
Abstract
Objective:
To evaluate the effect of structured hands-on simulation training on obstetrics and gynecology (OB/GYN) residents’ knowledge, confidence, and procedural preference for vaginal natural orifice transluminal endoscopic surgery (vNOTES).
Methods:
This prospective, observational study was conducted between July and August 2022 at a single tertiary medical center. Twelve fourth-year OB/GYN residents completed a didactic online curriculum on adnexectomy and hysterectomy via vNOTES, followed by three monthly hands-on simulation labs using box trainers under direct faculty supervision. Residents’ confidence in key surgical steps and procedural preferences was assessed with pre- and post-simulation surveys. Faculty procedural assessments were recorded for each simulation.
Results:
A total of 49 procedural assessments were completed, including 23 adnexectomies and 26 hysterectomy procedures. Competence was achieved in hysterectomy and adnexectomy by 5 out of 12 and 2 out of 12 residents, respectively. Seven residents completed feedback surveys before and after the simulations. Residents reported a 33% increase in confidence performing anterior and posterior colpotomy. Confidence in transecting the uterosacral ligaments increased from 71% to 85% after simulations. Confidence in transecting the uterine artery via vNOTES doubled from 14% to 28% compared with the laparoscopic approach following simulation. Confidence in performing adnexectomy increased by 15% after simulation; however, there was a 14% reduction in the preference for choosing vNOTES for hysterectomy.
Conclusions:
Hands-on simulation in vNOTES enhances residents’ knowledge and confidence in performing key surgical steps of adnexectomy and hysterectomy. These findings support the integration of vNOTES simulation into residency training programs to improve surgical proficiency.
Introduction
Vaginal natural orifice transluminal endoscopic surgery (vNOTES) is an innovative minimally invasive technique in gynecology by creating a colpotomy, typically in the posterior vaginal wall, vNOTES provides direct access to the peritoneal cavity without the need for abdominal incisions, combining the advantages of vaginal surgery with enhanced endoscopic visualization.
In the last decade, vNOTES has been successfully applied in various gynecological procedures, including ovarian cystectomy, myomectomy, and hysterectomy.1–5 A recent multicenter, prospective cohort study demonstrated that vNOTES high uterosacral ligament suspension is a safe and effective approach for treating pelvic organ prolapse and preventing post-hysterectomy vaginal vault prolapse. 2 Another study demonstrated the safety and feasibility of vNOTES in salpingectomy for ectopic pregnancy, showing comparable outcomes to conventional laparoscopy while offering benefits such as shorter operative time and reduced hospital stay. 3 Baekelandt et al. 5 demonstrated its feasibility for ovarian cystectomy, highlighting its role in fertility-sparing surgery with minimal complications.
Studies comparing vNOTES to conventional gynecological surgeries consistently report favorable safety profiles and improved patient comfort. A systematic review and meta-analysis by Marchand et al. 6 showed that vNOTES hysterectomy was associated with shorter operative times, lower pain scores, and fewer postoperative complications than laparoscopic hysterectomy. The HALON trial confirmed the non-inferiority of vNOTES hysterectomy compared to total laparoscopic hysterectomy, with a higher rate of same-day discharge. 4 Additionally, the NOTABLE trial found vNOTES adnexectomy to be associated with shorter operating times, lower pain scores, and reduced analgesic use. 7 A systematic review by Benton-Bryant et al. 1 further reinforced its feasibility across benign gynecological procedures, demonstrating low conversion rates. Finally, a large international registry-based cohort study found a low overall complication rate (3.2% intraoperative, 2.5% postoperative), with most complications occurring during a surgeon’s early learning curve. 8
Given the increasing adoption of vNOTES, integrating this approach into gynecological surgical training has become imperative. However, limited data exist on the impact of structured training programs on resident competency and confidence in performing vNOTES. This study aimed to evaluate the effectiveness of hands-on simulation training in improving residents’ perception, knowledge, and confidence in performing vNOTES procedures.
Materials and Methods
This prospective observational study was conducted at a single tertiary medical center between July and August 2022. Fourth-year gynecology residents participated and were evaluated by seven faculty surgeons with experience in the vNOTES approach.
All residents first completed a structured didactic online training program covering the theoretical principles and stepwise techniques for adnexectomy and hysterectomy via vNOTES, provided by Applied Medical©. Following this, three hands-on simulation labs were conducted monthly (Table 1). During each session, residents performed both procedures under the direct supervision of experienced vNOTES surgeons, who provided real-time guidance and feedback. Each resident’s technical performance was assessed based on procedural accuracy, adherence to surgical steps, and overall competence.
Hands-On Simulation Labs

Adnexectomy/Hysterectomy performed via vaginal natural orifice transluminal endoscopic surgery.
