
Abstract
Much research has been directed at childhood cancer survivors and their families to learn how to best provide care. However, little is known about parents’ experiences of transitioning to a time when their child has completed treatment for cancer when living at a distance to the tertiary cancer center. The purpose of this study was to talk to such parents about their experiences. Five Canadian parents of children who had completed treatment for cancer in the past 3 months to 5 years took part in qualitative opened-ended interviews using a phenomenological hermeneutic approach. Data analysis revealed the essence of the parents’ lived experience as a journey within a journey; 4 themes characterized the essence. Parents living a 2.5- to 5-hour drive from the cancer center expressed a willingness to travel wherever necessary in order to receive specialized care for their child. Parents emphasized the importance of having a local health care provider in whom they trusted. Assessing families’ needs, support systems, and readiness to return home are important nursing roles throughout the cancer trajectory.
Introduction
Childhood cancer is diagnosed in approximately 1,300 Canadian children younger than 20 years every year (Canadian Cancer Society [CCS], 2009). It is now considered a chronic rather than fatal disease. Rates of survival have increased from less than 50% prior to 1970 to greater than 80% (National Cancer Institute, 2008). Currently in Canada, 5-year survival rates are 82% (Ellison, Pogany, & Mery, 2007), which is comparable to those in the United States (National Cancer Institute, 2008) and Europe (Ellison et al., 2007).
Improved survival rates for childhood cancer can be attributed to the advances associated with treatment. The centralization of treatment into tertiary centers that specialize in pediatric oncology provides the child and the family with care from the experts in the field (Aitken & Hathaway, 1993; Bensink et al., 2007; Klein-Geltink, Pogany, Barr, Greenberg, & Mery, 2005; Scott-Findlay & Chalmers, 2001). These centers may be near or far from the child’s home. Families may have to travel several hours in order to obtain treatment for their child’s cancer and follow-up care. Traveling for cancer care may lead to differing experiences for family member during and after cancer treatment.
Canada has a large rural population and a vast expanse of land that spans great distances. As a result, about a third of pediatric cancer patients travel more than 100 kilometers for treatment (Limburg, Shaw, & McBride, 2008). The distance from the family’s home to the tertiary center may affect several aspects of care, including how the child is transported to and from the treatment center. Some families travel enormous distances for treatment such as children from the northern territory, Nunavut, who must travel more than 2,000 kilometers to receive care at a tertiary cancer center. Personal vehicles are often used with one of the parents driving the child. Planes may be required for certain areas that are not easily accessed by land. Regardless of how the child travels to and from the treatment center, issues surrounding weather, safety, and side effects may complicate the process. For example, in many parts of Canada, roads may be covered with snow or ice for many months of the year, increasing the danger of car crashes. Winds, rain, and snow can also cause delays in flights. Children with cancer are often dealing with symptoms of the disease itself or treatment side effects, such as nausea or pain, which may be exacerbated by travel.
When a child is diagnosed with cancer, the entire family is affected (Ljungman et al., 2003; Pai et al., 2007; Patterson, Holm, & Gurney, 2003; Wilkins & Woodgate, 2005; Woodgate, 2001, 2006a, 2006b). On initial diagnosis and throughout the cancer trajectory, the family may experience a variety of emotions such as devastation, helplessness, loss of control, fear, grief, and uncertainty about the disease and what it means for the child and the family (Patterson et al., 2003). The family’s life as they knew it is changed dramatically (Ljungman et al., 2003; Patterson et al., 2003; Woodgate, 2001, 2006b; Woodgate & Degner, 2003).
The dynamic nature of the childhood cancer experience is not exclusive to the periods of diagnosis and treatment but instead extends into the period when children have completed their treatment and are in remission. In short, for the children and their families, the cancer experience never ends (Woodgate, 2006b). The transition period as children complete treatment for cancer has been described as a time of celebration and hope coupled with fear (Haase & Rostad, 1994), of change (Labay, Mayans, & Harris, 2004), of crisis that creates anxiety (Arnold, 1999), and of uncertainty (Arnold, 1999; Haase & Rostad, 1994; Labay et al., 2004). New challenges surface for children and their families.
Children who complete treatment for childhood cancer are at risk for late or long-term effects from either the cancer itself or its treatment (CCS, 2008; Mehta, 2008). Long-term follow-up is necessary for these children to monitor late and long-term effects (CCS, 2008; Meadows, 2006). Most families must learn to live with the uncertainty of possible relapse of the child’s cancer or of late or long-term effects of the treatment the child has received (Duffey-Lind et al., 2006; Labay et al., 2004).
Although much has been learned about the transitions families must undergo at diagnosis and during the treatment period, relatively little has been done to explore the experience of families following the completion of treatment for cancer (Maurice-Stam, Oort, Last, & Grootenhuis, 2008; Van Dongen-Melman, Van Zuuren, & Verhulst, 1998). This is especially the case for children who have completed treatment for cancer and their families who live at a distance from the cancer treatment center.
Purpose
Little is known about parents’ experiences of transitioning to a time when their child has completed treatment for cancer when living at a distance to the tertiary cancer center. The purpose of this qualitative, phenomenological research study was to provide a description of the essence of the lived experiences of parents caring for a child who had completed treatment for cancer who do not live near the cancer center.
Methods
This study used the methodology of hermeneutic phenomenology, which is the study of persons, to learn about the uniqueness of individual people experiencing the same phenomenon. The aim of hermeneutic phenomenology is to transform the lived experience into textual expressions of its essence (van Manen, 1990).
