
Abstract
To treat patients affected with bestrophinopathies caused by mutations in the BEST1 gene, a recombinant adeno-associated virus vector (OPGx-BEST1 or rAAV2/2-VMD2-BEST1) is being developed. The vector construct includes the human BEST1 cDNA under control of the VMD2/BEST1 promoter and is packaged in an AAV2 capsid. This study evaluated the efficacy and toxicity of OPGx-BEST1 administered by subretinal injection in dogs that were homozygous mutant or compound heterozygotes for 3 naturally occurring mutations in BEST1. Twelve BEST1-mutant dogs were divided into 4 groups of 3 animals each, and they received in their left eye a subretinal injection of 0.15 mL of OPGx-BEST1 at 1 of 3 concentrations (9.5 × 109 vector genome [vg]/mL; 3.0 × 1010 vg/mL; or 3.0 × 1011 vg/mL) of OPGx-BEST1, resulting, respectively, in a low (1.4 × 109 vg), high (4.5 × 109 vg), and highest (4.5 × 1010 vg) dose or vehicle control. The right eyes were not injected. Subretinal injections were well tolerated and were not associated with any systemic or ocular toxicity. Electroretinography showed improved rod- and cone-mediated responses in eyes treated with OPGx-BEST1. Noninvasive retinal imaging by optical coherence tomography showed improved structural integrity with a reduction or prevention of appearance of vitelliform lesions and reversal of microdetachments in the retinal areas treated with OPGx-BEST1. These results support the use of OPGx-BEST1 in clinical studies with patients affected with bestrophinopathies and define the no-observed-adverse-effect level at 4.5 × 1010 vg/eye (0.15 mL, 3.0 × 1011 vg/mL).
Keywords
INTRODUCTION
In the retina, BEST1 (OMIM#607854) is selectively expressed in the retinal pigment epithelium (RPE), the highly specialized monolayer that supports the function and survival of photoreceptor (PR) cells and serves as the outer blood–retina barrier.1,2 Bestrophin 1 (BEST1) is a multifunctional, transmembrane calcium-activated chloride channel protein localized to the basolateral membrane of RPE cells.1,3–5 It has been implicated in anion transport, regulation of calcium signaling, and cell volume.6–8,9–12 Over 200 distinct human BEST1 gene mutations have been reported to be causally associated with a group of retinal disorders, termed bestrophinopathies.13–19 The most common and well-defined bestrophinopathy is a juvenile macular dystrophy called Best vitelliform macular dystrophy (BVMD or Best disease), which shows autosomal dominant inheritance (OMIM#153700). Clinically, the disease first manifests as bilateral vitelliform lesions, predominantly beginning in the macular and paramacular areas.19–25 A spectrum of molecular and structural alterations at the RPE–PR interface triggers the formation of these vitelliform lesions, which can accumulate lipofuscin, eventually progressing toward PR degeneration and vision loss.4,22,26–31 Clinical disease has been classified into 6 stages, 32 beginning with subclinical pre-vitelliform retinal microdetachments (stage I) that can progress to a vitelliform (stage II), pseudohypopyon (stage III), and vitelliruptive (stage IV) appearance followed by retinal atrophy (stage V) and choroidal neovascularization (stage VI).
Like several other inherited retinal diseases, BEST1 variants can cause biallelic (recessive) retinal disease in addition to the more common monoallelic BVMD.16,17 Canonical form of biallelic disease shows an autosomal recessive bestrophinopathy (ARB) phenotype with retinal involvement extending from fovea to midperiphery, demonstrating intraretinal cystic changes and subretinal serous detachments. However, biallelic BEST1 disease with central vitelliform lesions similar to the BVMD has also been described. 33
In dogs, 3 different naturally occurring mutations in BEST1 cause a recessive retinal disease called canine multifocal retinopathy (cmr) that shares close similarity with the human BVMD phenotype. 34 Lesions of retinal separation are frequently observed first in the area centralis (the canine equivalent to the human foveal/parafoveal area 35 ) and subsequently in the mid-peripheral/peripheral retina with disease progressing from stages I through V. 34 The subretinal space between PRs and the RPE is abnormally wide and expands with light exposure. 36 Proof-of-concept studies in this model have shown that a BEST1 gene augmentation strategy successfully corrects clinically visible subretinal vitelliform lesions as well as diffuse microdetachments. 31 In these preliminary gene therapy studies, the reversal of the obvious clinical lesions and microdetachments following the subretinal delivery of a single-stranded recombinant adeno-associated viral vector (AAV2/2) carrying human BEST1 cDNA under control of the human VMD2/BEST1 promoter was associated with the extension of RPE microvilli and restoration of the cytoarchitecture at the RPE–PR interface. 31
With the goal of developing a gene therapy product for patients affected with bestrophinopathies, this Investigational New Drug (IND)-enabling study tested the toxicity and efficacy of a good manufacturing practice (GMP)-grade batch of this AAV2/2-VMD2-BEST1 vector (OPGx-BEST1, formerly named IC-200) in BEST1 mutant dogs.
MATERIALS AND METHODS
Test article (OPGx-BEST1/AAV2/2-VMD2-BEST1)
The test article (OPGx-BEST1) was produced by co-transfection of human embryonic kidney 293 cells with 3 plasmids: the transgene plasmid VMD2-BEST1, the Rep2Cap2 plasmid, and the helper plasmid pALD-X80. It was subsequently purified by affinity and anion exchange chromatography, followed by cesium chloride ultracentrifugation, concentrated/buffer exchanged against balanced salt solution (BSS), and suspended in 0.001% Poloxamer 188, pH 7.0. The specific vector grade used in this study was a toxicity lot that was made under GMP conditions that were similar to that of the future clinical lot.
Vehicle control article
The vehicle control article consisted of BSS containing 0.001% Poloxamer 188 and pH 7.0 and was prepared by Catalent Maryland, Inc. It was used for dosing the vehicle treatment group and also to dilute OPGx-BEST1 to the concentration required for administration to the test article treatment groups.
Animals
A total of 12 dogs (homozygous mutants or compound heterozygotes for 3 different BEST1 mutations) with an age ranging from 16 to 194 weeks at the time of dosing were used. Dosing of animals as well as in vivo and ex vivo data acquisition and analysis were performed in a masked manner. Study day 0 was the day of injection for each animal. All animals were terminated at 13 weeks post injection. A mix of male and female dogs was allocated to each treatment group with the exception of the highest dose group, which consisted only of females due to limited availability of animals.
