
Abstract
Children with chronic health care needs, including those with cancer, require complex care under direct caregiver supervision. This intensive care management may result in increased stress and psychological distress for the caregiver and family. Respite care services are needed in providing alleviation of caregiver stress among families of children with complex health care needs. This report describes the feasibility of a pilot hospital-based respite care program for caregivers of pediatric oncology patients and their siblings and development of a permanent, expanded service to include both inpatient and outpatient units under the supervision of hospital volunteer services. During the feasibility pilot, 39 respite care requests were made by caregivers for care of patients, with 67% of these requests for care of infants and toddlers. The respite care providers were hospital volunteers. Reasons for the caregiver respite care request included a need to leave the hospital for running an errand, eating a meal, taking a mental break, or talking with the medical team. At the completion of the pilot, caregivers and staff were surveyed and expressed a strong desire for continuation of the service. The success of the pilot led to the implementation of a formal respite care program, Helping Hands, which provides services 7 days a week for inpatients, outpatients, and their siblings. Although this respite care service is specific to children with cancer, the program model is feasible within most pediatric care facilities.
Introduction
Children with special health care needs are defined as those requiring care and services beyond that typical for age (McPherson et al., 1998). The stress associated with the child’s special health care needs may become overwhelming, producing periods of stress and potentially poor psychosocial adjustment for the caregivers (Montes & Halterman, 2007; Moskowitz et al., 2007; Nolan, Camfield, & Camfield, 2006). The American Academy of Pediatrics (Johnson & Kastner, 2005) recommends respite care services for families of children with special needs. When asked to rank needed services, caregivers caring for children with special health care needs ranked respite care as one of the most needed services (Perrin, Lewkowicz, & Young, 2000).
Cancer constitutes a special health care need due to the complexity of medical treatment. Caregivers of children with cancer often provide complex home health care, including central line care and intravenous administration of fluids and medications. They also accompany the child to their frequent clinic appointments and attend to the child during hospitalizations. Although many programs describe respite care for children at the end of life or in chronic health conditions, no programs describing respite care for a child actively receiving cancer treatment were identified via a comprehensive review of the literature. The aim of this pilot program was to explore the feasibility of a hospital-based respite care service for pediatric oncology patients and their siblings, using the existing institutional volunteer services program.
Review of the Literature
Respite care is defined as complementary, flexible care in the home or another setting with appropriate medical and nursing support, offering parents or caregivers relief (Judd, 1995). Other venues of respite care may not provide direct medical or nursing care, instead providing relief of caregiver burden. These psychological support respite programs can be important for those along the continuum of care, from pediatrics to geriatrics. Respite care should be offered within a family-centered approach, as a partnership in caring, while promoting benefit in well-being to the caregiver (Corkin, Price, & Gillespie, 2006). The most effective respite services for children have been described as meeting the needs of the child and family, most specifically services providing accessibility, flexibility, and location (Glendinning & Kirk, 2000). However, respite care has been viewed as being a crisis intervention as opposed to a standard of care (Thurgate, 2005).
There are numerous types of respite care with services used in a variety of settings. Most of the described respite care services are associated with care of patients with special health care needs resulting from limited cognition, limited mobility, or at the end of life. One review described 2 types of respite care: institutional care, which includes the hospital, and residential care, which includes the home or facility setting (Miller, 2002). The author described respite care through hospitalization as being an inappropriate use of hospital and staff resources, whereas residential care was believed to be a reliable alternative. However, many residential settings have limited space and lack trained caregivers. Hospice care facilities have been used as respite care facilities; however, these facilities may not be available to or suited for pediatric patients. Another option is the shared respite resource, the provision of respite care between families with special needs children. Families may alternate the care responsibilities, allowing the respite family time away. Last, home-based respite is the most common and most convenient for the family. However, the caregiver must ensure that the respite caregiver is properly trained according to the child’s needs, with recruitment and retention of the respite caregiver challenging.
Respite care has been further described as a method of care in which the voluntary sector and statutory services may help support families in caring for children with special needs (Kendle & Companale, 2001). One program used the collaboration between respite care service and a school of nursing, with respite care services provided by nursing students in the community (Kendle & Companale, 2001). The nursing students were oriented to family-centered care, completed required pediatric training hours, and provided a needed community service of respite care to caregivers of children with special needs.