Setting
The study took place in Manitoba, a province in central Canada with an area of 649,947 square kilometers (250,946 square miles; Government of Manitoba, 2,011), in which there is one tertiary center in the capital city of Winnipeg. Nearly 60% of population lives in Winnipeg leaving just over 40% to live in small towns and rural areas (Government of Manitoba). The tertiary center in Winnipeg also services children with cancer from that province, areas of the 2 neighboring provinces, and the territory to the north of the province.
Participants
Permission to carry out this study was granted by a university-based ethical review committee and access approval from the recruitment site was secured. Informed consent was obtained from all participants. Using a phenomenological approach requires the participants to have experienced the phenomenon of interest and to be able to describe the meaning they attribute to that phenomenon in their lives (Creswell, 2007). Data are collected from individuals who have experienced the phenomenon by the inquirer who compiles it into a “description of the essence of the experience for all individuals” (Creswell, 2007). To capture the essence of lived experiences, the only legitimate informants are those who have lived the reality (van Manen, 1990). As Moustakas (1994) explains, this is a description of “what” the individuals experience as well as “how” they experienced it. Accordingly, in recruiting participants, attention was directed at selecting individuals who had experienced having a child complete cancer treatment while living at a distance from the tertiary cancer center. Individuals met the criteria for this study if they (a) were aged 18 years or older; (b) were able to speak, read, and write English; (c) were the primary caregiver (a parent/legal guardian/caregiver) of a child (aged 0 to 18 years at diagnosis) who had completed treatment for childhood cancer at least 3 months ago but not more than 5 years ago; and (d) lived outside the metropolitan center containing the tertiary cancer center at which the child was treated, with a travel time of at least an hour from their residence to the cancer center.
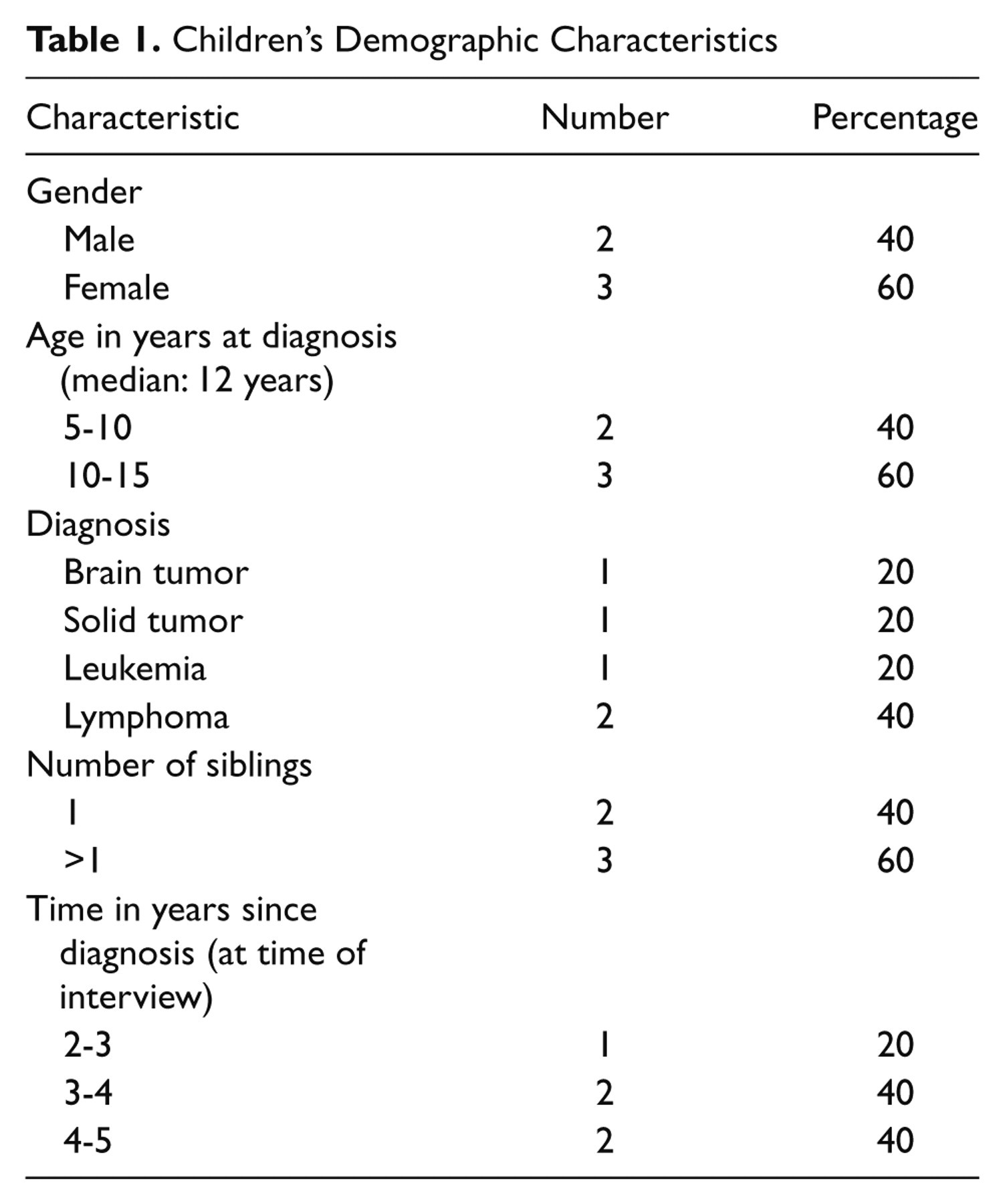
For this study, letters were sent to 22 parents. Five parents consented to participate in the project, all of whom had children who had completed treatment for cancer in the past 3 months to 5 years prior to the start of the study. All the participants lived at least 2.5 hours away (>200 kilometers) from the cancer treatment center. The length of travel ranged from 2.5 (200 km) to nearly 5 hours (330 kilometers) one-way. Of the 5 participants, 4 were mothers and 1 was a father whose ages ranged from 34 to 50 years with a median age of 41 years. Four were married and 1 was divorced. All the parents currently work either part or full time. The distance to the nearest health care facility ranged from 2 to 14 km. The children’s ages at diagnosis ranged from 7 to 15 years with a median age of 12 years; there were 3 girls and 2 boys. Diagnoses included both solid tumors and hematological malignancies. See Table 1 for information about the demographics of the children of the participants.
