
Abstract
Cervical cancer is the fourth most common cancer in women worldwide and is most frequently diagnosed in women who are between the ages of 35 and 44, with the incidence rates increasing nearly 2% each year in women ages 30–44. Standard surgical management of early-stage cervical cancer routinely involves hysterectomy. However, the prevalence of cervical cancer in young patients and the social shift of women electing to delay childbearing has created a reproductive dilemma. With the arrival of the radical vaginal trachelectomy in the late 1980s, patients with early-stage cervical cancer now had an option for fertility preservation. Over time, fertility-sparing surgeries for cervical cancer patients have become increasingly conservative while maintaining comparable oncologic outcomes. This surgical review examines the variety of fertility-sparing procedures available for early-stage cervical cancer in the context of their oncologic and reproductive outcomes.
Introduction
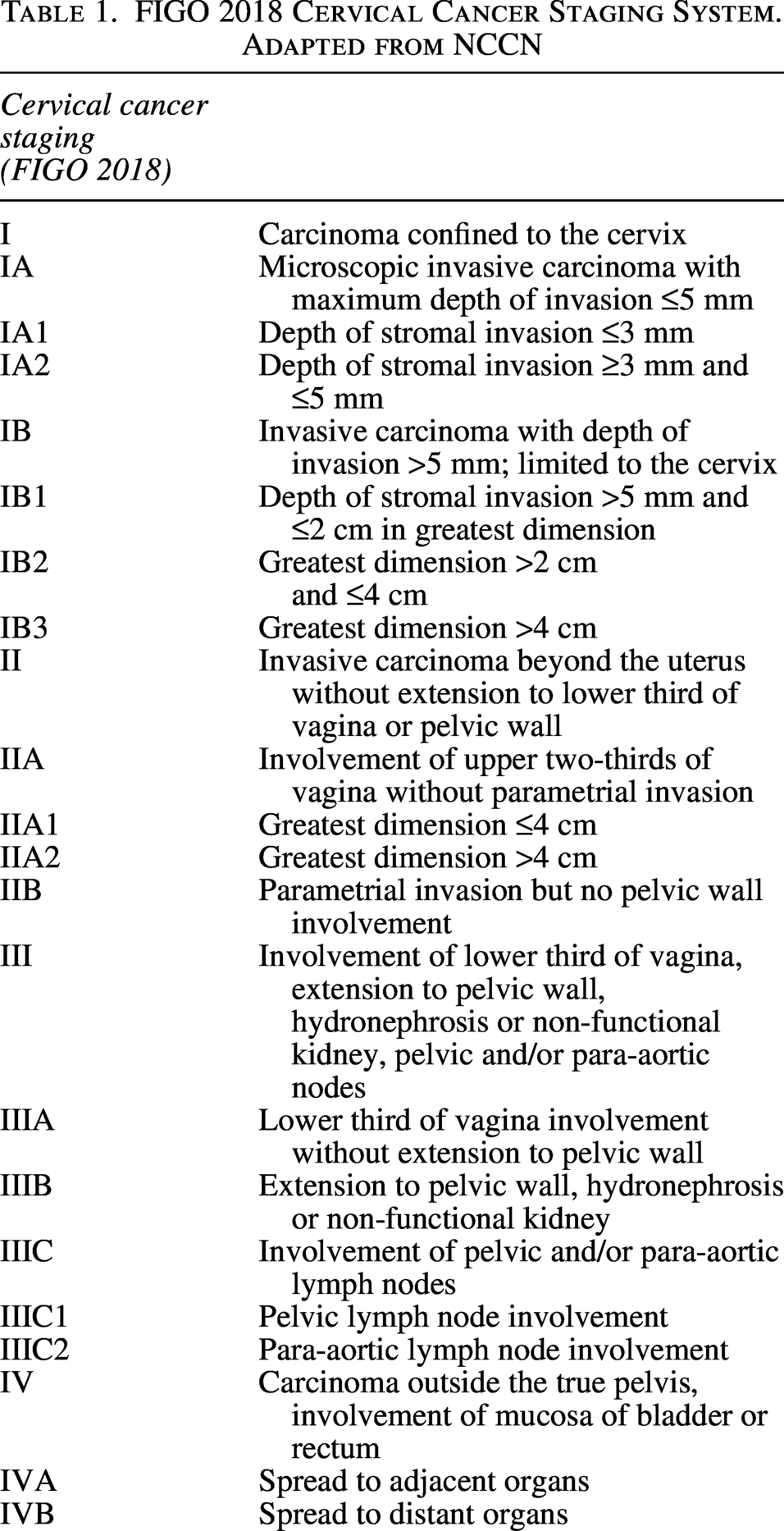
Cervical cancer is the fourth most common cancer in women worldwide and is most frequently diagnosed in women who are between the ages of 35 and 44, with the incidence rates increasing nearly 2% each year in women ages 30–44. 1 Cervical cancer is divided into early-stage (IA1–IB2), locally-advanced (IB3–IVA), and metastatic (IVB) disease (Table 1). Standard surgical management of early-stage cervical cancer routinely involves hysterectomy. However, the prevalence of cervical cancer in young patients and the social shift of women electing to delay childbearing has created a reproductive dilemma. With the arrival of the radical vaginal trachelectomy in the late 1980s, patients with early-stage cervical cancer now had an option for fertility preservation. Over time, fertility-sparing surgeries for cervical cancer patients have become increasingly conservative while maintaining comparable oncologic outcomes. In this review, we will examine the variety of fertility-sparing surgical procedures for early-stage cervical cancer and assess their oncologic and reproductive outcomes.
