
Abstract
Introduction:
Sciatic nerve endometriosis is a rare but debilitating form of deep infiltrating endometriosis (DIE) that typically presents with cyclical, refractory sciatica. Management requires meticulous surgical planning and a multidisciplinary approach to achieve both neurological relief and fertility preservation.
Case Presentation:
A 37-year-old nulligravid patient presented with severe, debilitating left-sided sciatica unresponsive to hormonal treatment. Transvaginal ultrasound and pelvic magnetic resonance imaging revealed a large nodule reaching the left obturator internus and piriformis muscles. A complete laparoscopic excision was performed. Complete excision of the nodule infiltrating the obturator internus muscle was achieved, followed by nerve neurolysis.
Conclusion:
Complete laparoscopic excision offers a safe and effective treatment for sciatic nerve endometriosis, providing excellent symptom relief. This video highlights the necessary anatomical landmarks and surgical technique for safe neurolysis in the context of DIE.
Introduction
Endometriosis is a common gynecological condition, but its involvement of the peripheral nervous system, particularly the sciatic nerve, is a rare cause of chronic, invalidating sciatica. 1 This form of deep infiltrating endometriosis (DIE) presents a significant diagnostic and therapeutic challenge. Early recognition, guided by characteristic cyclical pain and pelvic magnetic resonance imaging (MRI) findings, is crucial to prevent irreversible neurological damage.1,2
The gold standard for the treatment of sciatic nerve endometriosis is complete surgical excision, most effectively achieved via a minimally invasive approach. Laparoscopic neurolysis permits meticulous dissection and preservation of nerve fibers, which is essential given the complexity and sensitivity of the pelvic neuroanatomy.3,4
We present a case of severe sciatic nerve endometriosis in a patient with infertility, successfully managed through radical laparoscopic excision and neurolysis. This report aims to demonstrate the key anatomical steps required for safe and complete nerve release, contributing to the existing literature on managing this rare and intricate pathology.
Case Presentation
A 37-year-old nulligravid patient with a 4-year history of primary infertility consulted due to severe, debilitating left-sided sciatica refractory to medical treatment. The physical examination revealed a palpable nodule in the left obturator fossa. Transvaginal ultrasound showed an irregular nodule over the left iliac fossa and a left ovarian endometrioma.
Pelvic MRI confirmed left ovarian endometriosis and severe DIE involving the torus and uterosacral ligaments. The study highlighted extensive involvement of the ipsilateral hemipelvis with anterior extension reaching the left posterior bladder wall. In continuity with this focus, a large, posterolateral pseudonodular component reached the most cranial aspect of the obturator internus muscle and extended posteriorly, involving the caudal aspect of the piriformis muscle. The lesion was immediately caudal to the sciatic notch and encased the theoretical branches of the left hypogastric artery. Asymmetry and evidence of fatty infiltration within the obturator internus muscle suggested probable denervation atrophy (Figs. 1–4). Given the symptoms and extent of the disease, surgical treatment was proposed.