Children’s Demographic Characteristics
Data Collection Methods
Data collection took place in November 2009 and was carried out by the first author. Each of the parents participated in a semistructured, open-ended interview in a location chosen by the participant. Example interview questions are presented in Table 2. Interviews ranged in length from 45 minutes to 1.5 hours. To preserve the participants’ words in their truest form, all interviews were recorded and transcribed verbatim. Field notes were compiled after each interview and at each stage of the study by the interviewer, which provided thoughts, observations, and details about each interview.
Example of Open-Ended Questions

Data Analysis
Data analysis occurred concurrently with data collection and as described by hermeneutic phenomenologist Max van Manen (1990). van Manen’s approach combines characteristics of descriptive and interpretive phenomenology with the aim of grasping the essence of the parents’ experiences. This is accomplished through the reflective activity of writing as a means of conveying the essence of the lived experience. Following transcription of each interview, the recording was listened to and compared with its transcript to ensure accuracy. Phenomenological reflection, involving conducting thematic analysis and determining essential themes, results in an understanding of the essential meaning of the experience (van Manen, 1990). Recordings and transcripts were reviewed repeatedly for significant statements in an attempt to find meaning and understanding through themes, which are the structures of experience (van Manen, 1990).
Finding meaning and understanding occurred through a process of uncovering thematic aspects and isolating thematic statements (van Manen, 1990). Uncovering thematic aspects recognizes that a phenomenological theme describes one aspect of the experience but is unable to describe the entire lived experience on its own (van Manen, 1990). Thematic statements were isolated using van Manen’s approaches: the wholistic approach, the selective or highlighting approach, and the detailed or line-by-line approach (pp. 92-93). Using the wholistic approach, the text was viewed as a whole to determine the fundamental meaning. The highlighting approach drew attention to statements or phrases that appeared to be essential in the description of the experience. Each sentence was examined to find what it revealed about the phenomenon of interest. It was not only a matter of putting the participants’ words onto paper but also a dynamic process of interpretation of the findings by means of a descriptive account.
Collaborative analysis was used whereby both authors participated in discussions about themes and they were clarified, examined, and reinterpreted (van Manen, 1990). This resulted in the co-creation of the study’s essence and themes by both authors. Not only did this provide the first author with guidance and experience in thematic analysis, but it was also a method of ensuring that the interpretation of the material was an appropriate representation of what the participants shared.
Findings
Although the purpose of the study and the focus of the interviews were to describe the experience of the parents after their child’s cancer treatment had been completed, all the parents were unable to separate their “after-treatment” experience of parenting from their “on-treatment” experience. Hence these findings speak to parents’ experiences with the entire cancer journey, treatment and beyond, in the context of living at a distance to the tertiary cancer center. Data analysis revealed the essence of parents’ lived experience of transitioning to a time when their child has completed treatment for childhood cancer at a distance from the home is a journey within a journey. From the point of diagnosis onward, parents embarked on a cancer journey that continues today. Within their cancer journey, they navigated a treatment journey that seemed to be the only course of action to take in order to make their child better. Parents struggled to move on with their child’s cancer journey as it affected their own lives as a parent of a child with cancer and the lives of their whole family. Families had to travel to the tertiary cancer center for treatment where they met health care providers and other families experiencing childhood cancer. Alongside all these new people, parents continued along the treatment journey as part of their cancer journey. Once the treatment was complete, families were reunited at home and attempted to move on with their lives without cancer as the focus. Cancer did not, however, disappear from their lives rather it shifted out of the foreground of their daily routines. Their cancer journey embodied both positive and negative aspects of having a child with cancer. Although many facets of the treatment journey contained negative characteristics such as symptoms and side effects, the cancer journey included positive characteristics such as the relief and joy of their child’s cancer being cured. Parents spoke about how their childhood cancer journey continues in their families’ lives even though their treatment journey is complete and their child is currently healthy.