FIGO 2018 Cervical Cancer Staging System. Adapted from NCCN
Preoperative considerations
Prior to proceeding with surgical management, presence of locoregional and metastatic disease should be clinically and radiographically assessed. Preoperative imaging with magnetic resonance imaging (MRI) is a reliable method of evaluating locoregional spread of the disease. While the incidence of parametrial involvement in patients with early-stage cervical cancer <2 cm is <1%,2–6 it is imperative to determine the presence of such key factors (parametrial invasion, tumor size, lymph node involvement) that can impact candidacy and success of a fertility-sparing procedure. Prior studies incorporating MRI and positron emission tomography radiographical variables, plus or minus clinicopathologic factors, into risk assessment models have been highly predictive of recurrence and survival.7–9 These models have noted higher predictive ability than International Federation of Gynecology and Obstetrics (FIGO) stage alone.7–9
After a cervical conization procedure, interpretation of MRI for geographic and nodal spread of disease can be difficult in differentiating between postprocedural cervical scarring/inflammation and persistent disease. In a single-institution retrospective study evaluating MRI imaging in patients undergoing radical trachelectomy, more than half of patients who had an initial diagnostic cone biopsy ultimately had no residual carcinoma on the final trachelectomy pathology specimen, and the risk of detecting residual disease was even lower with negative cone biopsy margins. Tumor size measurements between MRI and final pathological specimen were noted to be very similar with an approximately 2 mm or less discrepancy. Accuracy in determining deep cervical stromal invasion on MRI may be challenging due to postconization inflammation; however, patients in this study with deep cervical stromal invasion (outer third involvement) or tumor size ≥2 cm on MRI were found to be more likely to undergo radical hysterectomy. The presence of 5 mm or less distance between the internal os and tumor on pretrachelectomy MRI may be an indication of patients likely to need a radical hysterectomy. Additionally, MRI after conization with negative cone margins may be helpful to verify absence of residual disease as all patients analyzed that had a negative cone biopsy and no residual disease on trachelectomy were found to have no tumor remaining on postconization MRI. Pretrachelectomy MRI may be helpful in recognizing patients who may be treated with a fertility-sparing procedure that is less extensive than a radical trachelectomy and should be included in preoperative workup. Distance between tumor and internal os, tumor size, and cervical stromal invasion are features evaluated by MRI that can be utilized for determining appropriate candidates for radical trachelectomy. 10
Fertility-sparing surgical management in cervical cancer
Fertility-sparing surgeries in early-stage cervical cancer have seen a de-escalation of radicality over several decades. The evolution from more to less radical primary surgery in cervical cancer coupled with the advent of sentinel lymph node (SLN) evaluation has now been deemed appropriate in several prospective studies. Obstetric outcomes have correlated accordingly, and term birth rates have seen improvement with less radical excision of cervical tissue for women undergoing fertility-sparing surgery. The following will review more to less radical surgical techniques and their outcomes.
Radical Vaginal Trachelectomy
With the introduction of radical vaginal trachelectomy, first performed by Dargent in the 1980s and subsequently published in 1994, fertility-sparing surgery for women with early-stage cervical cancer was codified into the literature. Given this was the first fertility-sparing procedure of its kind, it became one of the most well-studied fertility-sparing surgeries. Dargent’s procedure consisted of a combined laparoscopic approach to lymph node dissection followed by a vaginal approach to radical trachelectomy for the primary cervical tumor, where adjoining bilateral parametrial tissue is excised (Fig. 1).
