
Abstract
Throughout the trajectory of the cancer experience, children and adolescents will likely face pain and anxiety in a variety of circumstances. Integrative therapies may be used either alone or as an adjunct to standard analgesics. Children are often very receptive to integrative therapies such as music, art, guided imagery, massage, therapeutic play, distraction, and other modalities. The effect of integrative modalities on pain and anxiety in children with cancer has not been systematically examined across the entire cancer experience. An in-depth search of PubMed, CINAHL, MedLine, PsychInfo, and Web of Science, integrative medicine journals, and the reference lists of review articles using the search terms pain, anxiety, pediatric, child*, oncology, cancer, neoplasm, complementary, integrative, nonconventional, and unconventional yielded 164 articles. Of these, 25 warranted full-text review. Cohen’s d calculations show medium (d = 0.70) to extremely large (8.57) effect sizes indicating that integrative interventions may be very effective for pain and anxiety in children undergoing cancer treatment. Integrative modalities warrant further study with larger sample sizes to better determine their effectiveness in this population.
Introduction
Integrative medicine is a holistic body–mind–spirit approach that combines both Western medicine and complementary therapies to best serve patient and family health care needs. The term integrative acknowledges the blend of conventional and complementary therapies for the most comprehensive treatment for patients. According to the National Center for Complementary and Alternative Medicine, the general categories of integrative medicine are natural products (herbs, botanicals, vitamins, and other dietary supplements), mind–body practices (prayer, meditation, yoga, acupuncture, guided imagery, hypnotherapy, tai chi), manipulative practices (massage, chiropractic), biofield therapies (Reiki, healing touch, qi gong), traditional healers (sometimes called “folk healers”), and whole medical systems such as ayurvedic medicine or traditional Chinese medicine when used in addition to allopathic medicine (National Center for Complementary and Alternative Medicine, 2012). The purpose of this review is to determine which integrative modalities are most effective for the reduction of pain and anxiety in children and adolescents being treated for cancer.
Many cross-sectional studies of the prevalence of integrative medicine use in children have been carried out around the world including Italy (Clerici, Veneroni, Giacon, Mariani, & Fossati-Bellani, 2009), Turkey (Genc, Senol, Turgay, & Kantar, 2009), Mexico (Gomez-Martinez, Tlacuilo-Parra, & Garibaldi-Covarrubias, 2007), Malaysia (Hamidah et al., 2009), and the United States (Post-White, Fitzgerald, Hageness, & Sencer, 2009). The most common integrative therapies are natural products (herbs, vitamins, and dietary supplement), used to alleviate symptoms or improve health (Tomlinson, Hesser, Ethier, & Sung, 2011).
Very few randomized clinical trials have been conducted using integrative modalities to reduce pain or anxiety in either adults or children. Most review articles on the topic of integrative medicine use in children discuss the prevalence of integrative use (Bishop et al., 2010; Post-White, 2006), not the effectiveness of particular integrative modality for symptom relief. Although there have been some reviews discussing pain or anxiety during painful procedures (Kleiber & Harper, 1999; Landier & Tse, 2010; Richardson, Smith, McCall, & Pilkington, 2006), no review has discussed integrative medicine use for pain and anxiety during the overall cancer trajectory.
Pain is a common symptom during cancer diagnosis and treatment and may come from painful procedures, disease progression, or impingement of nerves, tissues, or organs from tumors at any stage of the cancer progression (McGrath & Brown, 2005). There are many well-established tools to measure pain in children. Children as young as 3 years who can distinguish the concepts “less” and “more” are able to use visual analog scales such as the FACES scale developed by Wong and Baker in the 1980s (Baker, 2009). For younger children parent proxy-report is often used to measure pain and anxiety, and several well-validated rating scales have been developed for this purpose. A study of 164 children and adolescents in the United Kingdom found that 91% of children with end-stage cancer endured pain and 45% experienced anxiety (Goldman et al., 2006). This review will focus on the use of integrative medicine, that is, practices used together with conventional medicine.
Study Question
Integrative modalities in general seek to alleviate suffering through a decrease in noxious symptoms. Many modalities have been studied for symptom relief in children including hypnosis, acupuncture, massage, virtual reality, folk healing, prayer, and others (Doellman, 2003). The question this review seeks to answer is, “Which integrative modalities are most effective for reducing pain and anxiety in children and adolescents with cancer?”
Criteria for Including Studies for Review
Types of Participants
Studies were considered if they were conducted with children or adolescents, aged 1 to 18 years, at any point in the cancer trajectory from new diagnosis, to ongoing treatment, to long-term survivorship, or end of life.
Study Design
Studies were included that used any type of randomization, a control group, published in peer-reviewed journals, used any type of integrative modality except natural products (herbs, vitamins, supplements, and the like), and measured both pain and anxiety. Natural products were excluded because they are ingested and may interact with other therapies the child is receiving in unpredictable ways.