Now cancer isn’t the center of our lives. Yeah, it happened but it’s not the focus anymore. (A3)
The experience of having a child complete treatment for childhood cancer will stay with the parents as part of their lives forever:
Yeah, you still think that even though the paper says he’s in remission . . . it’s never over, never . . . It won’t ever go away. You think about it daily and you are concerned always. It impacts me every day . . . But, we do have to keep living, we do have to move on and we have to hold on to the good stuff. I’m not saying that it’s easy. (A5)
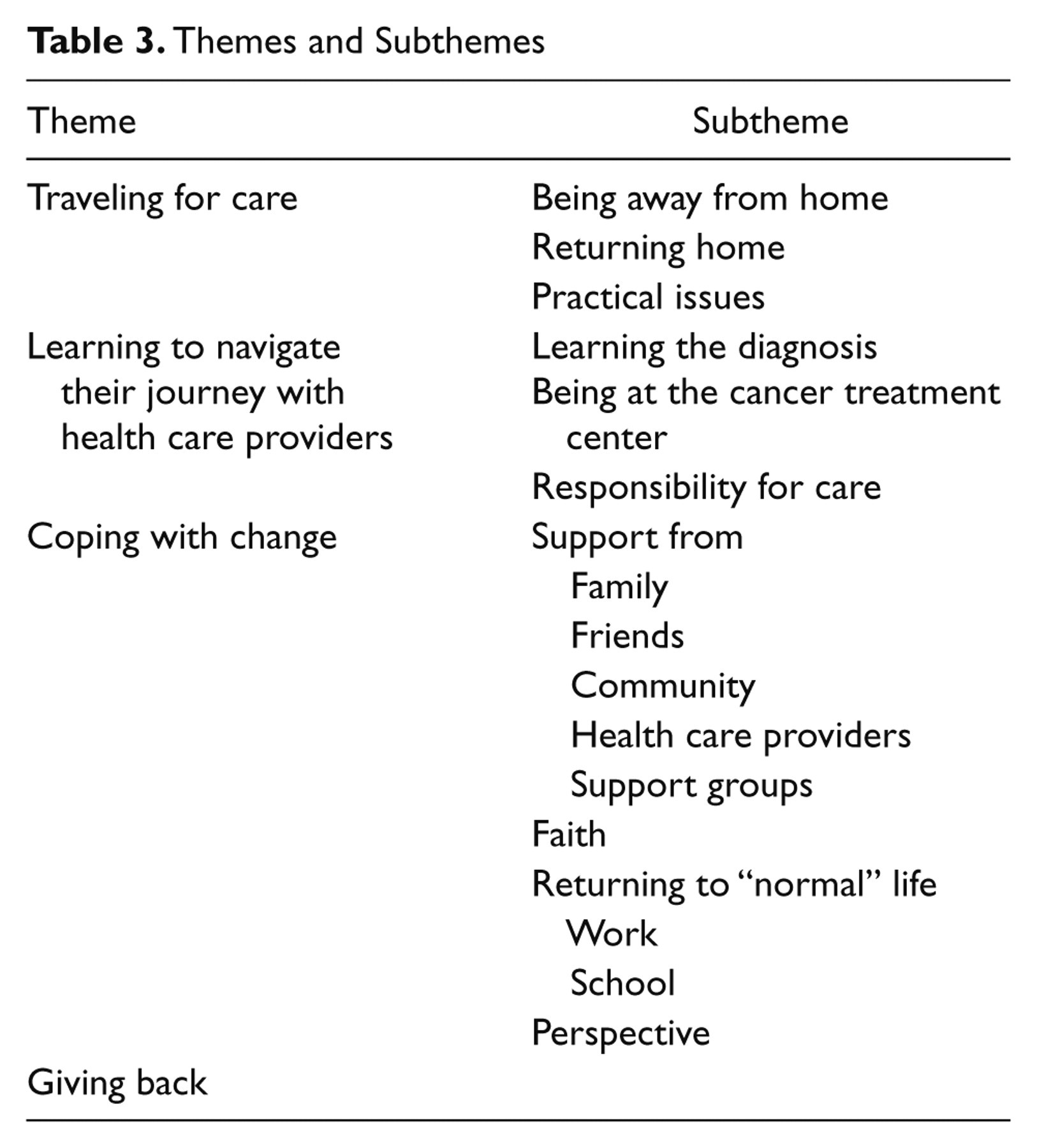
The 4 themes that emerged from the interviews that further characterized the essence were (a) traveling for care, (b) learning to navigate their journey with health care providers, (c) coping with change, and (d) giving back. See Table 3 for a list of the themes and subthemes.
Themes and Subthemes
Traveling for Care
The parents’ treatment and cancer journeys were influenced by the distance between their home and the tertiary center. Parents described a willingness to travel wherever, no matter the distance, in order to ensure that their child received the best care. Knowing their child was receiving care from the expert cancer specialists helped them to move on psychologically with their child’s diagnosis. Because of where the families lived, traveling was connected to the diagnosis of cancer itself. Parents had no choice but to travel to the city where the cancer center was located for treatment and follow-up care, and they understood this as part of their experience:
I think where we live . . . there is a lot of people that go for treatment for cancer . . . I think that we are just so used to being where we are . . . And because we don’t have the facilities . . . I would rather her be there and you don’t look at it so much as a negative or inconvenience though, you feel you are getting the better care. (A1)
Being away from home
Parents and the child with cancer had to be away from home for periods of time in order to receive treatment and follow-up care. As a result, families were separated from each other and from their regular routines because some of the family members remained at home while the child with cancer and a parent went to the city. Because of the distance, families often had to stay in the city after discharge, which kept them away from home for longer periods of time:
So, in between rounds of chemo we weren’t allowed to come home because we lived too far from the hospital. So home, when I said they discharged us home I mean it was to Ronald McDonald House. (A3)
Returning home
In between treatment cycles and after treatment was over, families were allowed to return to their home about which most of the families had mixed feelings. They were grateful to be home and to have their friends and family close by but they worried about being away from the cancer treatment center and their pediatric oncology team in case anything went wrong:
I was excited and completely terrified at the same time about coming home. Excited to sleep in my own bed and enjoy my home once again, and get back to a routine. Terrified it was going to happen all over again and we would have to go back to [cancer center]. I kept bags packed for about a year after, always afraid something was going to happen, and I wanted to be prepared. (A3)
Parents had a sense of security when they were staying at the hospital:
I remember the first time even just going to my mom’s, I was very frightened because you feel safe at the hospital—you are very secure. People are right there and if he breathed wrong I knew that they were there and I could ask someone. (A5)
According to the parents, the children with cancer did not share these feelings:
It was good to come home, she was happy to be at home, she was happier being here. Myself, personally, I liked seeing the doctors more often. (A4)
One mother spoke at length about the difficulties she faced on returning home. Her child had the longest treatment of all the children in the study during which she and her child had to relocate to the cancer center for more than 6 months. It was not until she was at home that she recognized the magnitude of the responsibility that she had to assume as the sole caregiver. She felt totally unprepared and wished she had been warned about what it might be like to be home:
I didn’t know it would be like this when we got home. I thought it was going to be the best thing on earth. And then . . . crash. No one told me about that—nobody. And I know I can’t be the first person that felt that way. Maybe they don’t want to scare us but maybe they should tell you—you know when you go home things are going to be tough, maybe not, maybe there’s a chance you will do okay . . . It would have been nice to know that my anxiety might really get out of control once I got home and I am going to feel really nervous about everything. I wasn’t prepared to be home and to feel the way I did. I wasn’t ready for this or for how I felt at all. Nope, not even a little bit. (A3)
Practical issues
Parents talked about practical issues that affected their travels. Some of these practical issues were related to driving whereas others were related to the time it took to travel to the tertiary cancer center. Families had to carefully plan their follow-up appointments because traveling to the city with the cancer center meant taking time off school and work and meant organizing child care for the sibling of the child with cancer:
It’s the middle of the week, you have to take the time off work . . . So we always have to leave the night before . . . It’s not an hour appointment. It’s a trip. It’s a day. You know it means missing school, missing work, making arrangements for the other [child]. (A1)
Learning to Navigate Their Journey With Health Care Providers
Parents learned to work with the health care providers as part of their cancer journey. By collaborating with their child’s health care provider, parents played an active role in their cancer journey. Parents and health care providers worked as a team to provide care to the child with cancer creating a balance of responsibility. Local health care providers and members of the pediatric oncology team were involved in the child’s care throughout the cancer journey especially as the treatment journey ended:
He had gone to this new family doctor for his blood work and a bit of a check-up. He gets a regular check-up with [oncologist] . . . You know what was good was our [oncologists] would talk to our [general practitioner]. The communication was good. (A5)
Learning the diagnosis
Parents started their diagnosis stories with the symptoms that the child had that started their cancer journey. Because of the rarity of childhood cancer and the vagueness of the presenting symptoms, the children had to see their local health care provider numerous times before a diagnosis was made and most of the children had originally been misdiagnosed. Parents talked about finding out as much as they could about their child’s diagnosis and subsequent treatment as a method of moving along their treatment journey.
Being at the cancer treatment center
Going to a tertiary center meant that the families met new health care providers and had to trust that they knew how to care for the child’s cancer. All the children received the course of treatment that the pediatric oncology team recommended at the tertiary center. Parents felt they had no choice but to follow the treatment journey set forth at the cancer center. Parents trusted that their child was receiving care from highly skilled professionals, which helped the parents move along their cancer journey. One mother found it hard to have to trust the health care professionals immediately on meeting them because there was no time to develop a relationship with the team prior to her child’s diagnosis. Once a relationship was established, she was very happy with the care they provided:
There was no time. The lousy part is that you are not in control. These people are saying “Your son is dying and we don’t know if we can fix him but in order to try—these are the things we have to do . . .” The options weren’t good . . . chemo, gobs of chemo. All you could do was try and absorb what they are trying to tell you and really just hope for the best . . . You totally have to trust these people you’ve never met before in your life. It’s a totally different situation than you have ever been exposed to . . . The nurses were really good; that’s what they do. We felt that they cared and had done it before so they were kinda used to the questions. They helped us a lot. (A5)
Responsibility for care
Parents spoke about working with a variety of health care providers both at home and at the cancer treatment center along their cancer journey, all of whom shared some proportion of care for the child with cancer. Parents had to learn to care for their child while at home between and after the completion of treatment. Local health care providers had varying levels of interest and knowledge about childhood cancer before and after the children were diagnosed. For this reason, some parents were comfortable taking their child to see their local health care provider during and after treatment and some were not. Many of the parents trusted their local doctor to care for their child. Contrary to the families who had local support, one parent talked about her lack of trust in the local health care providers in regards to her son. She felt that she had no choice but to return to the cancer center no matter what her query was about her child with cancer:
The doctors here [in local community] are fine but they even admitted that “[son] is beyond our realm of what we do.” They don’t want to . . . As soon as I have to take him in for something, even now—it’s like you got to go to [tertiary center]. They are still nervous about taking care of [son]. So that’s nerve racking! If I was concerned about something, we would need to go to [tertiary center]. (A3)
Coping With Change
Parents talked about many people and things that helped them deal with their child’s cancer journey and their travels along the way. The changes in their lives brought about from their child’s cancer diagnosis necessitated finding ways of coping with the changes.
Support
Parents talked about a variety of support that was available to them along the cancer trajectory. This support came from family, friends, their community, health care providers, and support groups. Families felt they were fortunate to have huge amounts of support:
Regardless of the horrible circumstances, being there, the diagnosis . . . things worked out along the way. The support has always been amazing, whether it’s the doctors, nurses, family, and friends, whatever. We’ve been very lucky. (A3)
Family
All the parents spoke about the importance of their spouses, siblings, and extended family in their lives prior to and since their child’s cancer diagnosis. Several families felt that the experience of having their child complete treatment for childhood cancer brought their families closer together:
Well my husband, we are good, we talk all the time about everything. If it did anything, it brought our whole family closer . . . and opened our eyes up. You know, we spend more family time together. Now, we eat more meals together, we do more things together. We always did a lot of family stuff . . . but we just make it more of a priority now. (A4)
One of the marriages ended during the course of the treatment journey but despite this, the parent felt that his relationship with his children was strengthened as a result of their family’s experience with cancer:
My wife and I went through a divorce during that time and the children chose to stay and live with me . . . The whole experience has brought me, my daughter, and my son a lot closer together. Although it pushed their mother away throughout it all. (A2)
Friends
Parents talked about friends who were essential means of support along their cancer journey. Some of the families had friends from home that helped them during the treatment journey. A couple of the parents talked about new friends who they met at the tertiary center while their child was in for treatment. These were often parents whose children were also going through treatment for childhood cancer and continue to provide support now.
