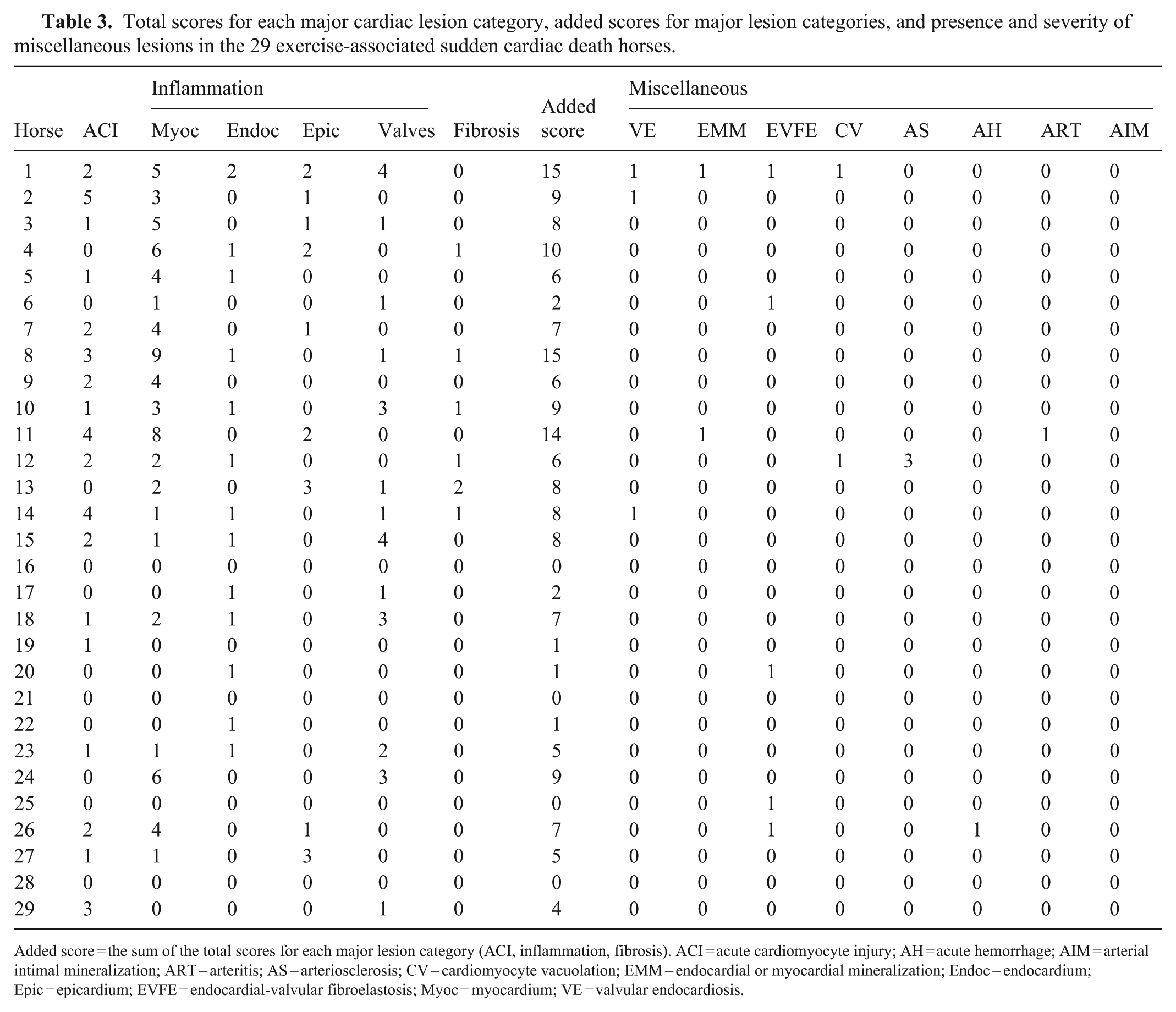
Added score = the sum of the total scores for each major lesion category (ACI, inflammation, fibrosis). ACI = acute cardiomyocyte injury; AH = acute hemorrhage; AIM = arterial intimal mineralization; ART = arteritis; AS = arteriosclerosis; CV = cardiomyocyte vacuolation; EMM = endocardial or myocardial mineralization; Endoc = endocardium; Epic = epicardium; EVFE = endocardial-valvular fibroelastosis; Myoc = myocardium; VE = valvular endocardiosis.
Total scores for each major cardiac lesion category, added scores for major lesion categories, and presence and severity of miscellaneous lesions in the 29 control horses.