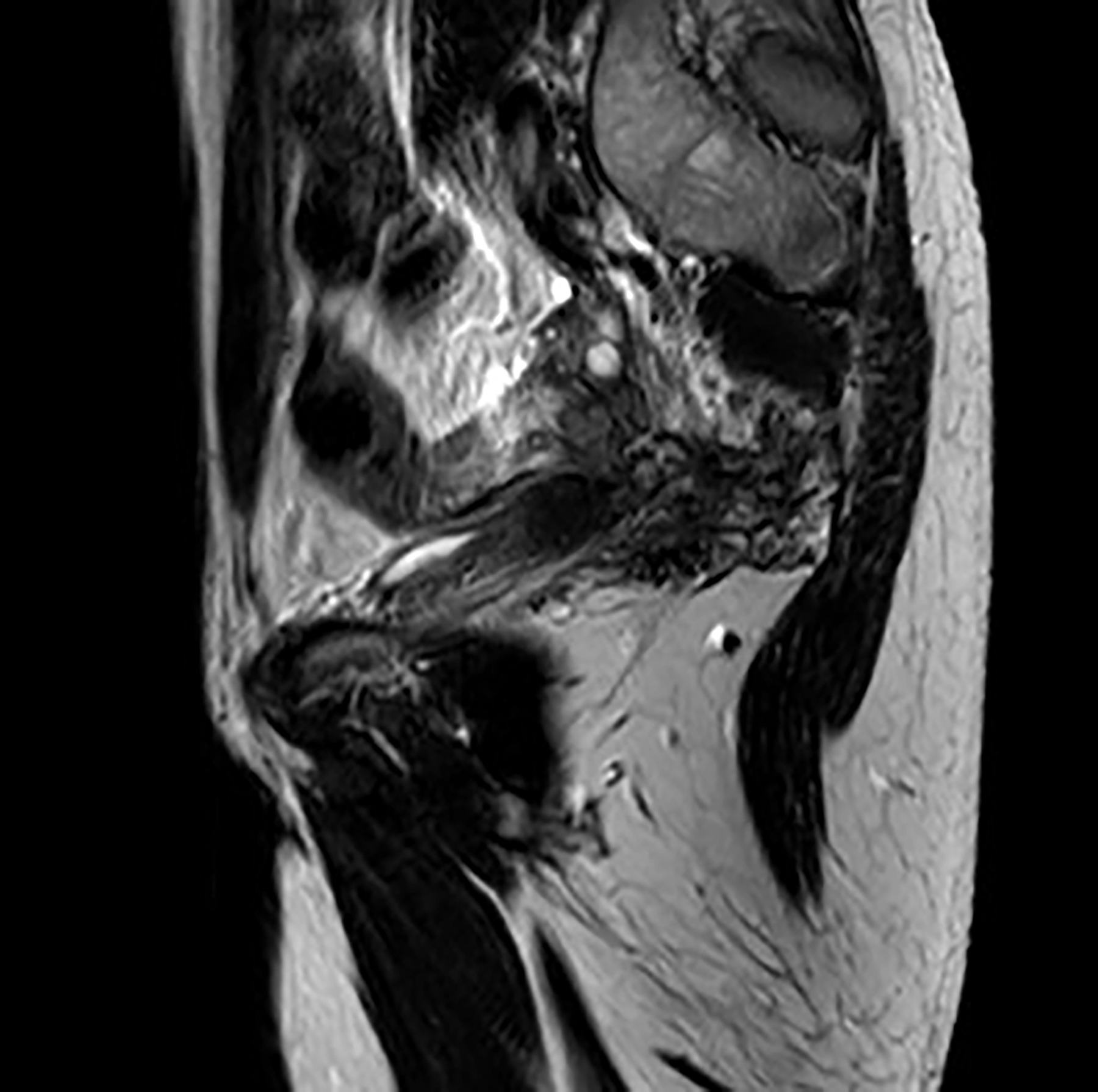
Sagittal T2-weighted magnetic resonance image (MRI) of the pelvis. This view demonstrates the posterior uterine involvement and extension toward the retroperitoneal space, indicative of extensive deep infiltrating endometriosis (DIE) affecting the cul-de-sac and uterosacral ligaments.