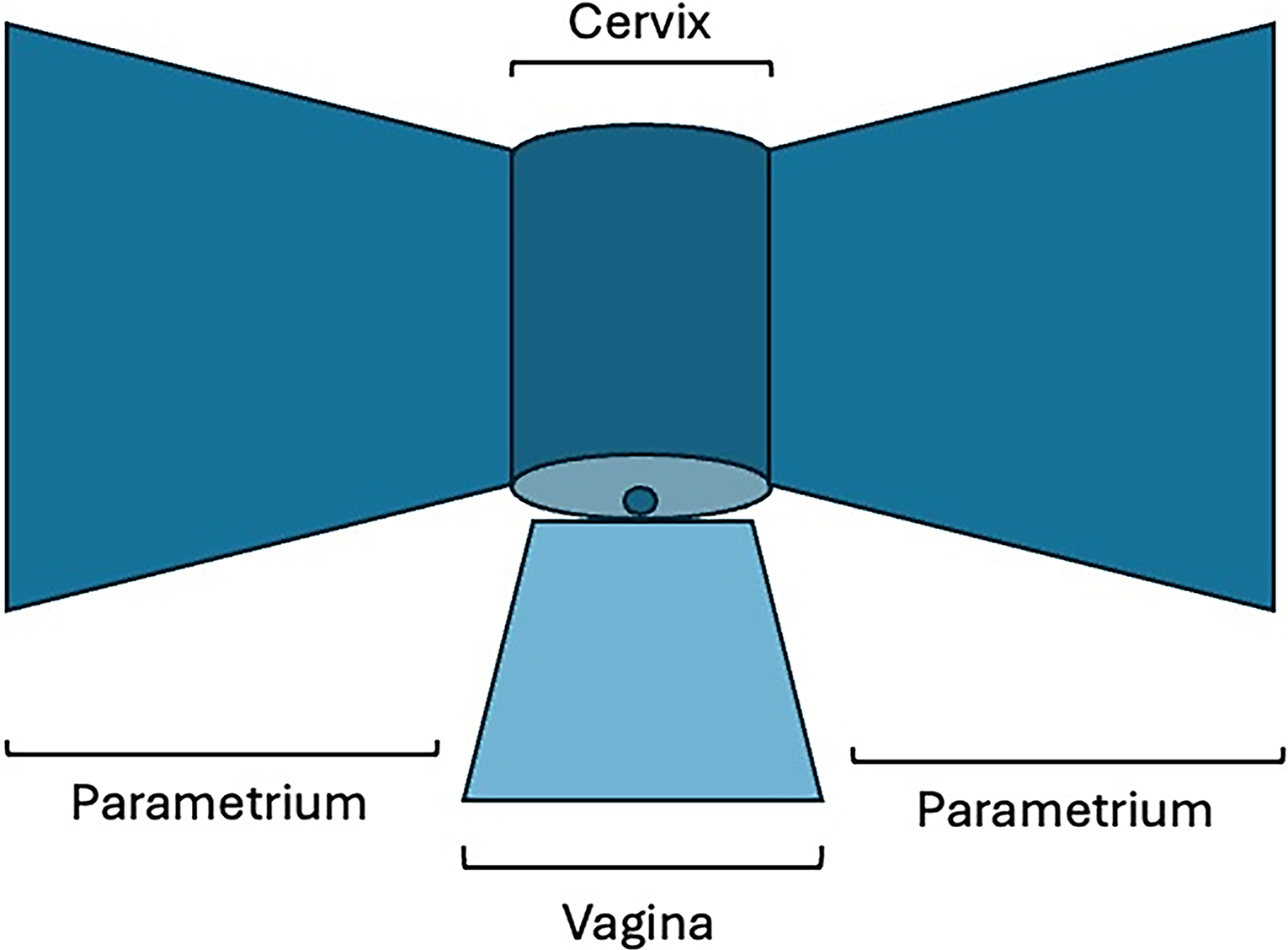
Cervix, vagina, parametrium schematic.