Community
For the parents in this study, living in a small town or community meant that many people knew about their child’s cancer diagnosis. Families described an enormous amount of support that they received from their community:
Yeah, and the community is still incredible. [Nearest town] is big enough, I don’t know everybody but everyone knows us. Yeah, they really rallied. That’s the one nice thing, okay maybe that’s the one pro of being from a small community. The support was beyond your imagination where I know in [city with tertiary center] it’s not the same. (A3)
Many of the members of the community wanted to help the family in some manner. For one family, this meant that community members helped to look after their property while they were away at the treatment center. Some of the parents talked about how their communities provided financial support by conducting fundraisers for the families:
They had a [party] and then they had this meat draw . . . and raised $20,000 . . . So it’s just unbelievable how people come together for stuff—for sick kids. It was great. (A3)
Health care providers
All the parents mentioned how valuable the support from the tertiary center health care providers was both during and after treatment. There were many positive comments about the health care team at the cancer center. After their treatment journey was completed, the parents found that being able to get in contact with their health care providers at the tertiary cancer center was extremely comforting. They felt they could call whenever they needed to at any time of day or night with concerns about their child:
I’m thankful that they didn’t mind me calling—the . . . nurses . . . I am thankful that I had the pager number so if it was midnight I could do that. Whoever was on call, I could tell them [child with cancer] had a fever and I felt comfortable doing that and I felt they were welcoming me to do that. I didn’t feel like “Oh, I don’t want to bother them.” I went ahead and did it and they never made me feel bad about it . . (A3)
Support groups
Parents talked about support groups that were available to them and their families both in person and online. One mother found that the online support group for parents of children with her child’s specific diagnosis was a tremendous source of support and of information because members are sharing similar experiences:
I’m on a support group on the computer like for [specific childhood cancer diagnosis] parents. But I have been on that since she was diagnosed. You know, everybody is living the same thing; we’re all fighting for your kids . . (A4)
Faith
Three of the parents discussed how certain aspects of their faith helped them cope with the changes brought on by their child’s cancer. Two families spoke about using prayer as a way of dealing with the diagnosis and between follow-up appointments. One parent spoke at length about how his faith helped him cope with the changes to his life that were brought about as a result of his child’s diagnosis. His faith was embedded within his cancer journey:
I knew it was going to be a long process, I was afraid. I had arguments with God . . . I remember the night that I found out she had cancer, I was looking at her lying on the couch and I was kinda like arguing with God about why her not me . . . Those thoughts come to me and I was able to let it go and turn it over to a higher power. And when I did that, I was okay with it—no matter what the outcome was it was out of my hands . . (A2)
Returning to “Normal” Life
As their treatment journey ended, their cancer journey continued. All the parents said that they had returned to lives similar to their lives prior to the child’s diagnosis.
Work
Parents spoke about the need to alter their work schedules during their child’s treatment and to accommodate follow-up care. Changing work schedules affected all the families’ finances to some degree.
School
Most of the children missed close to a year of school during their cancer treatment and parents reported that all the children were able to catch up in their studies when they returned to school although it was easier for some than for others. One parent spoke about how she felt it was important for her child to continue to do schoolwork during treatment and how returning to school helped her child return to “normal” life:
But I felt like if I wasn’t making him go to school then what was the point of it all. Like, I didn’t want him to think he was dying. It was all about “You’re going to be okay, we’re going to do this. We’re not gonna give up.” I didn’t want him to think “Oh mom’s not making me go to school so that must mean I don’t need to.” So I did, I made him. (A3)
Perspective
Several of the parents stated that they always knew that it could have been worse for their child than it was. Looking at it from this perspective helped the parents cope with their child’s diagnosis:
She is lucky though . . . When we were going through treatment, there were always kids worse off than mine. When she was in ICU, there were kids who were dying—like dying right then and there! She wasn’t dying. You know what I mean. So I always look at it and I still do look at it—there’s always worse than us so that helps—thinking that way. (A4)
The parents also talked about how their outlook on life had changed as a result of their child’s cancer. Parents reported positive consequences to their child’s diagnosis such as living in the moment and appreciating each day, which lead them to express love more readily.
Giving Back
Parents felt that they were in a fortunate position to have a healthy child who had completed treatment for childhood cancer and wanted to show their appreciation in some way. They talked about how they and their children spoke at and participated in fundraising events for cancer and associated causes. Parents were willing to share their stories in order to educate others and to raise funds to further improve the experience of others. The parents who participated in this study said they did so to help other parents who may be going through what they have already experienced. Their altruism extended to other ways of sharing their stories but it was always to help other families with cancer.
Anything I can do to help you and help maybe somebody else, some other parents or whatever . . . I just want to try to help out. (A2)
Discussion
The Essence of Parents’ Lived Experience
Once their treatment journey was over and travels to the treatment center for the child’s cancer were infrequent, the cancer journey continued to be part of the family’s lives. Parents felt that their child’s cancer diagnosis influenced who they are and how they live their lives even years after the treatment was complete. Their child’s cancer is never far from the parents’ minds and will always be concerned about recurrence. In a study talking to children undergoing treatment for cancer and their families, Woodgate (2006b) uncovered a similar narrative, “it is never over with . . . always a waiting game” (p. 6). Families felt that their child’s cancer journey would always be a part of their lives and that the fear of recurrence would be present long after treatment ended (Woodgate, 2006b). This has been previously described as the Damocles syndrome (Koocher & O’Malley, 1981), which is a persistent fear that the child’s cancer will return. Children with cancer and their families learn to live with uncertainty along their entire cancer journey (Woodgate & Degner, 2002) and the time period after treatment ends was no exception for parents in the current study.
