
Abstract
Pneumocystis pneumonia (PCP) can be life threatening for children receiving chemotherapy and immunosuppressive medication, including high-dose steroids. Although there are no current guidelines for prophylaxis in pediatric oncology patients, ongoing studies are evaluating the efficacy, side effects, ease of administration, and compliance of drugs used for PCP prophylaxis. Drugs currently being prescribed in practice include Bactrim, pentamidine, dapsone, and atovaquone. Bactrim remains superior for preventing PCP, but alternatives are being analyzed and investigated for those unable to tolerate Bactrim because of drug allergy or side effects. Educating patients and families about the importance of PCP prophylaxis and compliance should be a priority for all health care providers caring for children receiving immunosuppressive medications, including chemotherapy.
Introduction
Penumocystis jiroveci (formerly Pneumocystis carinii) pneumonia (PCP) was first described as a eukaryote with fungal and protozoa features in 1940 (Pyrgos, Shoham, Roilides, & Walsh, 2009). Though the scientific name formally changed in the 1990s, most clinicians continue to refer to PCP as Pneumocystis carinii (Lindemulder & Albano, 2007) pneumonia. Transmission is not well understood, but PCP invades the respiratory tract causing an acute onset of respiratory symptoms with or without fever. It is diagnosed by bilateral infiltrates with a ground glass appearance on chest X-ray or computed tomography scan or by staining from a sputum sample or lung biopsy (Pyrgos et al., 2009; Shankar, S.M. & Nania, J. J., 2007). The first pediatric case was reported in 1956 (Madden, Pui, Hughes, Flynn, & Leung, 2007). Although PCP is clinically diagnosed most often in immunocompromised individuals, including those with human immunodeficiency virus (HIV)/acquired immunodeficiency syndrome (AIDS), most healthy people are colonized with PCP by 2 to 3 years of age (“Cotrimoxazole Is Generally Used to Manage,” 2008). PCP has a higher mortality rate in non–HIV/AIDS patients, and the risk factors for developing PCP in non–HIV/AIDS patients include high-dose steroid therapy, chemotherapy-induced immunosuppression, solid organ or bone marrow transplant, and primary immune deficiency (Pyrgos et al., 2009). Also, a recent study cautioned that children younger than 2 years may be at an increased risk for developing PCP after chemotherapy treatment and stem cell transplant (SCT) though this was noted in a small sample of patients (Kim et al., 2008).
High-dose, prolonged steroid use is now considered the highest risk factor for developing PCP in pediatric patients, whereas patients with primary immune deficiency have the lowest risk (Bollée et al., 2007; Pyrgos et al., 2009). One case study published by Aviles, Boyce, and Thompson (2004) described a 3-year-old with airway hemangiomas who was treated with high-dose steroids for 6 weeks prior to developing PCP. The article further described 105 non–HIV/AIDS patients who developed PCP; 90% of those patients were receiving high-dose steroids. High-dose steroids were defined as a range of 2 mg/kg/d for 14 days to 30 mg/d for 12 weeks (Aviles et al., 2004). A systematic review by Green, Paul, Vidal, and Leibovici (2007b) also found a steroid dose of 30 mg of prednisone per day for 12 weeks as the number one risk factor for developing PCP. Pyrgos et al. (2009) further defined a prednisone dose of greater than 0.4 mg/kg/d over several months and greater than 20 mg/d for longer than 3 weeks as an increased risk for developing PCP with some clinical disease documented during steroid tapers.
In pediatric oncology patients, diagnosis, chemotherapy treatment, drug regimen, and need for SCT can increase the risk of PCP by 15% to 20% (“Cotrimoxazole Is Generally Used to Manage,” 2008), leading to mortality rates of 50% to 76% (Milstone, Balakrishnan, Foster, & Chen, 2006; Pyrgos et al., 2009). Children with high-risk leukemia have a 15% to 21% increased risk compared with 5% to 15% increased risk for those children 1 year post-SCT (Ohata et al., 2009). Pyrgos et al. (2009) listed patients with lymphoid malignancies as having the highest risk for PCP in addition to patients receiving the following drugs: fludarabine plus steroids, temozolimide, alemtuzumab, and antitumor necrosis factor. Another study by Prasad, Nania, & Shankar (2008) cited the intensity of the chemotherapy regimen, the underlying diagnosis, and the addition of steroids as increasing the risk for developing PCP. Leukemia and lymphoma patients may be at an increased risk because of the tumor burden present in the marrow or lymph system directly decreasing the functionality of granulocytes and lymphocytes produced. Of note, a study by Bollée et al. (2007) reported that PCP occurred in some leukemia patients prior to starting treatment; and of the 56 patients studied who developed PCP, none were neutropenic at clinical presentation. This study further supports the idea that a dysfunctional marrow may put patients at an increased rish for developing PCP.
