
Abstract
Background:
Despite an increase in the performance of minimally invasive hysterectomy, opioid overprescribing postoperatively is common and can contribute to chronic long-term use. This study evaluated local/regional patterns of immediate opioid use after benign hysterectomy and identified quality gaps in physician prescribing practices.
Methods:
A retrospective chart review was conducted on all hysterectomies performed for benign indications at two tertiary care hospitals between January and December 2019. The primary outcome was opioid use in morphine milligram equivalents (MMEs) within the first 24 hours after surgery. Secondary outcomes were opioid prescribing patterns in different patient populations and length of hospital stay. A survey on opioid prescribing practices was conducted among gynecological providers.
Results:
A total of 669 patient records were reviewed between January and December 31, 2019. Median opioid use <24 hours following benign hysterectomy was 10 and 15MMEs, at respective sites. Nearly 30% of patients used no opioids postoperatively, 97% were opioid naïve. The presence of at least one postoperative pain diagnosis significantly increased opioid use from 10.9 MME to 22.5 MME (p < 0.001). Postoperative opioid use was lower overall with a minimally invasive approach to hysterectomy (p = 0.009 total MME). Gynecological attendings were more likely than trainees to evaluate for risks of opioid dependency before prescribing.
Conclusion:
Patients undergoing hysterectomy for benign indications used minimal to no opioids in the immediate in-hospital postoperative period. Future directions are needed to investigate the role for integrated perioperative risk assessments to guide opioid prescribing.
Keywords
Introduction
Chronic postsurgical opioid dependency is impacted by opioid overprescribing in the perioperative period and contributes to the ongoing opioid epidemic worldwide, with 80% of deaths from drug use related to opioid misuse.1–4 Persistent postoperative opioid use (>90 days after surgery) occurs in 5.9%–6.5% of patients after minor and major surgical procedures. 5 Within gynecological surgery, long-term postoperative opioid after benign hysterectomy remains as high as 7.1% 3 years after surgery. 6 Chronic postoperative opioid dependency and abuse often begins at the index surgery, but the contribution of inpatient opioid use in the immediate postsurgical setting is not understood.
The immediate postoperative period plays a critical role in shaping analgesic response, but no universal framework exists to assess postoperative recovery or pain control.7,8
These challenges are amplified by increasing adoption of same-day surgery and enhanced recovery after surgery (ERAS) pathways, which reduce hospital stay and postoperative morbidity while shifting pain assessment and management to the outpatient setting.9,10 In gynecology, hysterectomy remains the second most common surgery in women after cesarean section, with a 45% lifetime prevalence.11,12 Despite the rise of minimally invasive hysterectomy, postoperative opioid prescriptions fills have risen 26%–82%, irrespective of hysterectomy routes.13,14
This discrepancy in postoperative opioid fills highlights key gaps in opioid management in the immediate inpatient period with decreasing length of hospital stay. Opioid overprescribing frequently does not correlate with actual pain requirements. 15 In a survey of patients after elective hysterectomies, 65% of patients used <50% opioids prescribed, and 16% used none. 16 Studies show that absence of accurate opioid use measurement after elective surgeries leads to up to 70% overprescribing, a problem exacerbated by increasing rates of same-day surgeries.17,18
Variation in opioid prescribing across surgical training levels has been documented, but actionable quality gaps remain poorly defined. 19 One prospective qualitative study found that gynecologists prescribe twice the opioids typically used after benign hysterectomy. 20 Similarly, a survey of American obstetrics and gynecology (Ob/Gyn) residents demonstrated substantial prescribing variation influenced by hospital culture, provider insight, limited formal training, and lack of individualized prescribing. 21 Discrepancies also exist between perioperative prescribing and persistent opioid use. A recent meta-analysis of >350,000 women reported a 5% rate of persistent opioid use after hysterectomy, independent of surgical route, with younger age, smoking, back pain, and fibromyalgia identified as significant risk factors. 22 Despite well-established knowledge of overprescribing after benign hysterectomy, granular local and regional data is lacking to guide actionable interventions to address quality gaps in care and changes in opioid prescribing practices.
Therefore, this study aims to describe local and regional opioid prescribing patterns in the immediate postoperative period in-hospital after elective, benign hysterectomy. Using a mixed-methods approach, we examined patient opioid use quantitively and provider prescribing practices qualitatively to identify key quality gaps in postoperative opioid management.
Materials and Methods
This descriptive study involved a mixed-method approach including a retrospective chart review and a gynecological surgery provider survey.
Part 1: Retrospective chart review
A retrospective chart review was conducted of all elective hysterectomies performed for benign indications at the Peter Lougheed Center (PLC) and South Health Campus (SHC), two tertiary-care hospitals in Calgary, Alberta, between January 1 and December 31, 2019. Data collection was limited to 2019 based on the timing University of Calgary Research Ethics Board (REB21-0290) approval. PLC and SHC are large academic-community hospitals each performing 200–300 elective hysterectomies annually, representing a substantial volume and diversity of benign hysterectomies. During the study period, SHC had an established same-day discharge protocol, whereas implementation at PLC was ongoing, providing an opportunity to evaluate immediate postoperative opioid use across different perioperative care pathways. All hysterectomy approaches were included (abdominal, vaginal, laparoscopic, or combined).
Data were collected from electronic medical records (Sunrise Clinical Manager© [SCM]). Preoperative medical history, surgical history, opioid use, and surgical indications were abstracted from gynecological surgery consultation notes. Patients were classified as opioid-naive if there was no documented opioid use in consultation notes or prior hospital encounters, acknowledging that outpatient prescription data were unavailable. Patients were classified as not opioid-naive if any opioid use was documented in consultation notes or previous hospital encounters in SCM. As outpatient postoperative opioid prescription and consumption data were inaccessible, opioid-naive status was based solely on preoperative opioid use history.
Surgical indication was documented from the gynecologist’s preoperative consultation note. Preoperative and postoperative diagnoses were documented as reported from the surgeon’s operative dictation. Intraoperative details including surgical approach, intraoperative findings, and/or intraoperative complications were documented from the operative report. Postoperative course in-hospital, final postoperative diagnosis, length-of-stay, type and dosage of opioids consumed in-hospital, and non-opioid analgesic adjuncts were documented from the medication administration record. Data from postoperative emergency room presentations or hospital readmissions were collected. Data from SCM were extracted with support from Data and Analytics services at Alberta Health Services.
Opioid use was converted to and reported as morphine milligram equivalent (MME) units. Conversions were performed according to the 2017 Canadian Guideline for Opioids for Chronic Non-Cancer Pain opioid conversion table. Conversion ratios were reported as follows: Hydromorphone 5:1, codeine 0.15:1, oxycodone 15:1, tramadol 0.1:1. 14 Fentanyl patch conversions were based on the BC Guidelines for Pain and Symptom Management. 15
Part 2: Gynecological surgery provider surveys
Following completion of the primary retrospective analysis, an exploratory provider survey was added to investigate prescribing factors underlying the observed results. As the survey was not part of the original study, a protocol amendment and additional ethics approval were further obtained. The survey was distributed electronically through Qualtrics XM, a secure research ethics board–approved platform, to all gynecological attendings, minimally invasive gynecology fellows, and Ob/Gyn residents in Calgary. Responses were anonymized and collected over a 4-month period between April and October 2022. The survey asked respondents to self-report postoperative analgesia and opioid-prescribing education/training, pain management and opioid-prescribing practices following benign hysterectomy, and when they provide postoperative care and pain management counseling.