Outcome Measures
In view of the fact that the disease itself, the treatment, and long-term side effects of treatment may cause pain both acute and long term, pain is one of the main outcomes variables of interest. Children and adolescents may feel anxious about treatments, procedures, staying in the hospital, clinic visits, or recurrence. Studies were included for review if they measured both pain and anxiety as outcomes.
Search Strategies for Identification of Studies
A systematic literature search was conducted using PubMed, PsychInfo, CINAHL, Web of Science, and MedLine via Ovid databases with no date limitation. Several journals were then searched individually including Integrative Cancer Therapies, Journal of Evidence-Based Complementary & Alternative Medicine, and Supportive Care in Cancer. Finally, the reference lists for integrative and systematic review articles identified in the original search were examined to find relevant articles. The following key words were used: pain, anxiety, pediatric, child*, complementary, integrative, CAM, unconventional, nonconventional, cancer, oncology, and neoplasm. After removing duplicates, there were 164 articles, 74 of which reported research findings with the remainder either informational or review articles. Of the 74 research studies, 20 involved natural products (herbs, supplements, etc), 21 measured prevalence of integrative medicine use, and 8 discussed the symptoms of pain or anxiety but did not measure them. The remaining 25 articles that reported integrative intervention findings made up the final sample for full text review.
Method of Review
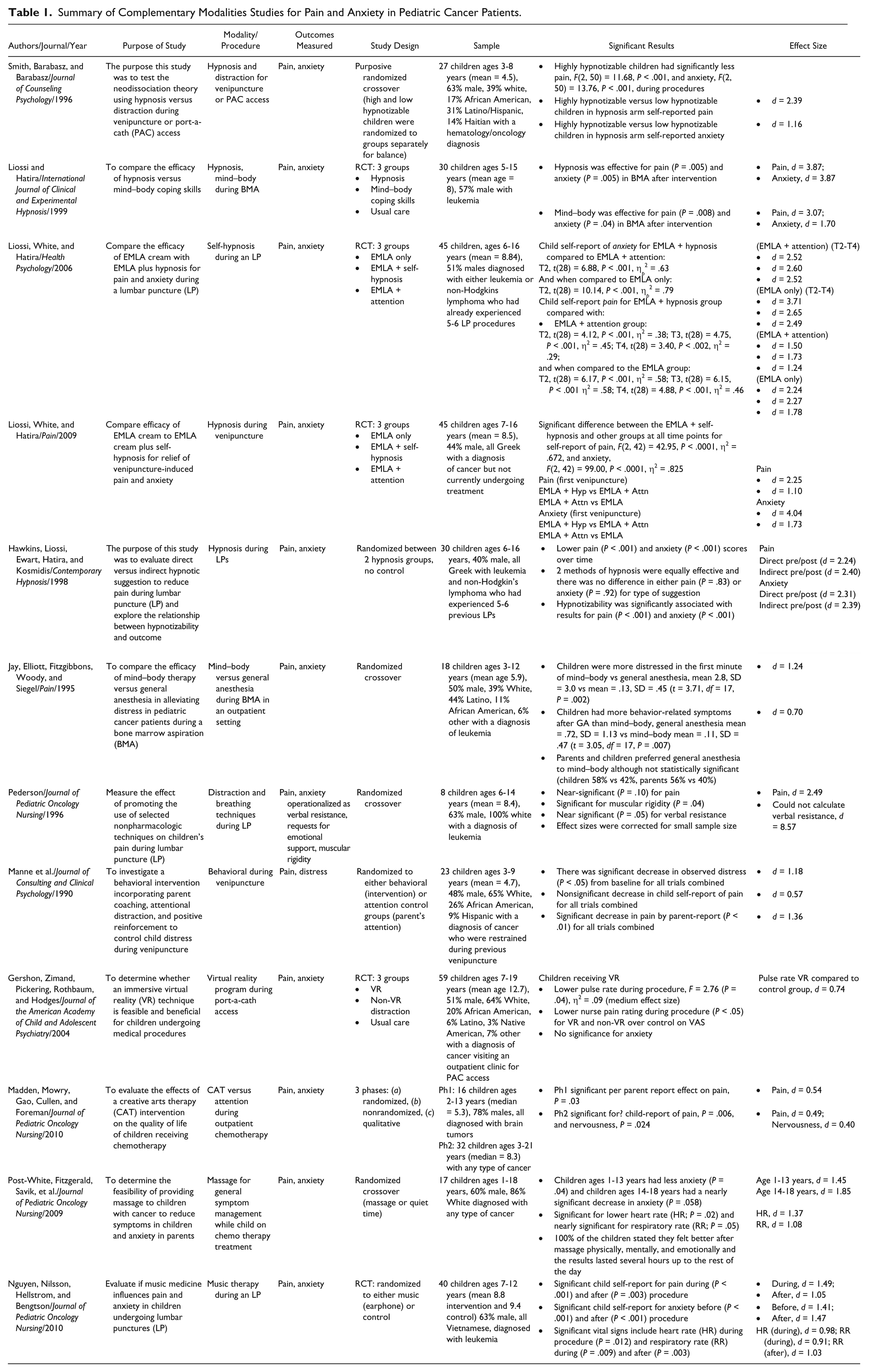
The 25 articles underwent full-text review using a systematic approach. Each article was carefully reviewed against the inclusion criteria. Thirteen studies were eliminated. The reasons for elimination included no randomization, no control group, or did not measure both pain and anxiety. Twelve studies met the review criteria and are included in the review (see Table 1).
