
Abstract
It is important for the responsive and effective treatment of pediatric cancer patients that functional disability is successfully measured, but no measures of functional disability have been validated for use with Arabic-speaking children and adolescents. The purpose of this study was to examine the psychometric characteristics of the first Arabic translation of the Functional Disability Inventory (FDI). A methodological study limited to the secondary analysis of functional disability data on 62 pediatric patients in Lebanon using the rating scale model and WINSTEPS Rasch analysis software was used. Disordered responses to 4 FDI times suggest that the Arabic translation of the rating scale categories might need revision or supplementation with a visual analogue scale. The dimensionality of the FDI needs further exploration because principal component analyses of residuals suggested the presence of secondary and possibly higher order dimensions. Additional FDI items are needed to improve targeting if low levels of functional disability are demonstrated to be clinically important for patient assessment and pain management. The FDI-A is suitable for clinical assessment and for monitoring the outcomes of pain management in Lebanese pediatric cancer patients. Our findings support the construct validity of the FDI-A and acceptable reliability for the 15-item scale, Cronbach α .93 and .85 for 4 of the item subsets we examined. Rating scale categories and the dimensionality of the FDI-A require further examination. The clinical relevance of distinctions between levels of functional disability in children and adolescents with cancer pain remains to be established.
Introduction
Researchers who want to investigate functional disability in new settings can choose between 2 broad strategies: they can develop new measures responsive to local needs or they can adapt existing measures to local requirements. Developing new measures is time consuming, costly, and can duplicate effort unnecessarily. In countries where funds for research are scarce, it is cost-effective to adopt the second strategy. However, when measures have been developed in English for use in a Western country, investigators in Arabic-speaking countries face the challenge of determining appropriateness. We faced this challenge as we worked toward validating a scale used by the first author to measure functional disability among pediatric cancer patients in Lebanon. We are aware from our different cultural backgrounds (Lebanese and Australian) that meanings of illness vary among languages, religions, and cultures. As a result, we resisted the temptation to rely on estimates of Cronbach’s α alone to determine the validity and reliability of the first Arabic translation of Walker and Greene’s (1991) Functional Disability Inventory (FDI). We conducted a Rasch analysis of an Arabic version of the FDI, the Functional Disability Inventory–Arabic (FDI-A), translated by the first author for use in her study of the relationship between pediatric cancer pain and functional disability in Lebanon (Madi, 2012).
Background
Rasch analysis examines how well items in a test or rating scale are useful for measuring an assumed 1-dimensional latent variable (Rasch, 1960, 1980). Rasch fit statistics indicate how well respondents and their responses fit the response pattern predicted by the Rasch model. Infit and outfit statistics are calculated as χ2 values that range from zero to infinity. Infit and outfit values for an item that perfectly matches the Rasch model have mean square values (MNSQs) of 1. Items with MNSQ values greater than 1 overfit the model because they lack precision. Items with values less than 1 are too predictable and may not contribute to successful measurement. An MNSQ of 1.2 indicates that there is 20% more randomness in the data than the model expects. An MNSQ of 0.5 indicates that there is a 50% deficiency in model predicted randomness (Linacre, 2012a). Outfit and infit MNSQs in the range 0.77 to 1.3 are acceptable for most purposes (Adams & Khoo, 1993; McNamara, 1996). An alternative rule of thumb is to accept MNSQ values in the range 0.6 to 1.4 (Frantom, Green, & Hoffman, 2002). For exploratory analysis a range of 0.5 to 1.5 is acceptable (Linacre, 2002). For this exploratory study, we regarded an item as too imprecise if outfit MNSQ values were >1.4. We regarded an item as overly predictable if outfit MNSQ and infit MNSQ were <0.5. We examined MNSQ values corrected for sample size (Smith, Schumacker, & Bush, 1998) as well and accepted outfit MNSQ values in the range 1.76 to 0.24 and infit MNSQ values in the range 1.25 to 0.75.
In Rasch analysis the dimensionality of rating scales and subscales can be checked by principal component analysis of residuals (Wright, 1996). The Rasch measurement model is the dimension of first comparison. Second and subsequent dimensions with eigenvalues greater than 2 suggest second and higher order dimensions and imply departures from unidimensionality. What matters in the analysis of second and subsequent dimensions is not the value of item loadings themselves but whether there are patterns of loading that are interpretable as response patterns distinct from the Rasch dimension (Linacre, 2009).
The Primary Study
The experience of pain in the Lebanese pediatric oncology population had not been investigated until the study undertaken by the first author in 2010. The purpose of her study was to identify the characteristics of cancer pain among children admitted to the Children’s Cancer Center of Lebanon (CCCL) in Beirut (Madi, 2012). A related aim was to explore the psychometric characteristics of the FDI-A. The findings of the primary study are reported elsewhere (Madi, 2012).
Secondary Analysis
The specific objectives of our Rasch analysis of the CCCL data were to
Identify FDI-A items that can be deleted or need modification
Determine whether the FDI-A is suitable for assessing functional disability among Lebanese pediatric cancer patients
Examine the psychometric characteristics of subsets of FDI-A items
Discover what further studies are required to further validate use of the FDI-A and FDI-A item subsets
Design
The initial study was designed as a cross-sectional survey of pediatric cancer patients. Participants were recruited from the CCCL in Beirut. Criteria for inclusion were the following: Lebanese children aged 8 to <18 years, admitted to an inpatient or outpatient department, diagnosed with any type of cancer for more than 1 month, admitted for active treatment or monitoring. Patients requiring pediatric intensive care, those with a preexisting mental disorder, or a hearing and/or speech problem, and those who were terminally ill were excluded. The first author interviewed the participants in Arabic at the CCCL.