Statistical analysis
We compared baseline operative characteristics between those who did and did not use opioids 24 hours postoperatively. The primary outcome was opioid use in MMEs within the first 24 hours after surgery. Secondary outcomes were opioid prescribing patterns in different patient populations and length of hospital stay. For continuous variables, comparisons between two groups were performed using a t-test or Wilcoxon rank sum test, and ANOVA or the Kruskal-Wallis test was used for comparisons across multiple groups. Chi-square or Fisher’s exact tests were used for categorical variables. A p-value of <0.05 was considered statistically significant. All statistical analyses were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA).
Ethics
This research study was approved by the University of Calgary’s Conjoint Health Research Ethics Board (REB21-0290). A waiver of consent for individual patient consent was obtained for access to pre-existing databases.
Results
In total, 696 patient records of elective hysterectomies performed for benign indications were reviewed between PLC (N = 426) and SHC (N = 270) from January 1, 2019, to December 31, 2019. A total of 27 records were excluded due to duplicate records, missing postoperative data, or in cases where surgery was not performed due to cancellation. In total, 669 patient records were included in the final analysis, 410 from PLC and 259 from SHC.
The median opioid amount used within 24 hours after surgery, regardless of surgical route, was 15 MME (IQR 0–40 MME) at PLC and 10 MME (IQR 0–30 MME) at SHC, p = 0.012, including all patients discharged home <24 hours postoperatively (Fig. 1). Across both sites, 27.8% at PLC and 29.7% at SHC of patients used no opioids postoperatively during admission, regardless of hysterectomy approach (Fig. 2). Given the low proportion of patients admitted ≥24 hours at SHC (96% same-day-discharge rate), opioid use ≥24 hours was assessed only at PLC (4.2% same-day-discharge rate). Beyond 24 hours, 90.2% at PLC used no opioids, 6.1% of patients used 1–30 MME, and 3.7% used >30 MME (Fig. 3). Among patients who did not require postoperative opioids, 97.4% were opioid-naive preoperatively (Table 1). Use of non-opioid medications, either as monotherapy or in combination with non-opioid analgesics, did not differ between patients who did and did not use opioids within the first 24 hours postoperatively (Supplementary Table S1).
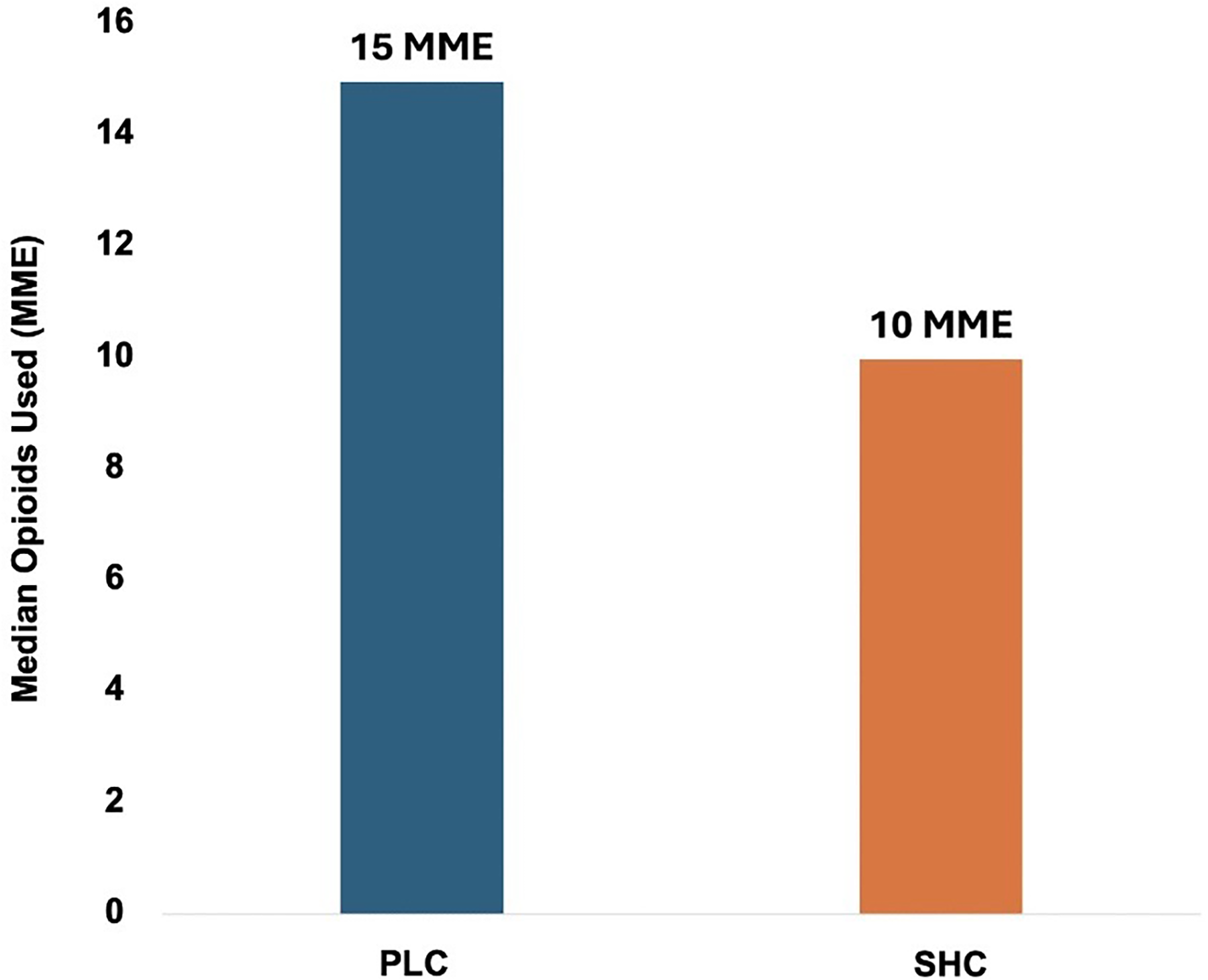
Opioids Use in First 24 Hours Postoperatively. Median opioids used in the first 24 hours after benign hysterectomy, across all surgical approaches, was 15 morphine milligram equivalents (MME) (IQR 0–40) at PLC and 10 MME (IQR 0–30) at SHC, p = 0.012.