Studies were carried out in strict accordance with the recommendations in the Guide for the Care and Use of Laboratory Animals of the National Institutes of Health, in compliance with the United States Department of Agriculture (USDA)’s Animal Welfare Act, Animal Welfare Regulations, and the Association for Research in Vision and Ophthalmology (ARVO) Statement for the Use of Animals in Ophthalmic and Vision Research. The protocols were approved by the Institutional Animal Care and Use Committee of the University of Pennsylvania (IACUC# 803254). The dogs were bred and maintained at the University of Pennsylvania Retinal Disease Studies Facility. This IND-enabling study conducted by the Division of Experimental Retinal Therapies (ExpeRTs) was designed in a manner that addressed the key components of the principles of Good Laboratory Practice (GLP) regulations as set forth in 21 CFR Part 58, GLP for Nonclinical Laboratory Studies, which included the involvement of quality control and quality assurance units throughout the duration of the study but was not formally fully GLP compliant.
For a comprehensive description of the methods, including subretinal injection, medication regimen, and in-life and postmortem toxicology and efficacy assessment, including statistical analysis, see Supplementary information and previously published methodologies.31,37,38
RESULTS AND DISCUSSION
Relevance for clinical trials
Results of this study supported a clinical trial in which patients with BVMD or ARB caused by mutation in BEST1 are receiving OPGx-BEST1 administered by subretinal injection. The clinical trial is a Phase 1b/2a, open-label, dose-exploring, safety, and tolerability study. Details are available at https://clinicaltrials.gov/study/NCT07185256.
Objective and study design
The study was designed to evaluate the toxicity and efficacy of OPGx-BEST1 administered by subretinal injection in BEST1-mutant dogs. The subretinal surgical procedure in the first 9 animals was performed over 3 consecutive days. On each day, both doses (high, low) of the test article and the vehicle were administered in the left eye (LE) of 3 different animals. To ensure similar representation in gender, ages, stages of disease, and genotypes, the animals were preassigned in a non-randomized manner to the different treatment groups. Three animals received a subretinal injection of OPGx-BEST1 at the high-dose (150 µL, 3.0 × 1010 vg/mL, 4.5 × 109 vg/eye, high-dose group). Three animals received a subretinal injection of OPGx-BEST1 at the low-dose (150 µL, 9.5 × 109 vg/mL, 1.4 × 109 vg/eye, low-dose group), and 3 animals received a subretinal injection of the vehicle control article (150 µL, Alcon BSS with 0.001% Poloxamer 188, vehicle group). After completion of this initial study, 3 additional mutant BEST1 dogs were added to test a higher dose (150 µL, 3.0 × 1011 vg/mL, 4.5 × 1010 vg/eye, highest-dose group) of the test article OPGx-BEST1. The right eyes (RE) of all 12 dogs remained untreated. At the time of surgery, visualization through the operating microscope of the formation of a large subretinal bleb (Fig. 1A2–D2) immediately following the injection was the criteria for retaining dogs in the study. As all dogs were successfully injected, they were all retained in the study and followed for 13 weeks post treatment, at which point they were euthanized for histopathological analysis. An outline of the study design can be found in Table 1 and Supplementary Table S1.
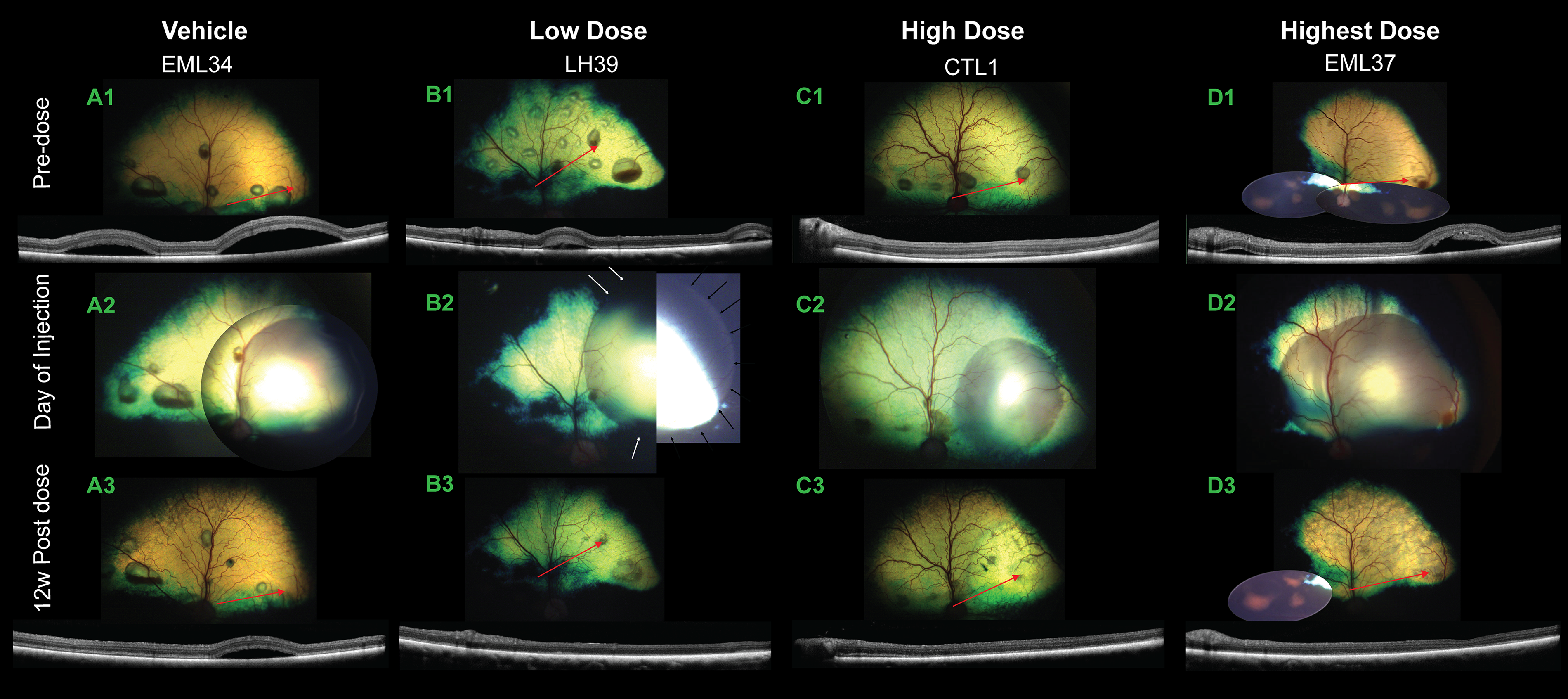
Retinal imaging from selected dogs of all treatment groups illustrating the location and appearance of the treated retinal area prior to, immediately after, and 12 weeks post dosing.