Sample
The participants ranged in age from 8 to 17 years, with a mean age of 12.3 years (standard deviation [SD] = 2.9). They were evenly distributed between school age and adolescence. Thirty-two children were boys (51.6%) and 29 were girls (46.8%), with 34 (54.8%) living in urban areas and 28 (45.2%) in rural areas. Forty-seven children (75.8%) were recruited from outpatient departments and 15 children (24.2%) from the inpatient department. The reasons for CCCL admission were chemotherapy (48.4%), routine monitoring (45.2%), procedures (21.0%), and fever related to infection or to febrile neutropenia (9.7%).
Instrument
The FDI (Walker & Greene, 1991) is the most commonly used tool to assess functional disability associated with pain in children (Eccleston, Jordan, & Crombez, 2006; Hermann, Hohmeister, Zohsel, Tuttas, & Flor, 2008). It has been validated for the assessment of pain-related functional disability in children aged between 8 and 17 years (Eccleston, Crombez, Scotford, Clinch, & Connell, 2004; Eccleston, Malleson, Clinch, Connell, & Sourbut, 2003; Kashikar-Zuck, Vaught, Goldschneider, Graham, & Miller, 2002; Lynch-Jordan et al., 2010; Reid, McGrath, & Langa, 2005). It consists of 15 activities that measure perceptions of functional limitations during the past 2 weeks (Table 1). The 15 daily activities are in the domains of school, home, recreation, and social interaction. Examples of activities include walking to the bathroom, being at school all day, and doing homework. Children rate items on a 5-point scale ranging from 0 = no trouble to 4 = impossible. Total scores are computed by summing the ratings for each item. The psychometric properties of the FDI have been well-established, with coefficient α’s of .88 to .95 in different populations (Claar & Walker, 2006; Lynch-Jordan et al., 2010; Palermo et al., 2008; Reid, Lang, & McGrath, 1997; Vervoort, Goubert, Eccleston, Bijttebier, & Crombez, 2006). The FDI is available in child and parent versions. The FDI has been shown to be appropriate for use with diverse pediatric pain populations (Palermo, 2000), for example, children who have sickle cell disease (Peterson & Palermo, 2004), juvenile idiopathic arthritis (Reid et al., 2005), recurrent abdominal pain (Robins, Smith, & Proujansky, 2002; Walker, Smith, Garber, & Claar, 2005), headaches (Long, Krishnamurthy, & Palermo, 2008; Palermo & Kiska, 2005), cerebral palsy (Engel, Jensen & Schwartz, 2006), and adolescents with cancer (Ameringer, 2010). The FDI has been recommended for use in clinical trials that investigate physical functioning in children and adolescents with acute, chronic, and recurrent pain (McGrath et al., 2008).
15 FDI-A Items and Item Subsets.
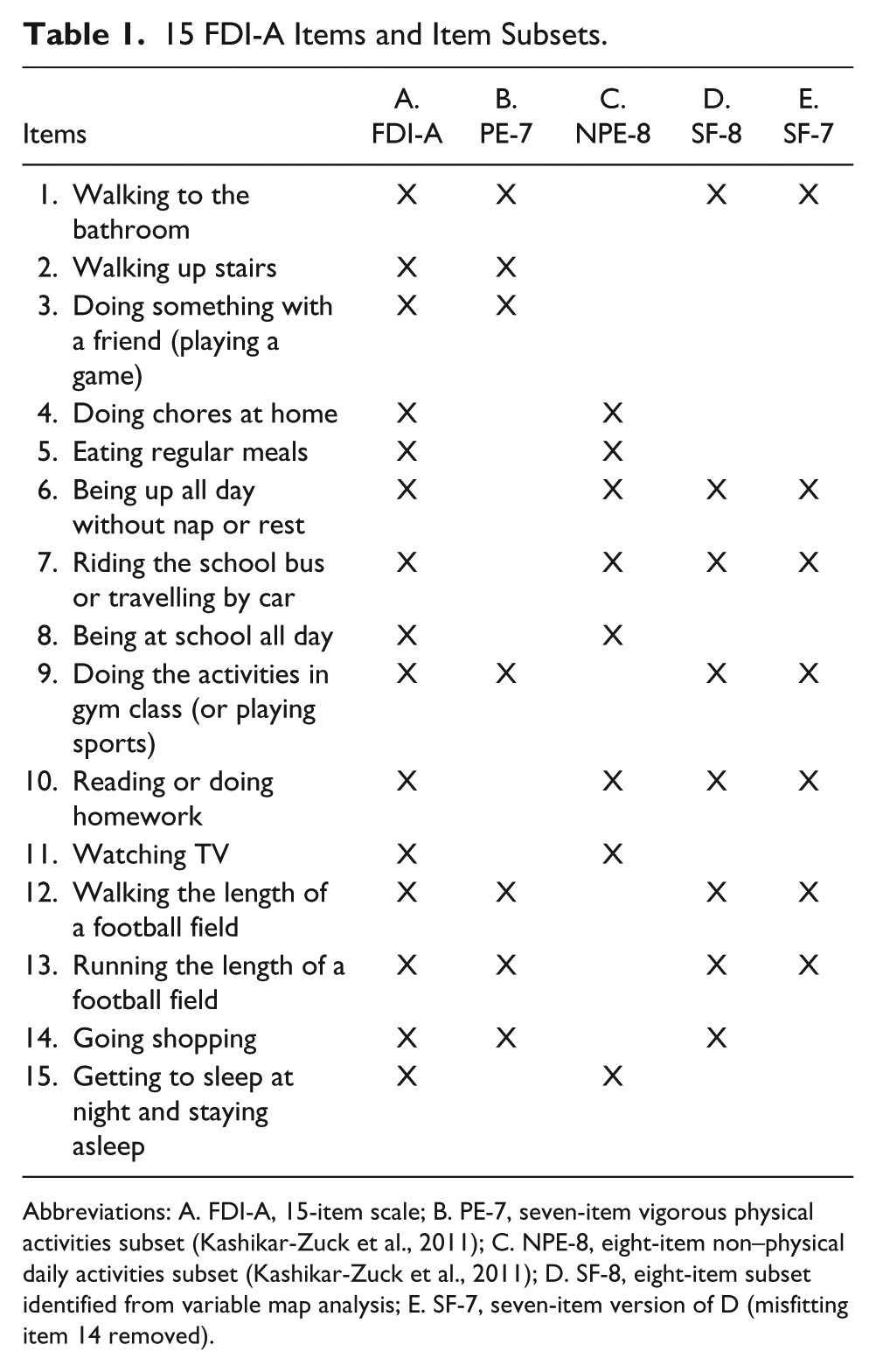
Abbreviations: A. FDI-A, 15-item scale; B. PE-7, seven-item vigorous physical activities subset (Kashikar-Zuck et al., 2011); C. NPE-8, eight-item non–physical daily activities subset (Kashikar-Zuck et al., 2011); D. SF-8, eight-item subset identified from variable map analysis; E. SF-7, seven-item version of D (misfitting item 14 removed).