Summary of Complementary Modalities Studies for Pain and Anxiety in Pediatric Cancer Patients.
Findings
All studies in this review had at least one statistically significant finding except for Pederson (1996), who used distraction and breathing techniques during a lumbar puncture. Effect sizes using Cohen’s d were calculated for each study based on data reported in the study. An Excel-based program (Wilson, 2001) was used when possible (Gershon et al., 2004; Hawkins et al., 1998; Jay et al., 1995; Liossi et al., 2006, 2009; Manne et al., 1990; Nguyen et al., 2010; Smith et al., 1996); however, we used hand calculations using z scores or p to z score conversions and the formula ES = r = Z/n1/2 if only P values were given (Liossi & Hatira, 1999; Madden et al., 2010; Pederson, 1996; Post-White, Fitzgerald, Savik, et al., 2009).
Study Design
All studies included in this review employed a form of randomization. Three studies used a randomized crossover design (Jay et al., 1995; Pederson, 1996; Post-White, Fitzgerald, Savik, et al., 2009) where the participants in the control group received attention. Two studies used randomization with the control group receiving attention from a volunteer (Madden et al., 2010; Manne et al., 1990). In one study, the control group had earphones but no music to blind the observers (Nguyen et al., 2010). One hypnosis study randomized between 2 treatment types: indirect versus direct suggestion with no control (Hawkins et al., 1998) and another purposefully randomized low- and high-hypnotizable children to achieve balanced groups (Smith et al., 1996). The remaining 4 studies used a 3-group design: the main intervention, a distraction intervention, and usual care control group (Gershon et al., 2004; Liossi & Hatira, 1999; Liossi et al., 2006, 2009). How subjects were randomized into groups was not detailed in 7 studies (Hawkins et al., 1998; Jay et al., 1995; Liossi & Hatira, 1999; Madden et al., 2010; Pederson, 1996; Post-White, Fitzgerald, Savik, et al., 2009; Smith et al., 1996); 1 study used an every other case randomization (Manne et al., 1990); 1 study used a table of random numbers (Liossi et al., 2006); 2 studies used computer-generated random numbers (Gershon et al., 2004; Liossi et al., 2009); and the final study used sealed, opaque envelopes (Nguyen et al., 2010).
Variables and Measures
All studies reviewed measured pain by child self-report for children ages 3 years and older in addition to either parent proxy report or other observer report. For children younger than 3 years, only proxy report was used. Table 2 summarizes the measures for each study.
Measures Used for Pain and Anxiety in Studies.