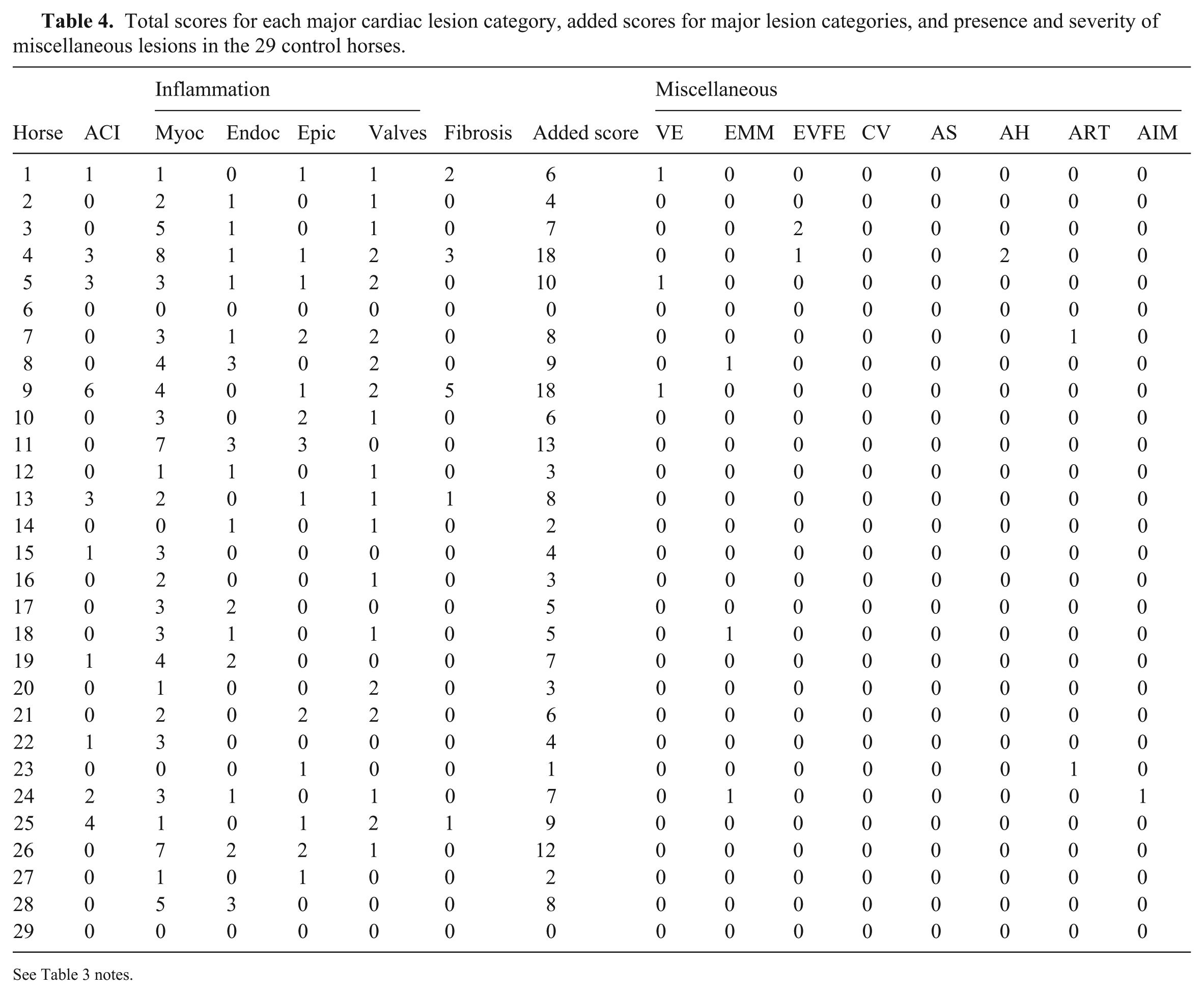
See Table 3 notes.
Comparison of the prevalence of each major lesion category (excluding miscellaneous lesions) in 29 exercise-associated sudden cardiac death (EASCD) and 29 control horses.
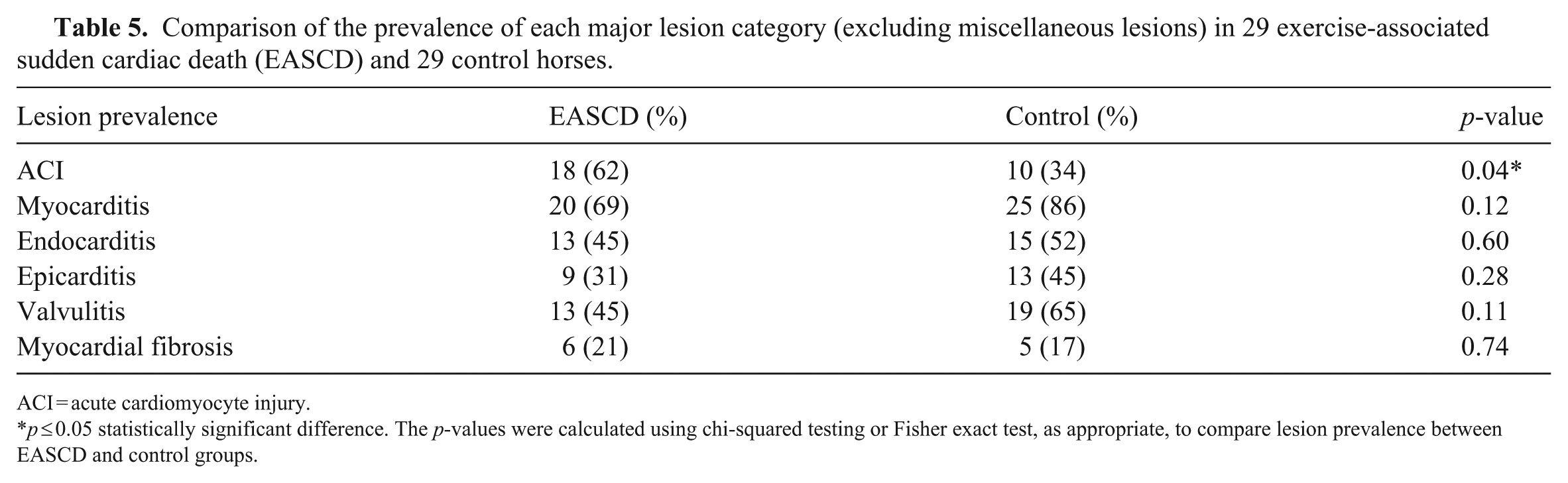
ACI = acute cardiomyocyte injury.
p ≤ 0.05 statistically significant difference. The p-values were calculated using chi-squared testing or Fisher exact test, as appropriate, to compare lesion prevalence between EASCD and control groups.