Translation and Adaptation of the FDI
We used the World Health Organization (WHO) process for translation and adaptation of instruments (WHO, 2010) to prepare the FDI-A. Forward–backward translation from English to Arabic and back to English was used to identify inaccuracies in translation. The purpose of this process was to generate an Arabic version of the FDI equivalent conceptually to the original version. A draft version of the FDI-A was sent to a panel of bilingual (English/Arabic) experts that included a group of specialists in the management of cancer pain in the pediatric population. The panel evaluated the draft FDA-A for clarity and cultural appropriateness. In addition to the draft FDI-A, the panel reviewed the English version of the FDI, the forward-translated version (English to Arabic), and the back-translated version (Arabic to English). The panel examined the suitability of the FDI-A for use in Lebanon. The panel commented positively on the clarity of the translated FDI items reviewed determined that the FDI-A was culturally appropriate. Since the panel recommended no changes, a pilot study was conducted with 10 pediatric patients to assess the intelligibility of the FDI items. No changes were necessary, so the first author proceeded to implement the study.
Data
The secondary analysis was conducted on functional disability data for 62 children and adolescents treated at CCCL inpatient and outpatient departments. The data were collected for the primary study. The data set was de-identified by the first author prior to secondary analysis by the second author.
Ethical Considerations
The School of Nursing, Midwifery, and Social Work Ethics Committee at the University of Manchester and the Social and Behavioral Sciences Institutional Review Board at the American University of Beirut (SBS-IRB) approved the primary study. Administrative approval for the primary study was obtained from the medical directors at AUBMC and the CCCL. The SBS-IRB approved an application for exemption from IRB oversight for the secondary analysis of the de-identified functional disability data.
Data Analysis
We used the rating scale model to conduct separate Rasch analysis on the 15-item version of the FDI-A and 4 author-created activity subsets using WINSTEPS 3.75 (Linacre, 2012b; Table 2). We examined response ordering for the 15-item scale to find out whether response categories had been interpreted and used correctly. Then we examined the dimensionality of the scale and local dependence to determine whether responses to individual items had overly influenced responses to other items. Interitem standardized correlations of ≥.7 were taken as evidence of high local dependence indicating ~50 common residual variance between items.
Comparative Analysis FDI-A and Item Subsets.