In a systematic review of three clinical trials, radical trachelectomy, including vaginal and abdominal, showed no difference in recurrence rates compared with radical hysterectomy. 11 Radical trachelectomy has been associated with lower morbidity compared to radical hysterectomy, particularly with the adoption of laparoscopic SLN evaluation. Increasing tumor size became a key factor associated with recurrence. In a systemic review, 17% of patients with tumor size >2 cm recurred, whereas 4% with tumors <2 cm had recurrence. 12 Another review noted a recurrence rate of <5% in early-stage disease with a <2% recurrence rate for tumors ≤2 cm. 13 Therefore, a tumor size larger than 2 cm came to be considered a relative contraindication for radical vaginal trachelectomy. High-risk histologies have also been noted as a significant risk factor for recurrence. Due to the propensity for skip lesions in adenocarcinoma, undiagnosed residual tumors can lead to cervical recurrences, but overall continues to be an allowable histotype along with squamous cell carcinomas. Grade 3 histologies have been noted to be a relative contraindication to undergo a fertility-sparing surgery.12,14 Many prior studies have long-established the safety and feasibility of radical vaginal trachelectomy15,16 in conjunction with laparoscopic SLN dissection in the appropriately selected patient population. 16 From here, many began exploring alternative surgical options, balancing optimal outcomes while minimizing surgical risk.
Abdominal Radical Trachelectomy
Patient selection criteria for radical abdominal trachelectomy varies and is a topic of debate. Although no formal criteria has been set forth, abdominal radical trachelectomy may be offered to patients with less favorable prognostic features (tumor size >2 cm, lymphovascular space invasion [LVSI]) who desire fertility preservation. Some centers perform radical trachelectomy for tumors <4 cm, especially if the tumor is exophytic, with any degree of stromal invasion. 10 Open trachelectomy offers wider parametrial and paracervical resection compared with vaginal radical trachelectomy and allows a more detailed tactile assessment by the surgeon. Radical trachelectomy performed via the vaginal route can be challenging as the procedure requires considerable surgical skill that may be prohibitive of many surgeons. The open approach to radical trachelectomy can be an alternative that allows trachelectomy to be more accessible to patients. However, increased blood loss, prolonged hospital stay, and formation of adhesions that impact fertility are potential downsides to abdominal trachelectomy. Significant postoperative morbidities seen with abdominal radical hysterectomy include intra-abdominal abscesses, cerclage erosion, cervical stenosis related to cerclage placement, and uterine necrosis. One prior study including an abdominal approach evaluated 29 patients with Stage 1B1 tumors measuring 2–4 cm. Of these, 31% had a fertility-sparing procedure, but 45% required immediate hysterectomy, 21% required adjuvant chemoradiation, and 1% required definitive chemoradiation. 17
As it is relatively similar to radical hysterectomy, abdominal radical trachelectomy is more commonly performed and more reproducible than its vaginal counterpart, but uterine artery management may differ between surgeons. Ligation of the cervicovaginal branches with preservation of the uterine artery aids in uterine vascularization, therefore is thought to better preserve fertility; however, blood loss and operative time are higher than the alternative of uterine artery ligation. 12 In a prior study of 26 patients evaluating uterine artery preservation in radical abdominal trachelectomy, only 12% had ongoing postoperative bilateral flow through the uterine arteries. 45% of patients saw unilateral uterine artery occlusion, and 45% had bilateral uterine artery occlusion suggesting that uterine artery preservation does not seem to impact postoperative uterine blood supply if alternative blood supply chains are preserved. 18
Examining the length of parametria resected in abdominal radical trachelectomy versus vaginal radical trachelectomy, parametrial length removed was described in a retrospective study as significantly higher in the abdominal versus vaginal radical trachelectomy group (3.97 cm vs. 1.45 cm, respectively), with proposed specimen correlation to a Class III radical hysterectomy for the abdominal route versus Class II radical hysterectomy for vaginal route. No parametrial nodes were detected in the vaginal trachelectomy group, whereas 57.3% of abdominal trachelectomy specimens contained parametrial nodes. There was no difference in LVSI, regional lymph nodes excised, or complication rates between the abdominal and vaginal cohorts. Abdominal radical trachelectomy can provide the ability to attain wider parametrial resection and parametrial lymph node removal with similar histopathologic and surgical outcomes compared to the vaginal approach, suggesting abdominal radical trachelectomy would be particularly beneficial for patients with large volume disease that require more extensive surgical margin resection. 19
Recurrence rates in patients with Stage IB1 disease have been described as lowest in those undergoing abdominal radical trachelectomy (2.4%) as compared with conization/simple trachelectomy (4.1%), vaginal radical trachelectomy (4.7%), and laparoscopic radical trachelectomy (5.2%). Rates of recurrence are higher in those with LVSI.20,21