Without PCP prophylaxis, the risk of developing PCP ranges from 22% to 45% (Pyrgos et al., 2009). Prophylaxis was first described in HIV/AIDS patients and was extrapolated to cancer in the 1970s when Bactrim was found to reduce the incidence of PCP by greater than 90% (Green, Paul, Vidal, & Leibovici, 2007a). Children at risk for developing PCP include those being treated for various malignant or nonmalignant tumors with treatment regimens containing steroids, chemotherapy, and SCT. Prophylaxis should be initiated for these identified high-risk populations by the advanced practice nurses caring for them. The most common drugs used and researched for prophylaxis in pediatric oncology patients are reviewed below.
Cancer and Prophylaxis: Review of the Literature
There are no current, evidence-based guidelines for PCP prophylaxis in non-HIV pediatric patients (Green et al., 2007b). Bactrim (trimethoprim/sulethoxazole or clotrimoxazole) remains the gold standard for both prophylaxis and treatment of PCP (Shankar, S.M. & Nania, J. J., 2007). The first study examining the clinical efficacy of Bactrim was published in 1977 by Hughes and colleagues (Lindemulder & Albano, 2007). With compliance, the prevention rate for PCP with Bactrim is 93% to 100% (“Cotrimoxazole Is Generally Used to Manage,” 2008; Lindemulder & Albano, 2007; Ohata et al., 2009; Prasad et al., 2008; Pyrgos et al., 2009). Several studies have looked at the timing of medication administration for prophylaxis. When compared with daily dosing, twice-daily dosing on 2 consecutive days a week, 2 nonconsecutive days a week, and 3 nonconsecutive days showed no difference in prevention rate (Green et al., 2007a; Lindemulder & Albano, 2007; Ohata et al., 2009; Pyrgos et al., 2009). Intermittent dosing was studied not only for efficacy but for side effect and compliance prevalence as well. Ohata et al. (2009) reported that 13.7% of patients were noncomplaint even with 2 day nonconsecutive, twice-daily dosing however, neutropenia was reduced with intermittent dosing. In addition to preventing PCP, Pyrgos et al. (2009) noted that Bactrim could also cover additional bacterial infections and toxoplasmosis. Side effects that required switching from Bactrim to alternate forms of prophylaxis include drug allergy, gastrointestinal upset, rash, myelosuppression, compliance, and oral formulation (“Cotrimoxazole Is Generally Used to Manage,” 2008; Lindemulder & Albano, 2007; Ohata et al., 2009; Prasad et al., 2008; Pyrgos et al., 2009; Shankar, S.M. & Nania, J. J., 2007).
Pentamidine is often used as the alternative to Bactrim for PCP prophylaxis and is given monthly via inhalation or intravenous (IV) routes. Studies (Pyrgos et al., 2009) report pentamidine as having a successful treatment rate of 40% when compared with Bactrim (93%) and atovaquone (80%). One retrospective review (Kim et al., 2008) looked at 232 immunocompromised patients who received IV pentamidine for prophylaxis over 5 years, and 3 of the children (1.3%) developed PCP. Two of the patients were younger than 2 years and had received a bone marrow transplant. This is the only study that examined IV pentamidine use in pediatrics for PCP prophylaxis. Side effects associated with IV pentamidine administration include hypotension when administered rapidly, long QT syndrome, arrhythmias, renal dysfunction, nausea and vomiting and perioral numbness that resolves when the infusion is complete (Milligan & Phillips, 2007; Pyrgos et al., 2009). In addition, there was a case report of a 21-month-old receiving IV pentamidine for prophylaxis who developed PCP after 2 unrelated SCTs (Milstone et al., 2006). The implications of age on developing or preventing PCP with pentamidine are not well-defined, and further controlled studies are need to evaluate IV pentamidine for PCP prophylaxis in pediatric oncology patients (Prasad et al., 2008). Inhaled pentamidine is also used for prophylaxis, though there are limited studies in pediatrics evaluating the efficacy and long-term side effects of this route of administration (Kim et al., 2008). Inhaled pentamidine should not be used in children younger than 5 years (Pyrgos et al., 2009) or those who are unable to breathe in the inhaled medication properly because of concern for adequate distribution. Side effects for the inhalation route include coughing, wheezing, nausea and vomiting, and bronchospasm (“Cotrimoxazole Is Generally Used to Manage,” 2008). Bronchospasm may be prevented or minimized with the use of age-appropriate albuterol prior to administration of pentamidine.