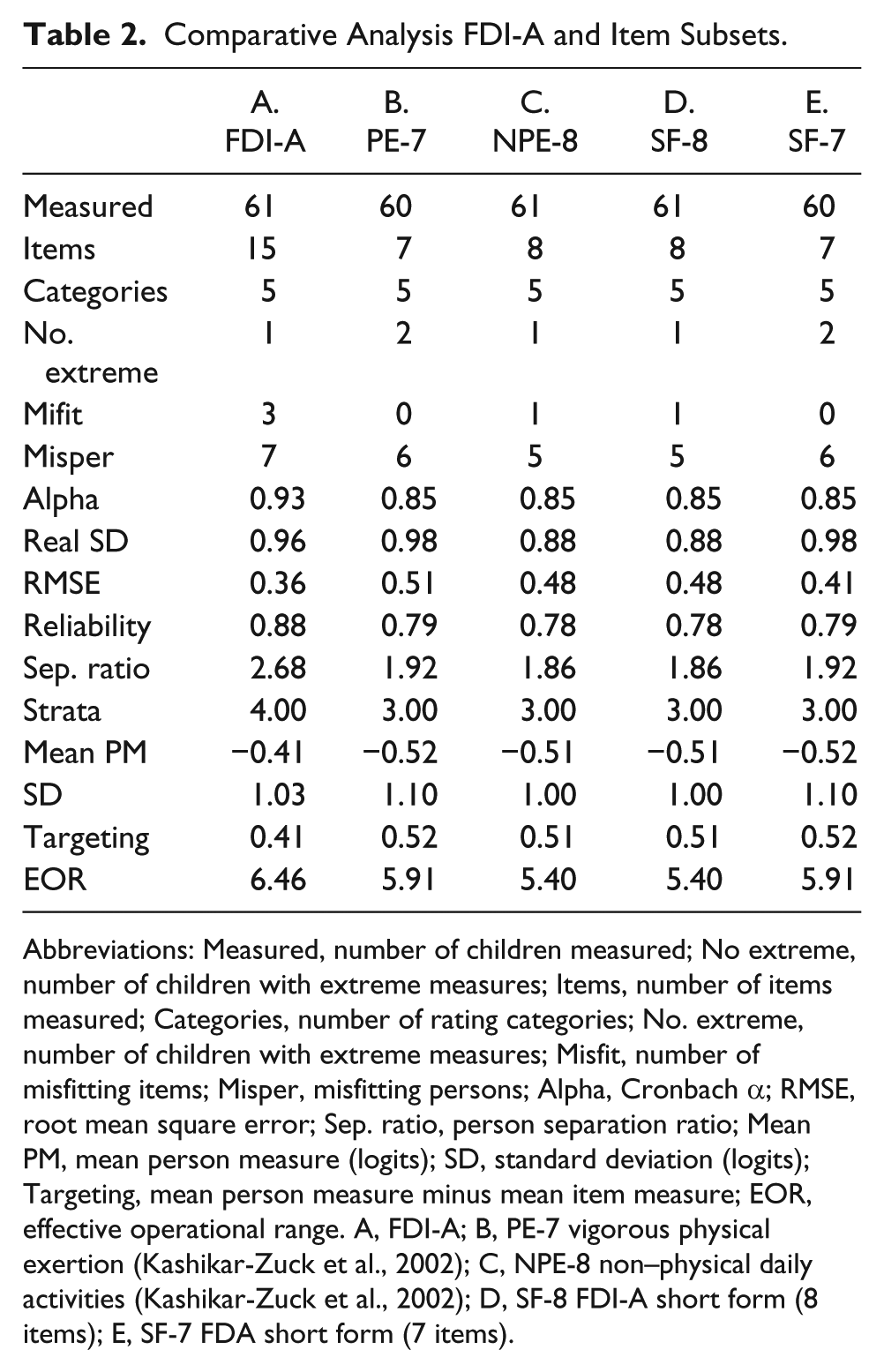
Abbreviations: Measured, number of children measured; No extreme, number of children with extreme measures; Items, number of items measured; Categories, number of rating categories; No. extreme, number of children with extreme measures; Misfit, number of misfitting items; Misper, misfitting persons; Alpha, Cronbach α; RMSE, root mean square error; Sep. ratio, person separation ratio; Mean PM, mean person measure (logits); SD, standard deviation (logits); Targeting, mean person measure minus mean item measure; EOR, effective operational range. A, FDI-A; B, PE-7 vigorous physical exertion (Kashikar-Zuck et al., 2002); C, NPE-8 non–physical daily activities (Kashikar-Zuck et al., 2002); D, SF-8 FDI-A short form (8 items); E, SF-7 FDA short form (7 items).
We then examined targeting to assess the match between the ability of our sample to report degrees of functional disability and the difficulty for them of endorsing rating scale categories.
Our next step was to examine MNSQ values for the 2 fit statistics provided by Rasch analysis. The outlier-sensitive fit statistic (outfit MNSQ) indicates the discrepancy between observed and Rasch expected responses, irrespective of how far the response is from the person’s ability level. The inlier-pattern sensitive statistic (infit MNSQ) indicates an unexpected response near to the person’s level of ability. In this study, we regarded an item as too imprecise if outfit MNSQ values were >1.4. We regarded an item as overly predictable if outfit MNSQ and infit MNSQ were <0.5. We examined as well MNSQ values corrected for sample size (Smith et al., 1998) outfit MNSQ in the range 1.76 to 0.24 and infit MNSQ in the range 1.25 to 0.75.
We continued our analysis of the full scale by examining person separation indices and item reliability coefficients to assess the precision of the FDI-A. We looked for person separation indices of ≥2.0 and item reliability coefficients of ≥0.8.
Since the Rasch measurement model is based on the assumption that measures are invariant across populations, we compared the responses of girls with those of boys, and those for children aged <12 years and adolescents aged 12 to ≤18 years.