Residents’ self-reported knowledge and confidence in performing vNOTES procedures were assessed using surveys administered before and after the simulation program. Survey items addressed the cardinal surgical tasks of vNOTES, including anterior and posterior colpotomy, transection of the uterosacral ligaments, and uterine artery ligation. Changes in residents’ preferences for selecting vNOTES versus laparoscopic approaches were also evaluated before and after the simulation sessions to assess the impact of training on surgical decision-making.
Statistical analysis
Demographic information for the study population was collected as part of the pre-evaluation questionnaire. Continuous variables were reported as means with standard deviations or as medians with interquartile ranges, as appropriate, while categorical variables were presented as frequencies and percentages. All statistical analyses were performed using IBM SPSS Statistics, version 19 (IBM Corporation, Armonk, NY).
Trial registration
This study did not involve patient care or human subjects and was therefore exempt from the Institutional Review Board (IRB); no IRB approval number was required. Informed consent was obtained from all resident participants prior to inclusion in the simulation training and data collection. As the study did not involve patients or identifiable patient information, no clinical consent was required.
Results
A total of 12 fourth-year obstetrics and gynecology (OB/GYN) residents participated in the vNOTES simulation program conducted between July and September 2022. All residents completed online didactic training, followed by three structured hands-on simulation labs, during which each resident performed both vNOTES adnexectomy and hysterectomy. A total of 49 procedural assessments were completed during the study period, 23 adnexectomies and 26 hysterectomies, under the supervision and evaluation of seven experienced faculty members.
By the end of the program, procedural competence in adnexectomy and hysterectomy using the vNOTES approach was achieved by 2 out of 12 and 5 out of 12 residents, respectively. Pre- and post-simulation surveys were completed by seven residents and demonstrated an increase in confidence across multiple surgical steps. Confidence in performing both anterior and posterior colpotomies increased by 33% following the simulation training. The proportion of residents reporting confidence in transecting the uterosacral ligaments increased from 71% before the training to 85% after. Confidence in transecting the uterine vessels during vNOTES doubled, rising from 14% to 28% post-simulation. Residents also reported a 15% increase in their confidence to perform adnexectomy using the vNOTES approach.
Despite these technical gains, post-simulation responses revealed a shift in procedural preference. When asked whether they would feel more comfortable performing hysterectomy using the vNOTES approach, fewer residents favored vNOTES after the simulation sessions. Pre-simulation, 57% of residents preferred using vNOTES for hysterectomy, while 29% preferred the non-vNOTES approach, and 14% were unsure. After the simulation, 43% preferred vNOTES, 14% preferred the non-vNOTES route, and 43% were unsure (Fig. 1).
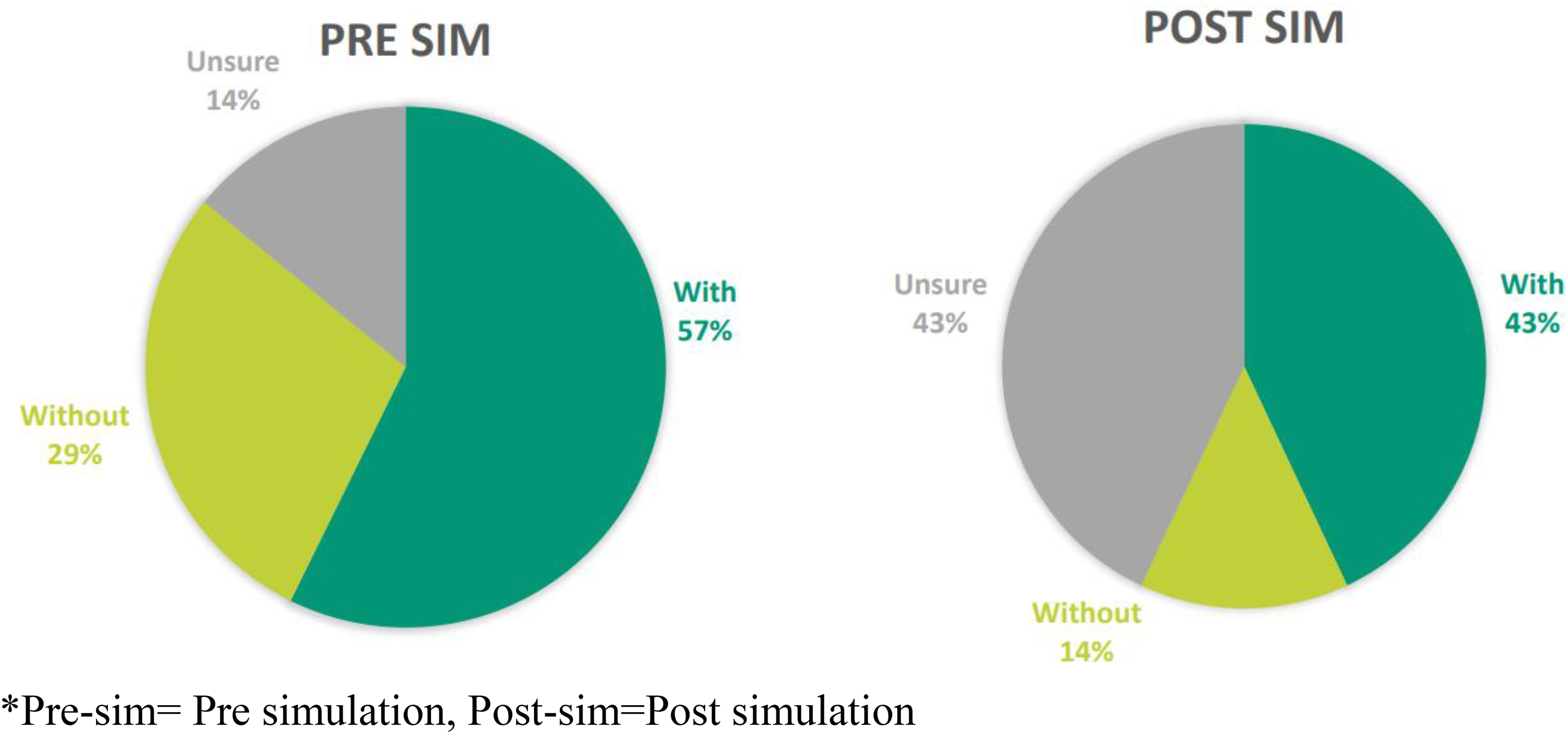
Residents’ preference to perform hysterectomy by vaginal natural orifice transluminal endoscopic surgery approach.
Discussion