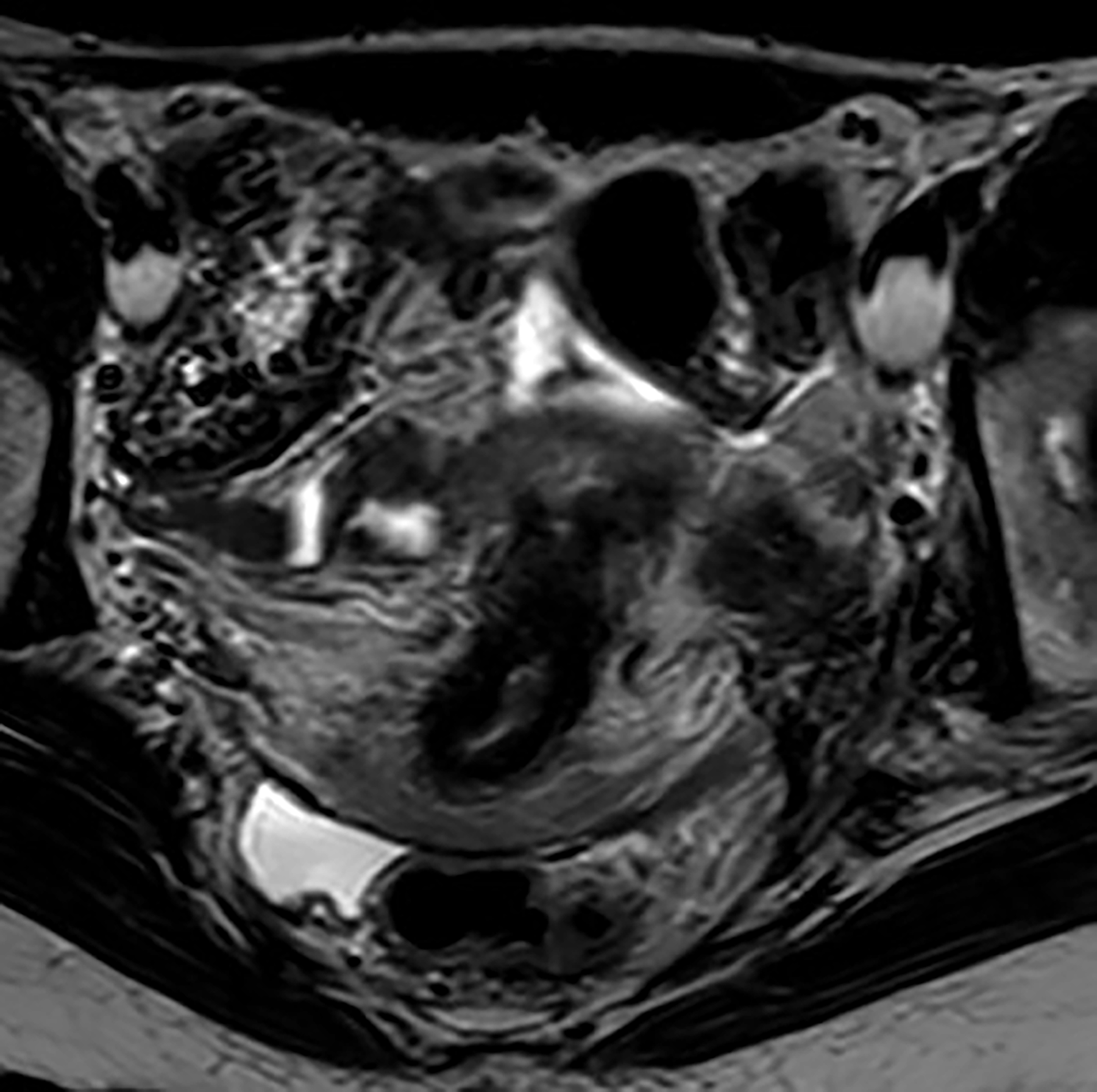
Axial T2-weighted MRI at the level of the uterus. This image clearly shows the left ovarian endometrioma and the associated severe infiltration of the uterosacral ligaments, particularly prominent on the left side.