Study Design to Evaluate Subretinal Injection of OPGx-BEST1 in BEST1 Mutant Dogs
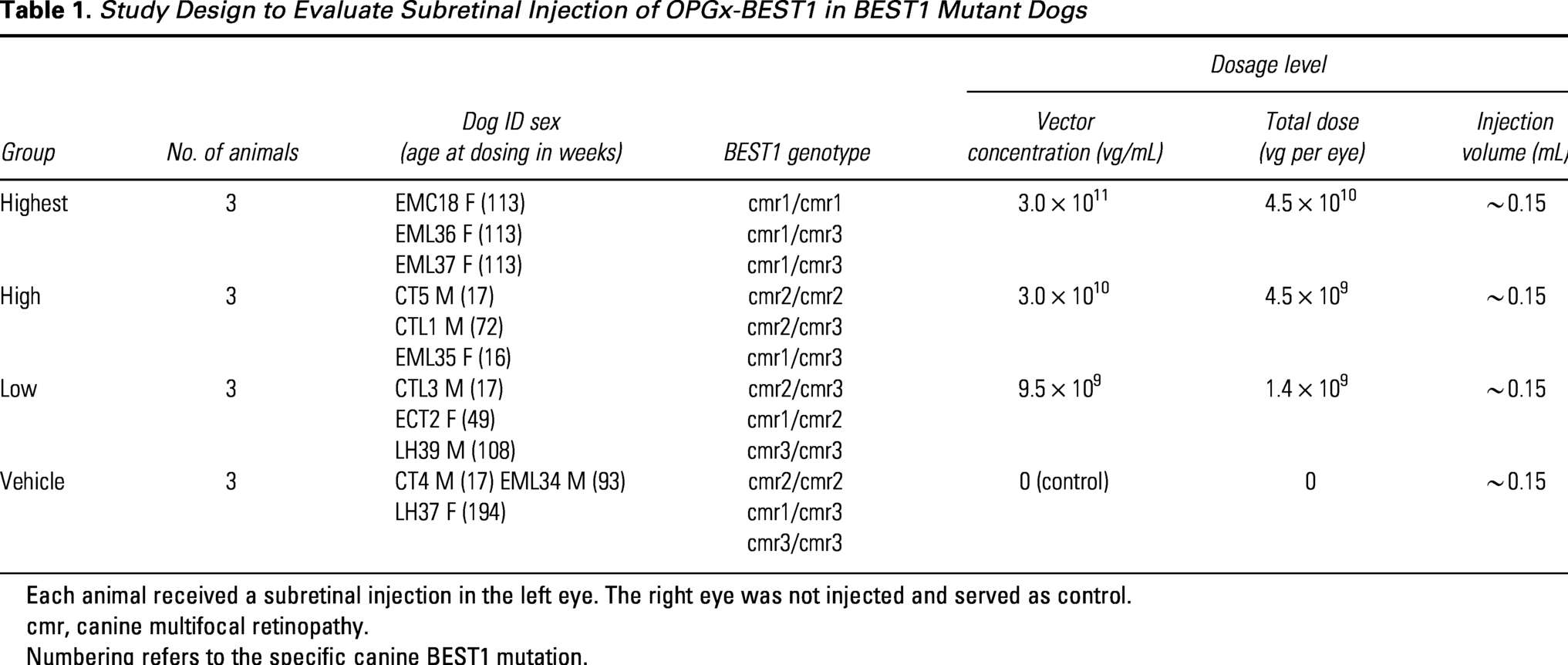
Each animal received a subretinal injection in the left eye. The right eye was not injected and served as control.
cmr, canine multifocal retinopathy.
Numbering refers to the specific canine BEST1 mutation.
Summary of data
1. Clinical observations
Daily clinical observations did not reveal any systemic toxicity associated with the test article. Comparison of body weights across treatment groups throughout the in-life portion of the study did not show any effect of the test article. All animals reached the end of the study (week 13) with good body condition.
2. Ophthalmic examinations
BEST1-associated lesions observed by indirect ophthalmoscopy and confocal scanning laser ophthalmoscopy (cSLO) were staged, 34 and their progression in the treated area of the injected eyes was compared with the progression of lesions observed in the untreated area of the injected eyes and equivalent treated area of the contralateral non-injected eyes. Note: the earliest stage that can be diagnosed by funduscopic examination or cSLO imaging is stage II (vitelliform lesion).
Ophthalmic findings in the 12 non-injected eyes (Supplementary Table S2) showed persistence or lesion appearance in 8 out of 12 eyes. Persisting lesions in the treated area were also observed in the 1 out of 3 vehicle-injected eyes (Supplementary Table S3; Fig. 1A1–A3).
Ophthalmic findings in the 3 eyes that were injected with the low dose of OPGx-BEST1 are summarized in Supplementary Table S4. In the single eye from this treatment group that had funduscopically visible lesions (stage III) at pre-dose, lesions persisted in the untreated area but were less pronounced and appeared to have reverted more to a stage II appearance in the treated area (Fig. 1B1–B3). No lesions appeared in the 2 remaining eyes. Thus, evidence for some potential efficacy of low-dose OPGx-BEST1 could be detected in 1 out of 3 dogs. In one animal, the retina in the treated area had not fully reattached by 1 week post dose. In this area, a localized site of hyperreflectivity and retinal folds was seen that persisted until 12 weeks post dose. This could have been caused by the surgical procedure and thus cannot be unambiguously related to the test article. No clinical signs of toxicity were seen in the other 2 of 3 low-dose OPGx-BEST1-injected eyes.
Ophthalmic findings in the 3 eyes that were injected with the high dose of OPGx-BEST1 are summarized in Supplementary Table S5. In one eye, a single focal stage III lesion detected at pre-dose in the treated area disappeared following treatment (Fig. 1C1–C3), yet all stage II and III lesions in the untreated area persisted. In another eye, no lesions developed in the treated area, yet numerous multifocal Stage II lesions appeared at 8 weeks post-dose in the untreated area. Finally, no lesions appeared in the third eye. Thus, evidence for some potential efficacy of high-dose OPGx-BEST1 could be detected in 2 out of 3 dogs. No clinical signs of toxicity were seen in any of the high-dose OPGx-BEST1-injected eyes, and ocular findings were related either to the surgical procedure or to natural course of disease in this model.