Traveling for Care
A literature review of traveling for cancer care found that adults with cancer who had to travel to receive treatment for cancer considered traveling to the treatment center from a minor inconvenience to a barrier to treatment (Payne, Jarrett, & Jeffs, 2000). A couple of parents in the current study said that the distance they had to travel for their children’s care was counterbalanced by the higher quality of care their child received. This particular finding is contrary to previous studies of rural families with children with cancer who reported many difficulties associated with traveling for cancer treatment (Scott-Findlay & Chalmers, 2001; Woodgate, 2001).
Learning to Navigate Their Journey With Health Care Providers
In pediatric oncology, the most effective relationship between nurses and parents is when they work together to provide care to the child with cancer (Romaniuk & Kristjanson, 1995). Trusting the pediatric oncology providers is an integral part of treatment for childhood cancer (Kerr, Harrison, Medves, Tranmer, & Fitch, 2007; Woodgate & Yanofsky, 2010). Pediatric oncology health care providers play an important partnership role with the family along the cancer journey starting at the cancer center during treatment and provide valuable support for families during and after treatment (Kerr et al., 2007; Scott-Findlay & Chalmers, 2001; Woodgate & Yanofsky, 2010). Parents in the current study felt strongly that their child was receiving the highest quality care by the experts in the field who worked at the tertiary cancer center.
Several of the families had local care providers in whom they trusted and had traveled along their journey with them starting prior to diagnosis. These parents felt confident that their local health care provider was willing to learn about their child’s diagnosis and treatment plan along the course of treatment and beyond. One of the parents did not have anyone in her local community in whom she trusted to look after her child’s medical needs so she had to return to the tertiary center any time there was a health issue with her son. Having someone close to their home, in whom the family can trust to provide medical care, may influence the parents’ experience of having to travel to receive cancer treatment.
Coping with Change
Support
For families with a child with cancer, social support is an important need that must be met (Dahlquist, Czyzewski, & Jones, 1996; Hoekstra-Weebers, Jaspers, Kamps, & Klip, 1998; Kerr et al., 2007; Ljungman et al., 2003; Shields et al., 1995; Woodgate & Degner, 2003; Yeh, Lee, Chen, & Li, 2000). According to past studies about children with cancer, support may include family, friends, other parents whose child had cancer, and health care providers (Aitken & Hathaway, 1993; Enskar, Carlsson, Golsater, Hamrin, & Kreuger, 1997; Lindahl Norberg & Boman, 2007; Shields et al., 1995; Woodgate, 2001; Yeh et al., 2000). All the parents in the current study had these sources of support as well as from their community, which has been reported to be an important source of emotional, financial, and practical support for rural children with cancer and their families (Labay et al., 2004; Scott-Findlay & Chalmers, 2001;Woodgate, 2001). It is possible that the support that the parents in the current study received was at least partly responsible for their willingness to travel to the tertiary center. All the parents felt they had strong support systems while at home and at the hospital. This may have affected their experience of having to travel to receive treatment.
Faith
Religion has been reported as a coping mechanism for some families with children with cancer (Goldbeck, 2001; Kerr, Harrison, Medves, & Tranmer, 2004; Patterson et al., 2003). In the current study, 2 parents discussed how and when they used prayer along their cancer journey, which has been reported in pediatric oncology literature (Post-White, 2006; Wilkins & Woodgate, 2007).
Returning to “normal” life
As parents moved on with their child’s cancer, they were able to return to a life similar to one they had known before. In pediatric oncology literature, this is referred to as the “new normal” (Clarke-Steffen, 1993; Woodgate, 2001). All the families had their work and school lives interrupted to some degree as a result of their child’s cancer diagnosis. For the parents, a loss or reduction of income was reported, which is common for families with children with cancer (Aitken & Hathaway, 1993; Enskar et al., 1997; Mercer & Ritchie, 1997; Ortiz & Lima, 2007; Scott-Findlay & Chalmers, 2001; Woodgate, 2001). Financial aspects of being a rural oncology patient are well documented (Aitken & Hathaway, 1993; Clavarino, Lowe, Carmont, & Balanda, 2002; Scott-Findlay & Chalmers, 2001; Wilkes, White, Mohan, & Beale, 2006; Woodgate, 2001). Parents in the current study did mention finances but it did not feature prominently in the findings, contrary to what would have been expected based on the literature. Neither did they expand on their child’s return to school. This may be a reflection of the small number of participants or the lack of probing by the interviewer.
Perspective
A few of the parents talked about how they always compared their situation with others and felt that it could have always been worse for their child. Previous research found that parents rationalized their child’s symptoms that lingered after treatments by thinking that it could always be worse (Woodgate & Degner, 2004). In the literature about children with cancer, several studies report positive aspects of a diagnosis of childhood cancer, such as a deeper appreciation of life (Parry & Chesler, 2005), of the present day (Lindahl Norberg & Steneby, 2009), and of the small things in life (Ortiz & Lima, 2007). Parents in the current study described that they appreciated life more than they had before their child’s diagnosis and that they lived more for today, which has also been found in other studies of parents with children with cancer (Van Dongen-Melman et al., 1998).
Giving Back
All the parents felt grateful to have currently healthy children and felt it was important to be able to give something back. Many families were involved with cancer fundraisers. This is a common occurrence for cancer survivors and is echoed in a recent study of parents’ experience with pediatric oncology clinical trials (Woodgate & Yanofsky, 2010). Parents recognized and were grateful to previous parents for agreeing to participate in the studies that had improved treatment for childhood cancer and wanted to give back to the childhood cancer community as a whole (Woodgate & Yanofsky, 2010).