Major histologic lesion categories (acute cardiomyocyte injury [ACI], inflammation, and fibrosis) in the hearts of horses in the exercise-associated sudden cardiac death (EASCD) and control groups. H&E.
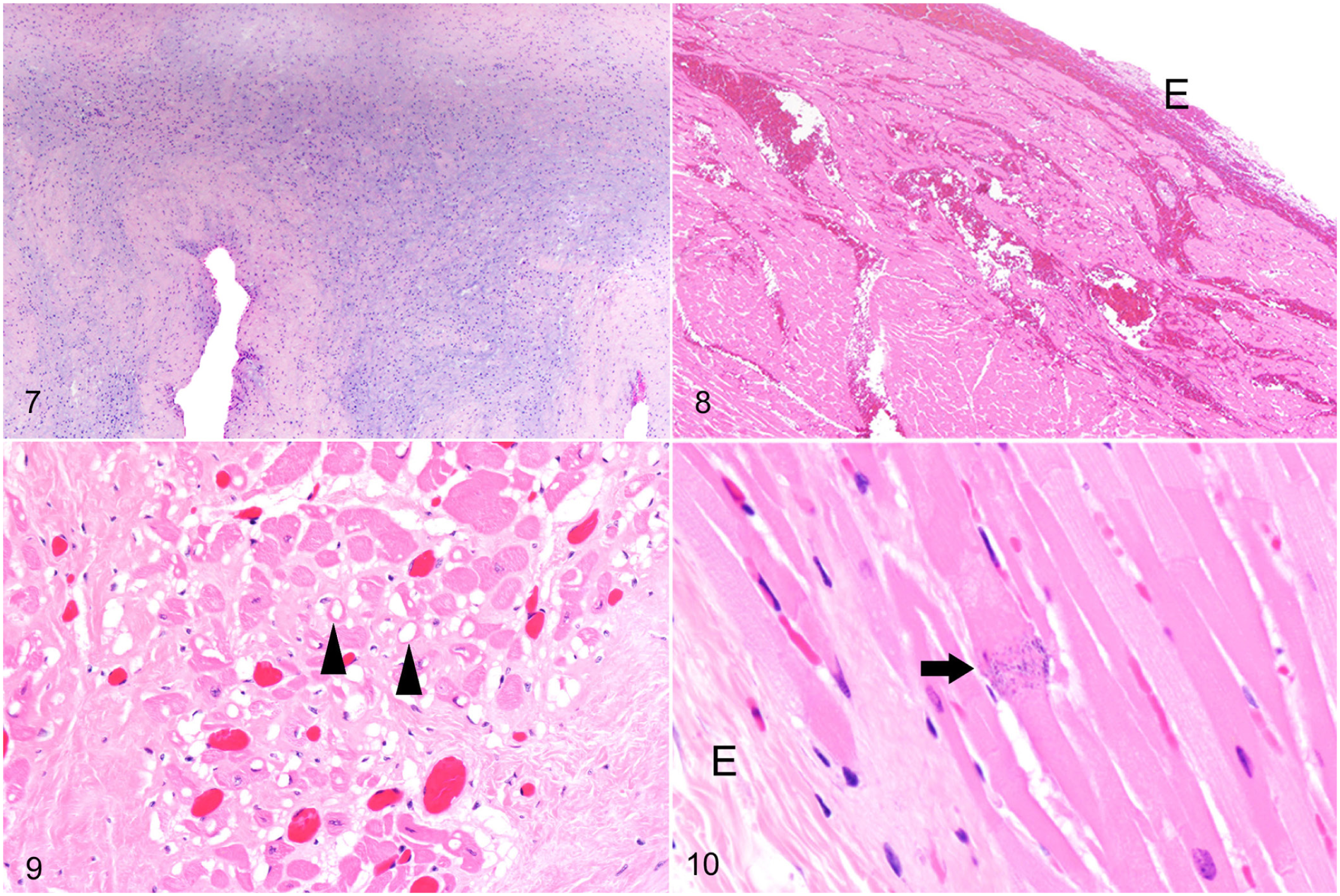
Histologic lesions in the hearts of horses in the exercise-associated sudden cardiac death (EASCD) and control groups. H&E.
The total severity scores did not differ significantly or by specific lesion type between the EASCD and control groups ( Table 6 ). When comparing the severity score for ACI by specific regions, only the left atrial appendage (slide 5 of the cardiac histology protocol) had significantly higher severity in EASCD horses compared with control horses (p < 0.01).
Comparison of overall and lesion-specific total severity scores (excluding miscellaneous lesions) in the 29 exercise-associated sudden cardiac death and 29 control horses.