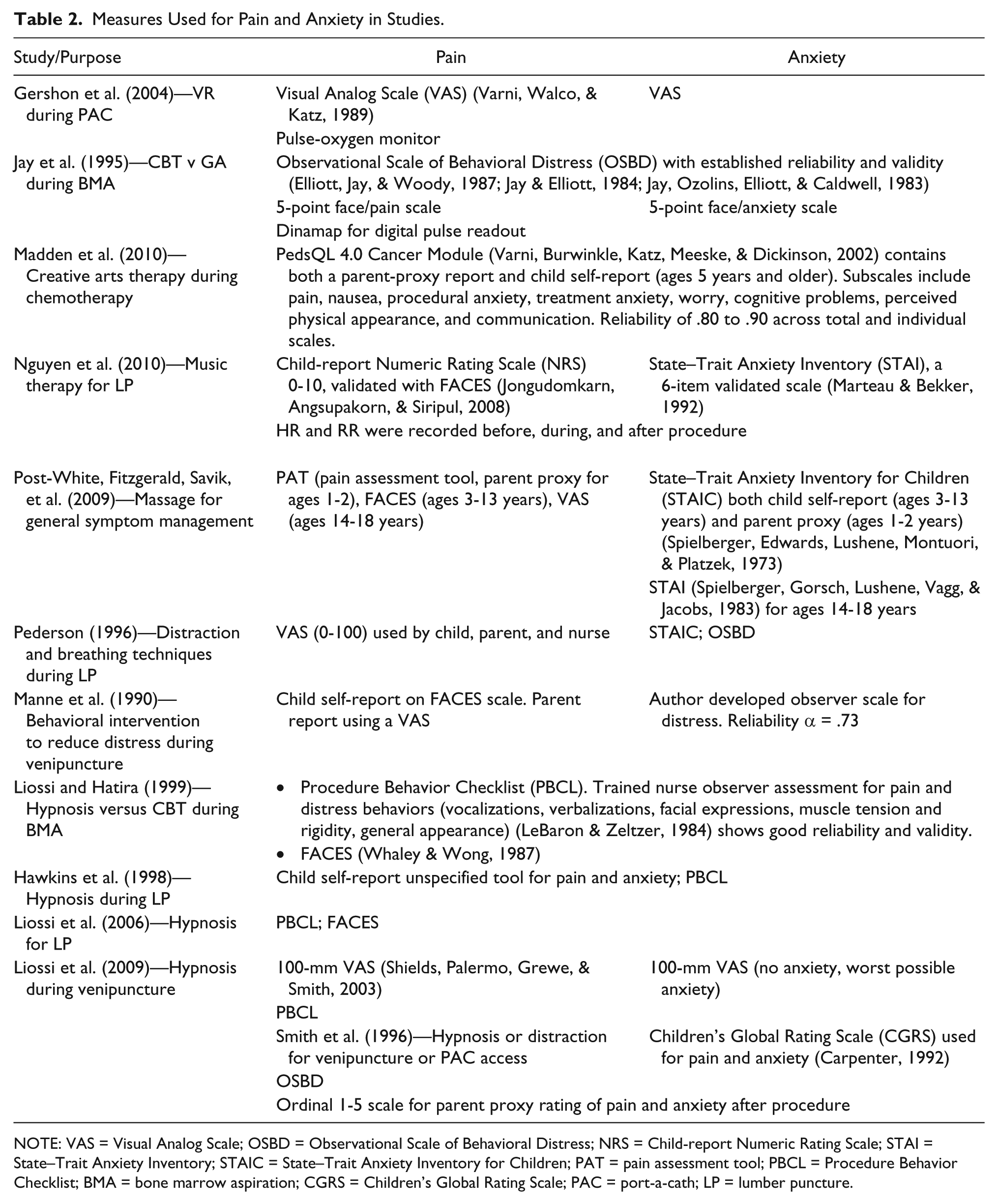
NOTE: VAS = Visual Analog Scale; OSBD = Observational Scale of Behavioral Distress; NRS = Child-report Numeric Rating Scale; STAI = State–Trait Anxiety Inventory; STAIC = State–Trait Anxiety Inventory for Children; PAT = pain assessment tool; PBCL = Procedure Behavior Checklist; BMA = bone marrow aspiration; CGRS = Children’s Global Rating Scale; PAC = port-a-cath; LP = lumber puncture.
Participants and Sample Size
There were a total of 358 children participating in the studies ranging from 1 to 19 years old. Combined mean age from 10 out of 12 studies that included data was 8.4 years old. Fifty-five percent of the participants were male. Three separate studies took place in Greece for a total of 120 Greek children (Hawkins et al., 1998; Liossi et al., 2006, 2009), and 1 study took place in Vietnam including 40 children (Nguyen et al., 2010). Of the studies that took place in the United States that mentioned race, a total of 160 children were 62% White, 15% African American, 14% Hispanic/Latino, 1% Native American, 2% Haitian, and 6% other (Gershon et al., 2004; Jay et al., 1995; Manne et al., 1990; Pederson, 1996; Post-White, Fitzgerald, Savik, et al., 2009; Smith et al., 1996).
Sample sizes ranged from 8 to 59 participants (mean = 29.8, standard deviation = 14.9). Many of the studies examined painful procedures such as lumbar punctures and bone marrow aspirations meaning that the majority of the subjects were diagnosed with either leukemia or lymphoma (Gershon et al., 2004; Hawkins et al., 1998; Jay et al., 1995; Liossi & Hatira, 1999; Nguyen et al., 2010; Pederson, 1996). The remaining study subjects had either brain tumors (Madden et al., 2010; Post-White, Fitzgerald, Savik, et al., 2009), rhabdomyosarcoma (Manne et al., 1990; Post-White, Fitzgerald, Savik, et al., 2009), Wilms tumor (Manne et al., 1990; Post-White, Fitzgerald, Savik, et al., 2009), Ewing sarcoma (Post-White, Fitzgerald, Savik, et al., 2009), nonspecified solid tumors (Smith et al., 1996), or nonspecified types of cancers (Liossi et al., 2009).
