
Abstract
Objective:
The aim of this pilot study is to evaluate the feasibility and clinical outcomes of bilateral salpingectomy performed using the vaginal natural orifice transluminal endoscopic surgery (vNOTES) technique under spinal anesthesia in women requesting permanent contraception.
Methods:
In this study, bilateral salpingectomy was performed using the vNOTES technique under spinal anesthesia in 12 multiparous patients who requested permanent contraception. Demographic characteristics, surgery duration, intraoperative vital signs, preoperative and postoperative hemoglobin and hematocrit values, pain scores using the visual analog scale (VAS), and postoperative complications were recorded. The Quality of Recovery-15 (QoR-15) recovery questionnaire was administered prior to discharge.
Results:
The mean age of the patients was 36.66 ± 5.67 years, and the mean body mass index was 27.33 ± 6.97 kg/m2. The mean surgery duration was 25.66 ± 14.55 minutes, and the mean hospital stay was 22.45 ± 3.30 hours. The mean VAS score was 3.83 ± 1.74 at 6 hours postoperatively and 2.23 ± 1.15 at 12 hours postoperatively. Shoulder pain was observed in three patients. No major intraoperative or postoperative complications were observed in any patient. The mean total score on the QoR-15 Recovery Questionnaire was 107.83 ± 15.74.
Conclusion:
Bilateral salpingectomy performed with vNOTES under spinal anesthesia appears to be a safe and feasible minimally invasive surgical method in women seeking permanent contraception, offering a short surgical duration, low postoperative pain scores, and a short hospital stay. Prospective studies with larger patient series are needed to validate these findings.
Introduction
Salpingectomy is one of the most commonly performed surgical procedures in gynecological practice worldwide. 1 Bilateral salpingectomy is considered one of the most effective surgical methods for contraception. 2 It is increasingly preferred as a permanent method of contraception, as it has been shown not to adversely affect ovarian function in women of reproductive age.1,3 Studies examining surgical sterilization preferences show that many women prefer permanent contraception methods due to contraindications, side effects, or difficulties with regular use of hormonal or intrauterine methods. 4
Minimally invasive surgical techniques have brought about a significant transformation in gynecological surgery by reducing postoperative morbidity and accelerating the recovery process. Among these techniques, vaginal natural orifice transluminal endoscopic surgery (vNOTES) stands out as a new minimally invasive approach that provides access to the peritoneal cavity through the vaginal route without making an incision in the abdominal wall.5,6 This hybrid technique, which combines natural orifice access with endoscopic visualization and surgical instrumentation, allows for the successful performance of many gynecological procedures, such as hysterectomy, adnexal surgery, myomectomy, and pelvic reconstructive procedures.7–9 Previous studies have shown that the vNOTES technique may offer various advantages over traditional laparoscopy, including less postoperative pain, shorter hospital stays, faster recovery, and better cosmetic results.10–12
With the growing interest in the vNOTES technique, there is no evidence regarding the use of this method in bilateral salpingectomy performed under spinal anesthesia for permanent contraception. Although current studies suggest that vNOTES may be a safe and effective alternative to traditional laparoscopy, the data in the literature are mostly based on small and heterogeneous patient series.12,13 Therefore, additional clinical data are needed to better demonstrate the feasibility and surgical outcomes of this technique. In this context, the aim of the current pilot study is to evaluate the feasibility and outcomes of bilateral salpingectomy performed using the vNOTES technique under spinal anesthesia in women requesting permanent contraception.
Materials and Methods
This pilot study was conducted at a secondary public hospital in Bartın, Turkey, between May 2025 and February 2026. Approval was obtained from the local hospital ethics committee (date: 29/04/2025, decision no: 2025/03), and the study was conducted in accordance with the principles of the Helsinki Declaration. All patients were provided with detailed information about the study, and their written informed consent was obtained. The inclusion criteria for the study were being married, multiparous, and having presented with a request for bilateral salpingectomy for permanent contraception. The exclusion criteria were active pelvic infection, suspected pelvic malignancy, history of rectovaginal endometriosis, and presence of pelvic abscess.