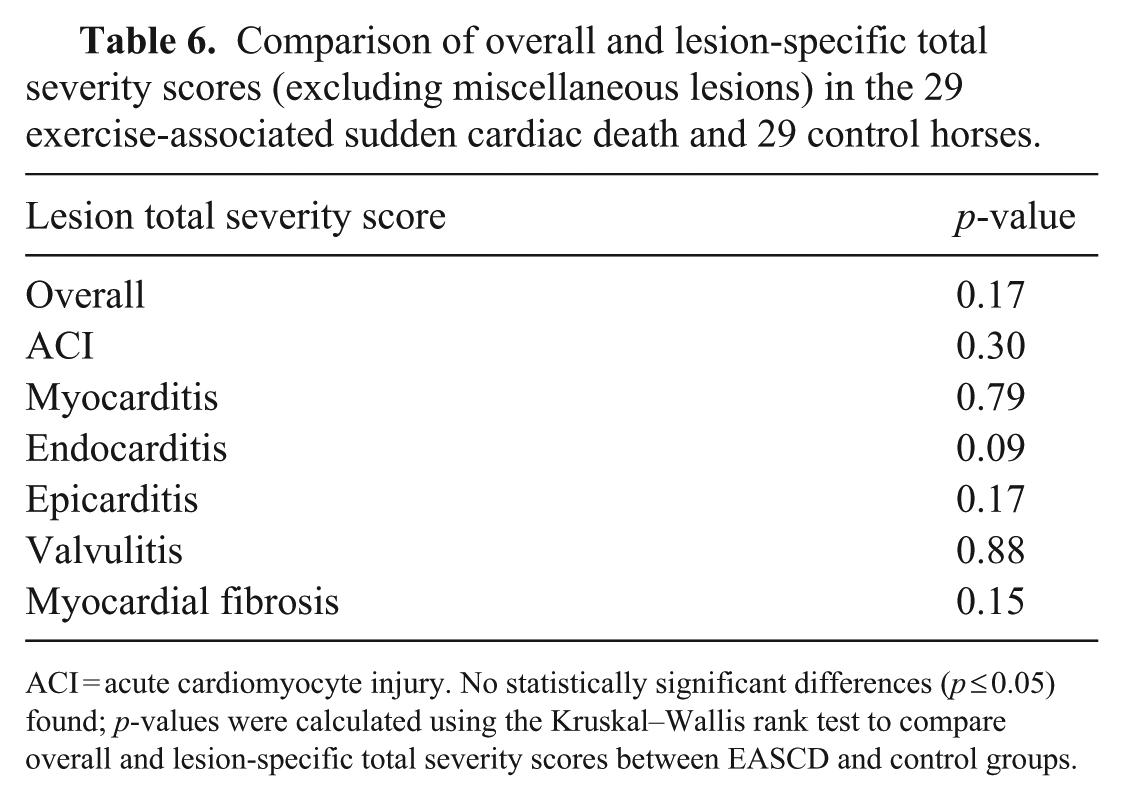
ACI = acute cardiomyocyte injury. No statistically significant differences (p ≤ 0.05) found; p-values were calculated using the Kruskal–Wallis rank test to compare overall and lesion-specific total severity scores between EASCD and control groups.
Analysis of control horses likewise identified significant regional variation in the distribution of histologic lesions involving ACI, endocarditis, and valvulitis. In addition, epicarditis had significant regional variation only in control horses, whereas myocardial fibrosis had significant regional variation only in the EASCD group. ACI was most frequent in the left atrial appendage (section 5, 10 of 29, 34%) and left ventricular papillary muscle number 1 (section 7, 7 of 29, 24%). Endocarditis was most frequent in the left ventricular outflow tract (section 11, 5 of 29, 17%). Valvulitis was most frequent in the pulmonic semilunar valve (section 2, 7 of 29, 24%), followed by the left atrioventricular valve (section 6, 5 of 29, 17%) and aortic semilunar valve (section 11, 9 of 29, 31%). Myocardial fibrosis was most frequent in the right ventricular outflow tract (section 2, 3 of 29, 10%).
Within control horses, the distribution of histologic lesions differed significantly across cardiac regions for ACI, endocarditis, epicarditis, and valvulitis. ACI was most frequent in the left ventricular papillary muscle number 1 (section 7, 5 of 29, 17%) and left ventricular papillary muscle 2 (section 8, 7 of 29, 24%). Endocarditis was most frequent in the left ventricular papillary muscle 1 (section 7, 8 of 29, 41%). Epicarditis was most frequent in the right ventricular free wall (section 1, 8 of 29, 28%). Valvulitis was most frequent in the pulmonic semilunar valve (section 2, 5 of 29, 17%), left atrioventricular valve (section 6, 5 of 29, 17%), and aortic semilunar valve (section 11, 12 of 29, 41%).
No significant differences in the proportion of horses with myocarditis, endocarditis, epicarditis, and/or valvulitis and type of inflammatory cell infiltrate were identified between the EASCD and control groups ( Table 7 ). Similarly, no significant differences in combinations of cardiac lesion categories were identified between the EASCD and control groups ( Table 8 ).
Prevalence of myocarditis, endocarditis, epicarditis, and/or valvulitis and type of inflammatory cells in 29 exercise-associated sudden cardiac death (EASCD) and 29 control horses.