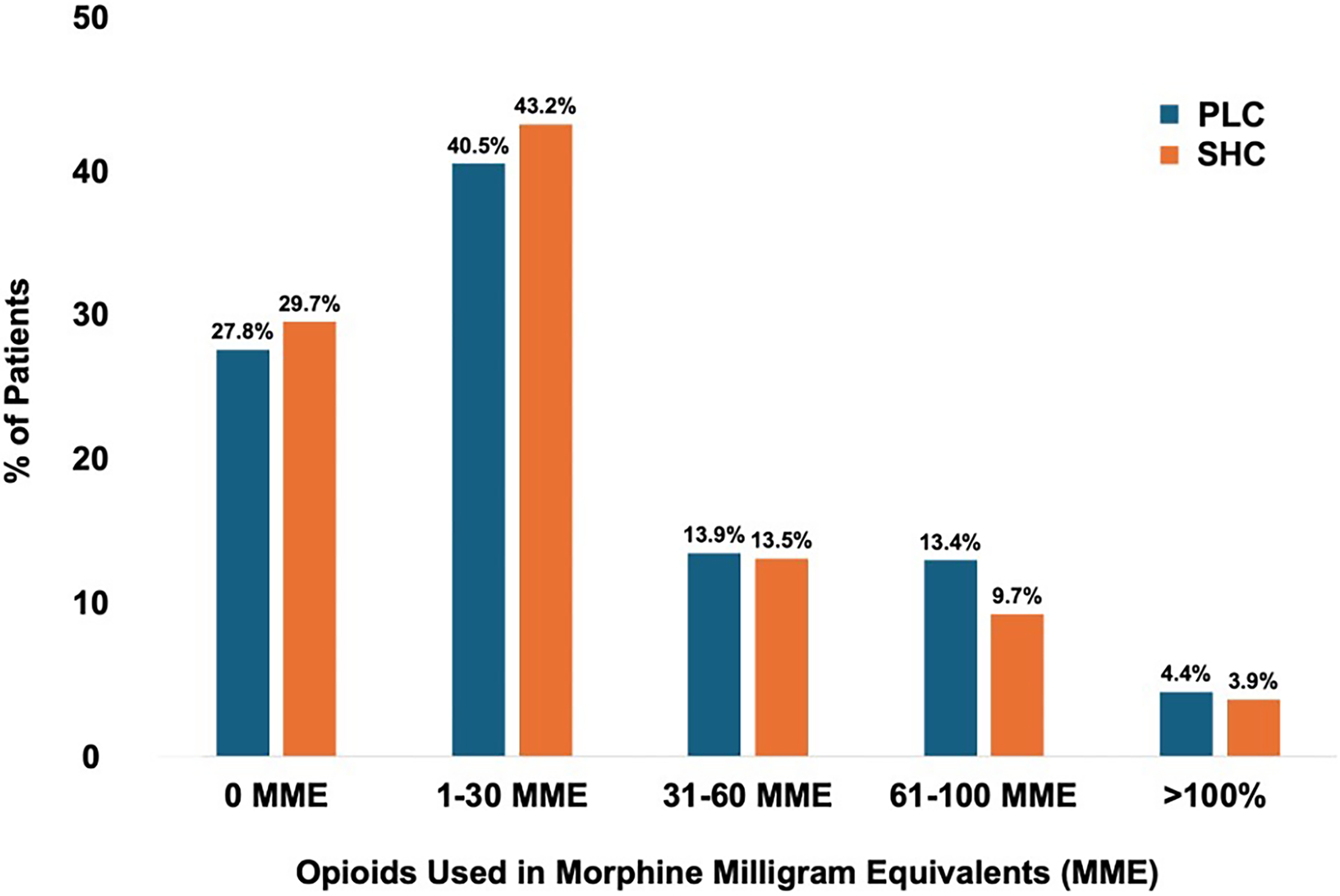
Total opioids used postoperatively in-hospital. Majority of postoperative patients used none or minimal opioids postoperatively after elective hysterectomies for benign indications. 27.8% of patients at PLC and 29.7% of patients at SHC did not use any opioids regardless of the route of surgery, p = 0.025.
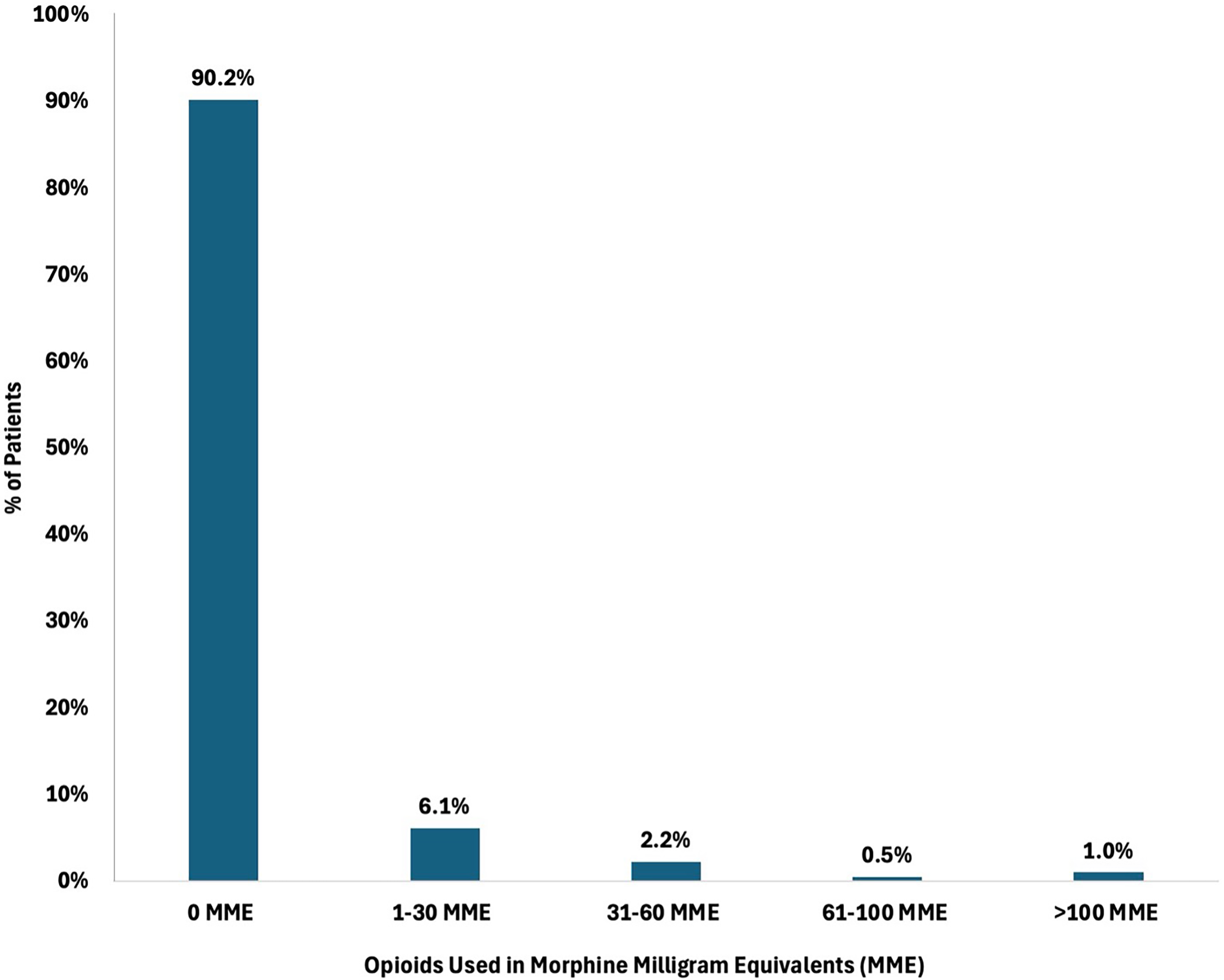
Opioid use by postoperative patients at PLC beyond 24 hours. Majority of postoperative patients did not require any opioids beyond 24 hours after elective hysterectomy. 90.2% of patients did not use any opioids beyond 24 hours. SHC patients not shown due to high proportion of same-day-discharge at SHC.