A detailed medical history was obtained from all patients, and physical examinations were performed. Patients were evaluated with abdominal examination, bimanual pelvic examination, and transvaginal ultrasonography; abdominal ultrasonography was also performed when necessary. Patients aged 18–65 years who were classified as American Society of Anesthesiologists (ASA) I–II according to the ASA classification and had no contraindications for spinal anesthesia were included in the study. Bowel preparation was not performed before surgery. Standard anesthesia monitoring was performed on all patients in the operating room. Prior to spinal anesthesia, the patients’ initial heart rate, systolic blood pressure, diastolic blood pressure, and peripheral oxygen saturation were recorded. Patients were placed in a sitting position on the operating table, and the area where the procedure would be performed was prepared according to antisepsis rules. A 25-gauge Quincke spinal needle was used to enter the subarachnoid space at the L3–L4 intervertebral space. After observing clear cerebrospinal fluid flow, 15 mg of 0.5% hyperbaric bupivacaine was injected. The sensory block level was assessed using the pinprick test. Patients received oxygen support at 2 L/min via a nasal cannula. After spinal anesthesia, heart rate, systolic and diastolic blood pressure, and peripheral oxygen saturation were measured and recorded regularly every 5 minutes for the first 20 minutes and every 10 minutes thereafter. One patient developed nausea during surgery and was given 4 mg of intravenous ondansetron.
Bilateral salpingectomy was performed in all patients under spinal anesthesia using the vNOTES technique. Intravenous antibiotics (cefazolin 1 g) were administered to all patients prior to surgery for infection prophylaxis. After adequate spinal anesthesia was achieved, patients were placed in the lithotomy position. Prior to the surgical procedure, the vaginal and perineal areas were prepared with povidone-iodine solution according to antisepsis rules, and sterile draping was performed. Following sterile preparation, a posterior colpotomy was performed to gain access to the peritoneal cavity. No commercial single-port system was used in any patient in the study. Instead, an artificial port system (glove port technique) prepared using surgical gloves was created and placed via the posterior fornix. Subsequently, pneumoperitoneum was created with carbon dioxide (CO2) insufflation, and standard laparoscopic surgical instruments were used with a laparoscopic camera through the glove port. After evaluating the pelvic cavity, both fallopian tubes were identified. Bilateral salpingectomy was performed by coagulating and cutting the mesosalpinx from the fimbrial end toward the uterine cornu using energy-based closure devices. After removing both tubes, hemostasis was checked. At the end of the procedure, the port was removed, and the posterior colpotomy incision was closed with absorbable sutures. The removed tissues were extracted transvaginally.
The patients’ age, height, weight, number of pregnancies and births, history of previous abdominal surgery, and history of cesarean section were recorded. Preoperative and postoperative biochemical and hematological parameters were evaluated. The duration of surgery and the level of postoperative pain at 6 and 12 hours were assessed using the visual analog scale (VAS). Complications that may develop due to spinal anesthesia, such as nausea, vomiting, headache, and shoulder pain, were recorded. Postoperative hospital stay durations were recorded, and the Quality of Recovery-15 (QoR-15) recovery questionnaire was administered to patients prior to discharge. The QoR-15 questionnaire is a clinically applicable tool that assesses the quality of the postoperative recovery process. 14 Responses to the questionnaire were recorded as 10 for always and 0 for never. QoR-15 test scores were classified as excellent (QoR-15 > 135 points), good (122 ≤ QoR-15 ≤ 135 points), moderate (90 ≤ QoR-15 ≤ 121 points), and poor (QoR-15 < 90 points). 15 Patient characteristics were presented as counts in the data analysis. Numerical variables were presented as mean and standard deviation and visualized with graphs.