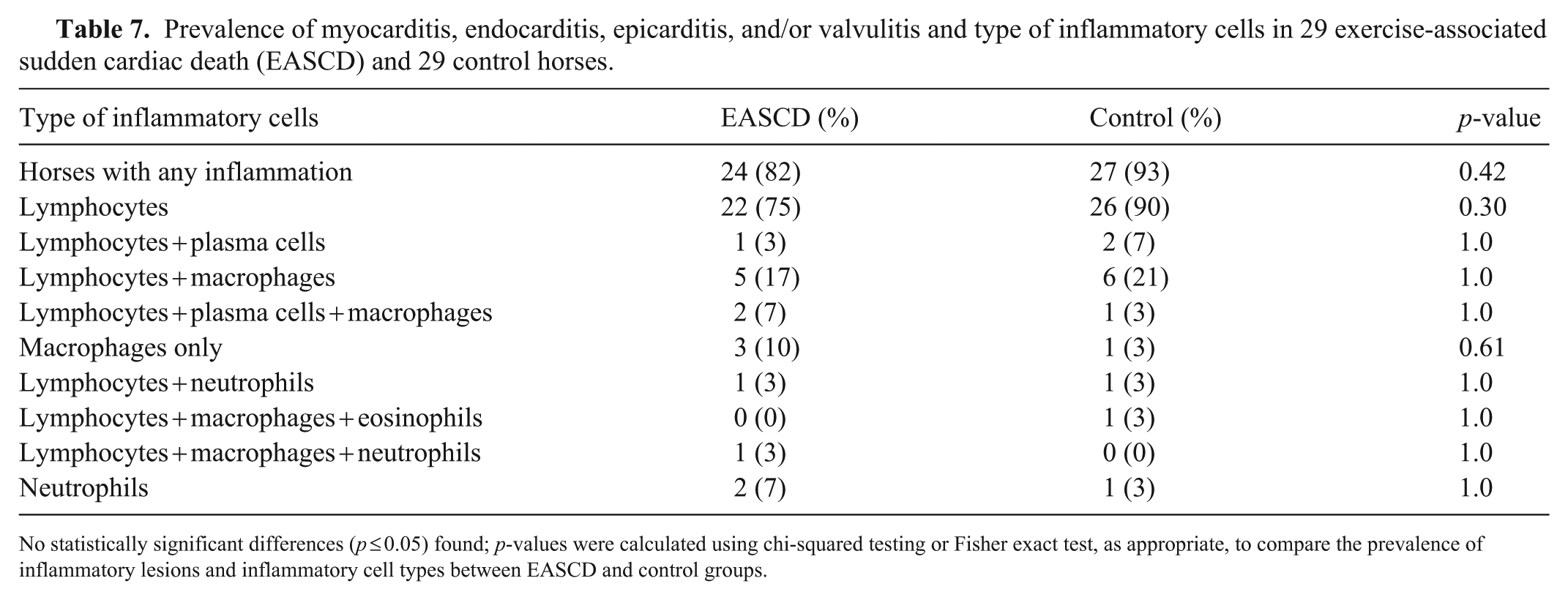
No statistically significant differences (p ≤ 0.05) found; p-values were calculated using chi-squared testing or Fisher exact test, as appropriate, to compare the prevalence of inflammatory lesions and inflammatory cell types between EASCD and control groups.
Prevalence of lesion type combinations in the 29 exercise-associated sudden cardiac death and 29 control horses.
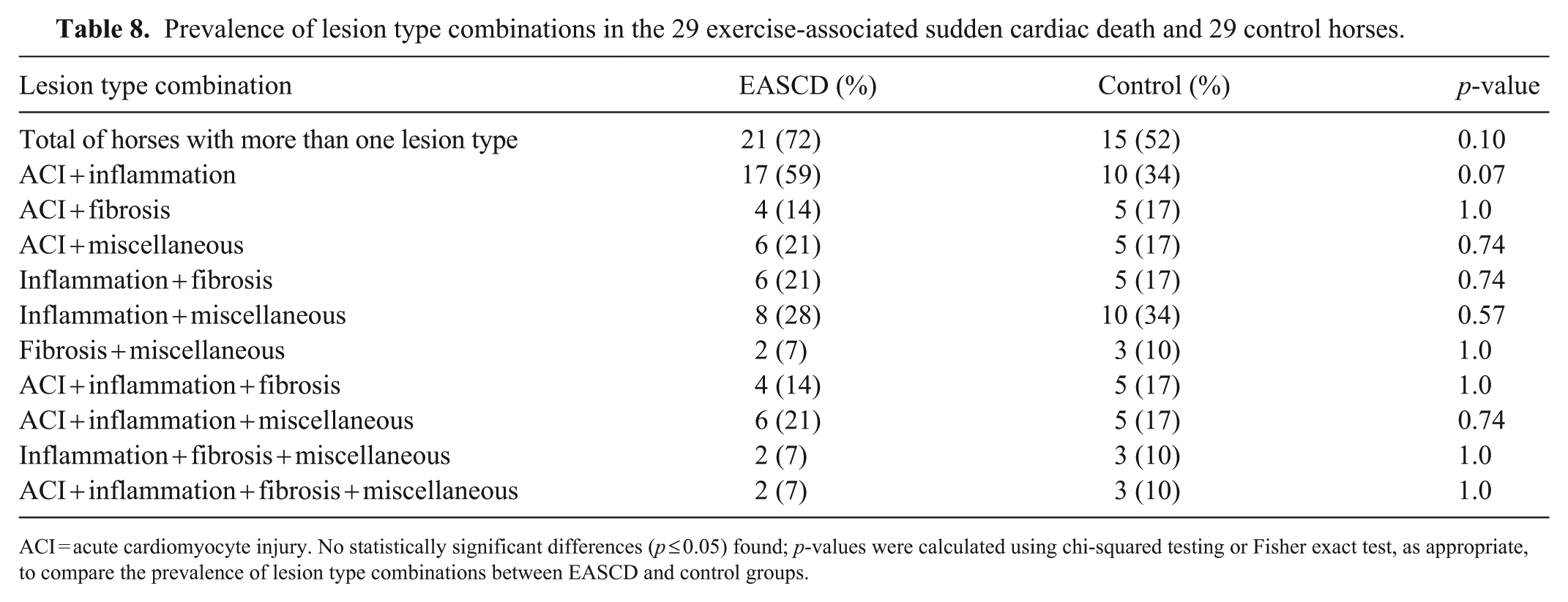
ACI = acute cardiomyocyte injury. No statistically significant differences (p ≤ 0.05) found; p-values were calculated using chi-squared testing or Fisher exact test, as appropriate, to compare the prevalence of lesion type combinations between EASCD and control groups.