Laparoscopic Radical Trachelectomy
The first purely laparoscopic radical trachelectomy was described in 2002 by Pomel et al. Such a minimally invasive approach has noted several advantages, including shorter hospital stay, reduced postoperative pain, improved cosmesis, and quicker return to normal activities. In terms of surgical technique, use of a uterine manipulator is not recommended when a visible cervical lesion is present. Instead, colpotomy can be made vaginally with care taken to clamp the excised vaginal margin as a cover over the cervix followed by extraction of the specimen. If no cervical lesion is visible, a uterine manipulator can be utilized and colpotomy made laparoscopically after the cervix and parametria are resected. 21 A prior Italian retrospective study evaluating tumors ≤2 cm noted that this modality was noted to have similar intraoperative and postoperative complications compared with laparoscopic-assisted radical vaginal hysterectomy. Further, similar recurrence rates were noted compared with laparoscopic-assisted radical vaginal hysterectomy. 22
In 2018, the use of minimally invasive surgery for nonfertility-sparing management of early-stage surgical cancer was recommended against and abdominal surgery became the new standard of care. This occurred following publication of the landmark laparoscopic approach to cervical cancer trial that saw a significantly worse disease-free and overall survival for minimally invasive (both laparoscopic and robotic) versus open approach for patients undergoing radical hysterectomy. 23 However, this study did not evaluate the use of minimally invasive techniques for fertility-sparing surgery. Although retrospective in nature, previously available data, as discussed above, show that outcomes of minimally invasive and open approaches to radical trachelectomy have been equivalent.
In 2022, the International Radical Trachelectomy Assessment (IRTA) institutional, international, retrospective study was published. Of 646 patients, 358 underwent open surgery, and 288 underwent minimally invasive surgery. Eligible patients had squamous carcinoma, adenocarcinoma, or adenosquamous carcinoma; had a preoperative tumor size of ≤2 cm; and underwent either open or minimally invasive (robotic or laparoscopic) radical trachelectomy with nodal assessment (pelvic lymphadenectomy and/or SLN biopsy). Authors noted no difference in 4.5-year disease-free survival rates: 94.3% (95% confidence interval, 91.6–97.0) for open surgery and 91.5% (95% confidence interval, 87.6–95.6) for minimally invasive surgery (log-rank p = 0.37). 24 Given the low prevalence of readily available candidates for these types of procedures, prospective randomized data will not likely be feasible. This study to-date provides the most comprehensive data as to the safety of minimally invasive surgery in the setting of fertility preservation for cervical cancer.
Robotic Radical Trachelectomy
Robotic radical trachelectomy was first described in 2008 by Geisler et al. The robotic surgical platform has allowed surgeons to perform more intricate surgical procedures through finer instrumentation and three-dimensional visualization, enabling enhanced dexterity and detailed surgical accuracy. In contrast to vaginal radical trachelectomy, a potential advantage of open, laparoscopic or robotic radical trachelectomy is the ability to resect the parametria in its entirety and divide the uterine arteries at their origin, thus allowing for complete parametrial removal along with the parametrial lymph nodes that may be involved in smaller cervical tumors. 25
In a retrospective study comparing robotic radical trachelectomy to open radical trachelectomy, robotic radical trachelectomy had significantly less blood loss compared with open radical trachelectomy (median estimated blood loss 62.5 mL vs. 300 mL) and shorter postoperative length of stay (LOS) (median LOS 1 day vs. 4 days) with no difference in operative time or intraoperative complications. 26 Further, there was no difference in median length of parametrial tissue removed between the two surgical modalities. Open radical trachelectomy had a greater cumulative rate of late morbidity (58% vs. 13% for robotic radical trachelectomy), consisting of cervical stenosis, cerclage erosion, and abnormal uterine bleeding. Serious morbidity (reoperation, readmission, blood transfusion, venous thromboembolism, loss of fertility, ICU admission, death) did not differ between these two surgical routes. Four percent of open cases and 33% of robotic cases were converted to radical hysterectomy due to close (<10 mm) or positive surgical margins, which is a significant finding that should be taken into account when selecting surgical route. 25 Following resection, one study noted that compared to vaginal trachelectomy, cervical length is equally preserved via a robotic approach and cerclage placement is less variable. 26
In a study of Stage IB patients, incidence of cancer recurrences between abdominal and laparoscopic or robotic radical trachelectomy were similar with a nonsignificant difference in recurrence rates of 3.3% and 5.5%, respectively. 20
Based on the IRTA study discussed above, a robotic modality, just like laparoscopy, appears to offer a safe minimally invasive approach that can be considered.