Results
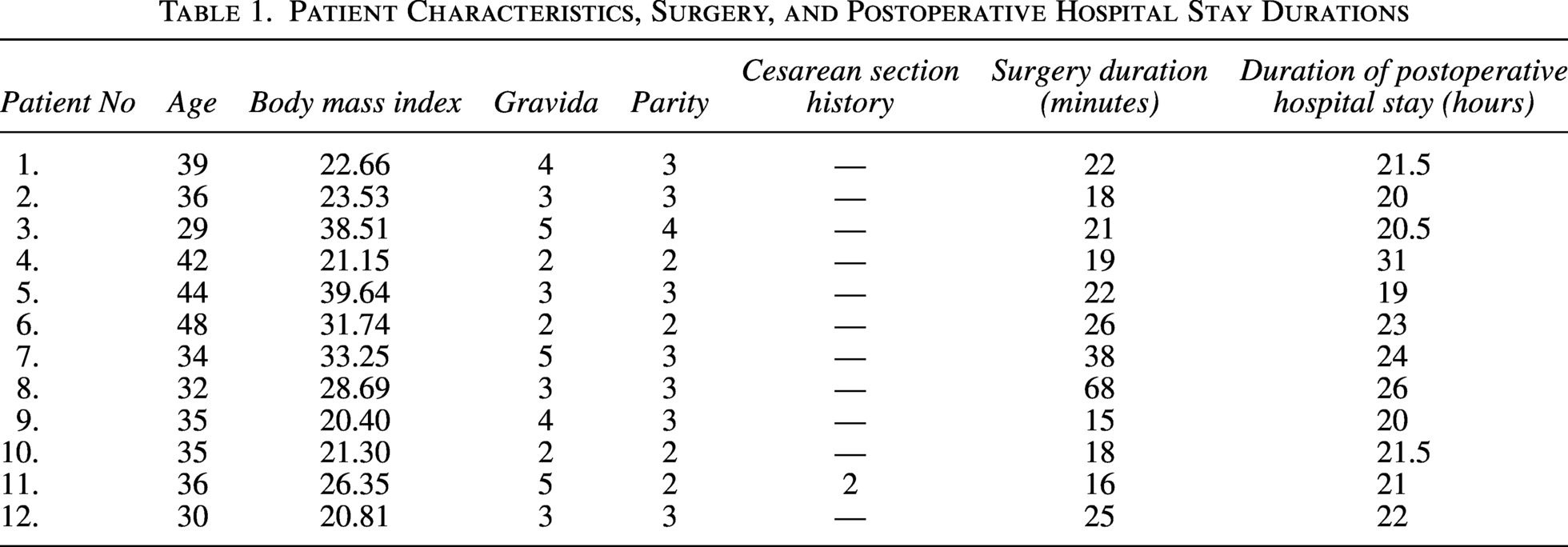
The mean age of the patients was 36.66 ± 5.67, and the mean body mass index was 27.33 ± 6.97. None of the patients had a history of abdominal surgery; only one patient had a history of cesarean section. The mean surgery duration was 25.66 ± 14.55 minutes, and the mean postoperative hospital stay was 22.45 ± 3.30 hours (Table 1). No headache, nausea, or vomiting was observed in the postoperative period. Shoulder pain was observed in three patients, and 50 μg of intravenous fentanyl was administered to these patients. Four patients received a single dose of analgesic, and eight patients received two doses of analgesic administered 4 hours apart for analgesia. Additionally, the mean total score of the QoR-15 Recovery Questionnaire was 107.83 ± 15.74.
Patient Characteristics, Surgery, and Postoperative Hospital Stay Durations
The mean preoperative hemoglobin and hematocrit values were 12.56 ± 1.06 and 37.95 ± 2.64, respectively, while the postoperative values were 10.99 ± 0.96 and 32.81 ± 0.77. The mean VAS score was 3.83 ± 1.74 at 6 hours and 2.23 ± 1.15 at 12 hours (Fig. 1). The mean blood pressure was 126.91/82.41 mmHg preoperatively and 117.58/72.75, 124.18/79.09, 122.60/72.50, and 116.00/80.50 mmHg at the 10th, 20th, 30th, and 40th intraoperative minutes, respectively. The mean oxygen saturation was 99.50 ± 0.52 preoperatively and 99.50 ± 0.90, 99.30 ± 0.67, 99.25 ± 0.50, and 97.50 ± 2.12 at the 10th, 20th, 30th, and 40th intraoperative minutes, respectively (Fig. 2).