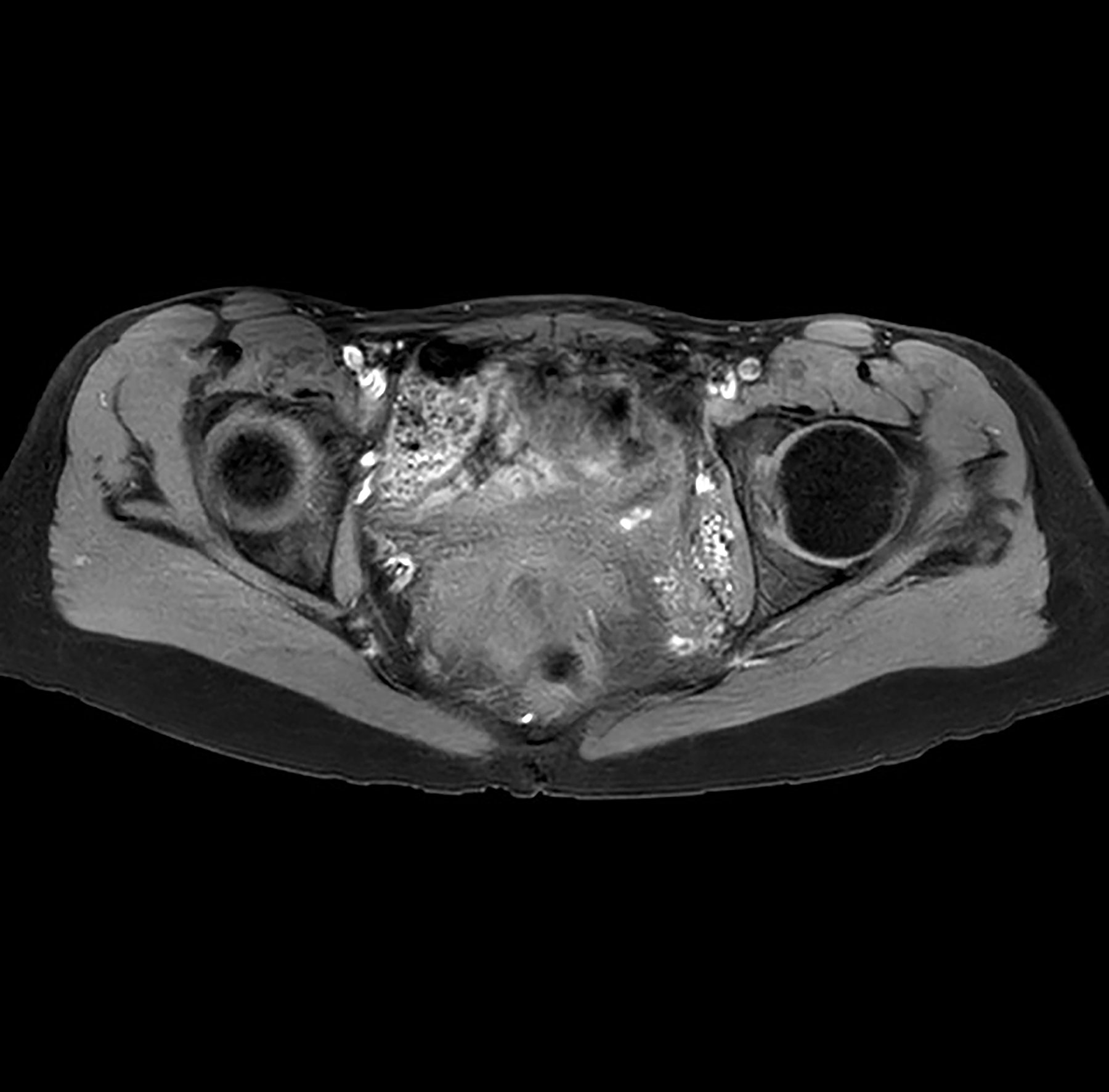
Axial T2-weighted MRI at the level of the obturator fossa and sciatic notch. A large, irregular pseudonodular component of DIE is visible, extending toward and significantly infiltrating the left obturator internus muscle.