Comparison Groups and Outcomes
With the exception of studies that used different treatment modalities for comparison (Hawkins et al., 1998; Liossi et al., 2006, 2009; Smith et al., 1996), the remaining studies used usual care as the comparison group. All studies measured pain and some form of anxiety. Manne et al. (1990) measured distress during venipuncture whereas Pederson (1996) measured anxiety operationalized as verbal resistance, requests for emotional support, and muscular rigidity during a lumbar puncture (see the Measures section for further explanation of operationalization of anxiety).
Intervention Modalities
The effectiveness of integrative modalities was primarily studied during painful procedures common throughout cancer treatment including lumbar punctures (Hawkins et al., 1998; Liossi et al., 2006; Nguyen et al., 2010; Pederson, 1996), bone marrow aspiration (Jay et al., 1995; Liossi & Hatira, 1999), implanted port (or port-a-cath) access (Gershon et al., 2004; Smith et al., 1996), and venipuncture (Liossi et al., 2009; Manne et al., 1990; Smith et al., 1996). Post-White et al. explored massage therapy for general symptom management, whereas Madden et al. investigated creative arts therapy during chemotherapy infusions.
Hypnosis was used in 5 out of the 12 studies (Hawkins et al., 1998; Liossi & Hatira, 1999; Liossi et al., 2006, 2009; Smith et al., 1996). Mind–body methods (imagery, distraction, breathing techniques) were the primary focus of 3 studies (Jay et al., 1995; Manne et al., 1990; Pederson, 1996) and were used as comparison groups for 2 of the hypnosis studies (Liossi & Hatira, 1999; Smith et al., 1996). Other modalities included a virtual reality program (Gershon et al., 2004), creative arts (Madden et al., 2010), massage (Post-White, Fitzgerald, Savik, et al., 2009), and music (Nguyen et al., 2010).
Hypnosis
Five studies used hypnosis to help children with pain and anxiety during procedures ranging from venipuncture to lumbar puncture and bone marrow aspiration. Hawkins et al. (2008) evaluated the effects of direct versus indirect hypnotic suggestion and the effectiveness of hypnotizability for children undergoing LPs. Thirty children ages 6 to 16 years were randomly assigned to either the direct or indirect suggestion groups. Both methods of suggestion were equally effective for decreased pain (P < .001) and anxiety (P < .001) over time and there was no difference in either pain (P = .83) or anxiety (P = .92) for type of suggestion. Hypnotizability was significantly associated with results for decreased pain (P < .001) and anxiety (P < .001).
Smith et al. (1996) tested 27 children ages 3 to 8 years for hypnotizability then stratified to achieve a balance of low- and high-hypnotizable children in each group. Children were tested for hypnotizability by staff not participating in other areas of the study so medical personnel and observers were blind to hypnotizability. The study used a crossover design so all children participated in both the hypnosis and distraction interventions. Highly hypnotizable children had significantly less pain (P < .001) and anxiety (P < .001) during venipuncture or implantable port access than low hypnotizable children during the procedure. When highly hypnotizable children were in the hypnosis intervention effect size for child self-report of decreased pain was very large (d = 2.39) as was child self-report of decreased anxiety (d = 1.16).
Three studies used a 3-group randomized control group design to test effectiveness of hypnosis for pain and anxiety during venipuncture (Liossi et al., 2009), LP (Liossi et al., 2006), and bone marrow aspiration (BMA; Liossi & Hatira, 1999). Liossi and Hatira (1999) utilized 3 groups: hypnosis, mind–body techniques, and usual care with 30 children ages 5 to 15 years with leukemia during BMA. Hypnosis was effective for decreased pain (P = .005, d = 3.87) and anxiety (P = .005, d = 3.87) after BMA compared with mind–body and usual care, mind–body was effective for decreased pain (P = .008, d = 3.07) and anxiety (P = .04, d = 1.70) after BMA compared with usual care.
Eutectic Mixture of Local Anesthetics (EMLA) cream is a common topical anesthetic cream used with children before procedures and is often considered usual care. Liossi et al. (2006) used 3 groups (EMLA only, EMLA with attention, and EMLA with hypnosis) to test the effectiveness of EMLA cream plus hypnosis on pain and anxiety in 45 children ages 6 to 16 years who had already experienced at least 5 LP procedures compared with EMLA cream plus attention and EMLA cream only. For the EMLA plus hypnosis group there was a significant effect for child self-report of decreased anxiety when compared with the EMLA only group (T2, P < .001, d = 3.71) and when compared with the EMLA plus attention group (T2, P < .001, d = 2.52). There was also a significant effect on child self-report of less pain in the EMLA plus hypnosis group when compared with the EMLA plus attention group at each time point (time T2, P < .001, d = 1.50) and when compared with the EMLA only group at each time point (time T2, P < .001, d = 2.24).