Toxicology
For the extended heavy metal screen and selenium tests, 17 of 19 EASCD and 8 of 10 control horses had mineral concentrations within RIs, 1 EASCD and 2 control horses had low zinc, and 1 EASCD horse had low selenium. Co was below the RI in 4, above the RI in 5, and within the RI in 9 of the 18 EASCD horses and within the RI in 7 and below the RI in 3 of the 10 control horses evaluated (
No toxic compounds were detected in any of the 17 EASCD or 10 control horses tested by GC-MS. The anticoagulant screen was negative in 16 of 19 EASCD and 6 of 10 control horses evaluated. Trace amount of brodifacoum anticoagulant was detected in 3 EASCD and 3 control horses, and a trace amount of diphacinone was detected in 1 control horse.
Discussion
Our first goal was to identify and compare microscopic lesions in the hearts of horses with EASCD and horses that were previously healthy but euthanized because of catastrophic musculoskeletal injuries (control group). Twenty-seven horses from each group had at least one of the major lesion categories established (ACI, inflammation, fibrosis, or miscellaneous lesions). However, the only lesion category that was significantly more prevalent in EASCD horses compared with the control horses was ACI, which was observed in 18 (62%) EASCD horses and 10 (34%) control horses.
Severity scores did not differ overall or by specific lesion between case and control groups. However, comparing the severity scores for specific regions among the EASCD and control groups, the ACI score was significantly higher in the left atrial appendage of the EASCD group. The ACI observed mainly in the left atrial appendage and left ventricular papillary muscles required careful examination of histologic sections at 100× or 200× magnification. This injury was segmental hypo- and/or hypereosinophilia, loss of cross striations, segmental narrowing or widening, and formation of hypercontraction bands, with normal nuclei. In the human literature, morphologically similar changes have been described in ACI as myofibrillar degeneration 30 and myocytolysis 24 and are associated primarily with ischemic injuries. However, these lesions also may result from non-ischemic causes, such as catecholamine-induced injury, myocarditis, massive release of cytokines (as in sepsis), toxic myocardial injuries, and others.8,24,30 We hypothesize that, in EASCD cases, this morphologic alteration may be a very early stage of cardiomyocyte injury, perhaps driven by myocardial ischemia and/or a surge of catecholamines during high-intensity exercise or severe stress, as could be experienced in horses with catastrophic musculoskeletal injuries before they are euthanized. Anecdotal evidence collected from pathologists who were consulted about this lesion suggests that this acute morphologic alteration of cardiomyocytes could also be induced by euthanasia or appear in the agonal stage just before death. Additional morphologic studies using a combination of histopathology, histochemistry, immunohistochemistry, and ultrastructure are required to better characterize this acute cardiomyocyte alteration in horses.
At elevated heart rates, diastole shortens disproportionately compared with systole, decreasing the time for coronary perfusion, which primarily occurs during diastole. 13 Thus, even in structurally normal hearts, excessively high heart rates can reduce myocardial perfusion time below a critical threshold, leading to transient ischemia, myocardial dysfunction, and mechanical inefficiency. 16 The left ventricle relies more on diastolic coronary blood supply than does the right ventricle and, therefore, is more susceptible to ischemia at elevated heart rates. 10 Additionally, subendocardial blood flow decreases as the heart rate rises, compromising oxygen delivery to this area of the heart.13,16 ACI in our study was observed at the highest prevalence in the left atrial appendage and subendocardial cardiomyocytes of the left ventricular papillary muscles in the EASCD group and in subendocardial cardiomyocytes of the left ventricular papillary muscles in the control group, which supports the hypothesis of an ischemic origin to this lesion. In humans, myocardial ischemia can lead to loss of function almost immediately (within 1–2 min), and contraction band necrosis can be seen as early as 10 min after the onset of acute injury.24,32 The use of a total severity score incorporates both lesion severity and distribution across cardiac sections, which may give more weight to multifocal mild lesions than to isolated severe lesions. However, this approach did not result in increased statistical significance in comparisons between EASCD and control groups.