When developing respite care services, the demographics of those in need of respite care should be considered. In a study by Nageswaran (2009), family respite care needs were found to be higher among those with younger children, low maternal education, low household income, and minority race/ethnicity. Caregivers having children younger than 6 years were three times more likely and those with children between 6 and 11 years of age were twice more likely to request respite care than those with children from 12 through 17 years of age. However, regardless of age, as limitations or health care complexity increased, the need for respite care increased. Although the study found that 9% of the surveyed families needed respite care, 25% of the surveyed families had unmet needs. While respite care is needed by more than a quarter of families with special needs children, the request may not be verbalized, or the request may go unmet due to lack of resources. For those with respite resources, many parents do not use them because they do not want their child to be viewed as a burden (Nageswaran, 2009).
Feasibility of an In-House Respite Care Program
Setting
A single-site feasibility program was implemented at the largest freestanding pediatric cancer hospital in the United States. The hospital has 63 inpatient beds and treats an average of 230 outpatients each day. Most patients are not local residents, and treatment protocols often dictate that patients and families stay in designated housing for weeks to months. As many families are from out of town, they may not have extended family members to assist in the care of the patient and siblings. Staff and volunteers get to know families intimately, and the care of the entire family becomes a high priority. As a hospital dedicated to family-centered care, siblings of patients are allowed in the inpatient and outpatient room and common play areas, with the inpatient bone marrow transplant unit being an exception.
Initiation of A Pilot Respite Care Program
In the fall of 2008, the inpatient nursing staff noted that during the child’s hospitalization, several caregivers would ask if staff were available to sit with their child while they attended to family business or took a break from the unit. This prompted discussion and committee formation with representatives from outpatient and inpatient nursing, child life, social work, and volunteer services to determine the feasibility of a respite care service. The committee reviewed potential solutions to providing respite care without placing an additional burden on the clinical service providers. The committee drafted a pilot feasibility program to determine the practicality of offering hospital-based respite care through the volunteer services program. Providing respite care through volunteer services would not interfere with clinical care staffing and would not require additional funding. The program development was exempt from institutional review board approval.
Volunteers play an integral role within the hospital, with more than 500 volunteers in active service and 2 full-time volunteer coordinators under the director of Volunteer Services. All volunteers are screened through completion of an application, prescreening questionnaire, interview and information session, completion of a competency checklist, background check, and occupational health clearance. Orientation consists of hazard surveillance, confidentiality, boundary training, Health Insurance Portability and Accountability Act training, characteristics of populations served, and patient neglect, abuse, and social network policies. The volunteer program has more than 15 standard placements, each with job-specific duties and standard requirements. Volunteer training is specific to the placement, with one being respite care. The respite care volunteer must be at least 24 years of age and attend a 3-hour respite care training session. Each session describes the respite care volunteer’s role and scope, education regarding the patients and families served, professional and personal boundaries, confidentiality, infection control, navigating an inpatient unit, and volunteer limitations. Training also includes where to find supplies, how to communicate with staff, how to communicate care handoff between volunteers, and instruction in operation of equipment (ie., bedrails, call button). Each volunteer has a 2-month probationary period to assure they are competent in the care of patients. At the completion of the probationary period, volunteers complete a satisfaction survey to determine their fit for the assignment.
The pilot program began with respite care offered to caregivers of hospitalized patients and their siblings once per week, every Tuesday from 9 AM to 4 PM, with each session limited to 2 hours. Three experienced volunteers were chosen as respite care providers, and the day of service was determined according to the volunteer’s schedule. The pilot program was conducted over 4 months and was promoted among all Patient Care Services disciplines.
At the initiation of the pilot program, caregivers were informed of the respite care service. Flyers were placed in hospital rooms and common areas of the hospital. Additionally, the volunteers made rounds within the units to inform families that respite care was available, and business referral cards were left with families and staff. Caregiver requests were made directly to a staff member, most often the inpatient nurse. Requests were further facilitated by the staff ensuring that the caregiver and patient needs were conveyed to the respite care volunteer. Additionally, staff referral provided a specific contact for the volunteer to relay any questions or concerns during the encounter.
Respite Care Service Demographics
During the 4-month pilot respite care program, there were 39 requests to volunteer services for respite care. The range for requested services was 1 to 5 per week, with an average of 2 requests. Most respite care requests were initiated by caregivers from the inpatient leukemia service to the inpatient nurse, followed by social work. The majority of the children cared for in the respite care pilot were less than 6 years old (infants [23%], toddlers [41%], and preschoolers [27%]). There were 5 requests for sibling respite care, and the average duration for patient or sibling encounters was 1 to 1.5 hours.