Ophthalmic findings in the 3 eyes injected with the highest dose of OPGx-BEST1 are summarized in Supplementary Table S6. One eye had a stage II lesion at baseline, which was treated and resolved from the 1-week post-dosage timepoint onwards. Stage III lesions that were noted in 2 dogs pre-dosing all resolved by the end of the study (Fig. 1D1–D3). Areas of mottled gray coloration with reduced tapetal reflectivity were seen in the bleb/injected region of all 3 eyes (Fig. 1D3). These observations were not considered adverse events, as these changes could not be associated with any detectable signs of structural alterations by optical coherence tomography (OCT) nor on histological sections.
In summary, ophthalmoscopic evidence of a positive therapeutic effect was observed in some dogs across all OPGx-BEST1 treatment groups. Most of the other ophthalmic findings (e.g., conjunctival hyperemia, retinotomy, retinal folds) seen in the injected eyes across all treatment groups were observed postoperatively and considered to be related to either the surgical procedure or the medication regimen (subconjunctival injection of triamcinolone acetonide). No such findings were seen in the contralateral non-injected eyes.
3. Quantification of retinal structure in vivo
Canine BEST1 disease is defined by the following 3 anatomical features detectable by in vivo imaging: large vitelliform separations of the RPE from PR, microdetachment at the level of RPE–PR interface, and loss of PR cells by thinning of the outer nuclear layer (ONL). Two different approaches using standard resolution OCT-derived maps (Fig. 2; Supplementary Figs. S1–S3) and single high-resolution (HR) OCT B-scans (Supplementary Fig. S4) allowed independent assessment of the effect of treatment on preservation of the ONL thickness and restoration of the RPE–PR interface (OS+ thickness).
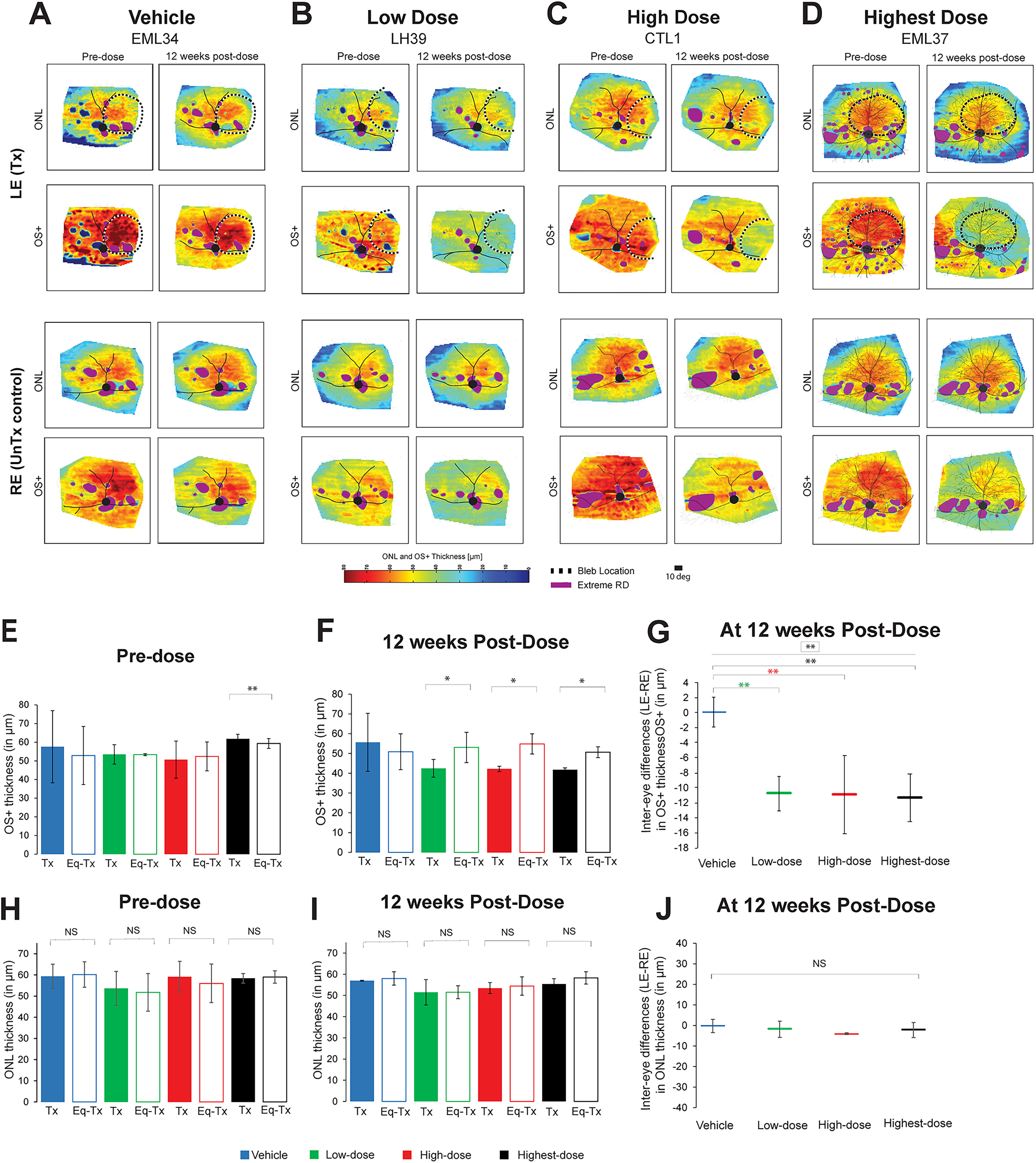
In vivo assessment of outer nuclear layer and RPE–photoreceptor interface thickness at pre-dose and 12 weeks post-treatment by optical coherence tomography imaging.
OCT map analysis of OS± thickness
Qualitative analysis of OS+ thickness on OCT maps revealed a positive treatment effect (reduction of the RPE–PR distance) that was limited to the treated area of eyes injected with the low, high, and highest doses (Supplementary Fig. S2). No such effect was seen in any of the vehicle-injected eyes. However, in the contralateral non-injected eyes (Supplementary Fig. S3), although multifocal retinal lesions persisted or appeared, pan-retinal reduction in OS+ thickness was seen when comparing the pre-dose with the 12-week post-dose timepoint in 3 out of 3 dogs from the highest dose group and in 1 out of 3 dogs in the vehicle, low, and high dose groups.