We repeated our analyses on 2-item subsets identified as FDI factors by Kashikar-Zuck et al. (2011): a 7-item “vigorous physical activities” subscale (B) and an 8-item “non–physical daily activities” subscale (C). We also examined the properties of an 8-item short version of the FDI identified by removing redundant items following examination of variable maps (D). We removed 1 redundant item from (D) to determine the characteristics of a 7-item version of the shorter scale (E; Table 2).
Results
Functional Disability
The overall functional disability reported by children fell in the moderate disability category, FDI-A = 13 to 29, mean score = 25.04 (SD = 13.81). The children reported the greatest physical limitations with running the length of a football field (mean = 2.85), doing the activities in gym class (mean = 2.40), and walking the length of a football field (mean = 2.07). The children reported little limitation in watching television (mean = 0.45) and in basic activities of daily living, such as going to the bathroom (mean = 1.08). These findings support the construct validity of the FDI-A (Figure 1).
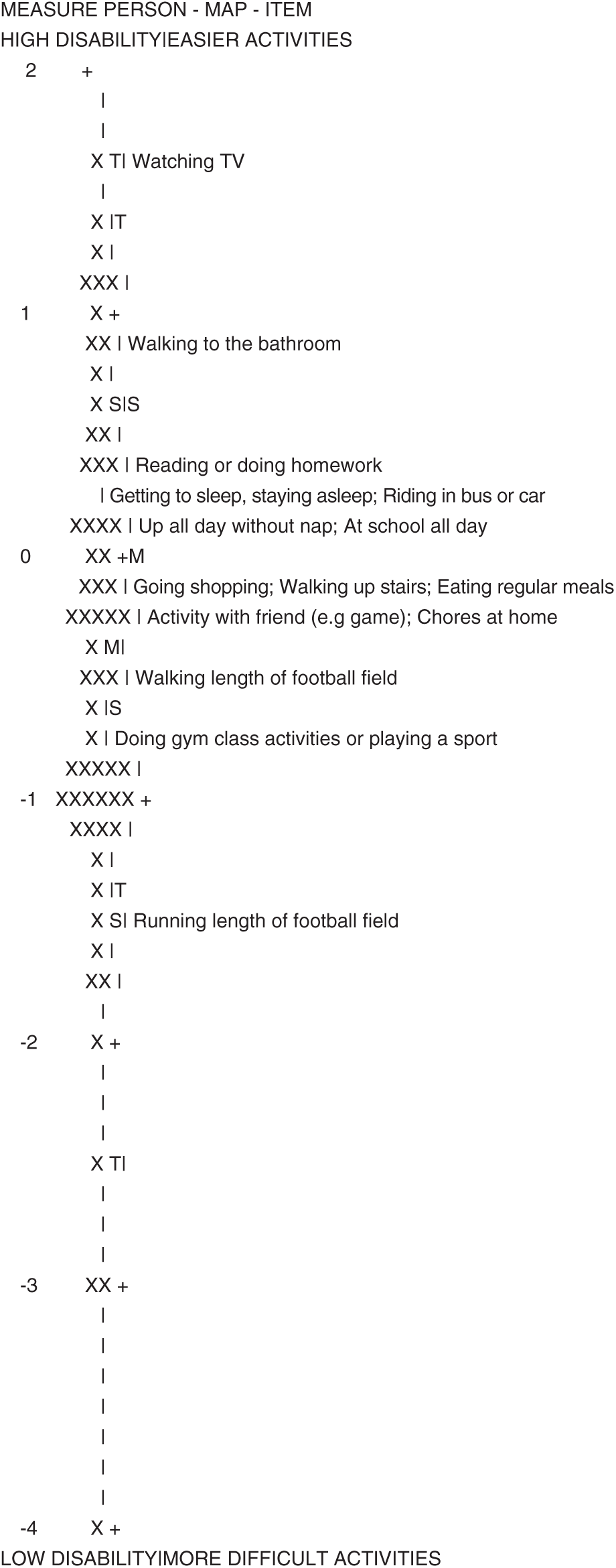
Construct validity and targeting of FDI-A.
Figure 1 shows the relationship between the level of functional disability among the children and the difficulty for them of undertaking activities that involve different levels of exertion. The numbers in the first column from −4 to −3 are measures of functional disability in logits. Each child is represented with an X in the next column. The distribution of disability measures for this sample of children is positively skewed. The difficulty of each activity referenced by an FDI-A item is shown in the column on the right. The most difficult activity for the children is Item 13, “Running the length of a football field,” which coincides with a level of disability more than 1 standard deviation above the mean level of disability for this sample of children. Reading up the column on the right from the easiest item, Item 1, “Walking to the bathroom,” the items requiring physical exertion are plausibly ordered from those that require less physical exertion to those that require more physical effort. This ordering of items supports the plausibility and content validity of the FDI-A. However, Item 15, “Getting to sleep at night and staying asleep,” is quite difficult for these children. Similarly, Item 5, “Eating regular meals,” is as difficult for these children as walking up stairs.
Response Ordering
When we examined response ordering for the full scale (A), we found disordered response categories for Items 1, 5, 8, and 10. The categories disordered for Items 1 and 8 were some trouble and a lot of trouble. The disordered categories for Items 8 and 10 were a lot of trouble and impossible. These results indicate that our Arabic version of the FDI may require modification for future studies because the distinctions between response categories in translation may not be clear enough for Lebanese children and adolescents. Category disorder was corrected to facilitate further analysis.