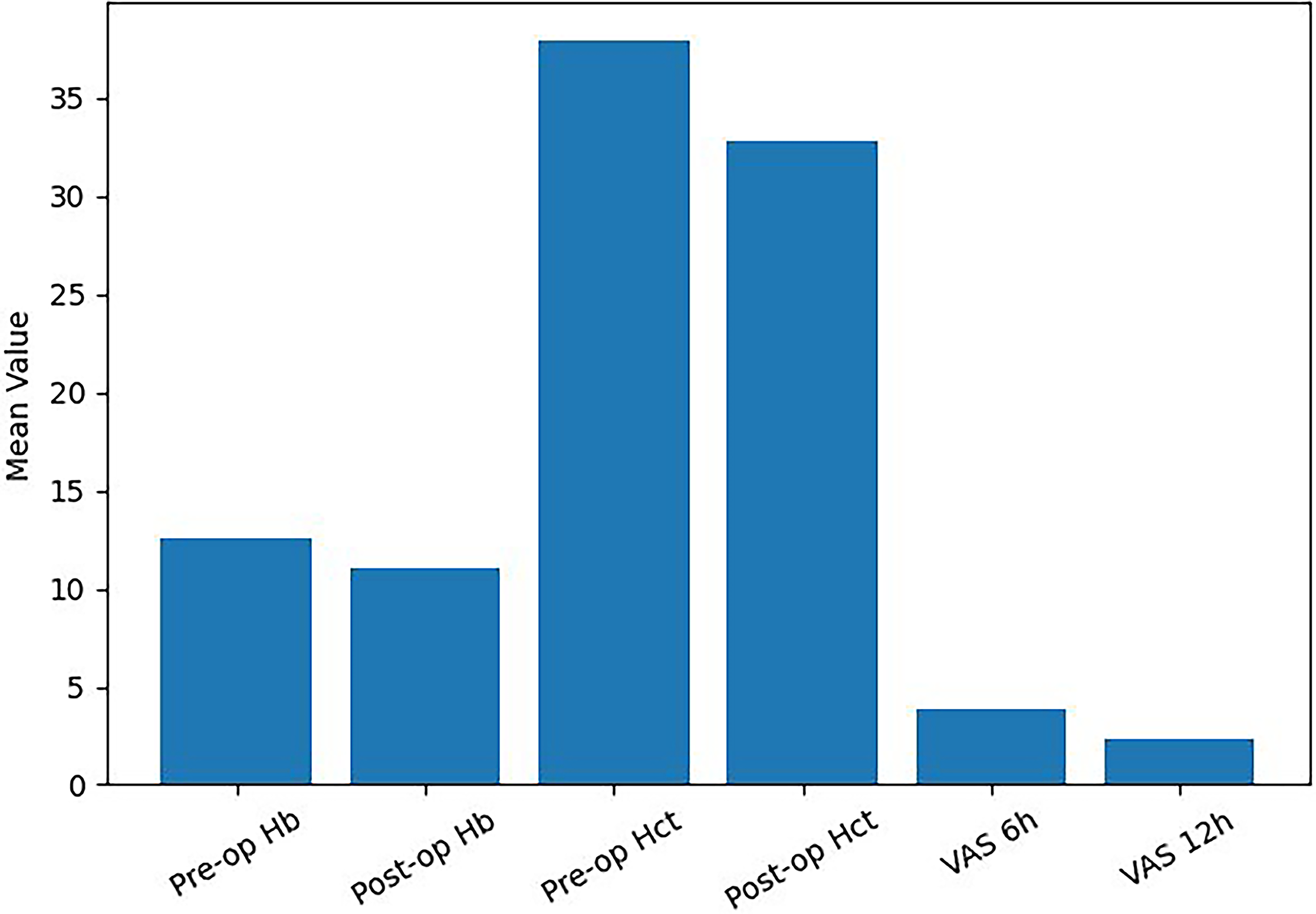
Hemoglobin, hematocrit, and VAS values.