When compared with the pre-dose timepoint, OS+ thickness in the treated areas of the eyes injected with the test article was reduced (Fig. 2E, F). In addition, comparison of the OS+ thickness between treated areas of the injected eyes and equivalent areas of the non-injected eyes showed a reduction in all 3 dose groups, which was statistically significant with the low and highest doses (Fig. 2F).
Quantitative comparison across treatment groups of the mean inter-eye differences (IED) in OS+ thickness at 12 weeks post-dose (normalized to the IED at pre-dose) between the treated area of the injected left eyes (LE) and the equivalent treated area of the non-injected contralateral RE showed an overall statistical difference (p = 0.01) (Fig. 2G). Post hoc comparison showed a statistically significant reduction in the low-dose OPGx-BEST1 (−10.7 ± 2.3 µm; p = 0.005), the high-dose OPGx-BEST1 (−10.9 ± 5.2 µm; p = 0.005), and the highest-dose OPGx-BEST1 (−11.3 ± 3.2 µm; p = 0.004) groups when compared with vehicle (0.0 ± 2.0 µm).
HR OCT single B-scan analysis of OS± thickness
Qualitative evaluation of the HR OCT B scans showed a reduced distance between the inner segment/outer segment (IS/OS) and RPE/T layers in animals from both the low and high dose groups (Supplementary Fig. S4B1 and B2, C1 and C2) when comparing the treated area of the injected eyes (LE) and the equivalent treated area of the non-injected contralateral eyes (RE). This treatment effect was less apparent in the highest dose group (Supplementary Fig. S4D1 and D2) and not observable in the vehicle group (Supplementary Fig. S4A1 and A2). Quantitative comparison across treatment groups of the mean inter-eye differences in OS+ thickness at 12 weeks post-dose between the treated area of the injected eyes (LE) and the equivalent treated area of the non-injected contralateral eyes (RE) showed an overall statistically significant (p = 0.04) difference across all dosage groups. Post hoc comparison confirmed statistically significant reduction in the low-dose group (−22.6 ± 15.2 µm; p = 0.008) and the high-dose group (−17.7 ± 11.8 µm; p = 0.02) but not the highest-dose group (−11.4 ± 1.5 µm; p = 0.07) when compared with vehicle (5.6 ± 4.6 µm).
In summary, taken together, both independent methods of OCT analysis confirmed that administration of OPGx-BEST1 results in reduction of OS+ thickness across all dosage groups.
OCT map analysis of ONL thickness
No significant differences in ONL thickness were seen within each treatment group between the treated area of the injected eyes and the equivalent area of the contralateral (non-injected) eyes at pre-dose (Fig. 2H) and 12 weeks post-dose (Fig. 2I). Similarly, when interocular difference in ONL thickness was compared across treatment groups at 12-weeks post-dose, no significance was found (Fig. 2J). When examining individual ONL thickness maps (Supplementary Figs. S2 and S3), it was apparent that some individuals from all 4 treatment groups had a reduction in ONL thickness between the pre- and the 12-weeks post dose timepoints (e.g., animals CT4, CTL3, EML35, EML36). However, as this was seen in the treated and untreated areas of the injected eyes and the equivalent areas in the non-injected eyes, this was most likely not related to the test or vehicle articles.
HR OCT single B-scan analysis of ONL thickness
In all 3 dogs of the low, high, and highest groups, ONL thickness in the treated area at 12 weeks post-dose was within the 95% confidence intreval (CI) of normal dogs, except in areas of BEST1-associated focal retinal detachment where the ONL was below the 95% CI. No significant differences were seen when comparing the mean ONL thickness in the treated area of the injected eyes to that of the equivalent treated area of the contralateral non-injected eyes. In 12 out of 12 non-injected eyes, ONL thickness at 12 weeks post-dose was within or slightly above the 95% CI of normal dogs, except in areas of a focal BEST1 lesion with retinal detachment where ONL thinning was seen. A similar finding was observed in all 3 vehicle-injected eyes. Representative images from a dog of each treatment group are shown in Supplementary Fig. S4.
4. Electroretinography
At the pre-dose timepoint, the mean interocular amplitude differences were minimal, and there were no significant differences across treatment groups under conditions that elicit rod, mixed rod-cone, and cone responses (Fig. 3A, C, E, G; Supplementary Fig. S5). At 11 weeks post-dose, an increase in interocular amplitude differences between treated and contralateral non-injected eyes was seen in the low, high, and highest dose groups (Fig. 3B, D, F, H; Supplementary Fig. S5). The most prominent and statistically significant differences in interocular amplitudes following stimulations under scotopic conditions with a range of light intensities were found in the high-dose group (Fig. 3B, D). These results suggest that OPGx-BEST1 improves rod and mixed rod-cone ERG responses. Under photopic conditions that isolated cone-mediated ERG responses (Fig. 3F, H), there was also an increase in interocular amplitude differences in favor of the injected eye in all 3 OPGx-BEST1 treatment groups.
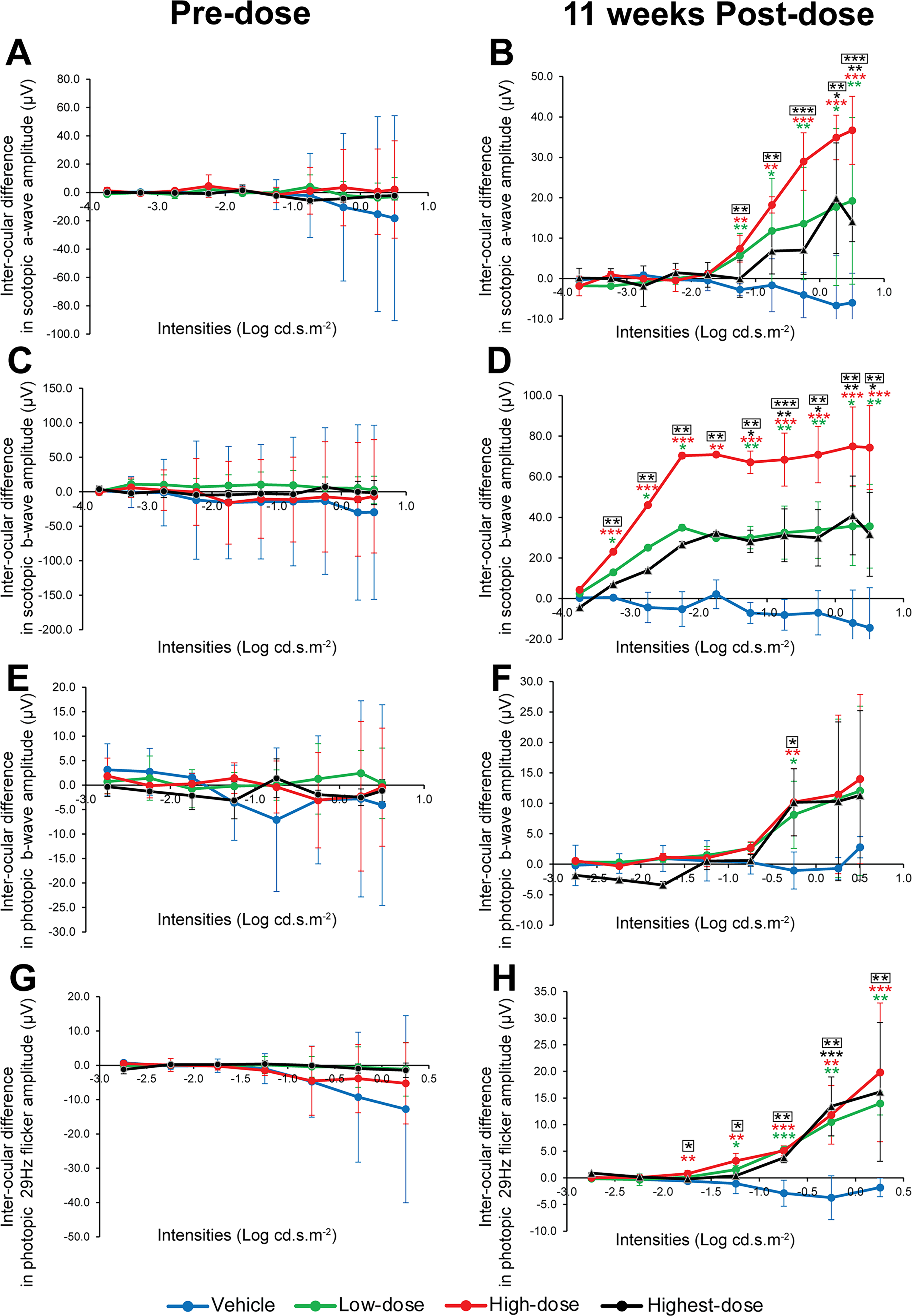
Comparison of full-field ERG amplitudes across treatment groups at pre-dose and 11 weeks post-dose. Mean (±SD) interocular differences in scotopic a-wave
In summary, no signs of retinal toxicity that could be associated with the low-, high-, or highest-dose groups of OPGx-BEST1 were detected by ERG. Results showed, on the contrary, a dose-dependent improvement in ERG responses following treatment with OPGx-BEST1, which was maximized when using the high dose.
5. Clinical pathology
There were no test article-related effects on hematology, coagulation, or clinical chemistry parameters in any of the treatment groups. Any abnormal clinical pathology findings were seen across all groups and were most likely not caused by the administration of OPGx-BEST1. Mild transient liver value elevations and leukocyte elevations were attributed to medication such as corticosteroids administered post dosage, 39 especially since cessation of corticosteroids resulted in a reversal of these abnormalities. Other transient abnormalities were attributed to the sampling process itself—physical restraint likely caused elevated creatinine kinase levels40,41 in 2 dogs at separate timepoints, while focal cases of mild increases in reticulocyte counts. No clinically relevant coagulation abnormalities were noted. All anomalous clinical pathology results were deemed unremarkable by a board-certified veterinary clinical pathologist.
6. Non-ocular histopathology
There were no test article-related effects on organ weights. None of the gross pathology and histopathological findings were obviously test-article related. Most dogs exhibited axonal degeneration in the optic nerves and optic tracts, characterized by dilated myelin sheaths, swollen and hyper-eosinophilic axons (spheroids), and/or myelinomacrophages within digestion chambers. These changes remained minimal and were often seen bilaterally throughout all experimental groups, including the vehicle-injected group. The cause for the axonal degeneration is difficult to ascertain and may have been caused by the focal retinal disruption at the site of retinotomy.
In the highest dose group, 2 dogs showed multifocal mild epicardial discoloration of the right atrium of unknown significance. No cardiac-related clinical signs were reported in these dogs, and histopathological examination of cardiac tissue revealed changes reminiscent of atrial myocarditis. 42 While transient myocarditis has been reported in humans following AAV gene therapies, most cases are reported within 1–3 weeks post-treatment and are associated with doses greater than 1 × 1013 vector genomes per kilogram body weight, which is far higher than the highest dose used in this experiment (4.5 × 1010 vg in total). 43 In addition, AAV vectors commonly associated with myocarditis 43 do not include the one used in the present study (rAAV2/2) that has a known tropism for PRs and RPE when delivered subretinally.44–46 In summary, regarding this poorly understood inflammatory condition, a test article-related effect is unlikely but not fully ruled out.
7. Ocular histopathology
No histological evidence of intraocular hemorrhage, inflammation, or necrosis was observed in any of the injected or non-injected eyes. Significantly, no signs of ocular toxicity toward the viral vector could be seen within all 3 OPGx-BEST1 dosage groups (Fig. 4A). All injected eyes in the treatment groups showed preservation of the ONL and inner and outer segments in the treated area, with a mean ONL thickness that was comparable with that of the equivalent area of the non-injected contralateral eyes (Fig. 4B,C; Supplementary Fig. S6). There was no significant difference in the mean interocular (treated vs contralateral non-injected) ONL thickness across treatment groups (Fig. 4D). The few cases of ocular abnormalities that were observed included focal retinal detachments with RPE hypertrophy and occasional accumulation of RPE cytoplasmic lipofuscin—all commonly seen lesions associated with BEST1 disease itself. Absence of test article-induced retinal toxicity observable via light microscopy was seen even in the highest dosage group.
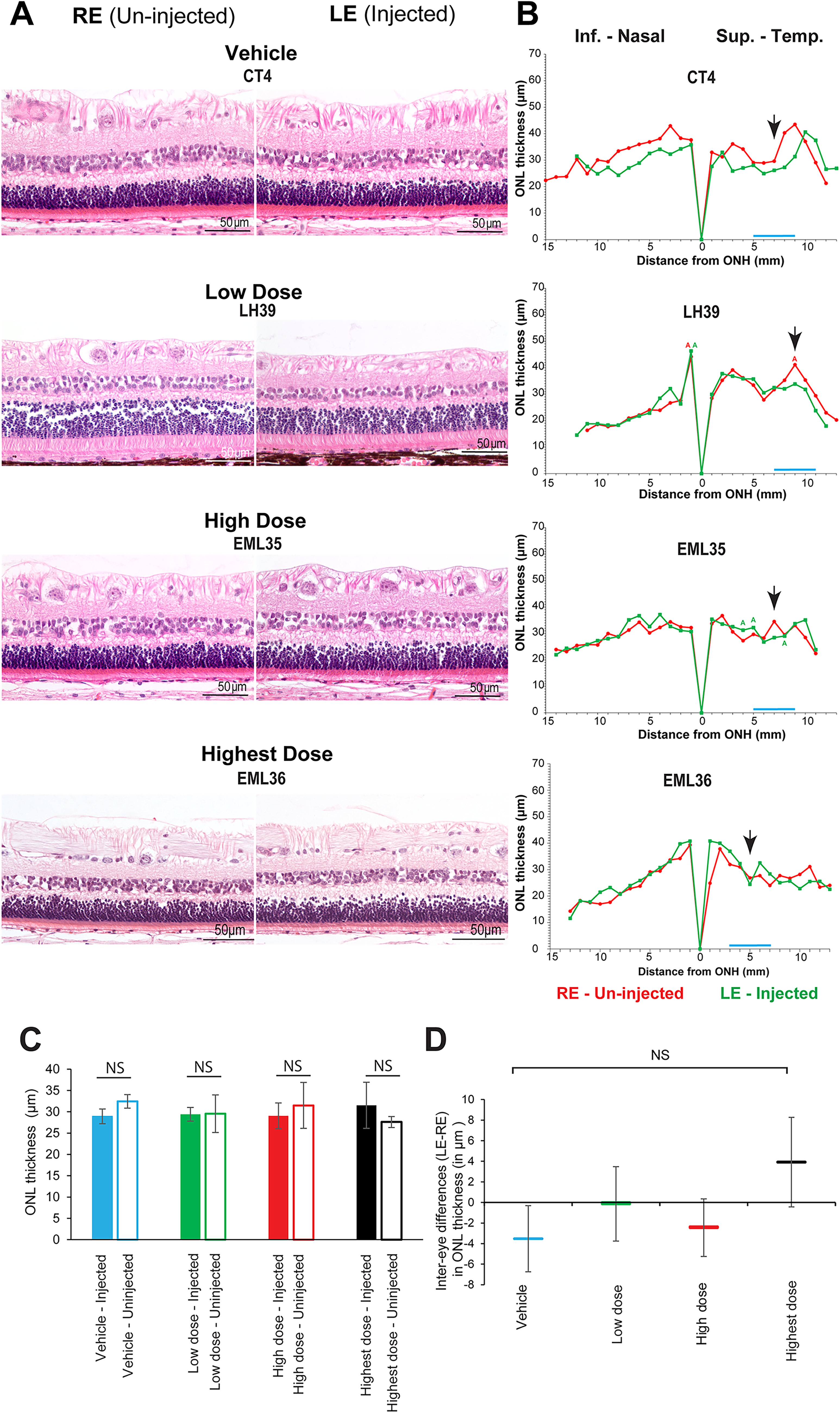
Representative retinal histology and quantification of ONL thickness at 13 weeks post dose in individual injected and non-injected eyes from all 3 treatment groups.
8. Viral vector shedding and biodistribution
A validated qPCR assay performed on fluids collected throughout the study and on tissues sampled postmortem revealed dose-dependent levels of OPGx-BEST1 within the aqueous humor of the treated eyes at 4 weeks post-dose. OPGx-BEST1 remained detectable until week 13, although the copy numbers were lower than at week 4, pointing toward a decrease in OPGx-BEST1 concentration in the aqueous humor over time (Supplementary Fig. S7). Low positive signals were detected in the bulbar conjunctiva, optic nerve, tears, spleen, and saliva of dogs injected with OPGx-BEST1. All other tissue samples contained no detectable levels of OPGx-BEST1.
9. Immunological studies
Mean total blocking antibody titers (expressed as inverse of greatest dilution) directed against AAV2 from animals of each treatment group are shown in Figure 5. While low titers were observed at pre-dose and post-dose in both vehicle-, low-dose-, and high-dose-injected animals, a prominent increase in total blocking antibody titers directed against AAV2 was seen at 8 weeks post-dose in the highest dose group, and levels persisted until termination.
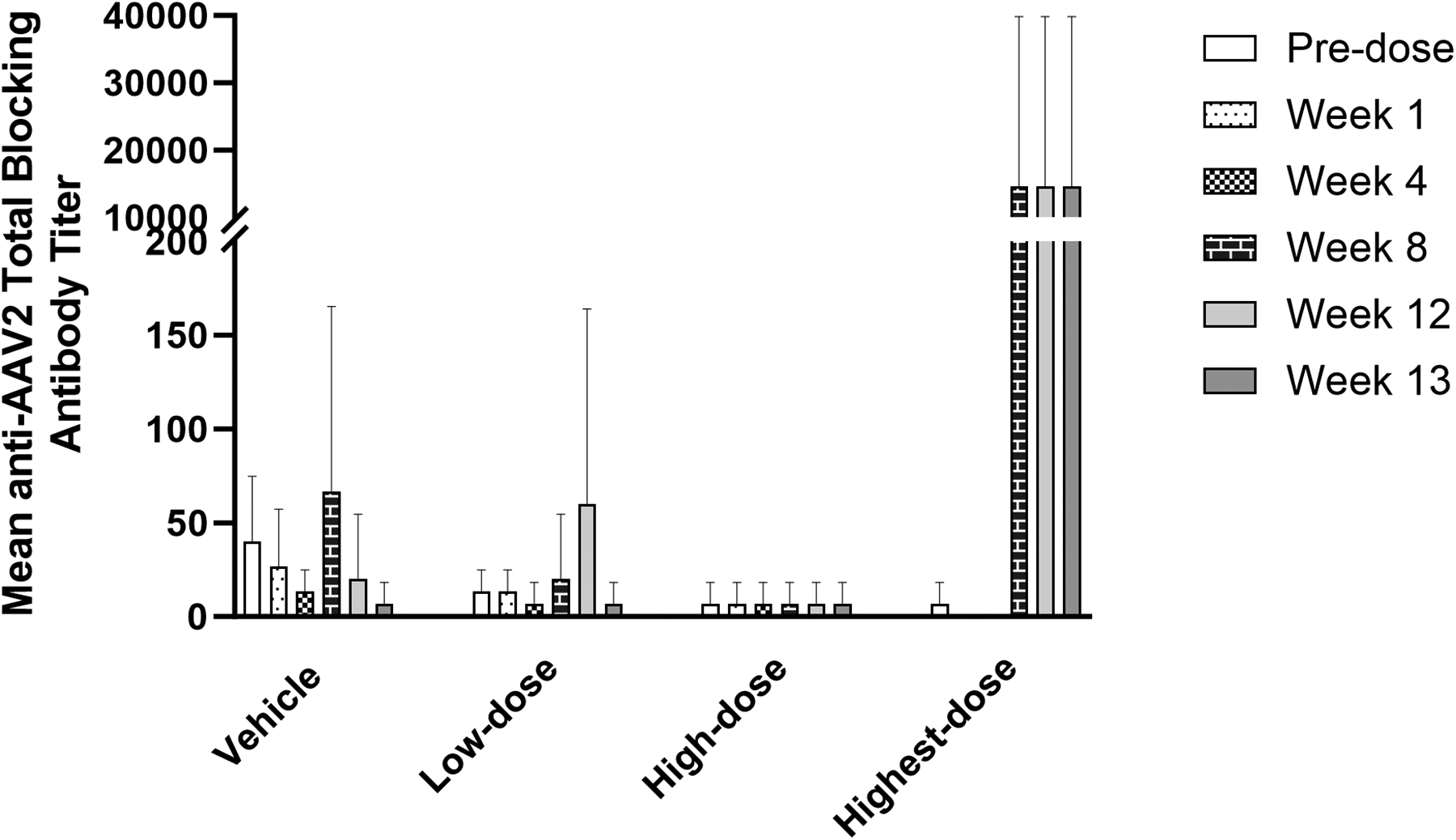
Serum titers of total blocking antibodies directed against AAV2 capsid proteins. Antibody titers (mean ± SD) measured in serum collected at baseline (pre-dose), 1, 4, 8, 12, and 13 weeks post-dose from all dogs of the 4 treatment groups.
CONCLUSIONS
This IND-enabling study in a naturally-occurring canine model evaluated the efficacy and toxicity of an AAV-based gene therapy (OPGx-BEST1) developed for the treatment of bestrophinopathies in human patients. In vivo OCT imaging and ERG analysis showed evidence of restoration of the PR to RPE interface and improved retinal function following subretinal injection of the low-, high-, and highest doses of OPGx-BEST1 when compared with vehicle. However, we observed that the interocular differences in scotopic ERG a- and b-wave amplitudes were most pronounced in the high-rather than in the highest-dose group. Although we cannot exclude the possibility that this non-monotonic (bell-shaped) dose response could be due to saturation of the cellular translational machinery at high multiplicity of infection, 47 the most plausible cause for this result is that subretinal blebs in all 3 eyes from the highest dose covered a smaller retinal surface than that achieved in the eyes of the high-dose group. No signs of toxicity associated with OPGx-BEST1 were detected by clinical assessment, histology, and clinical pathology for up to 13 weeks post injection in any of the dosage groups. While a significant elevation in the titers of AAV2 total