Demographic Characteristics Based on Opioid Use within 24 Hours Postoperatively After Elective Hysterectomy
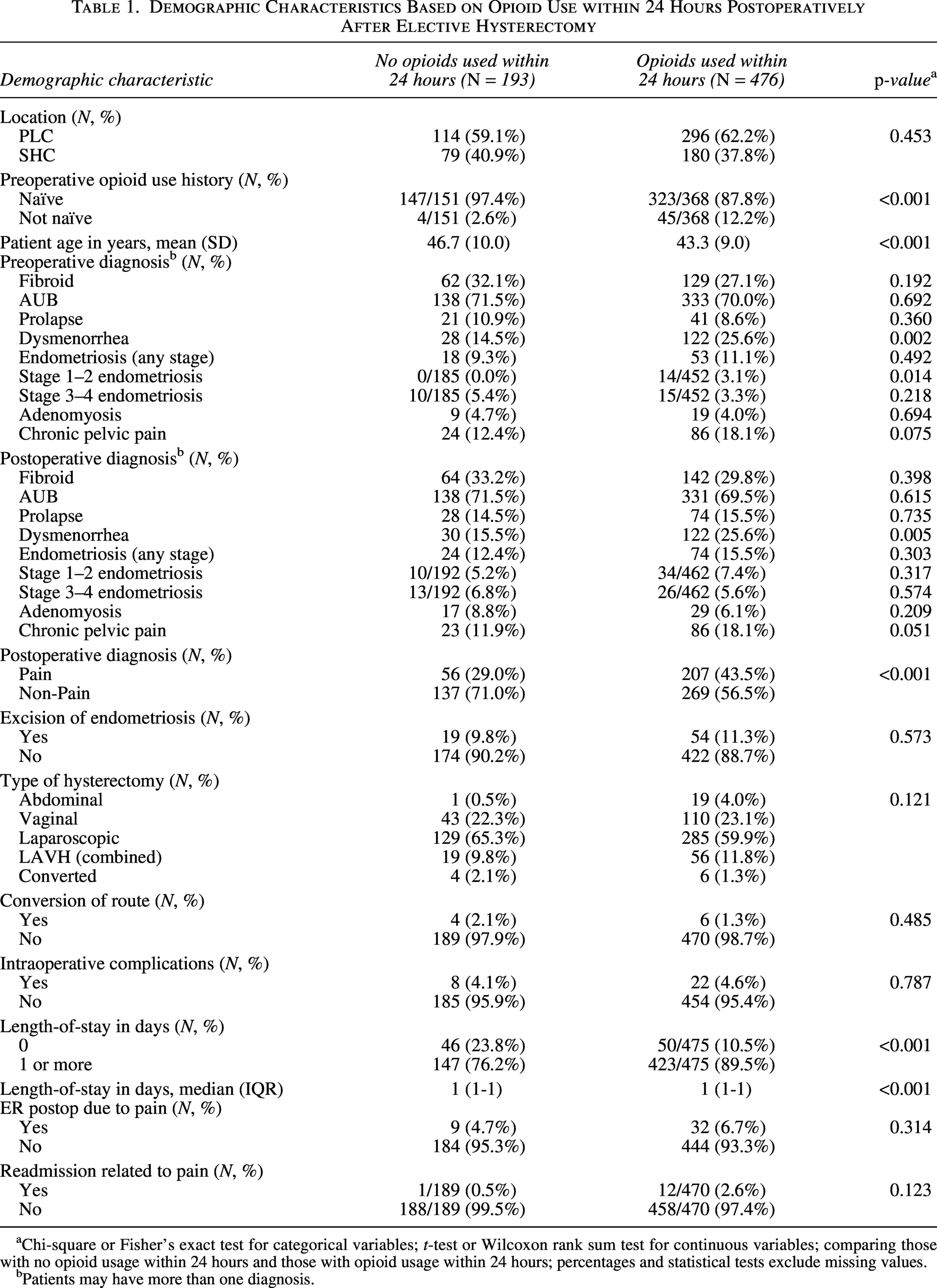
Chi-square or Fisher’s exact test for categorical variables; t-test or Wilcoxon rank sum test for continuous variables; comparing those with no opioid usage within 24 hours and those with opioid usage within 24 hours; percentages and statistical tests exclude missing values.
Patients may have more than one diagnosis.
Baseline demographic characteristics are summarized in Table 1. Younger patients were more likely to use opioids <24 hours postoperatively (43.3 years in opioid users versus 46.7 years in non-opioid users, p < 0.001). Excision of endometriosis, conversion of surgical route, nor the presence of intraoperative complications increased postoperative opioid use. Delayed postoperative presentations or hospital readmissions for pain-related reasons did not differ between patients who used or did not use opioids.
With respect to surgical indication, dysmenorrhea diagnosed preoperatively (14.5% in non-opioid users versus 25.6% in opioid users, p = 0.002) or postoperatively (15.5% in non-opioid users versus 25.6% in opioid users, p = 0.005) increased the risk of opioid use postoperatively (Table 1). The presence of at least one postoperative pain diagnosis (endometriosis, adenomyosis, or chronic pelvic pain) significantly increased postoperative median opioid use <24 hours to 22.5 MME (IQR 5.0–47.5 MME) compared to 10.9 MME (IQR 0–30 MME) if no prior pain diagnosis was documented, p < 0.001 (Table 2). Total opioid use in-hospital was also increased among patients with a postoperative pain diagnosis at 22.5 MME (IQR 5.0–47.5 MME) compared to 13 MME (IQR 0–33.8 MME) without a pain diagnosis, p < 0.001 (Table 2).