Staff and Volunteer Perspective
At the completion of the pilot, 150 surveys were distributed to clinical staff for service evaluation. Sixty nine were returned, with more than half of the surveys completed by inpatient nurses. The survey asked the staff to report their perceptions regarding why caregivers used respite care. As perceived by the clinical staff, the most common response was that the caregiver needed to run an errand or eat a meal, needed a mental break, or the health care team requested a private meeting with the caregiver. Staff also evaluated the respite care provided by the volunteer. All staff responses indicated that the volunteers were friendly, professional, informed, timely, calm, safe, and communicative. Finally, the staff rated the overall success of the pilot, with 97% evaluating the respite care service as meeting a need and expressed that the program should continue with expansion of respite care offerings throughout the week and weekend.
Volunteers completed a daily verbal summary of their respite care experiences with the volunteer coordinator. In addition, volunteers participated in a focus group that included the respite care volunteers, the director of volunteer services, and the volunteer coordinators. The focus groups were continued monthly with discussion of what worked, what did not work, and what needed to be changed. The volunteers completed a survey at the conclusion of the pilot program and reported that the experience was enjoyable, the respite care was necessary, they enjoyed working directly with the families, found that needed supplies were available in caring for the patient or sibling, and agreed that staff gave appropriate instructions during the handoff to the respite care volunteer. During the focus groups, volunteers did indicate opportunities for role clarification, specifically for staff education regarding the differences in job duties between child life volunteers and respite care volunteers. Staff also expressed confusion between the roles and scope of the daytime respite care volunteers and the existing evening amenity relief volunteers. The amenity relief volunteer is a role for evening and weekend volunteers who distribute blankets, food items, toys, games, and equipment on the inpatient and outpatient units. These volunteers provide play opportunities for the patients during the evenings and weekends. Many caregivers would take the opportunity to leave the nursing unit when an amenity relief volunteer was present, but it was not a service marketed as respite care. Due to similarity of services, the 2 programs merged to lessen staff and caregiver confusion and expand available respite care services to evenings and weekends.
Caregiver Perspective
Five caregivers who used the pilot program completed a 4-item Likert-type scale (poor to excellent) satisfaction survey. The survey results ranked volunteers’ performance as “excellent” in the following categories: friendly, professional, confident, informed, timely, calm, safe, and communicative. Caregivers indicated that they would absolutely use the service again, and one caregiver expressed, “Respite care is the avenue for my family when I need a break.”
Helping Hands: Hospital-Based Respite Care
Data collected from the satisfaction survey, volunteer focus groups, and program impact figures determined that the pilot was a utilized service and in need of expansion in providing respite care for patients and family. To expand the program, additional volunteers were recruited, and hours were expanded to Tuesday and Wednesday from 9 AM to 9 PM, with services offered all other weekdays from 6 PM to 9 PM and from noon to 8 PM on Saturdays and Sundays. In September 2010, the expanded respite care program for patients and their siblings was launched under the name “Helping Hands.” These volunteers may care for the patient and sibling in the patient’s hospital room or common play area. Play guidelines for the sibling are the same as those for the patient, with no sharing of disposable supplies such as clay, and all toys are cleaned after each use. For siblings who require assistance with toileting, the caregiver must stay within close proximity; for patients, the nursing staff provides assistance.
From September 2010 to June 2011, a total of 595 individuals were served through the Helping Hands program, with 60 of these being patients’ siblings. Caregivers of children with leukemia used the respite care service most during hospitalization, whereas caregivers of children with solid tumors used the respite care service most during outpatient clinic appointments. Not surprisingly, the most frequent request was for patients and siblings aged 1 to 5 years, followed by those aged 6 to 12 years. Most respite encounters were less than 1 hour, and most of them occurred during the evening hours, 6 to 9 PM. Figure 1 shows the use of the service over the 10-month period according to time increments within the volunteer’s shift.
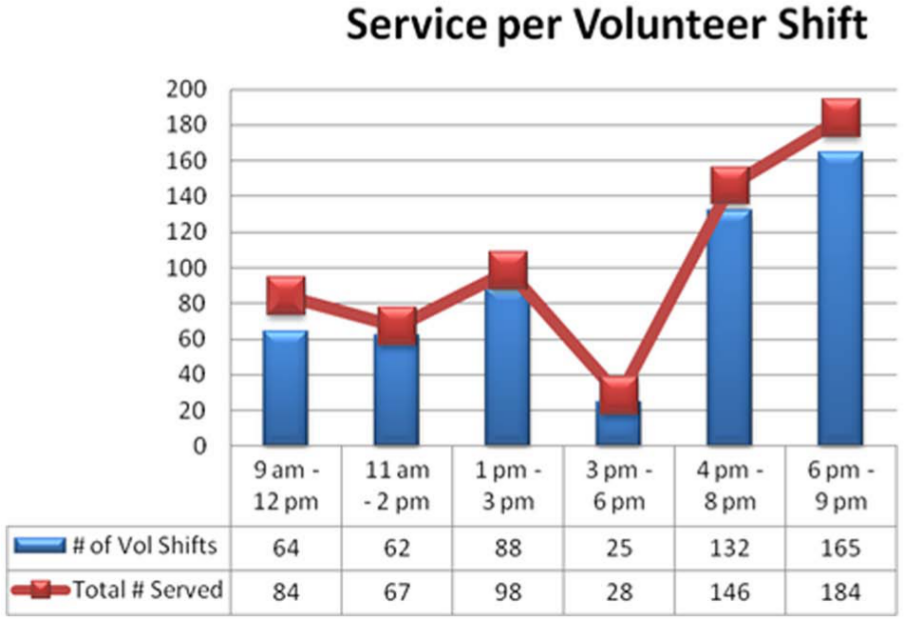
Number of patients and siblings served per volunteer shift over 10 months.