blocking antibody occurred as early as 8 weeks post injection in the highest dose group, several publications have shown that production of systemic anti-AAV2 antibodies in dogs, nonhuman primates, and in RPE65-LCA2 patients does not impede or neutralize AAV-mediated expressions or therapeutic effect when the same vector construct is administered subretinally 15 days to years later to the contralateral eye.48–50 Based on these study results, the no-observed adverse effect limit of OPGx-BEST1 is 4.5 × 1010 vg/eye (0.15 mL, 3.0 × 1011 vg/mL) in naturally occurring BEST1-mutant dogs. This study supports the use of OPGx-BEST1 in clinical studies with patients affected by bestrophinopathies caused by BEST1 gene mutations.
AUTHORS’ CONTRIBUTIONS
A.V.C., G.D.A., and W.A.B. designed the experiments. A.G., J.C.K, Y.S., C-A.A., and W.A.B. performed the experiments. A.G., J.C.K., and W.A.B. interpreted the data and wrote the article. All the authors read and approved the final article.
Supplemental Material
sj-docx-1-hgt-10.1177_10430342261458076 — Supplemental material for Evaluation of the Toxicity and Efficacy of an Adeno-Associated Viral Vector Expressing BEST1 Delivered by Subretinal Injection in a Canine Model of Human Bestrophinopathy
Supplemental material, sj-docx-1-hgt-10.1177_10430342261458076 for Evaluation of the Toxicity and Efficacy of an Adeno-Associated Viral Vector Expressing BEST1 Delivered by Subretinal Injection in a Canine Model of Human Bestrophinopathy by Alexa Gray, Jennifer C. Kwok, Yu Sato, Charles-Antoine Assenmacher, Mayur Choudhary, Ash Jayagopal, Peiying Hua, Gui-Shuang Ying, Malgorzata Swider, Alexander Sumaroka, Artur V. Cideciyan, Aguirre D. Gustavo, and William A. Beltran
Supplemental Material
sj-docx-2-hgt-10.1177_10430342261458076 — Supplemental material for Evaluation of the Toxicity and Efficacy of an Adeno-Associated Viral Vector Expressing BEST1 Delivered by Subretinal Injection in a Canine Model of Human Bestrophinopathy
Supplemental material, sj-docx-2-hgt-10.1177_10430342261458076 for Evaluation of the Toxicity and Efficacy of an Adeno-Associated Viral Vector Expressing BEST1 Delivered by Subretinal Injection in a Canine Model of Human Bestrophinopathy by Alexa Gray, Jennifer C. Kwok, Yu Sato, Charles-Antoine Assenmacher, Mayur Choudhary, Ash Jayagopal, Peiying Hua, Gui-Shuang Ying, Malgorzata Swider, Alexander Sumaroka, Artur V. Cideciyan, Aguirre D. Gustavo, and William A. Beltran
Footnotes
ACKNOWLEDGMENTS
The authors thank Jacqui Wivel and the RDSF staff for canine husbandry and assistance in all in-life studies and Lydia Melnyk for research coordination.
AUTHOR DISCLOSURE STATEMENT
A.V.C., G.D.A., and W.A.B. are coinventors on a patent application related to this work. M.C. and A.J. are employees of Opus Genetics, Inc.
FUNDING INFORMATION
This work was supported by
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.