Postoperative Opioid Use by Pain Diagnoses
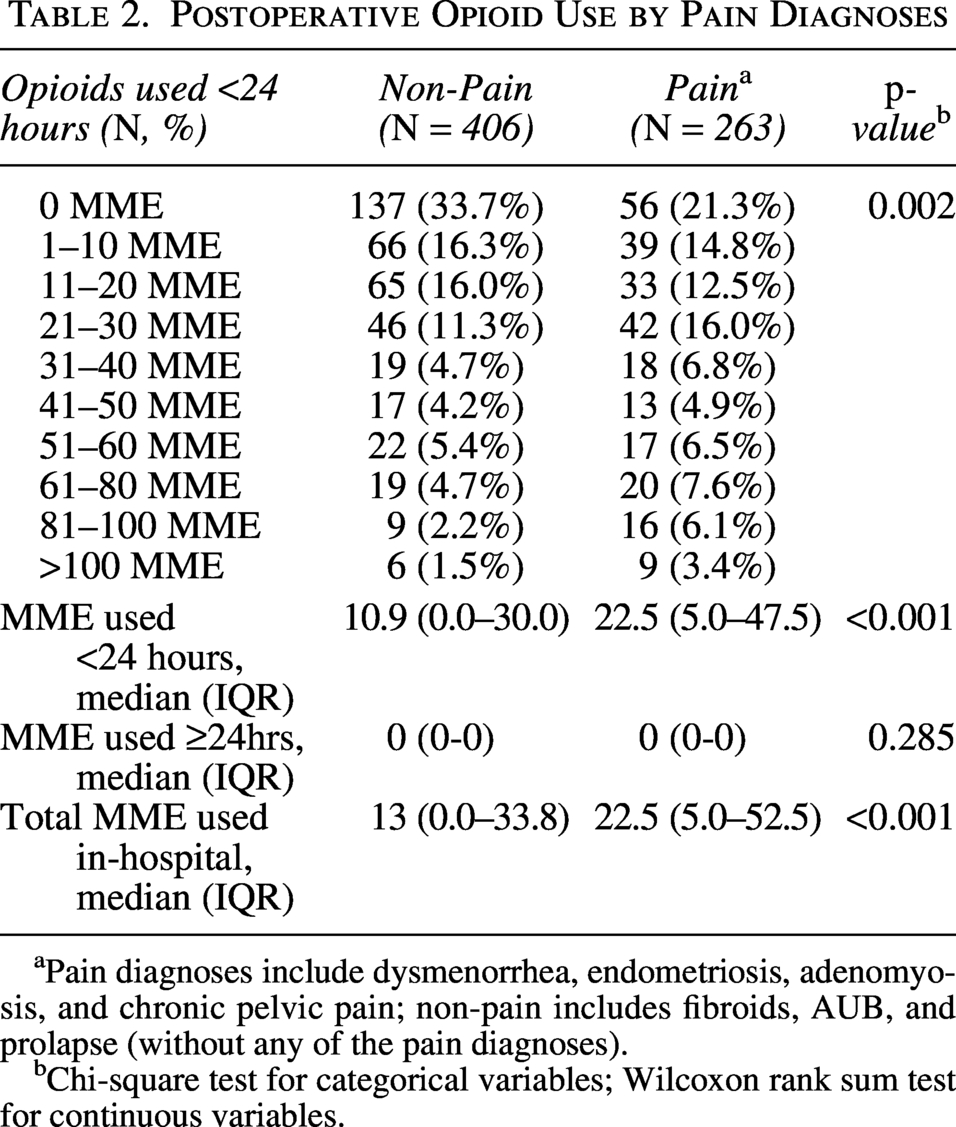
Pain diagnoses include dysmenorrhea, endometriosis, adenomyosis, and chronic pelvic pain; non-pain includes fibroids, AUB, and prolapse (without any of the pain diagnoses).
Chi-square test for categorical variables; Wilcoxon rank sum test for continuous variables.
Postoperative opioid use by surgical approach is summarized in Table 3. Although the proportion of patients requiring opioids did not differ by surgical approach (Table 1), total in-hospital opioid use was significantly lower following minimally invasive hysterectomy (15 MME, IQR 0–33.8 for laparoscopic and 15 MME, IQR 0–45 for vaginal) than abdominal hysterectomy (34.4 MME, IQR 10.25–85.0; p = 0.009). In fact, at all points in the patient’s admission, opioid use was significantly less in the minimally invasive compared to the abdominal hysterectomy patients: within 24 hours (18.75 MME, IQR 8.75–40.0 abdominal vs. 15 MME, IQR 0–30 laparoscopic vs. 15 MME, IQR 0–45 vaginal; p = 0.025) and beyond 24 hours (2.5 MME, IQR 0–37.5 abdominal vs. 0 MME laparoscopic vs. 0 MME vaginal; p < 0.001).
Opioid Use Patterns by Route of Hysterectomy Performed
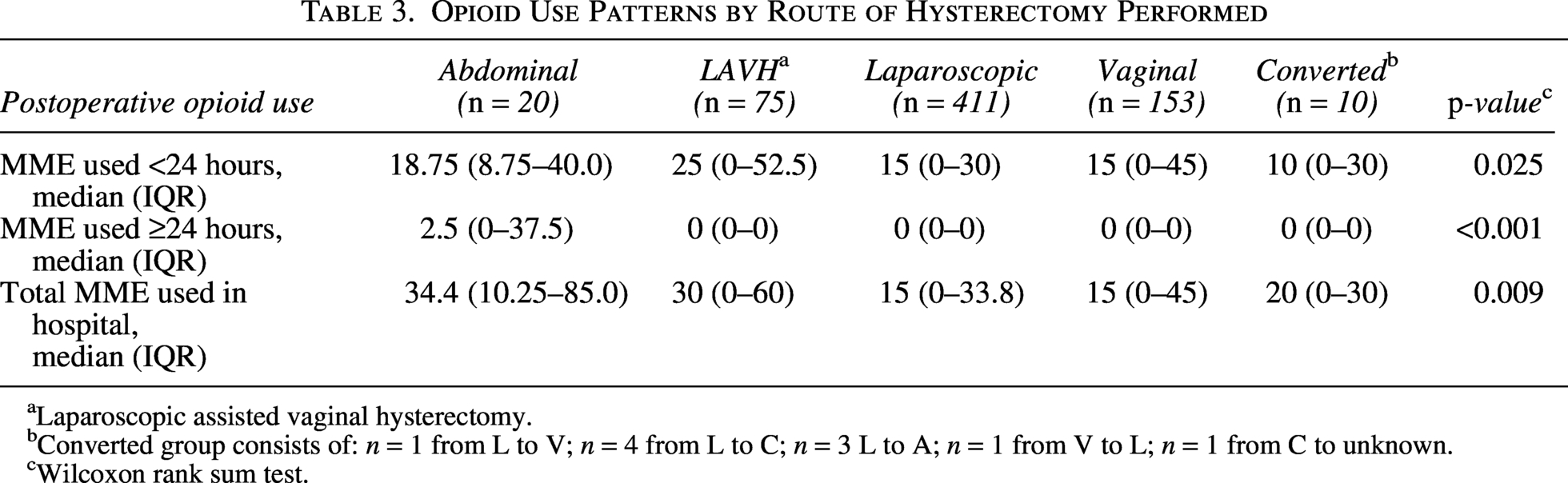
Laparoscopic assisted vaginal hysterectomy.