Simple Vaginal Trachelectomy
In the early 2000s, several studies started to surface noting the low risk of parametrial involvement in select early-stage patients with cervical cancer. This began challenging the traditional dogma of parametrial resection for patients with tumor size ≤2 cm, depth of invasion ≤10 mm, and negative pelvic lymph nodes.2–6 One of these studies noted that in 60% of patients who underwent conization followed by radical trachelectomy, no residual disease was found on final specimen, suggesting that a less radical approach could be undertaken. 2 Additionally, removal of the parametrium and the pelvic autonomic nerves within the parametria has been associated with greater surgical morbidity including bowel, bladder, and sexual dysfunction. 15
Therefore, a simple vaginal trachelectomy was introduced as a potential alternative approach to radical trachelectomy for patients with low-risk tumors. 27 In 2017, through a prospective series of early-stage cervical cancer, simple vaginal trachelectomy with lymph node evaluation was noted to be a safe fertility-sparing procedure for patients with Stage IA1-IB1 with low-risk lesions <2 cm. These patients received laparoscopic sentinel lymph node mapping followed by complete lymphadenectomy and subsequent simple vaginal trachelectomy. All patients had negative trachelectomy surgical margins with 63% of patients having either no residual disease or dysplasia in the trachelectomy specimen. There was a 96.8% recurrence-free survival rate at 48 months. 5.7% had lymph node metastases of isolated tumor cells with no otherwise positive lymph nodes, affirming the low probability of positive lymph node involvement in small-volume lesions. Fifty-one percent of patients became pregnant with a lower prematurity rate compared with radical trachelectomy, with 40% of patients in this study having cerclage placement.28,29
A subsequent review in 2018 of patients with Stage 1B1 disease noted no difference in survival between those who underwent radical hysterectomy versus those that underwent fertility-sparing trachelectomy or cone biopsy. 14 The same year, a systematic review of five nonrandomized studies concluded that simple vaginal trachelectomy or conization could be safely performed for IA1 cervical cancer patients with LVSI. 30 Given the comparable oncologic and improved reproductive outcomes using such an approach, this had led to an ever more conservative management for women seeking to maintain fertility.
Cervical Conization
Cervical conization was originally designated as a stepping stone, collecting diagnostic tissue to assess need for a subsequent radical trachelectomy. Conization involves only the removal of the affected portion of cervix allowing for expedited recovery without the need for parametrial dissection or removal of excess tissue. In light of new prospective data consistent with prior retrospective data, it has now come to replace more radical procedures as the optimal standard of care for low-risk patients. The nonrandomized ConCerv trial showed that conservative surgery with conization or simple hysterectomy was feasible for early-stage IA2-IB1 low-risk cervical cancer with a 5% positive lymph node rate and 3.5% overall 2-year recurrence rate. 31 This trial determined that in presence of low-risk features, cervical conization with or without lymph node evaluation alone was safe and feasible in lieu of trachelectomy.