In humans, the mechanism of SCD is often a lethal arrhythmia, and even when the original cause was ischemic heart disease, enzymatic, electrocardiographic, or morphologic evidence of myocardial necrosis may not be found in people who suffer SCD but are successfully resuscitated. 32 Therefore, it seems likely that myocardial ischemia during high-intensity exercise in racehorses could lead to fatal arrhythmias that leave no histologic evidence of ACI.
We found no significant differences in the prevalence of the other 3 major lesion categories (inflammation, fibrosis, miscellaneous) between EASCD and control horses, and severity scores did not differ significantly for inflammation and fibrosis. Hence, inflammation, fibrosis, and the various miscellaneous lesions were not consistently more prevalent in horses with EASCD than in healthy control horses and are essentially “background” lesions in horses dying of non-cardiac causes. Our data highlight how difficult it is to associate these lesions as the possible cause of SCD. Therefore, pathologists must be careful not to overinterpret the clinical significance of microscopic cardiac lesions in EASCD cases.
A limitation of our study is that discrepancies in lesion detection were resolved by a single pathologist, which may introduce observer-related bias. However, discrepancies primarily reflected subtle lesions recorded by one pathologist and not identified by the other, rather than differences in lesion classification or severity grading. Lesions were documented using predefined morphologic criteria, clinical significance was intentionally not assigned, and both EASCD and control hearts were examined using the same standardized protocol. Given the descriptive nature of our study and the identical evaluation of cases and controls, any residual observer-related bias is unlikely to have systematically affected the comparative findings.
Most of the miscellaneous lesions described in our study were mild and, therefore, we believe likely incidental or of unclear clinical significance. However, miscellaneous lesions encompass a wide variety, and they should be assessed and interpreted on a case-by-case basis. For example, it could be argued that arteriosclerosis was the cause of death in EASCD case 12, given that thickened arterial walls and narrowing of the arterial lumen may lead to ischemia of the myocardium. Moreover, this horse had mild ACI, which, as discussed above, could be the result of an ischemic event. However, as described previously, 25 coronary arteriosclerosis can be detected in horses with SCD as well as in horses euthanized because of severe musculoskeletal injury. Therefore, coronary arteriosclerosis could be a risk factor for myocardial ischemia during high-intensity exercise, but it is also found in horses euthanized because of severe musculoskeletal injuries. Arteriosclerosis was not found in any of the control horses in our study.
When comparing horses that had >1 type of major lesion category (e.g., ACI + acute inflammation or inflammation + fibrosis), we found no statistically significant differences between the EASCD group (21 horses; 72%) and the control group (15 horses; 52%). Therefore, no association was established between a certain combination of lesions and EASCD cases. The clinical significance of a given combination of lesions in the heart needs to be evaluated on a case-by-case basis, considering lesion type, frequency, and severity.
The data regarding the distribution of inflammation and fibrosis do not give clear insight into the cause or pathogenesis of EASCD cases but serve as a baseline to build upon. Microscopic heart lesions are often mild and multifocal and, although not exhaustive, the cardiac examination protocol that we used offers a standardized, practical, and cost-effective approach for systematic evaluation of key cardiac regions. 7 However, even when no abnormalities are detected in the 11 sections of heart included in the protocol, the presence of lesions in unexamined areas cannot be ruled out. Given the large size of the equine heart, the proportion of myocardium evaluated histologically represents only a small fraction of the total organ, which further limits lesion detection unless changes are relatively widespread or involve preferentially sampled regions. This limitation is yet another challenge that veterinary pathologists face when attempting to determine risk factors for, or the cause of, EASCD, given that the presence of lesions does not necessarily imply a functional cardiac impairment, and their absence in the sampled sections does not exclude lesions elsewhere in the heart.
Depending on frequency, severity, and distribution throughout the heart, ACI, inflammation, fibrosis, and miscellaneous lesions may have clinical relevance in individual cases of SCD, but they can also be confounding lesions unrelated to the cause of SCD. For example, horses 1 and 8 had the highest total severity score (15) for ACI, inflammation, and fibrosis in the EASCD group. In addition, horse 1 had a score of 1 for each one of the following miscellaneous lesions: valvular endocardiosis, endocardial or myocardial mineralization, and cardiomyocyte vacuolation. However, the highest total severity score for ACI, inflammation, and fibrosis in all horses included in this study (18) was found in control horses 4 and 9. Horse 4 also had a score of 1 for endocardial or valvular fibroelastosis, and a score of 2 for acute subendocardial and myocardial hemorrhage; horse 9 also had a score of 1 for valvular endocardiosis.
Our results demonstrate the difficulty of establishing a causal relationship between microscopic lesions in the heart and EASCD cases. This conclusion is further supported by the collective pathology experience of the authors. Therefore, contrary to a previous study, 25 we abstained from assigning clinical significance to the lesions observed in the EASCD group. Instead, we compared the lesion prevalence, lesion types, and their total severity scores between the EASCD and control groups.