The study evaluated the impact of a structured, simulation-based curriculum on OB/GYN residents’ confidence and perceived competency in performing vNOTES adnexectomy and hysterectomy. Following a combination of online didactics and repeated hands-on sessions using box trainers, residents demonstrated increased confidence in key vNOTES-specific surgical steps, including anterior and posterior colpotomy and uterosacral ligament transection. While confidence improved across several domains, some residents continued to express a preference for laparoscopy over vNOTES for hysterectomy. These findings emphasize the growing importance of structured simulation-based curricula in modern surgical education, particularly for emerging minimally invasive approaches such as vNOTES. As operative exposure during residency becomes increasingly constrained, simulation provides trainees with a safe environment for repetitive practice, technical familiarization, and progressive skill acquisition prior to clinical implementation.
Surgical training during residency is a comprehensive process designed to develop the technical and cognitive skills necessary for independent practice. Traditional training models have evolved significantly due to changes in educational environments and the increasing complexity of surgical procedures. 9 Simulation-based training has become an integral component of surgical education, particularly in minimally invasive surgery (MIS). This approach provides a safe and controlled environment for residents to practice and refine their skills without compromising patient safety. The Society of American Gastrointestinal and Endoscopic Surgeons has been instrumental in developing standardized simulation curricula, such as the Fundamentals of Laparoscopic Surgery and the Fundamentals of Endoscopic Surgery, which are widely adopted in residency programs.9,10
In gynecology, simulation-based training has become an essential component of surgical education, bridging the gap created by decreasing surgical exposure during residency and the increasing complexity of minimally invasive techniques. 11 A randomized controlled trial validated a standardized laparoscopy curriculum, demonstrating that residents trained through simulation outperformed those receiving conventional residency training in operative performance. 12 Another study emphasized that simulation allows for structured skill acquisition in a controlled environment, enabling residents in gynecology to practice procedures repetitively and gain competency before performing surgeries on patients. 13 Additionally, simulation-based curricula have been shown to help residents develop critical decision-making skills and improve confidence in performing complex procedures. A recent study evaluating the proctored learning curve of vNOTES hysterectomy in experienced surgeons demonstrated that competence was achieved after 18 cases, with specific steps like anterior colpotomy and right uterine artery transection requiring longer to master—underscoring the need for structured, step-specific training in vNOTES. 14 Despite these advances, simulation training specific to vNOTES remains largely unexplored. This study addresses this gap by introducing a targeted simulation experience for vNOTES procedures, which showed meaningful gains in resident confidence across several surgical steps, supporting its potential as a valuable educational tool in gynecological endoscopy. Such simulation models may be particularly relevant for surgical educators and residency programs seeking structured methods to introduce emerging minimally invasive techniques while maintaining a supervised and low-risk learning environment.