For children unable to tolerate Bactrim or pentamidine, dapsone may be used as the next line of treatment. Dapsone can be given orally daily or 3 times a week, and both schedules are equally effective (Williams, MacDonald, Hoyer, Barr, & Athale, 2005). Prevention of PCP with dapsone is similar to prevention of PCP with Bactrim (Sangiolo et al., 2005). One retrospective study reported that out of 223 children, 1 of the 36 patients (2.7%) taking dapsone developed PCP (Prasad et al., 2008). Most research on dapsone has been related to potential adverse events including methemoglobinemia, rash, hemolytic anemia, liver dysfunction, and agranulocytosis (“Cotrimoxazole Is Generally Used to Manage,” 2008). Williams et al. (2005) did a 10-month retrospective study evaluating the incidence of methemoglobinemia in 15 children with acute lymphoblastic leukemia. He found that there was a correlation with cytocrome b5 reductase (Cb5R) enzyme levels in the patients who received Dapsone prophylaxis daily on Monday, Wednesday and Friday weekly. Three of the patients developed symptomatic methemoglobinemia and all patients had oxygen saturations greater than 95%. The study concluded that heterozygosity for the cytocrome b5 reductase gene may affect the incidence of methemoglobinemia and that hemolytic anemia associated with dapsone use worsens with increased age. When dapsone was stopped, the symptoms resolved (Williams et al., 2005). A case report of a patient who died from sulfone syndrome after receiving dapsone prophylaxis post-SCT reported the patient had fever, methemoglobinemia, hemolytic anemia, exfoliative dermatitis, and transaminitis that lead to multisystem organ failure (Abidi, Kozlowski, Ibrahim, & Peres, 2006). These side effects can occur at various doses, most often occur within 2 months of starting the drug, and can even appear as late as 2 weeks after discontinuing the drug (Abidi et al., 2006). With an increased risk of sulfone syndrome and potential oxidative drug interactions (Williams et al., 2005), dapsone should not be used in patients with glucose-6-phosphate dehydrogenase deficiency (“Cotrimoxazole Is Generally Used to Manage,” 2008).
Atovaquone is currently being studied for efficacy in preventing PCP in the pediatric population and may be an effective second-line therapy, but it has only been studied in small samples (Kim et al., 2008). Atovaquone is an oral medication taken daily. Madden et al. (2007) retrospectively examined 86 patients with leukemia receiving atovaquone because of intolerance to Bactrim and none of the patients developed PCP. The study additionally looked at the interaction of atovaquone with etoposide. There was a slight increase in the concentration of the metabolite from etoposide with concurrent atovaquone administration when compared with Bactrim. Diarrhea and rash were reported as the most common side effects (Madden at al., 2007). Green et al. (2007b) also reported no significant difference for prevention of PCP compared with Bactrim, but atovaquone could provide some gram negative bacterial coverage that Bactrim would likely not because of increased antibiotic resistance to Bactrim. Another study reported that atovaquone was better tolerated but less effective than Bactrim (“Cotrimoxazole Is Generally Used to Manage,” 2008), indicating studies with larger sample sizes are needed to further examine the efficacy, side effects, and potential drug interactions related to atovaquone.
Implications for Practice
A summary of current recommendations for PCP prophylaxis, route of administration, administration frequency, side effects, monitoring parameters, and additional considerations is provided in Table 1. Educating families about the need for PCP prophylaxis can be overlooked at time of diagnosis when patients and families are overwhelmed with consents and information for chemotherapy, surgery, or radiation. However, PCP education should be a priority because of the fatality risk associated with PCP in children undergoing cancer treatment.