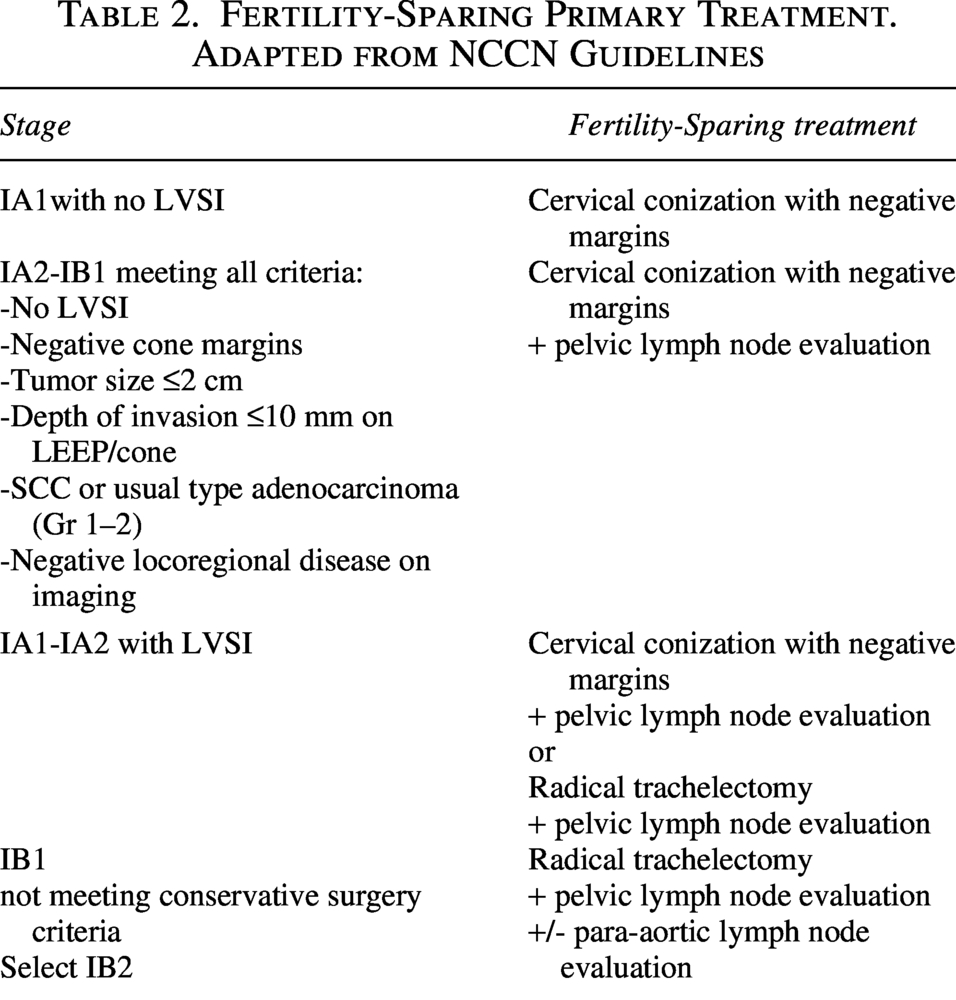
Conization is now considered optimal management for Stage IA1 tumors without LVSI and select Stage IA2-IB1 who meet all conservative surgery criteria (negative LVSI, negative cone margins, squamous cell or usual type Grade 1–2 adenocarcinoma histology, tumor size ≤2 cm, depth of invasion ≤10 mm, no metastatic disease) (Table 2).32,32 Of those women who received fertility-sparing conization in this trial, 27.5% in this group achieved pregnancy.31,32 A subsequent surveillance, epidemiology, and end results retrospective cohort study examining Stage IA–IB2 patients who underwent nodal evaluation plus cervical conization or trachelectomy revealed a trend of 15% increase in patients receiving conization with lymph node evaluation, particularly SLN biopsy, over a 10-year time span up to 2019. 32 Those with Stage 1B tumors and adenocarcinoma histology were less likely to receive conization. In a propensity score-weighted model, those receiving conization versus trachelectomy had comparable overall survival (7-year rates, 98.9% vs. 97.8%). 32 This rise in early-stage cervical cancer patients undergoing cervical conization with nodal evaluation reflects a population-level trend and practice change toward significantly less radical fertility-sparing surgery. Cervical conization offers expedited recovery with similar oncologic outcomes and lower reproductive complications with higher live birth rates. Therefore, cervical conization has become the most practical choice for certain patients with early-stage cervical cancer seeking to retain fertility.
Fertility-Sparing Primary Treatment. Adapted from NCCN Guidelines
Neoadjuvant Chemotherapy with Conservative Surgery
Cervical cancer primarily spreads through direct local extension as well as dissemination via the lymphatic system. Parametrial extension and lymph node metastasis have a direct correlation. A case series by Benedetti-Panici et al. noted that 100% of patients with positive pelvic lymph nodes had parametrial involvement compared with only 2% of patients with negative lymph nodes with parametrial invasion. 33 For those with Stage IB1 disease, 16%−20% had positive lymph nodes and 31% had parametrial involvement.33,34
Fertility-sparing surgery has been most established in early-stage cervical cancers with tumor size ≤2 cm. For patients with tumors >2 cm who strongly desire fertility, fertility-sparing surgery can be offered but it should be made known that recurrence rates are higher, ranging between 10% and 20%.17,20
However, for any tumor ≤4 cm, fertility-sparing surgery was not associated with a significant difference in the 5-year life expectancy. 34 This is likely because as tumor size increases, the odds of requiring immediate conversion to hysterectomy or need for adjuvant radiation increases, with a nearly 7-fold rise in probability for a 4 cm tumor compared with a 1 cm tumor.17,34 The ideal management strategy for patients with tumors >2 cm but ≤4 cm desiring to preserve fertility is still to be determined but there is data to suggest that upfront fertility-sparing surgery may be safe to offer in these patients. 34 Patients with tumors >2 cm to ≤4 cm who strongly desire to preserve fertility should be thoroughly counseled regarding the increased chance of immediate conversion during their operation, need for adjuvant radiation therapy, and the higher risk of recurrence.