Virtual reality simulators and box trainers are among the most effective types of simulation-based training for MIS. 15 A systematic review and meta-analysis confirmed that both high- and low-fidelity simulators significantly enhance laparoscopic surgical competency. High-fidelity simulators, including virtual reality trainers, were particularly effective in improving technical proficiency and reducing errors and operative times, while low-fidelity models, such as box trainers, improved technical competency but showed no significant effect on procedure duration. 16 A Cochrane review further supported the use of box trainers in laparoscopic surgery, demonstrating that they significantly improve operative performance and may reduce operative time and hospital stay after initial procedures. However, further research is needed to fully understand their long-term educational and clinical impact. 17
While simulation-based training is well established in laparoscopic gynecological surgery, there is a notable lack of literature on simulation training specific to vNOTES. To date, only one study has described a vNOTES presacral fixation simulation model for sacrocolpopexy, aimed at enhancing trainee preparedness for this technically challenging procedure. 18 To our knowledge, this is the first study to evaluate the impact of a structured, hands-on simulation curriculum using a box trainer for vNOTES adnexectomy and hysterectomy in OB/GYN residents, highlighting its role in enhancing resident confidence and skill acquisition in this surgical approach.
Given that vNOTES is a distinct surgical technique with different visual orientation and anatomical access compared to laparoscopy, it is critical to assess the effectiveness of simulation-based training specifically for this modality. This is further supported by recent findings showing that while simulation effectively improves laparoscopic skills, it does not yield the same benefits for robotic surgery, underscoring the importance of tailoring training to the specific surgical platform being taught. 19 A randomized controlled trial by Kanitra et al. 20 demonstrated that laparoscopic training improved robotic performance, but the reverse was not true—robotic training did not enhance laparoscopic skills—further emphasizing the value of platform-specific simulation approaches. This distinction may also help explain our study’s findings that, despite improved confidence in specific vNOTES steps, 14% of residents reported decreased preference for using vNOTES over laparoscopy for hysterectomy. This may reflect the fact that residents are still more familiar with and extensively trained in laparoscopic techniques. It is possible that with further structured vNOTES training and increased clinical exposure earlier during training, this preference may shift as familiarity and proficiency continue to increase.
One of the main strengths of our study is that it is the first to assess a structured, hands-on simulation-based training curriculum using a box trainer specifically designed for vNOTES adnexectomy and hysterectomy within an OB/GYN residency program. The study was conducted at a single high-volume, tertiary academic center with experienced faculty in the vNOTES approach and included repeated procedural simulations, allowing residents to perform and be assessed on both procedures multiple times. Additionally, combining didactic training with hands-on simulation provided a comprehensive educational experience that closely mirrors the evolving trends in surgical education. The use of both subjective feedback (surveys) and objective procedural evaluations supports a more robust understanding of how simulation impacts resident confidence and perceived skill development.
The study has several limitations that need to be acknowledged. First, the sample size was small, with only 12 residents participating and only 7 completing pre- and post-simulation surveys. Accordingly, these findings should be interpreted as preliminary educational outcomes from a pilot simulation experience, which may limit generalizability and preclude definitive conclusions regarding operative competency transfer. Second, the assessment of competence was based on faculty evaluations and self-reported confidence, without independent objective structured assessments (e.g., Objective Structured Assessment of Technical Skills scores) or long-term follow-up to determine actual operative performance in the clinical setting. Third, the study was limited to a single institution, and the findings may not be applicable to programs with different levels of vNOTES experience or surgical volume. Future studies with larger, multi-institutional cohorts and long-term clinical follow-up are needed to evaluate whether continued exposure and expanded simulation training can shift resident preference and real-world adoption of the vNOTES approach.
Conclusions
As vNOTES continues to gain acceptance as a minimally invasive option for benign gynecological surgery, establishing effective training models becomes essential to support its safe and widespread adoption. Our findings suggest that structured, simulation-based training may enhance resident confidence in performing specific vNOTES steps but may not be sufficient alone to influence procedural preference. Future steps should include the development of standardized, validated simulation curricula for vNOTES, integration of objective competency metrics, and efforts to extend simulation into real-world operative mentorship. Incorporating vNOTES earlier and more consistently into residency exposure may be key to preparing the next generation of gynecological surgeons for this evolving technique.
Ethical Considerations
This study did not involve patient care or human subjects and was therefore exempt from the Institutional Review Board (IRB); no IRB approval number was required. Informed consent was obtained from all resident participants prior to inclusion in the simulation training and data collection. As the study did not involve patients or identifiable patient information, no clinical consent was required.
Authors’ Contributions
A.M.-S. conceived and designed the study, supervised its execution, coordinated the simulation sessions, and critically revised the article. R.M. drafted and wrote the article, prepared and edited tables and figures, and finalized the submission. M.H., R.J., O.D., and M.L. participated in the simulation training implementation, data collection, and article review. A.M. contributed to study design, data interpretation, supervision, and provided critical revisions to the article. A.B. provided senior oversight, supervision, study conceptualization, interpretation of findings, and final approval of the article.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.