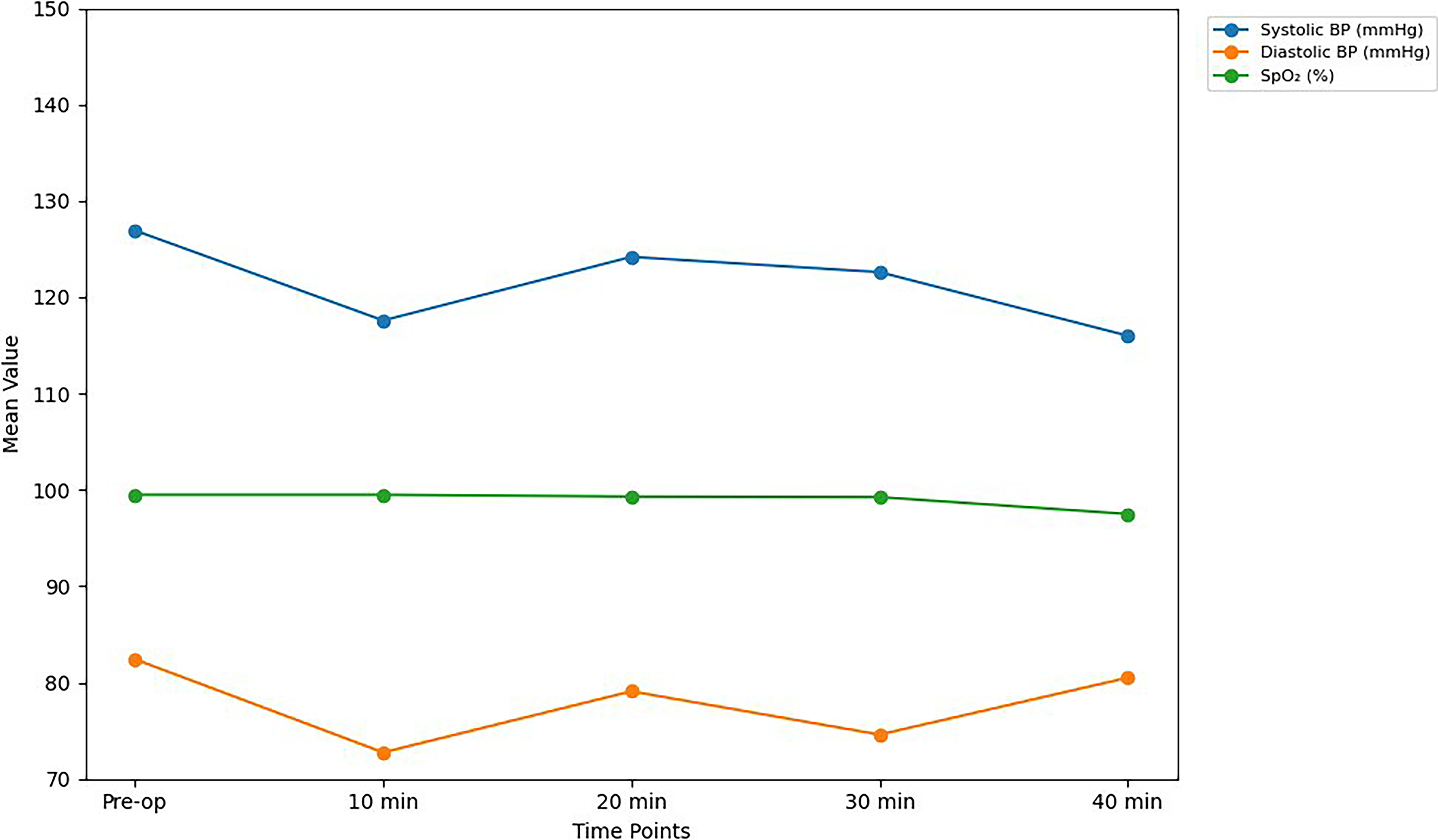
Systolic blood pressure, diastolic blood pressure, and oxygen saturation values.