Converted group consists of: n = 1 from L to V; n = 4 from L to C; n = 3 L to A; n = 1 from V to L; n = 1 from C to unknown.
Wilcoxon rank sum test.
Same-day discharge after elective hysterectomy occurred in 96 patients (14.4%), majority at SHC (N = 92, 95.8%) compared to PLC (N = 4, 4.2%). This reflects the timeline of same-day discharge protocol implementation during the study period, as PLC was still developing a same-day discharge protocol and had substantially fewer same-day discharges than SHC. Overall, 521 patients (77.9%) were discharged on postoperative day 1, and 51 (7.6%) were discharged on postoperative day 2 or later. Median in-hospital opioid use was 5 MME (IQR 0–10), 15 MME (IQR 0–40), and 82.5 MME (IQR 20–120) for patients discharged the same day, on postoperative day 1, and on postoperative day ≥2, respectively (p < 0.001). Patients who were opioid-naive preoperatively were more likely to be discharged the same day (90.1%) or within 24 hours (92.3%), whereas 27.8% of patients admitted beyond 24 hours were not opioid-naive preoperatively (Table 4).
Postoperative Opioid Use by Length of Admission
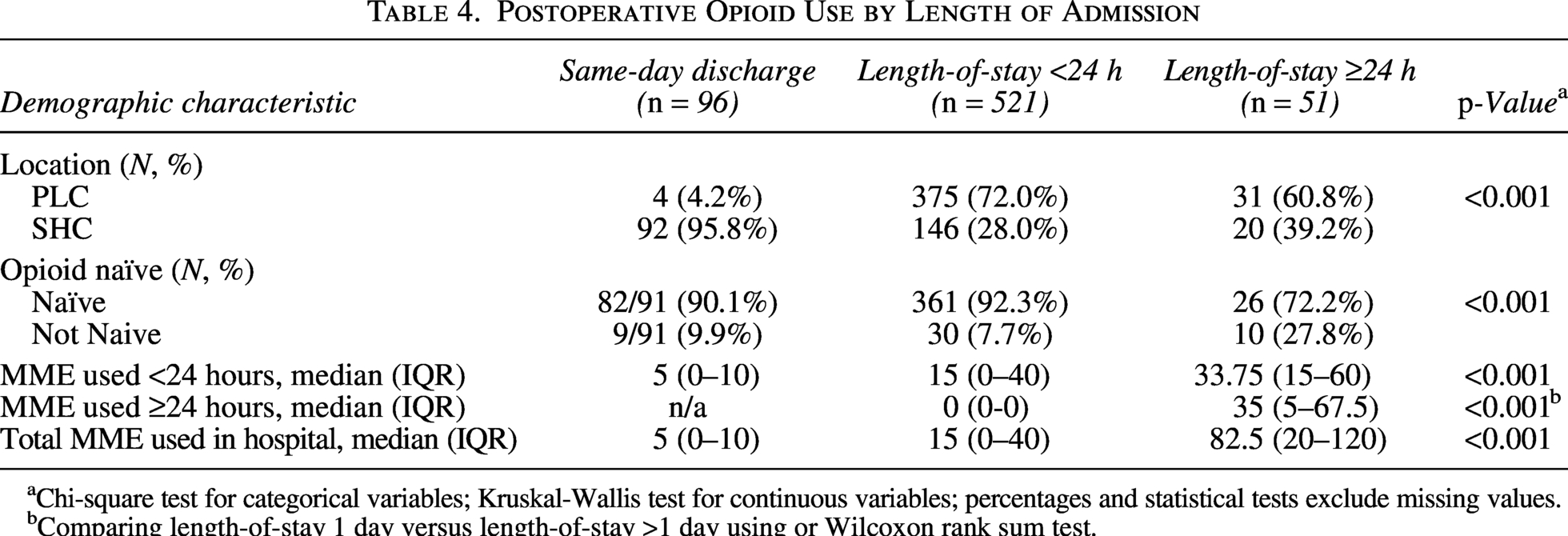
Chi-square test for categorical variables; Kruskal-Wallis test for continuous variables; percentages and statistical tests exclude missing values.
Comparing length-of-stay 1 day versus length-of-stay >1 day using or Wilcoxon rank sum test.
Postoperative provider opioid prescribing patterns
In total, there was a 66% response rate from gynecological attendings, fellows, and resident trainees (Supplementary Fig. S1, N = 65 total respondents, N = 44 gynecology attendings, N = 3 gynecology fellows, N = 18 gynecology residents). There was considerable variation among gynecological providers with regard to assessment of opioid use risk postoperatively. Overall, gynecological attendings were more likely to routinely ask questions around perioperative opioid use risks compared to gynecological trainees (Fig. 4). Gynecology staff were more likely to assess opioid use risk across the perioperative journey from opioid use risks to surgical complications, postoperative prescription fills and follow-up compliance (Fig. 5). Unlike gynecology staff, gynecology residents were limited to in-hospital opioid risk assessments but also less likely to base opioid prescribing on perioperative complications or opioid use in the immediate postoperative period prior to discharge (Fig. 5). In terms of timing for prescribing, attendings and trainees were most likely to write prescriptions at time of discharge as opposed to preoperatively or immediately after completion of the surgery.
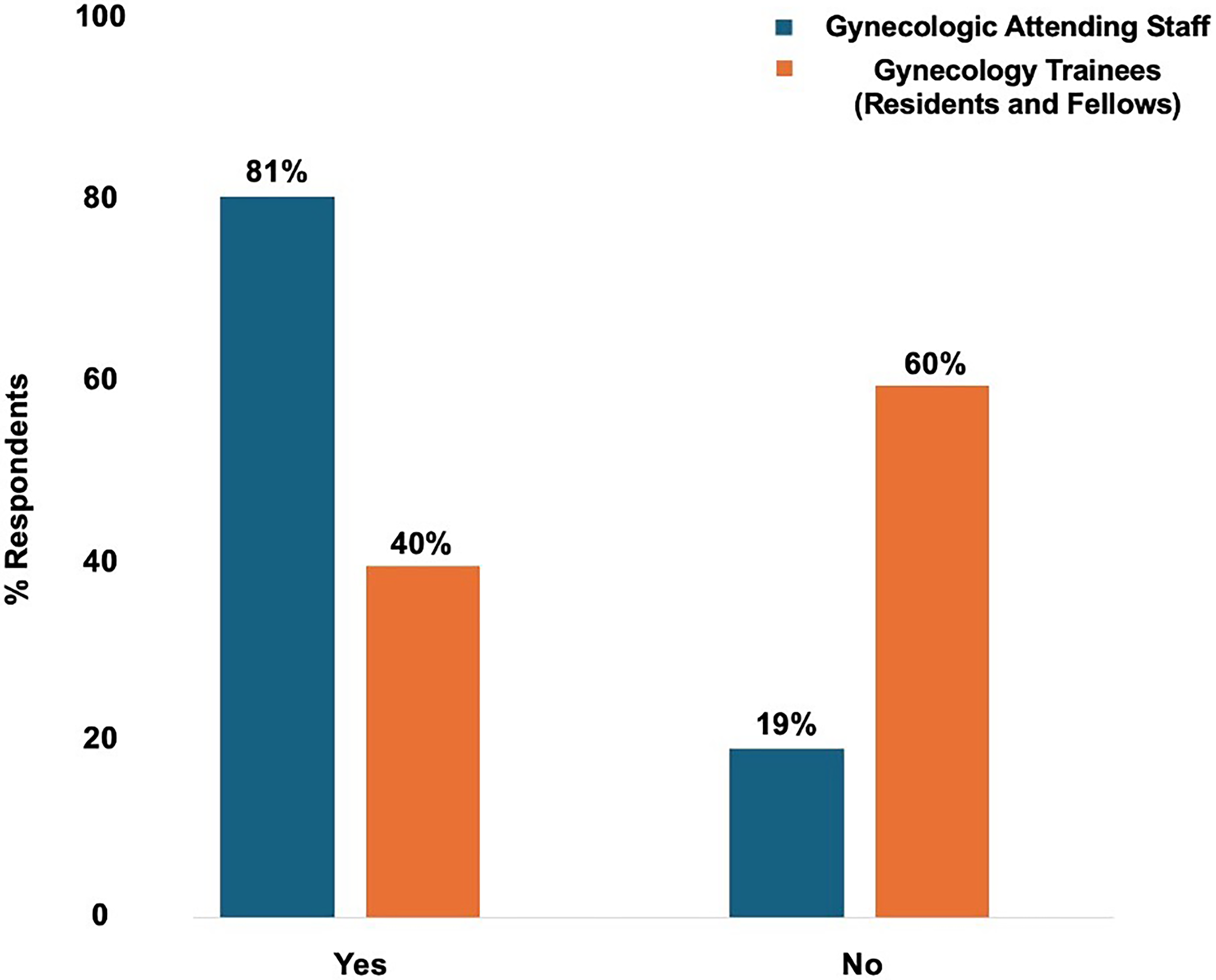
Opioid prescribing patterns among gynecological attendings and trainees. Variation seen in opioid risk assessments used in the perioperative setting based on the type of provider and the level of training. Gynecological attendings were more likely to evaluate a patient’s preoperative risk for opioid use/abuse than residents and fellows.
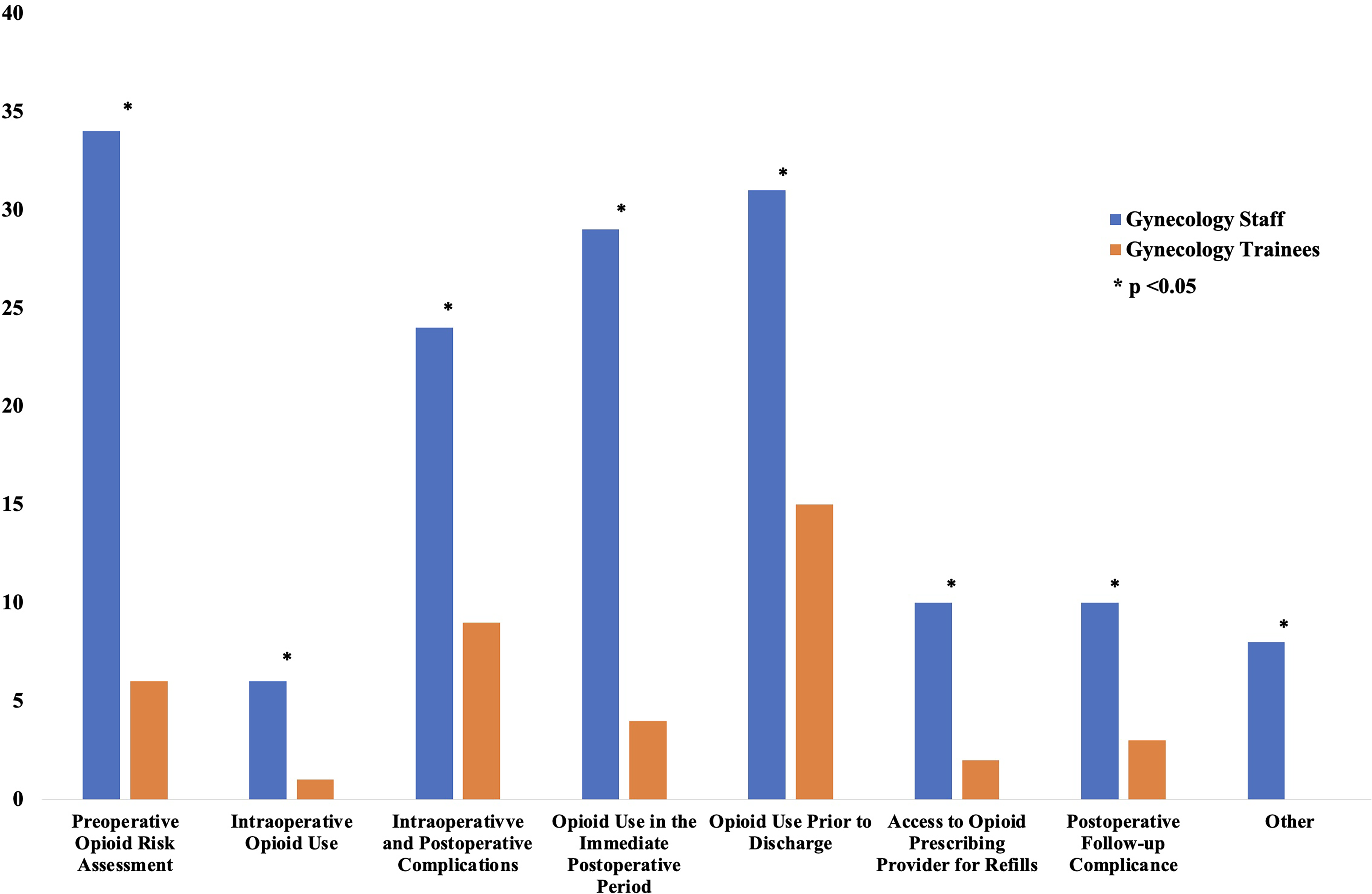
Most Common Predictors Influencing Provider Opioid Prescribing Practices. N = 40 gynecology staff and N = 21 trainees (including gynecology residents and minimally invasive gynecology fellows) were asked to identify factors used to guide opioid prescribing decisions at discharge, including preoperative opioid risk assessment, perioperative opioid exposure, postoperative clinical factors, and follow-up considerations. Multiple responses were permitted. The most frequently selected factors influencing opioid prescribing at discharge were opioid use prior to discharge, opioid use in the immediate postoperative period, preoperative opioid risk assessment, and intraoperative or postoperative complications, all of which were selected more frequently by gynecology staff than trainees. Asterisks indicate statistically significant differences between groups (p < 0.05, by chi-square test). Values represent the number of respondents selecting each response option.