Discussion
Caregivers with children younger than 11 years are most likely to use a respite service (Nageswaran, 2009) consistent with the age of patients and siblings participating in both the described pilot and the Helping Hands program. The Helping Hands program was used most frequently by caregivers during their child’s hospitalization, with the Leukemia Service having highest utilization. This is probably explained by the lengthy leukemia treatment plan, including periods of induction, consolidation, and re-induction, as well as higher occurrences of hospitalization secondary to episodes of fever with neutropenia (Hakim, Flynn, Knapp, Srivastava, & Gaur, 2009). Due to lengthy hospital stays, caregivers are in need of mental breaks, eating a meal away from the unit, doing laundry, and returning to housing. Since the service has been expanded to the outpatient setting, the Solid Tumor Service families have used outpatient respite care more than other services. The increased utilization by the Solid Tumor Service families may reflect the length of the outpatient clinic visit. Patients with solid tumors are more likely to have lengthy clinic visits, including diagnostic imaging, rehabilitation services, and psychology, than patients with leukemia. Caregivers have also requested respite care while they donate blood products in the on-site Blood Donor Center.
Helping Hands respite services for both inpatient and outpatient occur most often between the hours of 6 and 9 PM. Several caregivers expressed appreciation for having time away from the hospital. One couple with no local family support was able to use the respite service and celebrate their wedding anniversary with a dinner away from the hospital. Others have stated that it provides a time of reflecting and regaining of strength needed to support their child through the cancer journey. Respite care then serves the purpose of promoting the well-being of the caregiver and family (Corkin et al., 2006).
Although the literature does not support hospitalization as a venue in providing respite care (Miller, 2002), our program has made respite care a standard of practice during the child’s hospitalization. Through the utilization of hospital volunteers, the service does not place a burden on clinical care and therapeutic services nor does it place a financial burden on the caregiver or institution. Additionally, the needs of the patient and sibling can be met in the hospital through an accessible service within a convenient location, as convenience is an important consideration in successful respite care programs.
Future Direction
Although the program has provided an accessible, convenient service for caregivers, several limitations are noted. The current program has limited daytime offerings due to the number of available respite care volunteers. Daytime expansion of services beyond Tuesday and Wednesday is being considered by Volunteer Services, with recruitment of daytime respite care volunteers.
Caregivers who have not used the service have subsequently been surveyed and have expressed that they would use Helping Hands if they were more familiar with the program. The Helping Hands program continues to be promoted internally, with an article recently published in the family newsletter, explaining the program from a caregiver perspective. Informative flyers in both English and Spanish have been placed in all inpatient caregiver overnight rooms and within the family booklet given to all new patients. In addition, staff is encouraged to promote the program to all families.
Many caregivers do not use respite care services even when in need. Caregivers have reported the greatest barrier being the effort of time and resources in arranging respite care services (Neufeld, Query, & Drummond, 2001). The Helping Hands program eliminates the barrier of effort and resources; therefore, further study should determine reasons for participation and nonparticipation in accessible respite care programs. In the context of family-centered care, it is important that health care providers instill in caregivers the importance of caring for the caregiver of children with cancer and other chronic health conditions.
Footnotes
Acknowledgements
To volunteers, Swetha Shankar, Katy Johnson, and Maureen Kennedy, for their involvement in the respite care pilot. To Tricia Spence for her involvement in the day-to-day implementation of the Helping Hands program. To Pam Dotson, MBA, RN, Senior Vice President of Patient Care Services and Chief Nursing Officer, for her advocacy of the volunteer program overall, and its support in improving the quality of life for our patients and families. To David Galloway, PhD, ELS, for editing this article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported in part by a Cancer Center Support grant (CA 21765) from the National Cancer Institute and by the American Lebanese Syrian Associated Charities.