
Abstract
A 10-y-old American Paint Horse mare was presented to the Equine Field Services at Virginia-Maryland College of Veterinary Medicine (Blacksburg, VA, USA) for evaluation of mastitis and a possible abscess in the right mamma. Histologic evaluation of a mammary biopsy revealed a densely cellular, infiltrative neoplasm with cells arranged in packets supported by thin stroma. In a neuroendocrine immunohistochemistry panel, the neoplastic cells did not immunolabel for neuron-specific enolase or synaptophysin, positively immunolabeled for chromogranin A, and had moderate scattered immunolabeling for S100. These findings confirmed a diagnosis of mammary neuroendocrine tumor. Although the cells also did not immunolabel for cytokeratin, we cannot rule out a neuroendocrine carcinoma. Neuroendocrine mammary neoplasms are very rare and, to our knowledge, they have not been reported previously in horses. This neoplasm should be considered as a differential diagnosis for mammary tumors in mares.
A 10-y-old American Paint Horse mare was presented to the Equine Field Services at Virginia-Maryland College of Veterinary Medicine (Blacksburg, VA, USA) with a presumptive diagnosis of mastitis and an abscess in the right mamma. Palpation of the mamma revealed a non-painful, warm, very firm, 20 × 18-cm swelling that extended through the entire right mamma, with a tract draining purulent material. Based on its location, the tract did not appear to be directly associated with the teat canal or major ducts, although involvement could not be excluded definitively. No other significant clinical abnormalities were observed.
Direct, sediment, and cytocentrifuge smears were prepared from fluid of the right mamma for cytologic analysis. Cellular content was mixed. Microbiologic aerobic culture analyses and susceptibility were inconclusive, with no growth after 3 d, and only mixed flora and no probable pathogens found in 2 separate submissions. The mare was treated with systemic trimethoprim-sulfonamide (30 mg/kg, PO, q12h). After several weeks, the swelling of the mamma was reduced, but the draining tract remained patent. A biopsy was taken, fixed by immersion in 10% neutral-buffered formalin, and processed routinely for the production of 4-µm thick H&E-stained slides.
Microscopically, the mammary gland parenchyma was effaced and replaced by a multilobular, densely cellular, infiltrative, and poorly demarcated and unencapsulated neoplasm ( Fig. 1A ). The neoplastic cells were organized into closely arranged, variably sized islands and packets of polygonal pleomorphic cells, often surrounded by thin stroma ( Fig. 1B ). The neoplastic cells had abundant, highly vacuolated eosinophilic cytoplasm. The nuclei were single, round, often central, and occasionally indented, with stippled-to-clumped chromatin. One or 2 basophilic nucleoli were evident per cell. Anisokaryosis and anisocytosis were marked within the sections analyzed. The mitotic count was 16 mitotic figures in 2.37 mm2. Most (~60%) of the neoplasm was necrotic, including the center of some of the neoplastic islands ( Fig. 1C ). Numerous neutrophils and lymphocytes were admixed with cellular debris and fibrin, and the necrotic areas were hemorrhagic.
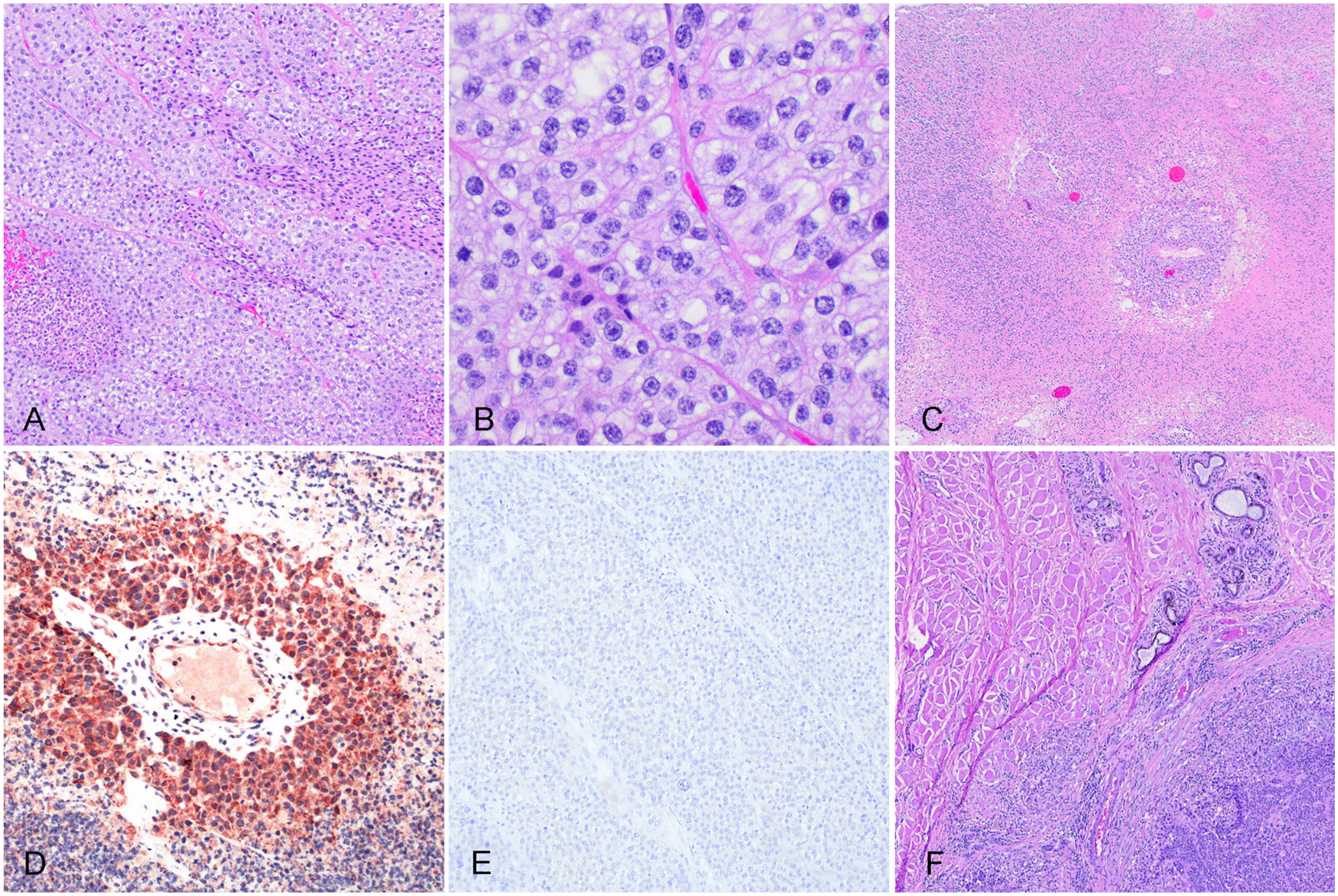
Neuroendocrine mammary neoplasm in a mare. Figure 1A–E are images from the biopsy specimen.
The histologic pattern of packets surrounded by thin fibrovascular septa raised concern for neuroendocrine differentiation. To determine if this was a neuroendocrine tumor (
Antibodies used for neoplasia characterization.
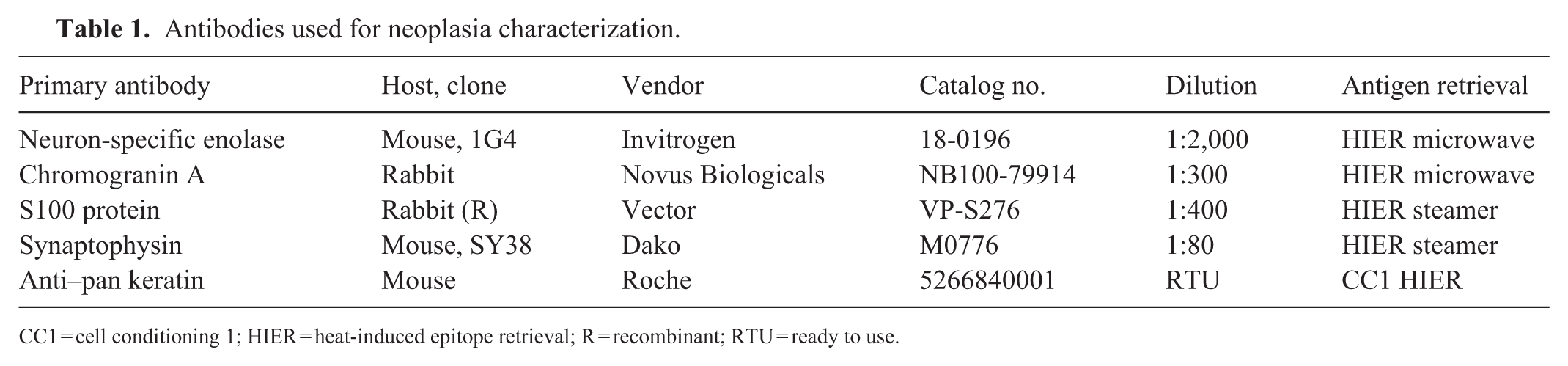
CC1 = cell conditioning 1; HIER = heat-induced epitope retrieval; R = recombinant; RTU = ready to use.
Neoplastic cells had moderate-to-strongly positive cytoplasmic immunolabeling for chromogranin A ( Fig. 1D ) and did not immunolabel for cytokeratin ( Fig. 1E ). The neoplastic cells also did not immunolabel for NSE or SYN. Scattered neoplastic cells had moderate nuclear-to-cytoplasmic immunolabeling for S100. Histologic and IHC results confirmed a diagnosis of neuroendocrine neoplasia.
The mass was extensive and infiltrative. Given the highly invasive nature of the mass and severe presumptive infection, the surgical approach involved an elliptical incision encompassing the mass, with the goal of excising the entire mamma and affected overlying skin to achieve clean margins. However, complete excision created a substantial closure deficit, and only the caudal portion of the incision could be primarily apposed. Consequently, >50% of the wound would be left to heal by second intention, carrying a high risk of dehiscence and postoperative infection. Also, despite extensive attempts at hemostasis, severe intraoperative blood loss (~4 L) occurred. Considering these complications and the overall severity of the condition, euthanasia was elected.
The surgically removed, firm, multilobular, 40-cm wide mass was submitted with the body of the mare. On cut surface, multiple, variably sized, firm, yellow-to-gray-to-tan nodules coalesced and were surrounded by firm tan connective tissue. Numerous cavitations containing hemorrhage and necrotic debris were observed. Close to the surgical margin, many similar firm nodules extended into the surrounding subcutis. The superficial inguinal, mammary, and iliac lymph nodes were 2–4 times their normal size but retained identifiable corticomedullary architecture. Samples from the mastectomy excision site had morphology similar to those in the biopsy submission. The neoplastic cells infiltrated the adjacent skeletal muscle ( Fig. 1F ) and were found rarely within blood vessels and lymphatics. However, metastases were not found in regional lymph nodes.
Various cytokeratin markers of high- and low-molecular-weight and smooth-muscle markers are routinely used to distinguish luminal epithelial cells from basal or myoepithelial cells, respectively. However, in mammary tumors, 7 a panel of markers—including chromogranin A,8,16,22 NSE, 10 S100, 4 and synaptophysin—can assist in the diagnosis of NETs. Chromogranin A 3 is widely utilized to identify neuroendocrine origin, such as gastroenteropancreatic NETs and pheochromocytomas.19,22 NSE and S100 are additional supportive NET markers; positivity for NSE often indicates undifferentiated or metastatic tumors,2,10 and S100 is immunolabeled in well-differentiated tumors, such as pancreatic NETs.4,18
Mammary gland disease in mares is uncommon and often inflammatory; mammary neoplasia is rare and frequently mimics mastitis, complicating and delaying diagnosis. Equine mammary neoplasms are sparsely reported and typically carry a poor prognosis. Neuroendocrine neoplasia of the mammary gland is exceedingly rare in veterinary medicine; a thorough search of PubMed, Google Scholar, and CAB abstracts for mammary NEC in mares did not yield any reports. We have classified mammary gland neoplasms in mares as those originating from the mammary gland (primary) and those of non-mammary origin (originating from tissues adjacent to the mammary gland or as a result of metastatic disease; Table 2). Carcinomas are the most common primary and metastatic mammary neoplasms in mares,1,20 and include solid carcinoma, ductal carcinoma, 9 papillary ductal adenocarcinoma, 6 and metastatic squamous cell carcinoma. 11 Additional neoplasms of non-mammary origin reported in the mammary region in mares include mammary sarcoma,21,23 melanoma, 13 lymphoma, 15 and sarcoid. 13 Histopathology, supported by IHC, remains the most reliable approach for diagnosis and prognostic assessment of mammary neoplasia.
Summary of primary and secondary mammary gland neoplasms reported in horses.
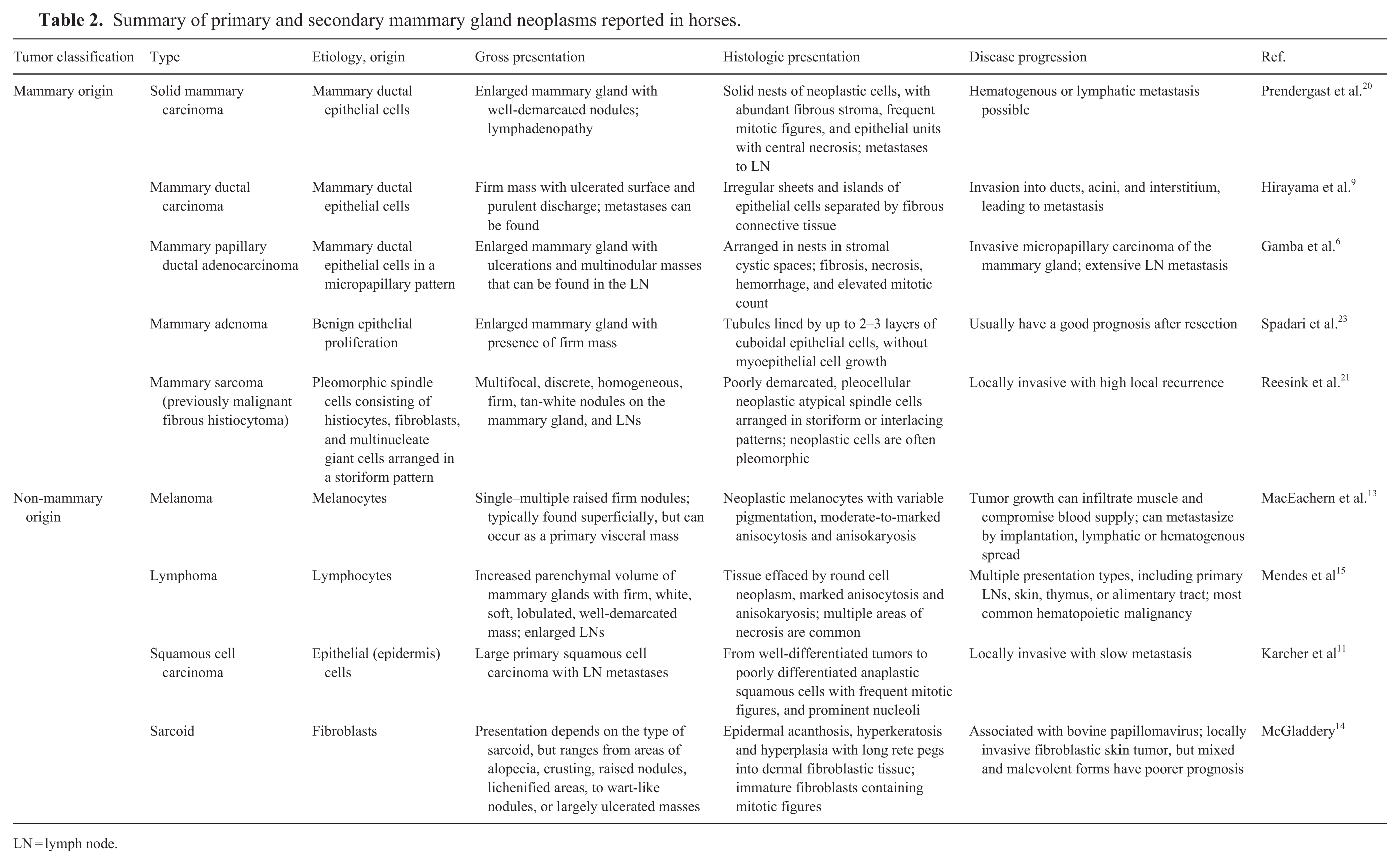
LN = lymph node.
Mammary neuroendocrine carcinomas (
Mammary NETs are exceedingly rare and have been documented predominantly in women; loss of cytokeratin expression has been reported in up to 10% of the cases. 12 The very few reports in veterinary species include only dogs 17 and a tiger. 5 The reported canine cases share some histopathologic features with human mammary NECs. Although the neoplasm in our equine case had negative immunolabeling for cytokeratin, we cannot rule out a NEC.
Standardized diagnostic criteria and comprehensive immunohistochemical characterization of NETs are lacking in veterinary medicine, and meaningful assessments of biological behavior and prognostic significance are not possible. Given the distribution of the neoplasm within deep sections of the mamma in our case, and the extensive replacement of the mammary tissue leaving only a few small normal glands, we favored a neuroendocrine mammary tumor. However, we cannot rule out a neuroendocrine tumor of cutaneous origin with infiltration of the mamma. Our case highlights the importance of considering NET as a differential diagnosis when evaluating mammary gland tumors in horses.
Footnotes
Acknowledgements
We thank Jinhua Zhang and ViTALs diagnostic services for their assistance with the slides.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.