Dimensionality
We examined the dimensionality of the 15-item FDI-A (Table 2); 56.3% of the raw variance in the observations was explained by the measures, which indicates strong measurement. The first contrast explained 17.1% of the unexplained variance, suggesting the presence of a second dimension (eigenvalue 2.6), with the strength of approximately 3 items. Items 13, 3, 9, 4, and 12 all loaded ≥.4 (.7 to .41) at one pole of the secondary dimension, in contrast with Items 10, 1, 8, and 5, which loaded −.58 to −.35 at the opposite pole. The second dimension may differentiate responses according to types of exertion. Item 13, “Running the length of a football field,” with the highest positive loading (.74), requires physical exertion, whereas Item 5, “Eating regular meals,” with a loading of −.35, requires less physical exertion. Factors described as vigorous physical activities and non–physical daily activities have been extracted from responses to the FDI (Kashikar-Zuck et al., 2011). We describe our evaluation of these subscales in Table 2. Using cutoff parameters adjusted for sample size of outfit (1.74 to 0.24) and infit (1.25 to 0.75), we noted that Items 5 and 8 marginally exceeded the cutoff value for outfit MNSQ, but that none of the items were overly predictable. When we examined infit MNSQ values, we found that Item 9 was overfit (1. 31) and 2 items were too predictable, Items 12 and 13 (Table 1).
Local Dependence
We examined local dependence for the FDI-A. The largest standardized residual correlations (LSRCs) were between 0.33 and −2.5, which indicates that no pairs of items shared more than around 11% of their random variance. Therefore, there no FDI-A items need to be removed for local dependence.
Targeting
We found that the items in the FDI-A directly matched 37% of the children and adolescents in the sample: person mean discrimination −.41, real root-mean-square standard error 0.36 logits, item mean discrimination 0.00, real root-mean-square standard error 0.16 logits (Figure 1). The participants ranged in functional disability from −4.82 to 1.64 logits. The mean difficulty of the items was modestly greater than the mean functional disability of the children (less than .5 logits), indicating that the items were reasonably well targeted to the disability levels of the children (Figure 1). However, none of the FDI items matched the functional ability levels of the children with disability measures below −1.45. Furthermore, no items matched children with disability measures between −1.45 and −.75 logits, between .41 and .93 logits, or between .93 and 1.64 logits. The effective operational range of FDI-A was 0 to 51 (raw score values), 6.46 logits, sufficient to measure the functional disability levels of 83% of the sample (Figure 1).The test information function for the FDI subscale is shown in Figure 2 and peaks at the mode for the sample as it should.
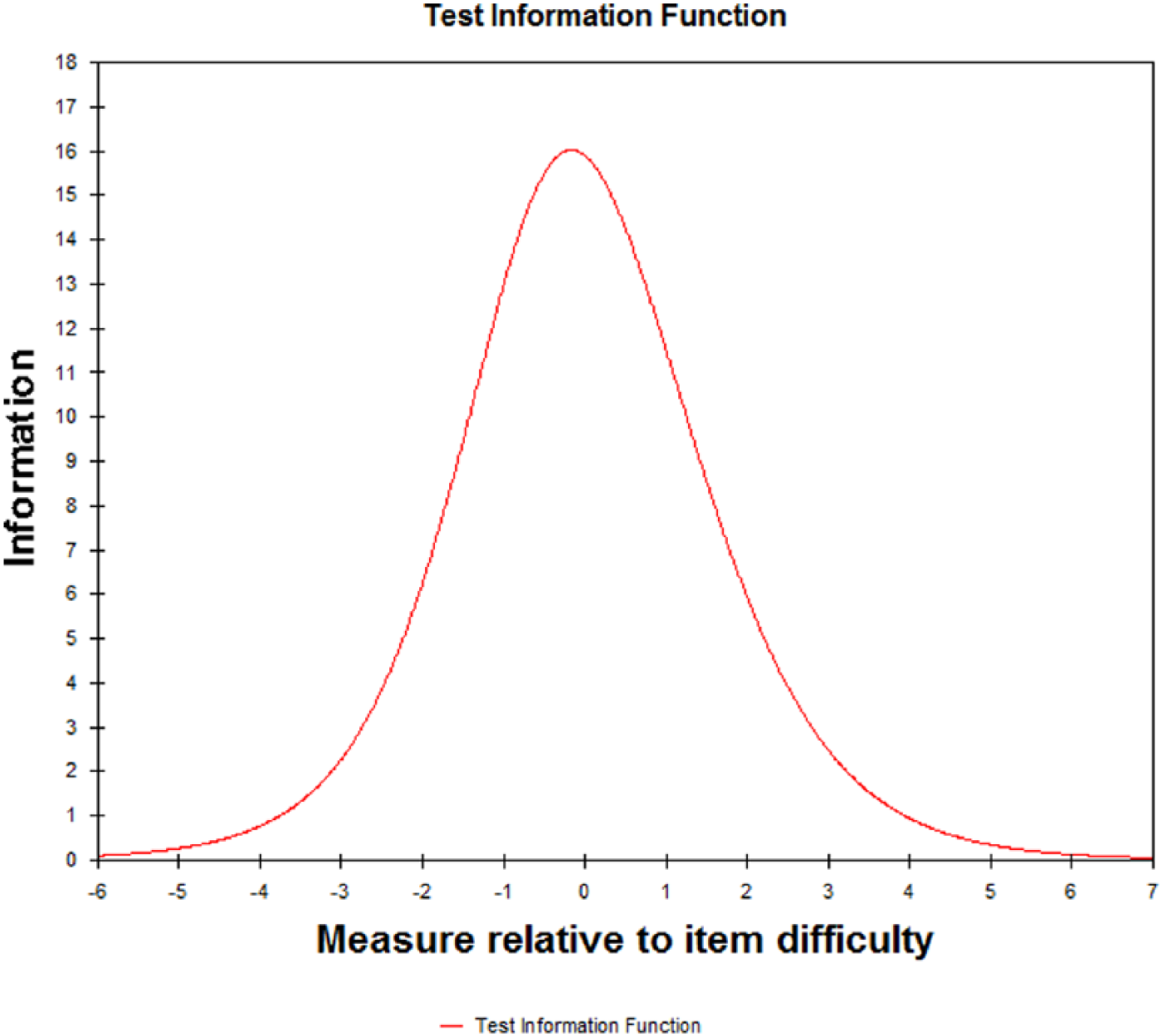
FDI-A test information function.