Our second goal was to identify illegal performance-enhancing drugs and other xenobiotics that may be risk factors for SCD in horses and to screen for Co to evaluate their possible role in SCD. Within the limits of the analytical procedures performed, no toxic compounds were detected in any of the 17 EASCD and 10 control horses tested by GC-MS, and no illegal or banned drugs were found in the urine or aqueous humor in all 8 EASCD and control horses tested according to the Horseracing Integrity and Safety Authority and the CHRB list of banned or prohibited substances. Despite these negative results, it is imperative to include toxicology testing for all equine athletes succumbing to EASCD that are submitted for autopsy.
The extended heavy metal screen and selenium tests were largely within RIs in both groups. Only 1 horse from the EASCD and 2 horses from the control groups had a low zinc concentration, and 1 horse from the EASCD group had a low selenium concentration. Therefore, we did not find heavy metal or selenium abnormalities that could be associated with (or be risk factors for) EASCD in these groups of horses. We also recommend that an extended heavy metal and selenium screen be performed in all autopsy investigations of EASCD cases.
Trace amounts of anticoagulants were found in 3 EASCD horses and 4 control horses. Anticoagulants have been associated with SD or EASD in horses with massive hemoperitoneum. 4 In the absence of significant internal bleeding, finding trace amounts of anticoagulants in the liver of horses with SCD or EASCD is probably of no clinical significance. Potential sources of anticoagulants include environmental exposure (e.g., ingestion of anticoagulant rodenticides), contamination of feed or feed storage areas, or exposure to residues from the stable environment. We recommend testing for anticoagulants in those cases in which internal bleeding is considered an important postmortem finding.
Hepatic Co above the RI was present in 5 of 18 EASCD horses and in 0 of 10 controls. Our data support an association between elevated hepatic Co and SCD in racehorses, but do not establish a hepatic overdose threshold or causality. Our results justify continued surveillance of Co in fresh tissue samples on racehorses submitted for autopsy after SCD or EASCD. Larger prospective studies are needed to better understand the potential clinical significance of high Co in the livers of these horses. In humans, the administration of Co stimulates RBC synthesis and has been used as treatment for anemia. Additionally, elemental Co activates the erythropoietin (EPO) gene, increasing hemoglobin and RBC synthesis, which had led to the suspicion that Co may be used as a performance-enhancing drug in human athletes. 2 Administration of high amounts of Co in humans is associated with a risk of toxicosis; adverse reactions include nausea, vomiting, heart failure, hypothyroidism, and goiter.2,17 Cobalt-associated cardiomyopathy in people has been described in cases of markedly elevated systemic exposure, such as with metal-on-metal hip prostheses or historical consumption of Co-containing beer (in which Co salts were used as foam stabilizers), often accompanied by multisystemic clinical signs and severe myocardial dysfunction. 31 In horses, a study on Co administration did not show an effect on EPO or red blood cell parameters or other adverse effects. 18 Experimental intravenous administration of CoCl2 to horses has resulted in hypertension and arrhythmia, which raise animal welfare and human safety concerns. 3 This concern is also shared by some of the horse racing regulatory agencies, such as the CHRB, which consider the administration of Co a potential equine health and safety issue. 19 We recommend routine Co testing in postmortem investigation of SCD and EASCD.
A standardized autopsy and cardiac examination protocol, along with toxicology testing, are essential to the diagnostic investigation of cases of sudden death in racehorses. Even when the cause of death remains undetermined, systematic autopsy and toxicology establish active surveillance for potential exposure to prohibited substances and possible toxicants. Additional morphologic studies of the heart, including investigation of region- and papillary muscle–specific lesion distribution analyses, along with continued toxicology testing, genetic studies, training regimen analysis, and research on the functional physiology of the heart of equine athletes during exercise and/or immediately after exercise are necessary to better understand the pathogenesis and causes of ESCD. These studies will likely require multidisciplinary collaborations, including veterinary clinicians, epidemiologists, pathologists, toxicologists, cardiologists, trainers, and horse racing authorities. Only with a better understanding of the risk factors and pathophysiology of SCD and EASCD can evidence-based prevention and control measures be designed and implemented to reduce their incidence in racehorses.
Supplemental Material
sj-pdf-1-vdi-10.1177_10406387261451776 – Supplemental material for Comparative cardiac histopathology and toxicology screens in horses succumbing to exercise-associated sudden cardiac death and control horses
Supplemental material, sj-pdf-1-vdi-10.1177_10406387261451776 for Comparative cardiac histopathology and toxicology screens in horses succumbing to exercise-associated sudden cardiac death and control horses by Santiago S. Diab, Federico Giannitti, Ashley Hill, Jessica Morgan, Jeff A. Blea, Rick Arthur, Robert Poppenga, Susan Stover and Francisco A. Uzal in Journal of Veterinary Diagnostic Investigation
Footnotes
Acknowledgements
We thank CAHFS San Bernardino and Davis autopsy, toxicology, and histotechnology technicians for their technical support and assistance. Federico Giannitti is a member of the “Sistema Nacional de Investigadores” of the Uruguayan “Agencia Nacional de Investigación e Innovación.”
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: from the Center for Equine Health, University of California, Davis (grant 14-08).
Generative AI statement
Authors used a generative AI tool (ChatGPT, OpenAI) to assist with grammar/readability and to help identify relevant human and veterinary literature. All AI-suggested text and sources were reviewed, verified, and edited by the authors, who take full responsibility for the content.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.