Common Prophylaxis Regimens and Guidelines
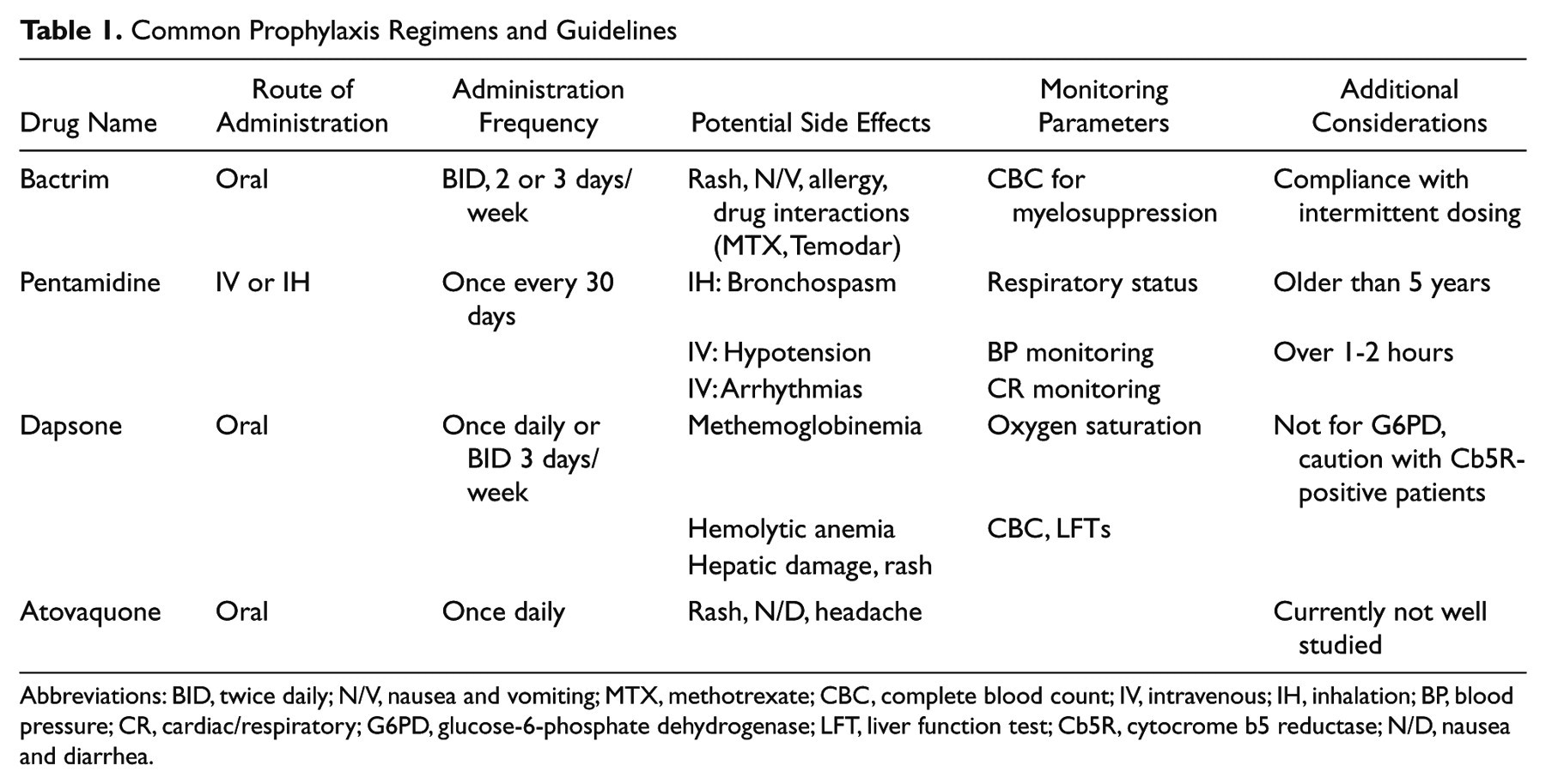
Abbreviations: BID, twice daily; N/V, nausea and vomiting; MTX, methotrexate; CBC, complete blood count; IV, intravenous; IH, inhalation; BP, blood pressure; CR, cardiac/respiratory; G6PD, glucose-6-phosphate dehydrogenase; LFT, liver function test; Cb5R, cytocrome b5 reductase; N/D, nausea and diarrhea.
Although Bactrim remains the gold standard, providers may choose to alter the prophylactic regimen based on drug allergies, age at diagnosis, intensity of chemotherapy, and steroid use. Some patients are allergic to sulfa medications and therefore cannot be placed on a Bactrim regimen. Children younger than 2 years may be at an increased risk for developing PCP and should be placed on Bactrim unless clinically contraindicated. PCP should be included in the differential diagnosis for immunocompromised children younger than 2 years presenting with symptoms of pneumonia or respiratory failure.