Discussion
To our knowledge, this pilot study is the first to examine the feasibility and early clinical outcomes of bilateral salpingectomy performed using the vNOTES technique under spinal anesthesia in women requesting permanent contraception. The mean operative time of approximately 25 minutes in our study is consistent with results reported in the literature. In a study by Genco et al. (2025), the average surgery time for bilateral tubal ligation procedures performed under general anesthesia using vNOTES was reported to be 25 ± 8 minutes. 13 Similarly, in a retrospective cohort study by Kaya et al. (2021), it was reported that the surgical time for adnexectomy procedures performed with vNOTES under general anesthesia was shorter compared to conventional laparoscopy. 16 These results support the feasibility and effectiveness of the vNOTES technique under spinal anesthesia in terms of surgical duration.
Postoperative pain is one of the most important clinical outcomes of minimally invasive surgery. Our study shows that low VAS scores detected in the early postoperative period may indicate that the vNOTES technique offers advantages in terms of patient comfort. Studies in the literature also report that the vNOTES approach is associated with lower postoperative pain scores compared to conventional laparoscopy.13,17 A study by Halisçelik et al. (2025) also reported that VAS scores at 6 hours postoperatively were significantly lower in the vNOTES hysterectomy group compared to the total laparoscopic hysterectomy group. 18 Shoulder pain was observed in three patients in our study. Diaphragmatic irritation and phrenic nerve stimulation due to carbon dioxide insufflation are the most important causes of shoulder pain in laparoscopic surgeries. It has been reported that the incidence of shoulder pain may be lower because vNOTES surgery can be performed with lower pneumoperitoneum pressure. In a study by Genco et al. (2025), shoulder pain was observed in 15% of the vNOTES group, while this rate was reported as 87% in the conventional laparoscopy group. 13
Several studies have shown that vNOTES surgery is associated with a shorter hospital stay.11,17 In our study, the average hospital stay was found to be approximately 22 hours. A study by Tang et al. (2025) reported that the hospital stay in the vNOTES hysterectomy group was shorter compared to the laparoscopic surgery group. 7 These results suggest that vNOTES surgery may offer advantages in terms of early mobilization and rapid recovery.
In our study, no clinically significant decrease was observed in preoperative and postoperative hemoglobin and hematocrit values. Meta-analyses in the literature also report no significant difference between vNOTES and conventional laparoscopy in terms of hemoglobin decrease or blood loss. 17 This suggests that vNOTES surgery offers a safe hemostatic profile. However, it is emphasized that the majority of the existing evidence on vNOTES is based on small patient series and that larger, prospective, and multicenter studies are needed. 12 Our study also has some limitations. First, the limited number of patients reduces the generalizability of the results. The fact that the study was conducted at a single center is another factor limiting external validity.
Conclusion
In this study, bilateral salpingectomy performed using the vNOTES technique under spinal anesthesia appears to be a feasible and safe minimally invasive surgical method for women seeking permanent contraception. The procedure was associated with acceptable operative times, low postoperative pain scores, and short hospital stays. However, prospective studies with larger patient series are needed to confirm these findings.
Research Ethic
We obtained the ethical approval from the Ethics Committee of the Istanbul Esenyurt University (date: 29/04/2025, no: 2025/03).
Authors’ Contributions
İ.K., Ö.Y.Y., and M.O.K. designed the study. İ.K., Ö.Y.Y., and M.O.K. collected the data. İ.K. and H.Ö. analyzed the data. İ.K., Ö.Y.Y., M.O.K., and H.Ö. prepared the article. İ.K., Ö.Y.Y., M.O.K., and H.Ö. provide critical revisions for important intellectual content. All authors approved the final version for submission.
Footnotes
Author Disclosure Statement
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.