Item Fit Analyses
With the exception of Item 8 (1.78), all outfit MNSQ values were lower than the sample adjusted cutoff value of 1.76. None of the items had an outfit MNSQ value that indicated overpredictability. Three items had infit MNSQ values that exceeded the sample adjusted cutoff value of 1.25, Item 5 (1.37), Item 8 (1.32), and Item 11 (1.95). Items 12 (MNSQ .62) and 13 (MNSQ .65) were overfit. The items with outfit ZSTD values greater than 1.96 (P = .05, 2-sided significance) were Item 8 (ZSTD = 2.8) and Item 5 (ZSTD = 3.3); the significantly overfit times were Item 12 (ZSTD = −2.3) and Item 13 (ZSTD = −2.1). The items with infit ZSTD values greater than 1.96 were Item 11 (ZSTD = 3.2) and Item 5 (ZSTD = 2.0), which are significantly underfit, and Item 12 (−2.5) and Item 13 (−2.0), which are significantly overfit.
Separation and Reliability
The WINSTEPS person separation value (Linacre, 2012a) indicates whether the FDI-A is sensitive enough to distinguish among higher and lower levels of functional disability. Person reliability in Rasch analysis is equivalent to traditional test reliability, estimated with Cronbach’s α. However, the estimated values for person separation are more conservative than those for Cronbach’s α. Therefore, person separation can be understood as an estimate of the lower bound of reliability. The person separation index of 2.68 for the FDI-A (15 items) indicates that the instrument is sensitive enough to distinguish between 4 strata of functional disability (no disability, low disability, moderate disability, high disability).
Differential Test Functioning
Differential item functioning (DIF) occurs when respondents with the same ability level have different probability of endorsing response categories of the same strength. We examined whether girls and boys and children (aged up to 12 years) and adolescents (aged 12 to <18 years) with the same levels of disability responded differently to FDI-A items. When comparing girls (n = 29) to boys (n = 32), we found that girls were more likely to endorse FDI (A) Item 6, “Being up all day without nap or rest,” than boys (DIF contrast = .69, t =2.52, df = 58, P = .0145). However, this difference may be more apparent than real due to the limited size of the reference group and the comparison group. Generally, DIF classification group sizes of less than 30 do not produce dependable results (Linacre, 2012a). We did not find any items that might be biased in favor of adolescents compared with children.
Analysis of Item Subsets
The analyses conducted so far indicate that the FDI-A was reasonably well targeted for participants in our sample. We examined subsets of items to determine their psychometric properties and to investigate whether it would be feasible for nurses to use a shorter version of the FDI-A to assess functional disability in pediatric cancer patients. The 4 item subsets we analyzed were the following: B. PE-7, seven FDI items identified by Kashikar-Zuck et al. (2011) as measuring physical exertion in children with persistent pain; C. NPE-8, eight FDI items identified by Kashikar-Zuck et al. (2011) as measuring non–physical exertion in children with persistent pain; D. SF-8, eight items selected by removing 7 redundant items after examining the variable map for all 15 FDI-A items; and E. SF-7, seven items in FDA(D) selected by removing Item 14, “Going shopping,” which was significantly misfit. The items in each subset are listed in Table 1. The results of our analyses of the subsets are shown in Table 2.
All 4 of the subsets examined produced the same acceptable value for Cronbach’s α of .85, somewhat lower than that of .93 for all 15 FDI-A items due to the reduction in the number of items. All the subsets of items have similar psychometric characteristics, but FDI (B) and FDI (E) have the same precision when measures are rescaled from logits to units measured on a scale of 0 to 100. For all practical purposes the person separation ratio values for all 4 subscales are equivalent in that they each support 3 strata of measurement (low, medium, and high functional disability). Similarly, the 4 subscales have almost identical effective operational ranges that vary within the narrow range of 5.4 to 5.91 logits (64 to 68 units).
The SD values for 2 of the subsets (B and E) marginally exceed the variability in functional disability measured by full scale (A), but as the RMSE values suggest the loss of some measurement precision. Furthermore, the subsets have a narrower effective operational range and are somewhat less well targeted than the 15-item FDI-A (Table 2).