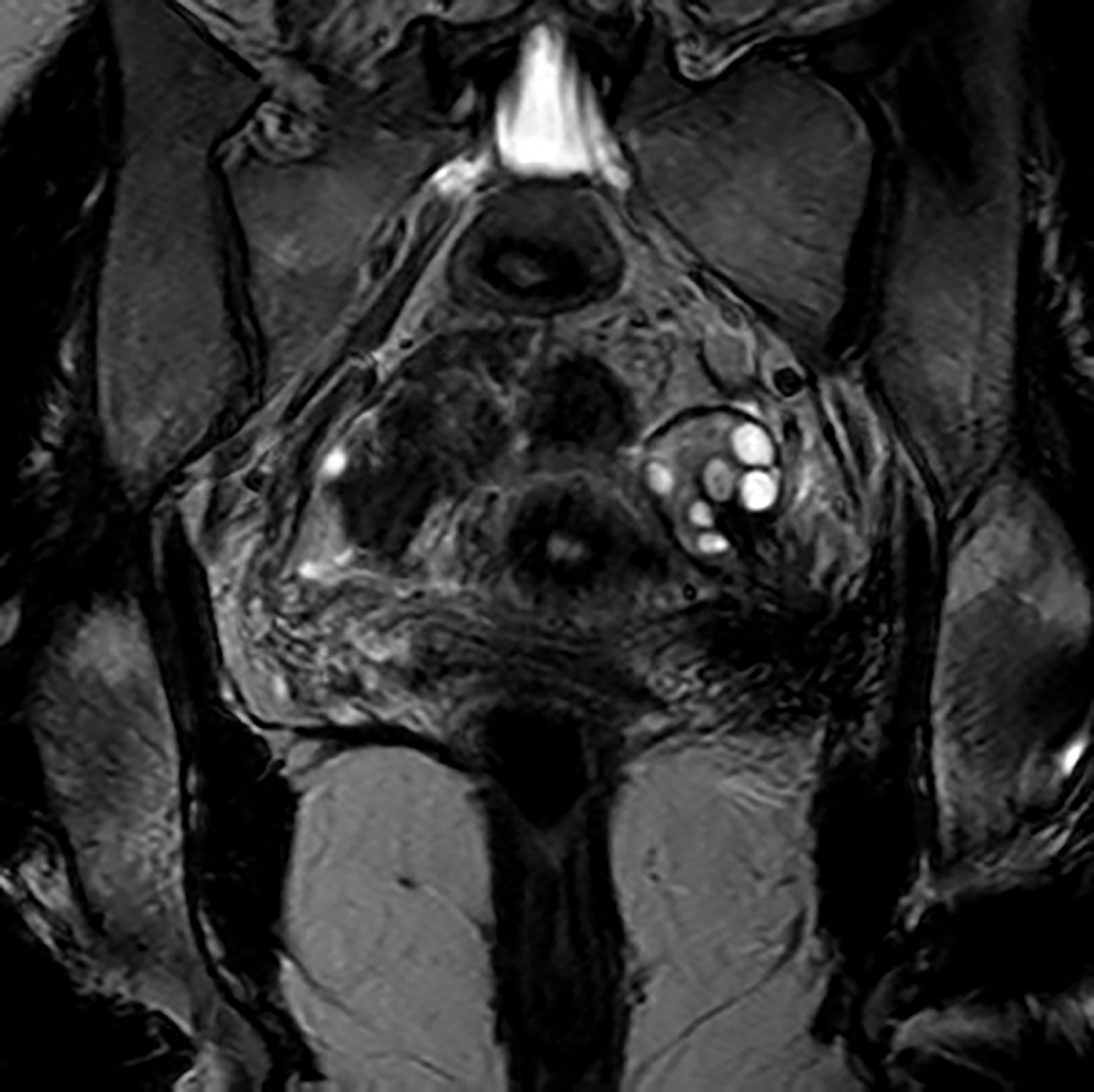
Coronal T2-weighted MRI of the pelvis. This view offers a comprehensive perspective on the left hemipelvis. It shows the left ovarian endometrioma and the extensive deep infiltrating endometriosis spreading laterally toward the pelvic side wall.