Liossi et al. (2009) used the same procedure as 2006 above to explore the effect of EMLA plus hypnosis, EMLA plus attention, and EMLA only for pain and anxiety during venipuncture. Study subjects were 45 children ages 7 to 16 years who had a cancer diagnosis but were not currently undergoing treatment. There was a significant effect for EMLA plus hypnosis when compared with both other groups at each time point for child self-report of decreased pain, F(2, 42) = 42.95, P < .0001, η2 = .672, and child self-report of decreased anxiety, F(2, 42) = 99.00, P < .0001, η2 = .825, both very large effect sizes. When comparing ELMA plus hypnosis to EMLA plus attention for child self-report of less pain the effect size was d = 2.25. When comparing ELMA plus attention to EMLA only for child self-report of less pain the effect size was d = 1.10. The same comparisons for decreased anxiety yield effect sizes of d = 4.04 and d = 1.73, respectively.
Mind–Body Techniques
Three studies used some type of mind–body intervention to help children cope with bone marrow aspiration (Jay et al., 1995), lumbar puncture (Pederson, 1996), and venipuncture (Manne et al., 1990). Mind–body techniques include breathing exercises, distraction (such as using a party blower or blowing bubbles), reward incentive, practicing positive coping behavior, coaching by the parent, relaxation techniques, and the like. Jay et al. (1995) used mind–body techniques compared with general anesthesia for a bone marrow aspiration in 18 children ages 3 to 12 years. Children experienced more distress (anxiety) during the first minute when using mind–body techniques (P = .002, d = 1.24) but more negative behavior-related symptoms after general anesthesia when compared with mind–body (P = .007, d = 0.70). However, both children (58% vs 42%) and parents (65% vs 40%) preferred general anesthesia over mind–body techniques (a nonsignificant result).
Pederson (1996) used distraction and breathing techniques during a lumbar puncture procedure in a sample of 8 children ages 6 to 14 years. Distraction techniques included blowing bubbles, pop-up books, plastic wands filled with sparkles, and foam puzzles. Child self-report was not significant for less pain (P = .10) but did have a very large effect size, d = 2.49 (corrected for small sample size). In observer report for anxiety, there was a significant result for less muscular rigidity (P = .04) (effect size could not be calculated because of small sample size) and a near significant result for less verbal resistance (P = .05) with a very large effect size, d = 8.57 (corrected for small sample size).
Manne et al. (1990) studied the use of attention distraction, paced breathing, and positive reinforcement versus parental attention (no intervention) with 23 children ages 3 to 9 years who had previously been observed being physically restrained during a venipuncture. There was a significant decrease in observed distress for the intervention group (P < .05, d = 1.18), a significant decrease in pain by parent report (P < .01, d = 1.36), and a nonsignificant child self-report for decreased pain that still achieved a medium effect size (d = 0.57).
Virtual Reality
One study (Gershon et al., 2004) explored the effect of a virtual reality (VR) program, a non-VR video game distraction, and usual care on pain and anxiety during implanted port access in 59 children ages 7 to 19 years. There was no significant effect for child self-report of pain or anxiety but nurses rated pain lower for VR and non-VR over control (P < .05) and pulse oximeter readings recorded lower pulse rate during implantable port access for VR group (P < .05). Effect size for pulse rate was d = 0.74, a large effect size.
Creative Arts Therapy
One study used creative arts therapy (CAT), which can include dance/movement therapy, music therapy, and art therapy and involves interaction with a trained therapist. Madden et al. (2010) used CAT to evaluate changes in quality of life including pain and anxiety for children ages 2 to 21 years during chemotherapy treatment with a cancer diagnosis. Phase 1 of the study was a randomized control trial of 16 children ages 2 through 13 years with brain cancer who received 6 one-hour CAT sessions (2 sessions each of dance/movement, music, and art therapies). Phase 1 had a significant effect on decreased pain (P = .03) per parent report. Phase 2 was a nonrandomized trial of children ages 3 to 21 years receiving chemotherapy with any type of cancer diagnosis. During this phase the children received group 1-hour sessions consisting of dance/movement, music, or art. This phase was significant for child self-report of decreased pain (P = .006).
Massage
In a study of 17 children ages 1 to 18 that were undergoing treatment for cancer, Post-White, Fitzgerald, Savik, et al. (2009) found that all of the children felt better after the massage, physically, mentally, and emotionally, and the results lasted from several hours up to the remainder of the day. Children 1 to 13 years had less anxiety (P = .04, d = 1.45) and children 14 to 18 years had a nearly significant decrease in anxiety (P = .058) while still achieving a large effect size (d = 1.85). For all children combined, there was a significant finding for lower heart rate (P = .02, d = 1.37) and nearly significant for lower respiratory rate (P = .05, d = 1.08) both of which indicate less pain and anxiety.