Discussion
In summary, this descriptive study is one of the first to explore both patient use and provider opioid prescribing practices in the immediate postoperative in-hospital period after elective benign hysterectomy using a large retrospective review across two different academic hospitals. We found that most patients use minimal to no opioids after surgery, with a median of 10 MME and 15 MME used in ≤24 hours at the two sites, with <10% using any opioids >24 hours in-hospital. We identified substantial differences in opioid prescribing and perioperative opioid risk assessment between gynecological attendings versus trainees. This study provides local and regional data highlighting the immediate postoperative period as a potential critical window for future interventions aimed at optimizing opioid prescribing practices and reducing the risk of subsequent persistent opioid use.
Prior studies have documented persistent opioid use and its contribution to chronic dependency. This study’s significance is its focus on the immediate in-hospital postoperative period, an important window for postoperative analgesia and a quality gap in prescriber variation. Whereas previous studies have focused primarily on discharge and outpatient opioid use and chronic opioid utilization, this study demonstrates lower opioid consumption in-hospital than anticipated. Opioid use during the immediate in-hospital postoperative period was minimal in our cohort, yet prospective data have demonstrated median outpatient opioid consumption up to 150 MME within 2 weeks following laparoscopic hysterectomy. 23 The immediate postoperative period represents an important opportunistic phase of care as same-day discharge becomes the predominant pathway following elective benign hysterectomy.
Since data collection, same-day discharge protocols have been formalized across Canada, including a 68% increase in one Calgary gynecological division where our study was performed. 24 In this study, 14.4% of patients were discharged home same-day, while another 78.0% were discharged <24 hours, reflecting contemporary hysterectomy recovery timelines. Furthermore, 97% who did not use opioids were opioid-naive preoperatively, and 90.1% were discharged same-day. With increasing standardization of same-day discharge pathways, most postoperative analgesic use will now occur at home. However, our survey showed that most respondents continue to base opioid prescribing on inpatient use, a practice that becomes increasingly challenging as same-day discharges increase. Given increasing adoption of same-day discharge and limited opportunities to assess outpatient opioid use, these findings highlight the need for studies evaluating early postoperative opioid use and perioperative opioid risk assessment, particularly as routine follow-up often occurs 6 weeks after surgery. This underscores the need for comprehensive preoperative risk assessment and stratification.
Although outpatient prescribing could not be assessed, 87.8% of opioid-naive patients were prescribed and used opioids within 24 hours of surgery, suggesting routine immediate postoperative prescribing regardless of preoperative opioid exposure. Existing opioid risk assessment tools (e.g., SOAPP-R, PROMIS-3a, and ORT-O) demonstrate variable performance in non-gynecological surgeries, and no standardized risk assessment tools exist for gynecology.25,26 While ERAS recommends a tiered approach to opioid prescribing, implementation in same-day settings is limited. 27 Integrating validated preoperative risk assessment with tiered pain management strategies may better tailor prescribing to individual risk, particularly in same-day discharge pathways where opportunities to assess postoperative opioid requirements are limited. The discrepancy between the minimal inpatient opioid use observed in our study and the higher opioid consumption reported up to 2 weeks after surgery highlights an important area for future investigation.
Our study showed that the presence of at least one postoperative pain diagnoses was associated with increased postoperative opioid use, consistent with prior evidence linking preoperative pelvic pain with increased postoperative opioid use. 2 Interestingly, in our study, opioid use postoperatively was not affected by surgical approach; however, a minimally invasive hysterectomy led to lower total MMEs use throughout the postoperative admission, consistent with previous findings.28,29 Taken together, these results support the continued expansion of minimally invasive hysterectomy and same-day discharge pathways when clinically appropriate in gynecology.
Variation in surgeon prescribing practices also contributed meaningfully to postoperative opioid use. In our survey, gynecology attendings (who follow patients from clinic through postoperative recovery) regularly incorporated a variety of perioperative opioid risk into postoperative prescribing decisions. In contrast, only a minority of gynecology trainees, who work primarily in inpatient settings, report doing the same. This aligns with literature showing that gynecology residents cite lack of formal training and institutional culture as key contributors to opioid overprescribing. 21 These results emphasize the need for more consistent and formalized training in comprehensive postoperative analgesia, particularly when most gynecological trainees are limited to inpatient settings for training and exposure.
Key strengths include the large sample size and comprehensive evaluation of perioperative opioid risk factors and postoperative analgesia following elective hysterectomy, one of the most performed surgeries. Despite extensive research on opioid use after discharge, this is among the first studies to examine the immediate in-hospital postoperative period. Its retrospective design enabled detailed assessment of analgesic use not captured in administrative databases such as Medicare. Inclusion of two large academic-community hospitals enhances relevance to many health care settings and provides granular insight into hospital- and provider-level practices, identifying local care gaps and informing quality-improvement initiatives. Given the paucity of local/regional data on opioid prescribing and use in clinical practice, this study bridges the gap between high-level evidence from published systematic reviews and practical considerations required for future quality-improvement and implementation initiatives.
A major limitation was the inability to capture outpatient opioid prescriptions or consumption, preventing assessment of discharge overprescribing and its contribution to long-term opioid use. Although limited to a 1-year inclusion period, high surgical volumes at both hospitals yielded a large eligible cohort. As the provider survey was added after completion of the primary analysis, it provided an exploratory rather than analytical comparison of prescribing practices. As a retrospective study, the findings are subject to selection bias and residual confounding. Additionally, PLC was transitioning to a same-day discharge protocol during the study period; therefore, differences in opioid consumption and prescribing between sites may reflect different stages of protocol implementation. Finally, this descriptive, hypothesis-generating study was not designed to evaluate associations between perioperative risk factors and persistent postoperative opioid use.
Conclusions
In conclusion, our study showed minimal opioid use in the immediate in-hospital postoperative period after elective benign hysterectomy. Risk factors including preoperative pain and provider prescribing variation heighten the vulnerability of this window on opioid prescribing. These findings underscore the need for integrated preoperative risk assessment and comprehensive postoperative pain management to reduce variation in this critical in-hospital period amid rising same-day discharge.
Ethics Approval
The study protocol was reviewed and approved by the University of Calgary Conjoint Health Research Ethics Board, Ethics ID: REB21-0290, Aug 5, 2021, Version 3.
Transparency Statement
Dr. Ari Sanders affirms that this article is an honest, accurate and transparent account of the study being reported. No important aspects of the study have been omitted, and that any discrepancies from the study as planned were explained in detail.
Data Sharing Agreement
De-identified data underlying this study are available from the corresponding author upon request and contingent on institutional approval.
Authors’ Contributions
All authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship. Specifically, all authors contributed substantially to the conception and design of the study, data acquisition, analysis and interpretation of data, drafting and critical revision of the article for important intellectual content, and approval of the final version to be published. All authors agree to be accountable for all aspects of the work.
Footnotes
Author Disclosures
The authors declare no conflicts of interest relevant to this work.
Funding Statement
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.