To-date, abdominal radical trachelectomy would be the preferred surgical procedure for larger tumors, although pregnancy rates are lowest with the open modality. There are studies of this subset of patients receiving neoadjuvant chemotherapy followed by conservative surgery with conization or radical trachelectomy. Three cycles of platinum-based chemotherapy has been the most commonly used neoadjuvant regimen. In a systemic review including 99 patients who received neoadjuvant chemotherapy followed by conservative surgery, 51 underwent laser conization or cold-knife or simple trachelectomy, and 42 underwent radical trachelectomy. 12 Forty-five patients (45%) had no residual disease and 19 patients (19%) required adjuvant therapy due to positive nodal involvement, positive margins, residual disease, or disease progression. 6% of the 99 patients developed recurrent disease. Fifty-four pregnancies were reported, with the highest proportion of pregnancies in those who underwent fertility-sparing surgery with no parametrial resection. 12 The extent of radical trachelectomy necessary to decrease the risk of positive margins should be weighed against the impact radical surgery may have on fertility outcomes which is the reason the procedure is being done in the first place.
Neoadjuvant therapy followed by conservative surgery could be an option for carefully selected patients with large tumor sizes of 2–4 cm that may not be ideal candidates for upfront fertility-sparing surgery who strongly desire fertility. However, caution should be utilized as this is not currently part of standard management. Further studies, including the ongoing, prospective Cervical cancer treated with Neo-adjuvant chemotherapy followed by fertility Sparing Surgery trial evaluating Stage IB2 cervical cancer treated with neoadjuvant chemotherapy seek to better assess this treatment approach.
Reproductive Outcomes
In a systemic review examining 3044 patients who underwent fertility-sparing surgery, there was a mean clinical pregnancy rate of 55.4%. Eighty percent of patients conceived spontaneously. Highest clinical pregnancy rates were seen after conization/simple trachelectomy. Radical vaginal trachelectomy had a higher clinical pregnancy rate compared with abdominal vaginal trachelectomy. This could be due to the sparing of the uterine arteries with vaginal trachelectomy as well as the decreased formation of pelvic and intra-abdominal adhesions with vaginal surgery, whereas abdominal trachelectomy may lead to more tubo-ovarian adhesions that can further contribute to tubal factor infertility. 21
Conization and simple trachelectomy had a higher mean live-birth rate at 86.4% compared with vaginal and laparoscopic radical trachelectomy (with or without robotic assistance). However, this could be affected by selection bias as those with smaller lesions are more likely to have a conization as compared to advanced lesions, which are more likely to receive trachelectomy, with the radical resection potentially affecting cervical competence. There was no difference in preterm delivery rates between the surgical approaches; however, there was a 31% preterm delivery rate after fertility-sparing surgery, which is higher than the global preterm delivery average of 10.6%. Cervical cerclage can be placed at time of trachelectomy but is controversial due to risks such as development of an ascending infection and premature rupture of membranes from cerclage displacement. Patients who undergo fertility-sparing surgery should be co-managed with reproductive endocrinologists to examine reproductive options and referred to maternal fetal medicine specialists for subsequent pregnancy management.
Conclusion
Several treatment strategies are available for fertility-sparing surgery in early-stage cervical cancer with various factors that can affect oncologic and reproductive outcomes. Higher pregnancy rates are seen with vaginal radical trachelectomy compared with abdominal radical trachelectomy, with similar oncologic data between all surgical routes. For tumors ≤2 cm, new prospective data suggest that cervical conization may be a safe and effective strategy for those with low-risk features. For tumors >2 cm, abdominal radical trachelectomy may be the preferred fertility-sparing modality due to the ability to obtain wider parametrial margins, though pregnancy rates may be lower. For patients who do require a radical trachelectomy procedure, minimally invasive modalities such as laparoscopy or robotic do not appear to increase risk of recurrence or worsen survival, unlike the increased risk noted with minimally invasive radical hysterectomy. Neoadjuvant therapy with subsequent fertility-sparing surgery is being actively studied as a potential strategy expanding fertility candidacy to a broader number of patients. Advantages and disadvantages exist for each of the surgical approaches, and the treatment strategy should be tailored to the patient’s clinicopathologic features and plans for fertility.
Footnotes
Author Disclosure Statement
No interests to disclose.
Funding Information
No funding was received for this article.