Surgical Technique (Video Steps)
Exposure and preparation: Surgical field exposure and ovarian pexy were performed to secure the left ovary away from the operating field. Ureteral dissection: The peritoneum was opened, and the left ureter was identified. The ureter was meticulously dissected from adhesions and fibrosis until its crossing with the uterine artery was reached. Space dissection and nerve identification: The left paravesical and pararectal spaces were opened. The left hypogastric nerve was identified in the mesoureter and appeared not to be infiltrated. The superior vesical artery was identified, and the obturator space was opened to visualize the obturator artery and vein. The sciatic nerve was visualized just inferiorly. The obturator nerve was also confirmed to be free of infiltration. Lateral approach and nodule delimitation: A lateral approach was performed with peritoneal opening, development of the lumbosacral space, and identification of the obturator fossa from the lateral side, medializing the iliac vessels. Obturator internus infiltration: The nodule was visualized at its lateral limit, clearly infiltrating the obturator internus muscle. A monopolar hook was used to safely delimit the nodule from its lateral margin until healthy tissue was reached Ureteral release and medial delimitation: Dissection returned medially to the ureter. The ureter was further released from compression and medialized. This permitted further delimitation of the nodule’s medial margin. Sciatic nerve neurolysis: The inferior margin of the nodule was formed by the sciatic nerve. The nerve was carefully freed from the infiltrating tissue superiorly and laterally until the greater sciatic notch was reached, completing the neurolysis. Nodule excision: The entire nodule was carefully excised en bloc and removed.
Postoperative Outcome
The patient had an uncomplicated postoperative course. At 3 months, there was a significant improvement in sciatica symptoms; however, paresthesia persisted, particularly in the gluteal region. At 1 year, the patient was asymptomatic, and pregnancy was achieved through in vitro fertilization (IVF).
Discussion
This case highlights the complexity of managing DIE with sciatic nerve involvement, a condition often misdiagnosed as purely orthopedic pain. The patient’s severe pain, coupled with the MRI findings showing a nodule adjacent to the nerve and signs of denervation atrophy in the obturator internus muscle, strongly supports the indication for radical neurolytic surgery. Our laparoscopic approach permitted the meticulous identification and preservation of critical structures, including the ureter, hypogastric nerve, the obturator nerve, and vessels, before safely accessing and releasing the sciatic nerve. It is very important that a systematic approach be used to identify the surgical spaces required for the nerve-sparing technique, as described in the literature.3–6
The surgical challenge in this case was the extensive infiltration reaching the obturator internus and piriformis muscles, which required careful dissection to obtain clear margins without damaging the nerve trunk. The key technical takeaway is the critical importance of first establishing the avascular spaces, such as the pararectal and paravesical spaces, to gain control of the ureter and vessels. This provides a safe surgical corridor to the sciatic nerve at the inferior margin of the DIE nodule, as detailed in surgical video articles.3,6
The excellent outcome, evidenced by the resolution of sciatica and the subsequent IVF pregnancy, underscores the dual benefit of aggressive, complete excision in patients with both pain and infertility related to DIE. While paresthesia may persist temporarily due to chronic nerve compression, complete neurolysis is essential for long-term functional recovery. 7
Conclusion
Complete laparoscopic excision and neurolysis is a safe and effective treatment for sciatic nerve endometriosis, offering significant neurological relief and improving the fertility landscape for patients with severe DIE.
Authors’ Contributions
S.I.: Conceptualization, methodology, writing—original draft, writing—review and editing, and visualization (video editing). A.C., C.Y., M.C., and R.N.: Review and editing. J.d.S.: Writing—review and editing and visualization (video editing).
Informed Consent
Written informed consent was obtained from the patient for the publication of this case report and the use of the surgical video/images.
Footnotes
Acknowledgment
The authors would like to express their deep appreciation to Dr. Raquel Sanz (Radiology Department, MD Anderson Cancer Center Madrid, Madrid) for providing MRI images.
Author Disclosure Statement
The authors declare no conflicts of interest related to this article.
Funding Information
This work did not receive any grant from funding agencies in the public, commercial, or not-for-profit sectors.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.