Discussion
Although the FDI has become a well-established and commonly used measure for the assessment of functional disability associated with chronic pain (Kashikar-Zuck et al., 2011) and is a standard component of pain assessment and pain management (Claar & Walker, 2006), it is not routinely used in Lebanon. Until now the absence of an Arabic version of the FDI has impeded the assessment of functional disability in Lebanese pediatric cancer patients. Our results are important because they indicate that the FDI-A is suitable for clinical assessment and for monitoring the effect on functional disability of pain management. They support the construct validity of the FDI-A and establish acceptable estimates of reliability, Cronbach α .93 for all 15 items and .85 for all 4 of the item subsets we examined. These values are comparable to the Cronbach α values of .86 to .91 reported by Claar and Walker (2006) and the .90 reported by Walker and Greene (1991). We have been conservative in our estimation of values for person separation and reliability. The separation ratios and reliability estimates we report for are based on real SD and RMSE rather than model SD and RMSE values, and support the 3 categories of disability reported by Kashikar-Zuck et al. (2011): no/minimum disability, moderate disability, and severe disability. Furthermore, our examination of FDI-A subsets confirms acceptable reliability of the 2 FDI factors identified by Kashikar-Zuck et al. (2011): vigorous physical activities (Cronbach α = .91) and no physically strenuous daily activities (Cronbach α = .77).
Whereas the FDI was developed as a brief screening tool without subscales reflecting domains of activity (Claar & Walker, 2006), the results of our dimensionality and fit analyses suggest the FDI-A might not be unidimensional. Consequently, further studies are required to establish the dimensional structure of the FDI-A and its convergent, discriminate, and predictive validity. Another reason for continuing to examine the dimensionality of the FDI-A is our concern to validate a shorter version of the scale, which we believe will encourage the routine use of functional disability evaluation in pain assessment and management in Lebanon. Concerns in the country for efficiency in health care delivery require assessment methods that rely on the minimum number of items required to measure domains precisely enough for most clinical and outcome purposes (Mallinson, Stelmack, & Velozo, 2004). Our analyses of FDI-A item subsets show that it is feasible to develop a shorter version of the scale with acceptable precision and reliability. However, as noted the clinical usefulness of a shorter scale needs to be established. Whether the full version or a shorter version of the FDI-A should be routinely used to measure functional disability among pediatric cancer patients in Lebanon depends on the purpose of assessment. For initial assessment and periodic outpatient assessment, the full scale may be required. However, for monitoring patients at home and those in remission by telephone, a shorter version of the FDI-A may be sufficient. Of the subsets examined, (E) SF-8, showed the most potential because it solicits responses to questions about physical and nonphysical exertion.
The disordered use of rating categories we identified for 4 FDI-A items could be corrected by collapsing response categories. However, this would have the serious disadvantage of making it impossible to compare the findings of our future studies with existing and future and international contributions to the field. Our preferred approach is to refine the Arabic translation of the rating categories and to include a visual analogue scale in our assessment interviews to better assist pediatric cancer patients in Lebanon to interpret FDI-A items.
We readily acknowledge the limitations of our study. Our Rasch analysis was conducted as a secondary analysis of data collected from a study that was not intended to establish the reliability of the FDI-A beyond an acceptable value for Cronbach’s α. Our sample consists of only 61 children and adolescents, recruited as a convenience sample from the CCCL. We were able to examine the psychometric characteristics of the FDI-A in our limited sample, but we were unable to compare the self-ratings of our sample with those of parents, nurses, or physicians. Despite these limitations, we have established that the FDI-A and 4 item subsets are worthy of further investigation. Our use of lower bounds for reliability, and therefore for person separation, have enabled us to establish that the FDI-A has the potential to be clinically useful. Future studies will enable us to rely on model rather than real estimates, which will help us distinguish among more than 3 levels of functional disability. Once the clinical utility for the 3-fold classification has been established, the way will be open for making finer distinctions between levels of functional disability that will assist with making decisions about treatment and patient management. However, DIF contrasts estimated for small samples are highly unreliable. Therefore, we need to reexamine whether there really is a difference in the way girls and boys respond to FDI-A items. In particular, we need to determine whether Item 6 is biased toward girls.
We conclude that the FDI-A is productive of useful measurement of functional disability in Lebanese pediatric cancer patients. We note that the children in our sample may have been confused by the Arabic terms used to refer to the response categories in the scale. We intend to refine the Arabic terms and will add a visual analogue scale to assist understanding and consistency in the use of rating scale categories. We have identified the need to reexamine the dimensionality of FDI-A with exploratory factor analysis and confirmatory factor analysis and further fit analyses. Future studies will enable us to report larger person separation ratios and reliability estimates using model rather than real SD and RMSE values. We have begun work on developing a shorter version of the FDI-A for use in monitoring outpatients following initial assessment. We intend to continue our work on the refinement of the scale and to clarify those situations in which it is appropriate to use the full version and shorter versions of the scale.
Footnotes
Acknowledgements
We would like to thank Dr Lynn S. Walker for permission to use the FDI in the primary study and for her approval of the English version (back translation) of the FDI-A. We would like to thank the children and adolescents at the CCCL who agreed to provide data and their parents for consenting to the participation in the primary study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.