Music
Nguyen et al. (2010) studied the use of music on pain and anxiety for children with leukemia undergoing lumbar punctures (LP). The children aged 7 to 12 years were randomized into intervention and control groups. To blind the observer to group, control group children wore identical headphones but had no music. The study found significant effects on child self-report for decreased pain during (P < .001, d = 1.49) and after the LP (P = .003, d = 1.05). There were significant effects on child self-report of anxiety before (P < .001, d = 1.41) and after (P < .001, d = 1.05) the procedure. Reduction in vital signs (an indicator of decreased pain and anxiety) during the procedure including decreased heart rate during the LP (P = .012, d = 0.98) and decreased respiratory rate during (P = .009, d = 0.91) and after (P = .003, d = 1.03) the LP.
Discussion
While the heterogeneous modalities and methodologies of the included studies prohibited conducting a formal meta-analysis, collectively they provide encouraging evidence for the effectiveness of integrative approaches for managing pain and anxiety in children with cancer. With the exception of the virtual reality study, which had a medium effect size, the remaining studies in this review achieved a large to very large effect size. These results validate the effectiveness of integrative modalities for children with cancer in coping with pain and anxiety during cancer treatment and the painful procedures that are a part of treatment. In addition, the effectiveness and variety of integrative modalities highlighted in this review show that there are many ways to benefit children and decrease suffering during cancer treatment. Furthermore, these studies demonstrate that individual children will respond to some but not all modalities.
The overall design quality of the studies reviewed was very good although some study designs stand out as excellent while others suffered design flaws. The recent hypnosis studies by the Liossi team using 3-group RCT design examining the effectiveness of hypnosis over attention or usual care reached the projected sample size of N = 45 with a power of 0.9 and a large effect size (Liossi et al., 2006, 2009) and an earlier 3 group RCT (N = 30) also used standardized procedures although the authors did not mention the power of the study (Liossi & Hatira, 1999). Pederson (1996) had difficulty recruiting subjects because of clinic changes in mid-study and personnel issues resulting in decreased power of statistical analysis but an additional design weakness included timing of assessments in relation to sedation during procedures. Measures were problematic in the massage study (Post-White, Fitzgerald, Savik, et al., 2009) as not all tools were validated for the age group (the STAI has not been validated for children younger than 8 years or for proxy report) or for the outcome variable (the study used a FACES-type scale to measure nausea in children younger than 9 years who did not understand a VAS for this purpose); a change in inclusion criteria might have been advisable.
With the exception of massage, the remaining studies used some sort of distraction to help children cope with pain and anxiety. Distraction has many forms and is a way to focus the mind on something pleasant (or even fun) and not on the suffering at hand. Virtual reality is a way to immerse the mind more completely than just playing a video game. This modality has been studied with small samples of children since its beginning more than 20 years ago. An earlier pilot study found that using a VR program made children’s chemotherapy experience “better” than receiving chemotherapy without VR (Schneider & Workman, 2000). It seems worthwhile to study VR more extensively for children and adolescents during treatment. It may be that using VR for implantable port access is too short of a time frame to be as effective as using VR for chemotherapy treatment.
By the time children are 18 to 24 months old, they have developed the cognitive ability to use symbols (eg, using a block as a truck) resulting in the increasing use of imagination and pretend play (Lillard, 2002). By preschool age, they are able to enjoy and participate in stories because of their ability to remember and follow the story line. This ability also makes children of this age appropriate for distraction techniques such as guided imagery, hypnosis, and using imagination to participate with an adult in mutual storytelling. Children of preschool through early school age also want to please their parents so techniques such as coaching and encouragement may be helpful. Toddlers from about 18 to 36 months are able to enjoy colorful toys such as glitter wands, pinwheels, party blowers, or blowing bubbles. The studies in this review used age-appropriate distraction techniques. There was variability in the distraction interventions that were investigated across studies. In the Jay et al. (1995) study, the mind–body intervention consisted of a 45-minute film that showed the child how to do breathing exercises, modeled positive coping strategies, and talked about imagery strategies such as imagining one is at Disneyland or eating pizza. The children in this study ranged in age from 3 to 12 years. It is difficult to find a “one size fits all” intervention for this range of developmental levels; however, it seems unlikely that a 3 year old would be able to stay attentive to an instructional film for this period of time although a therapist did give guidance during the BMA on coping strategies. Pederson (1996) also used a 22-minute videotape to teach strategies to children. The child was then able to choose a distraction material for use during the next BMA. A research support person went into the BMA to help support the parent in helping their child use the coping techniques. In the Manne et al. (1990) study, child–parent dyads were given personal instruction in the use of paced breathing, positive reinforcement, and distraction—in this case in the use of a party blower. The child could “win” stickers by using the party blower and holding still during venipuncture. Only children who had been observed needing physical restraint during a previous venipuncture were recruited to the study. The short, personal instruction seemed to work very well for this age group (ages 3 to 9 a therapist did give guidance during the BMA on coping strategies.) since the effect size was very large. In the Nguyen et al. study (2010), music was used as a distraction during an LP. Children were able to choose the type of music they would like to listen to. The large and very large effect sizes for child self-report of both pain and anxiety during the music intervention shows very good evidence for the effectiveness of this simple intervention.
Culture plays a role in children’s expression of pain and anxiety. This adaptation to culture begins in infancy as children are socialized into the culture of their environment. In Western cultures that value autonomy and individualism, assertiveness in social skills and expression of pain is normal although acceptability varies depending on age and gender (Chen & French, 2008). In collective societies such as East Asian, Latin American, or Israel, individuals are encouraged and guided from infancy to demonstrate self-control including expressions of pain or anxiety (Chen & French, 2008; Raval & Martini, 2009).
The studies reviewed here suggest that there are many integrative modalities that may be used with good effect to decrease pain and anxiety in children both during painful procedures and during general treatment for cancer. Many types of distraction techniques including hypnosis, mind–body, listening to music, and virtual reality may help decrease pain and anxiety and thereby suffering in children undergoing procedures that are part of cancer treatment. Other modalities such as massage and creative art therapy may decrease pain and anxiety associated with overall treatment while increasing mood and a feeling of well-being. Many of these techniques are easy to learn and all are within the scope of nursing practice. Nurses may use these techniques with children and teach them to parents to help support children through painful procedures and cancer treatment.
Limitations
While efforts were made to decrease bias as much as possible, the results of the review may be inflated by several factors. First, in order to increase the potential for significant findings, only studies that used randomization were included. This limits the studies published from other countries which tend to conduct open, nonrandomized designs. Only published peer-reviewed journal studies were included, no dissertations or conference abstracts were considered. Finally, because of the nature of research in childhood cancer and integrative medicine, sample sizes of even the more rigorous studies were small (≤59 participants), which may inflate results despite the use of small sample size corrections in the Cohen’s d statistic in the case of very small sample sizes.
Conclusion
There is good evidence that complementary modalities, also known as integrative medicine, can help children undergoing cancer treatment in general and in painful procedures in particular. The modalities in this review including virtual reality, various mind–body techniques, creative arts therapy, listening to music, massage, and hypnosis all had good effect sizes and significant results for pain and anxiety. Although these studies universally employed small sample sizes, all of the studies utilized some type of randomization and many used the gold standard randomized control design. Given that mind–body techniques and hypnosis showed good effect sizes for decreased pain and anxiety in several studies examining diverse painful procedures, there is ample evidence to recommend the use of these techniques during the painful procedures that are a part of childhood cancer treatments. They are both noninvasive and give the child a sense of control over their pain during the procedure. Creative art therapy seems like a natural modality for children with its combination of creativity and expression of feelings. However, more studies need to be done with this modality and population. Massage is another modality that has not been well studied with children in general or with cancer patients in particular. More research is needed with massage and touch therapies in order to be able to recommend their use for pain and anxiety in pediatric cancer patients.
Based on this review, further research is needed in integrative modalities. Larger sample sizes, perhaps through multisite studies, are needed in order to recommend the modalities reviewed in this study and the many other possibilities such as meditation, aromatherapy, yoga, acupuncture, Reiki, and other integrative therapies that may have benefit for this population. The clinical implications of the use of integrative modalities for children undergoing cancer treatment include empowering children and their families to gain control over their pain and anxiety, and to increase well-being. Many of these modalities are within the scope of practice for nursing. Although some nurses may view this as another task, many nurses will welcome adding a simple tool to their toolbox that enables them to help children in their care.
 Continuing Education Credit
Continuing Education Credit
The Journal of Pediatric Oncology Nursing is pleased to offer the opportunity to earn pediatric hematology/oncology nursing continuing education credit for this article online. Go to www.aphon.org and select “Continuing Education.” There you can read the article again or go directly to the posttest assessment. The cost is $15 for each article. You will be asked for a credit card or online payment service number.
The posttest consists of 11 questions based on the article, plus several assessment questions (e.g. how long did it take you to read the article and complete the posttest?). A passing score is 8 out of 11 questions correct on the posttest and completion of the assessment questions yields one hour of continuing education in pediatric hematology/oncology nursing for each article.
The Association of Pediatric Hematology/Oncology Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Footnotes
Acknowledgements
The author would like to thank Janet Stewart, PhD, RN, for her early critique of the article and her mentor, Susan M. Cohen, DSN, APRN, FAAN, for her encouragement and support.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by an NINR T32 Training Grant (T32NR011972) in Cancer Survivorship.