Initiation of prophylaxis is provider dependent, but care should be taken to not start more than one drug at a time to accurately evaluate side effects. If a patient is not beginning chemotherapy but is on postoperative steroids for a prolonged period of time, PCP prophylaxis may need to be initiated (see Table 2). The intensity of the chemotherapy regimen based on diagnosis and the expected length of neutropenia can also influence when PCP prophylaxis is initiated. Prophylaxis should be initiated for anyone who is expected to be neutropenic or functionally neutropenic (prolonged steroid use, relapsed leukemia, or other marrow disease) to minimize the risk of developing PCP. In addition to starting prophylaxis, there is also discussion of when to discontinue prophylaxis. Most studies recommend continuing prophylaxis for 3 to 6 months posttherapy or until immune function is fully recovered (“Cotrimoxazole Is Generally Used to Manage,” 2008; Shankar, S.M. & Nania, J. J., 2007; Suryaprasad & Stone, 2008).
Consider Prophylaxsis for Patients Who:

Patient compliance is an important consideration when prescribing prophylactic medications. A 2 days or 3 days a week regimen may be better tolerated, but it could be more difficult to remember to take a drug consistently if it is only taken 2 or 3 days a week. Conversely, it might be easier to remember to take a pill every day, but the patient may experience more side effects from this dosing regimen. Providers may feel more confident knowing a patient receives pentamidine once a month, even though it may be less effective, instead of risking poor compliance to oral regimens.
When patients are receiving multimodal drug therapy, potential drug interactions need to be identified. For example, Bactrim should be held with high-dose methotrexate until methotrexate is cleared because of potential drug interactions (Libecco & Powell, 2004). In addition, Bactrim should be used cautiously in patients receiving temodar because of an increased risk of myelosuppression when the drugs are used concurrently (Bachuss, 2008).
Another provider concern requiring patient and family education is antibiotic resistance. Some studies have shown that prophylaxis with Bactrim increases the resistance of certain strains of bacteria. Other studies conclude that Bactrim not only works for PCP prophylaxis but may suppress other bacterial infections as well. With high mortality rates associated with PCP infection, the risk of resistance is minimal compared with the benefit of preventing clinical infection (Green et al., 2007a).
In addition to taking the medications as prescribed, patients must be monitored closely for side effects. The number one reason for switching from Bactrim to an alternate form of PCP prophylaxis is thrombocytopenia and neutropenia (“Cotrimoxazole Is Generally Used to Manage,” 2008). This should be monitored with complete blood counts, though there is no time line for monitoring the complete blood counts. Pentamidine administration may require premedication with albuterol for the inhaled formulation and Zofran for intravenous doses to minimize side effects. Intravenous pentamidine should be administered with blood pressure and cardiac/respiratory monitoring for potential side effects (Kim et al., 2008). With methemoglobinemia being the most concerning adverse event associated with dapsone use, patients should have weekly oxygen saturation monitoring and an arterial blood gas for symptomatic or suspected methemoglobinemia (Williams et al., 2005). Since atovaquone is currently being studied, the nursing and monitoring parameters may change as more information becomes available on the drug. All side effects should be reported according to institution policy for data collection and adverse drug event reporting.
Nurses and health care providers play an important role in PCP prevention through patient and family education. Without proper education, patients and families may not understand the implications of acquiring PCP. After initial education, families require follow-up to ensure that the medication is being administered properly and potential side effects are being monitored for. If patients and families are not asked about side effects related to the medication, they may not be distressing enough to bring up during routine visits. Support from health care providers is important to increase compliance of medication administration. Additionally, health care providers are responsible for recognizing signs and symptoms of PCP. Families put a significant amount of trust in health care providers to prescribe medication that will not cause harm, but medication alone cannot prevent PCP in children. A mutual effort between health care providers and patients and families is imperative for PCP prevention.
Conclusion
As more children are being treated with immunosuppressive medications, including chemotherapy and high-dose steroids, increasing their risk for developing PCP pneumonia, it is imperative for health care providers to include PCP prophylaxis in treatment regimens. In addition to prescribing, providers and nurses play a vital role in increasing patient compliance to prophylactic regimens through patient and family education. Ongoing and future studies are needed to compile evidence-based guidelines for PCP prophylaxis for children receiving chemotherapy, transplants, and high-dose steroids that will outline who needs prophylaxis, how often, and for how long and what drugs are most effective with the least amount of toxicities.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) received no financial support for the research, authorship, and/or publication of this article.