Common Rural Experiences
For the parents in this study, where the families lived in relation to the cancer treatment center influenced every aspect of their cancer experience even though they did not consider the distance traveled as a burden. Families who live in rural areas have many experiences similar to families not residing in rural areas (Woodgate, 2001). These experiences nonetheless may be exacerbated for the families who live at a distance. All families of children with cancer spend a lot of time at the hospital and potentially apart from the rest of their family. Families who do not live close to the treatment center may not see members of their families during treatment at the cancer center. Returning home for the first time is a stressful time for families. However, rural families do not have the children’s hospital close at hand as a safety net.
Scheduling child care for siblings, the spouse having to continue to work and the children missing school are experienced by all families with childhood cancer whether they live near to or far from the treatment center. However, coordinating the family’s schedule may prove more difficult when one of the parents is away from home for long periods of time. Families with children with cancer experience additional costs such as parking, food, and travel-related costs. It is likely that families who must travel for cancer treatment incur higher travel-related costs because of the longer distances that are covered, which are doubled when the rest of the family come to visit the child in the hospital.
Community support is one aspect that seems to be stronger for families who must travel for cancer treatment than for urban families. All the families in this study and in 2 other studies (Scott-Findlay & Chalmers, 2001; Woodgate, 2001) involving rural children with cancer, talked about incredible amounts of social and financial support they received from their local community after their child was diagnosed with cancer. Woodgate (2001) uncovered that both rural and urban families had changes in social support and in their financial situations during the course of their children’s cancer treatment but for rural families, the differences were more pronounced. Finances were negatively affected for the rural families to a greater degree than their urban counterparts (Woodgate, 2001).
Implications for Nursing Practice
Although parents spoke about their experiences along their entire cancer journey, only nursing implications that will serve to help parents after the completion of treatment are presented.
Regular assessment of the family’s support system is important during the childhood cancer trajectory especially when families live at a distance from the treatment center. After treatment ends, the children are not seen by their pediatric oncology team as frequently, which means that a comprehensive assessment at their follow-up appointments is even more imperative. Recognizing that the parents may not be able to separate their experiences during treatment from their time after treatment ends is valuable for the entire team. Cancer remains part of their daily lives, in their thoughts, memories, and their child’s long-term or late effects. Health care providers working with this population should continue to address the needs of children and their families, especially informational and psychosocial needs that change as the treatment ends.
Nurses play an integral role in providing anticipatory guidance to families of children who are completing treatment for cancer. Nurses should regularly assess the family’s readiness to return home and talk with them about what going home may look like for their particular family especially if the family lives a great distance from the cancer treatment center. Informing them of possible emotions they may experience once they are home and resources for dealing with their emotions would prove valuable for all families including those who must travel for cancer treatment. This could be initiated during the last few admissions or visits to the cancer center. Parents in this study found the health care providers at the cancer center to be a tremendous source of information and support. Being knowledgeable, staying abreast of information for families, and providing suggestions for support groups for the child, the parent(s), and the sibling(s) is a key nursing function in pediatric oncology. Providing information about the child’s cancer and possible sources of support that can be accessed at home is important especially immediately after the completion of treatment.
Having health care providers in their local communities in whom they trust is important to families of children with cancer. Although many of the families in this study did have a family doctor they felt comfortable looking after their child, the doctor had little or no knowledge or experience with childhood cancer prior to their child’s diagnosis. Throughout the cancer trajectory, a link between the tertiary cancer center and the primary health care provider, such as using teleconferences and having a nurse who could serve as a liaison for the family may prove useful on many fronts. This link would provide information and support to the families when they are at home, education about pediatric oncology to the local health care provider, and facilitate communication between all members of the team especially the families. Continuing the link after treatment is complete would provide a valuable source of support and information to families and local health care providers in regards to follow-up care.
Limitations
There are several limitations to consider in regards to the current study. The sample size was small but was consistent with the principles of phenomenologic research, as it included only those people who had experienced and were able to discuss their experiences of the phenomenon of interest. Further research should be done to corroborate the findings. Having only one male perspective is a limitation; however, his experience did not differ significantly from the mothers in this study. Parents in this study were all Caucasian; talking with parents of different ethnic backgrounds would provide a more culturally diverse picture. The children had a variety of cancer diagnoses that affected the type, length, and intensity of treatment, which may influence the experience of the parents caring for these children after the completion of the treatment. Further study of the relationship between type, length, and intensity of treatment and ability to cope when returning home is warranted. Longitudinal work would also provide additional information about the rural experience of cancer. Finally, the major limitation of the study is that there were no families who lived in remote locations, which would have provided more information about the experience of having to travel for care. Compared with families in remote locations served by the tertiary cancer center, the distances that the families in this study had to travel for their child’s cancer treatment were relatively short.
Conclusion
Prior to this study, little was known about the experience of parents caring for a child who has completed cancer treatment while living at a distance from the cancer treatment center; this study provides insight into this experience. Overall, parents expressed a willingness to travel wherever required in order for their child to receive the best care and traveling for cancer care was part of their cancer journey. Several of the parents had local health care providers in whom they trusted and who were interested in working with the child with cancer during and after treatment. Families who do not live near their child’s tertiary cancer center have similar experiences as families living in an urban setting. Further research is required to examine whether families in other parts of Canada and the world, share similar experiences.
Nurses must recognize the potential needs of families who must travel for care during and after treatment for their child’s cancer.
Footnotes
Acknowledgements
The authors would like to thank the participants in this study who graciously shared their stories and experiences.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: