
Abstract
The doctorate in nursing practice (DNP) degree is recommended as the terminal degree for advanced practice nurses by 2015. Improvement in the quality of palliative and end-of-life care for children with cancer is recognized as a health care priority. The purpose of this article is to describe: (a) how the American Association of Colleges of Nursing’s 8 core elements and competencies can be used by DNP-advanced practice nurses in pediatric oncology settings and (b) the DNP-advanced practice nurses’ leadership role to advocate translation of evidence in the care of pediatric oncology patients and to promote interdisciplinary collaboration to improve health care outcomes for pediatric oncology patients.
Keywords
Although advances in cancer and supportive treatments have improved the prognosis and long-term survival rate of children with cancer, an estimated 25% of children will die of their disease (Heron, 2011). Thus, the health care goals for children during their cancer trajectory have expanded to include comprehensive care during cancer treatments and palliative care (PC) support and also when the child’s care is transitioned to focus on end-of-life (EOL) care support. This paradigm shift has heightened the importance of advanced practice nurses who are caring for children with cancer to obtain the doctorate in nursing practice (DNP) degree to be well positioned as leaders who will promote integration of evidence-based research into the care of children with cancer during their cancer trajectory (eg, cancer treatments, PC support, and transition to EOL care).
To date, several national nursing organizations have purported the DNP education as critical to advancing the knowledge and clinical skills of advanced practice nurses. For instance, a tenet of the American Association of Colleges of Nursing (AACN) is that because of increasing complexities of health care delivery and ongoing advancements in health care research, it is necessary that advanced practice nurses should obtain a doctoral degree in nursing practice (eg, DNP) to ensure safe and effective health care delivery to future patients (AACN, 2006). Additionally, a tenet of the National Association of Pediatric Nurse Practitioners is that nurses with the DNP degree are prepared to have a high level of scientific knowledge to translate evidence-based research into practice and to possess the highest level of clinical competence (National Association of Pediatric Nurse Practitioners, 2013).
Currently, 70% of oncology care provided to patients in the United States and Puerto Rico are in cancer centers accredited by the Commission on Cancer (CoC; American College of Surgeons, 2013). The CoC has established accreditation standards that purport the full spectrum of patients’ cancer care trajectory should encompass diagnostic screening for cancer detection and to palliative and EOL care (CoC, 2012). Also, adult and pediatric cancer centers in the United States that plan to seek or maintain accreditation will be required to comply with the new CoC standards by 2015. A new CoC standard related specifically to palliative care, titled “Standard 2.4: Palliative Care Services,” will mandate cancer centers seeking accreditation by 2015 to have the availability of on-site PC services available for their patients and have established communication with community resources for potential referral for PC services available for their patients ((CoC, 2012). Additionally, Standard 2.4 will mandate that the PC team can include 1 physician (preferably board certified in palliative care) and 1 non-physician member. According to the guidelines of Standard 2.4, the non-physician team member can include a nurse who preferably has obtained specialty training or certification in hospice and/or PC nursing ((CoC, 2012). Therefore, according to Standard 2.4, hospitals could choose to employ nurses with a wide range of palliative and hospice care training experience. Also, this guideline does not mandate or recommend that nurses working in PC/EOL should possess or seek PC/EOL certification or an advanced degree.
Practicing pediatric nurse practitioners (PNPs) certified in both primary and acute care are trained to provide comprehensive care for pediatric oncology patients. However, PNPs may have primarily received clinical training under the guidance of a primary care physician with limited or no research training. PNPs who obtain a DNP degree will receive advance training that will specifically position them to provide leadership in promoting the translation of evidence-based research findings into clinical practice (Graff, Russell, & Stegbauer, 2007). For example, pediatric oncology nurses who obtain a DNP degree will receive advanced training in research skills to equip them to be able to critically analyze evidence-based research in the literature and to propose recommendations about changes in care for pediatric oncology patients. Also, DNP-prepared advanced practice nurses will be prepared to promote the benefits of engaging in interdisciplinary collaboration and communication with other oncology team members with the goal of providing comprehensive and compassionate care to children with cancer across the cancer trajectory and especially during PC/EOL.
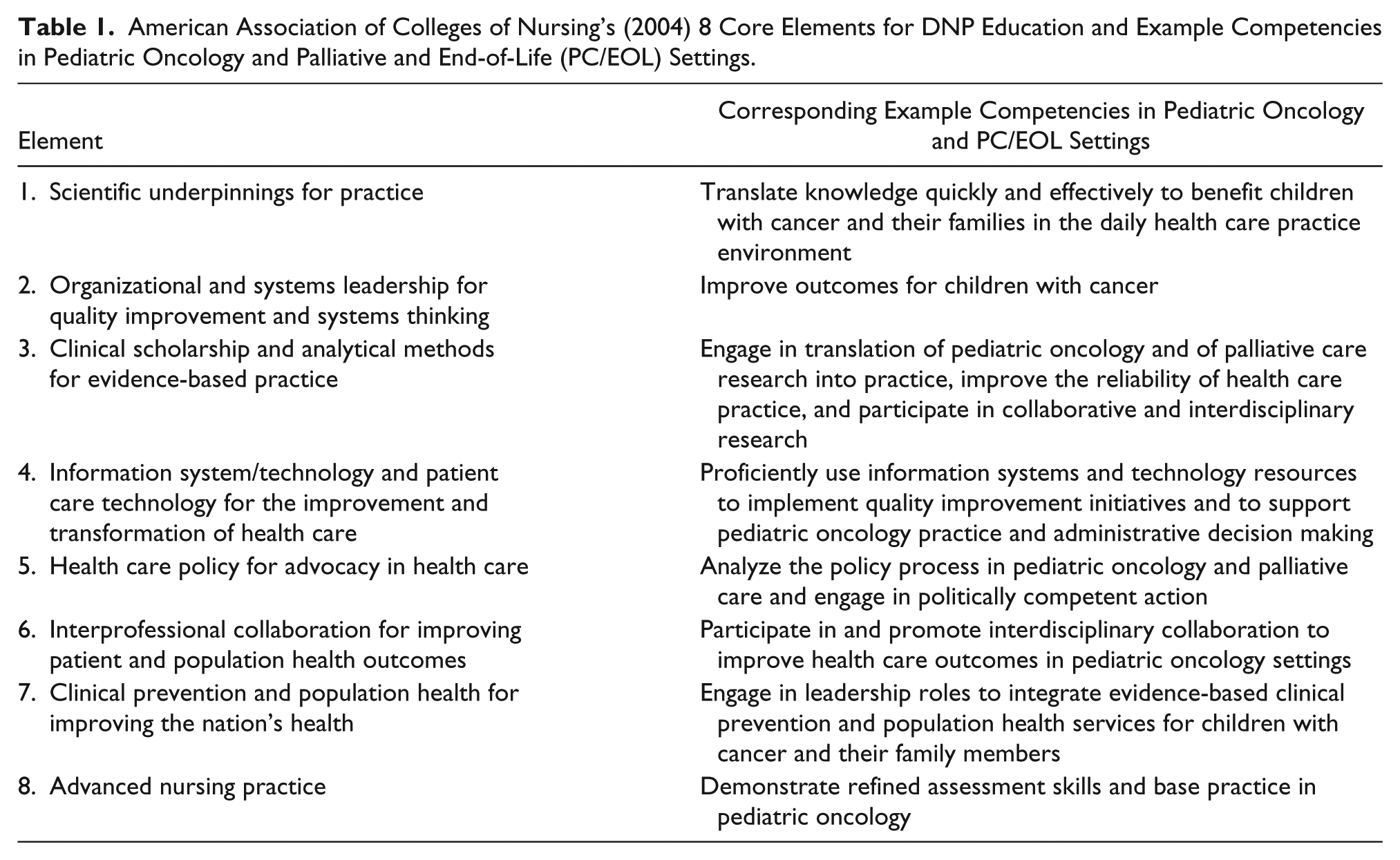
The unique role and contributions of the DNP-prepared advance practice nurse is still not widely recognized and used in pediatric clinical settings. Therefore, the purpose of this article is to (a) provide a concise review of how the 2004 AACN’s 8 core elements (see Table 1) can be translated to example competencies in pediatric oncology settings (with or without established PC support services) and can be used as a helpful guide by DNP advanced practice nurses during delivery of nursing care for pediatric oncology patients and (b) discuss how the educational preparation of the DNP equips advanced practice nurses to assume a leadership role to promote use of evidence-based research in the care of pediatric oncology patients and to promote interdisciplinary collaboration to improve health care outcomes for pediatric oncology patients.
American Association of Colleges of Nursing’s (2004) 8 Core Elements for DNP Education and Example Competencies in Pediatric Oncology and Palliative and End-of-Life (PC/EOL) Settings.
Description of the DNP
In contrast to the research focused on the nursing doctorate (PhD in nursing), the DNP is described as a clinical practice–focused doctorate (Barry, 2009). The DNP equips nurses to attain the highest level of scientific knowledge to use in their unique practice setting and to be a more thoughtful consumer of health care research in specialized roles (Smith, 2006). The DNP has gained national interest by nurses seeking a doctoral degree in nursing (Barry, 2009). The call for nurses to be well prepared to practice within an increasingly complex health care system has contributed to the 2004 AACN recommendation that advanced practice nurses should obtain a doctorate degree (eg, DNP, PhD) by 2015 (Drayton-Brooks, Barksdale, & Werner, 2011; Sperhac & Clinton, 2008).
DNP education programs prepare nurse graduates to have a high level of nursing knowledge and advanced research knowledge to use in their practice setting (Barry, 2009). DNP-prepared advanced practice nurses are equipped with leadership skills to be change-agents in complex health care settings and to critically appraise research findings to contribute to the development of a tailored (or individualized) plan of care for patients that is based on the best evidence-based research findings (Fain, Asselin, & McCurry, 2008). Tailoring evidence-based care is a basic principle of providing quality care to all patients (Rew, 2011). Thus, the pediatric oncology advanced practice nurse with a DNP will be especially well prepared with advanced research training to determine and incorporate appropriate evidence-based research to maximize quality PC/EOL for children with cancer and a poor prognosis (Sperhac & Clinton, 2008).
The DNP-Prepared Pediatric Oncology Nurse Practitioner
Pediatric oncology treatment settings have historically used advanced practice nurses (eg, PNPs) to plan and deliver care to children with cancer. Advanced practice nurses have also collaborated with other oncology team members to plan individualized care for children with cancer in pediatric oncology settings. A collaborative oncology team approach is warranted because the attending physician often has multiple rotating assignments between inpatient, outpatient, laboratory research, and administrative duties. Therefore, the advanced practice nurse is well positioned on the team to ensure continuity of delivered care across the inpatient and outpatient settings and subsequently for PC/EOL. The nature of oncology treatment requires ongoing outpatient clinic appointments combined with both unscheduled and scheduled admissions to the inpatient unit for treatment of complications or for routine therapy. In addition, pediatric oncology patients receiving treatments are at high risk for needing sudden admission to the intensive care unit. Parents of pediatric oncology patients, therefore, need and expect the oncology team to provide clear communication of what is in the best treatment recommendation during all phases of the child’s cancer care. The advanced practice nurse is likely to have a unique relationship with the family that combines graduate-level education with hands-on nursing education and counseling. The advanced practice nurse is often well positioned to follow the patient across health care settings in the community and to foster ongoing communication with interdisciplinary health care teams from other services who may also follow the patient. Examples of care transitions in which communication would be critical to ensure continuity of the child’s care may include (a) at diagnosis and during adjustment to the child’s diagnosis in an acute care setting, (b) during the spectrum of oncology treatments and PC support in an approved cancer center, (c) during the child’s transition back into the school environment, (d) while being monitored in the community by the child’s primary care physician, and (e) during the child’s transition to, and delivery of, PC/EOL.
While seeking the DNP degree, the advanced practice nurse will complete doctoral level nursing courses in accredited nursing programs that were developed based on the AACN’s (2004) 8 core elements. These elements are listed in the left column of Table 1. In the right column of Table 1, 2 of the authors of this article (ie, Hendricks-Ferguson & Foster, 2014) prepared example competencies to correspond with the 2004 AACN’s core elements (AACN, 2004) and to help illustrate the potential application of each of the 8 elements in pediatric oncology and palliative settings. Also, 2 of the authors of this article (ie, Hendricks-Ferguson & Foster, 2014) developed Figure 1, to provide a concise depiction of the authors’ proposed application of the AACN’s 8 core elements that are listed in the left column of Table 1. The AACN’s (2004) 8 core elements can easily be used as a guide by DNP-advanced practice nurses when planning for the comprehensive and sometimes complex PC/EOL needs of pediatric oncology patients. Therefore, the pediatric oncology nurse, prepared at the DNP level of education, is purported by the AACN to be especially positioned and equipped to be a leader in planning and providing comprehensive evidence-based multidisciplinary care to the pediatric oncology patient during the cancer treatment trajectory and during PC/EOL.
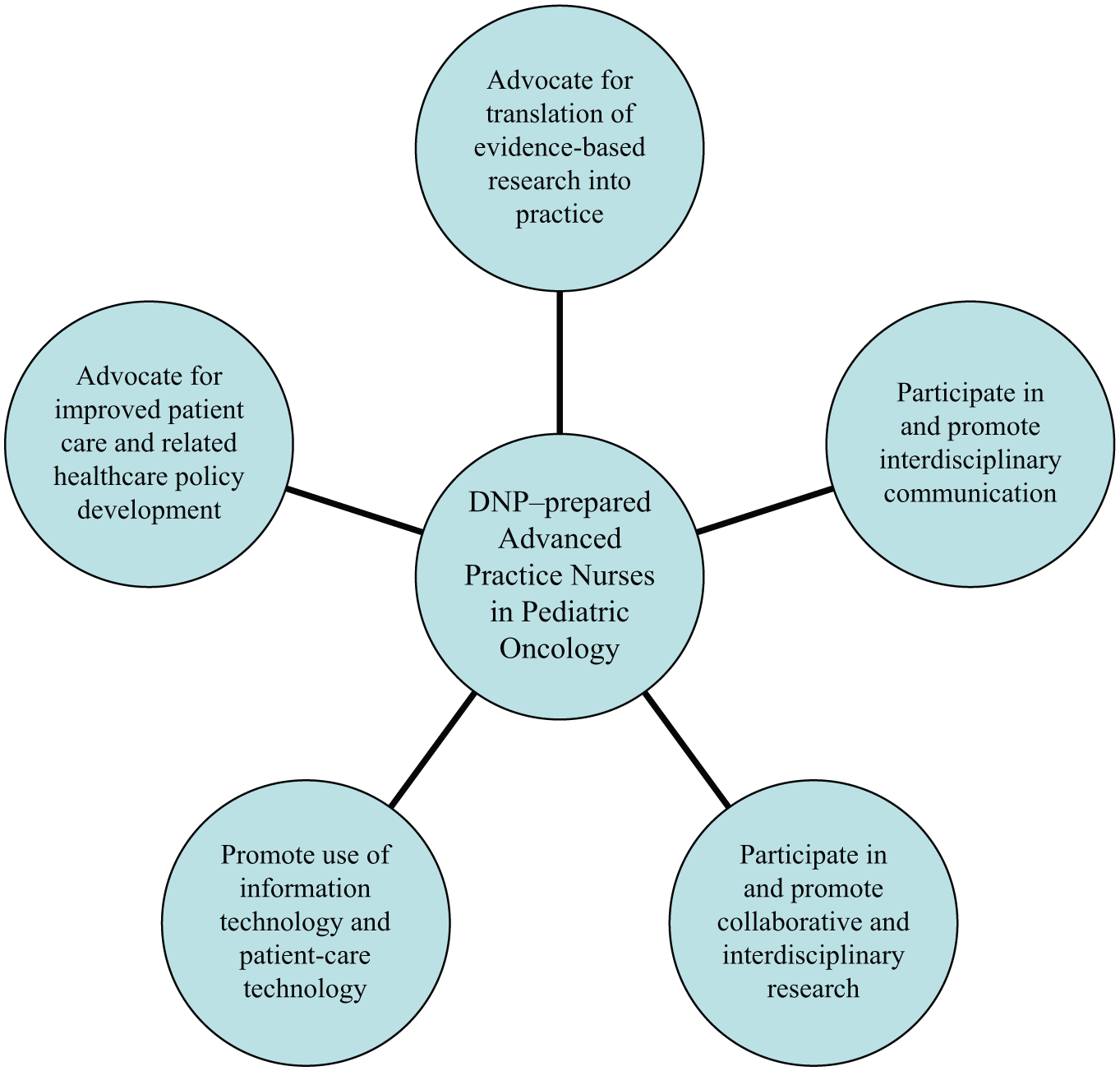
Unique contributions of the DNP advanced practice nurses in pediatric oncology (by Hendricks-Ferguson & Foster, 2014).
DNP Contributions
DNP-prepared advanced practice nurses offer a unique skill set (eg, research, advanced technology) to foster delivery of quality care to children with cancer during oncology treatments, palliative care support, and transition to EOL care. Figure 1 provides a depiction of skills that can illustrate the unique contribution of DNP-prepared advanced practice nurses to assume a leadership role to (a) advocate translation of evidence-based research findings into practice, (b) participate in and promote interdisciplinary communication, (c) participate in and promote collaborative interdiscipli-nary research, (d) promote use of current and advanced information technology to foster quality patient care, and (e) advocate for improved patient care based on current health care policies (see Figure 1). Examples that pertain to PC/EOL for children with cancer are provided in following sections.
Incorporating Theory Into Practice
The Newman Systems Model (NSM) can be used as a framework for implementing the key DNP elements and competencies in pediatric hematology/oncology practice. The NSM is a recognized multidimensional and comprehensive approach to assessing a client system (eg, children with cancer and their families) interacting with stressors (eg, transition to EOL care) in their environment (Newman, 1989). This model can be easily used to guide the DNP-prepared advanced practice nurse’s scope of practice, such as (a) advocating for quality care for children with cancer during their cancer trajectory; (b) advocating for translation of evidence-based research findings into the care of children with cancer; and (c) participating and promoting interdisciplinary communication to ensure effective delivery of care to improve health care outcomes for pediatric patients during oncology treatments, acute care and home care management, and during follow-up management and PC/EOL support according to patient and family preferences. Based on the NSM, DNP-prepared advanced practice nurses employed in pediatric oncology settings should develop a patient care vision that includes ongoing assessment and critical appraisal of current and future health care policies that may affect the health care of pediatric patients with cancer and their families. This vision can also be enhanced by keeping abreast of current literature, applicable nursing theory, and evidence-based research to better advocate for quality care for pediatric patients with cancer and their family members throughout the cancer trajectory (eg, during cancer treatments and PC support, EOL care, bereavement support).
For example, the PC/EOL care of a pediatric oncology patient with a poor prognosis can be improved if the DNP-prepared advanced practice nurse selects a respected theoretical framework, such as the NSM framework, to conduct a critical appraisal of published evidence-based research findings regarding parents’ preferred place of death for children with cancer. Also, the NSM framework can be used as a guide to conduct a comprehensive evaluation of available community hospice programs (ie, inpatient vs outpatient, home care nurse vs hospice nurse) for the child with cancer prior to the planned transition to EOL care in their respective community. In summary, the unique contributions of DNP-prepared advanced practice nurses, who are caring for children with cancer, can be enhanced by having doctoral-level nursing course work as well as by possessing years of clinical experience that will equip them to (a) conduct comprehensive assessments of the current and ongoing health care needs of pediatric patients with cancer, (b) critically appraise research findings and evidence-based guidelines that may contribute to the highest level of quality of life for the child during their cancer and PC/EOL trajectory, and (c) be recognized as a very valued oncology team member that is committed to advocate for changes in the child’s plan of care that is based on evidence-based research as the child’s health needs change during any point of their cancer and PC/EOL trajectory.
Practice With Advanced Clinical Skill Set
Nurses with previous pediatric oncology work experience who have obtained the DNP degree will have received advanced training to translate evidence-based research into their clinical practice while performing clinical skills to assess, evaluate, and recommend treatments for children with cancer during PC/EOL. Also, the DNP-prepared advanced practice nurse who has a personal goal of becoming recognized as possessing advanced PC/EOL skills for children with cancer will wisely plan their DNP course work (eg, taking PC/EOL and holistic care–focused electives) and clinical hours to develop or refine their assessment skills to acquire advanced clinical skill competencies to ensure excellent delivery of care for children during the dying process and during after-death care. Such specialized training can equip the DNP-prepared advanced practice nurse to provide evidence-based information to parents of what to expect as their dying child’s disease progresses and physical function decreases. In addition, the DNP-prepared advanced practice nurse caring for children with cancer can offer evidence-based guidance on the assessment and effective treatment of symptoms during PC/EOL. For example, a tailored symptom management plan should be carefully planned for children during PC/EOL that is based on evidence-based research findings. The DNP-prepared advanced practice nurse may also receive advanced education in holistic supportive care (eg, complementary and alternative therapies) to foster effective symptom management for children during PC/EOL. Effective management of symptoms is critical to ensure comfort and quality-of-life for children with cancer during PC/EOL. Effective symptom management has also been described as being affected by multidimensional domains, including physical, psychological, social, and spiritual well-being needs (Ferrell, 2005). Additionally, the comprehensive DNP course work will prepare the DNP-prepared advanced practice nurse to possess advanced technology skills to share with the health care team and to enhance access to resources describing these multidimensional care domains (Rew, 2011).
Translate Evidence-Based Research Into Practice
Important and unique to the contribution of the DNP-prepared advanced practice nurse, whose scope of practice includes pediatric oncology patients and palliative care, is the advanced preparation to translate evidence-based research into practice. DNP-prepared nurses are especially prepared to critically appraise current scientific literature and recommend translation of evidence-based policies and interventions into practice (Emanuele, 2011). Hence, DNP-advanced practice nurses practicing in pediatric oncology will be able to use these advanced skills to advocate to foster ongoing improvement in the pediatric oncology patients’ plan of care.
For instance, the literature includes several studies that provide evidence about symptom management during PC/EOL and parental preferences during PC/EOL of children with cancer (Arland, Hendricks-Ferguson, Pearson, Forman, & Madden, 2013; Hendricks-Ferguson, 2008; Hinds, Schum, Baker, & Wolfe, 2005; Madden, Hendricks-Ferguson, & Foreman, 2013). In one study (Arland et al., 2013), the prospective intervention of providing early referral to palliative care support for pediatric patients with a brain tumor and a poor prognosis was shown to result in decreased hospital admissions and improved symptom management. In a second study of one pediatric practice (Madden et al., 2013), administration of continuous infusion midazolam for pediatric patients with a brain tumor who are receiving hospice care in the home setting was reported as an effective pain management intervention. Hence, the DNP-prepared advanced practice nurse could share the symptom-related research evidence from these 2 studies with members of their oncology team practice and advocate evaluation of these interventions with future pediatric patients with cancer. In a third study (Hendricks-Ferguson, 2008), the majority of bereaved parents reported a preference to have received information about PC/EOL options earlier in their child’s cancer care rather than receiving this information near their child’s EOL care. The results from this third study along with tenets about the importance of assessing parents’ preferences to receive PC/EOL information could also be shared with the oncology team by the DNP-prepared advanced practice nurse. The findings in this third study could also be discussed with the oncology team as an example of evidence that supports the 2014 recommendation by the National Institutes of Health–National Institute of Nursing Research that early pediatric palliative care conversations matter (National Institute of Nursing Research, 2014). Each of the described examples of exchanging evidence-based research with members of the oncology team caring for pediatric oncology patients illuminates the importance of being an advocate to improve the care of future pediatric oncology patients with a poor prognosis.
Develop Practice and Research Goals
Further research is needed in validating site-specific strategies in symptom management of the dying child (Arland et al., 2013). Therefore, the role of the nurse with the DNP degree should include routine consultation with the health care team for the purpose of developing research studies focused on symptom management for pediatric patients with cancer. Strategies may include the following: (a) initiating a needs assessment through staff, parent, and child focus groups; (b) evaluating research studies and making recommendations for current patients; (c) evaluating the efficacy of new evidence-based interventions to improve acute and long-term health care outcomes; (d) developing a tailored plan for the patient and family; and (e) identifying grant funding resources for team members to plan a collaborative study (Mackey & Estala, 2008).
A total of 22 recognized cancer-specific assessment tools are currently available that could be used to plan a clinical research study by the DNP-prepared advanced practice nurse (Collins, 2002; National Quality Forum, 2012). For example, DNP-prepared advanced practice nurses can use their research training and clinical knowledge to lead the planning of a collaborative research study with the oncology team and to develop a research proposal and prepare required documents to be submitted to the institutional review board as a principal investigator to evaluate symptom-management strategies during PC/EOL for pediatric oncology patients. Another example is that the DNP-prepared advanced practice nurse could also lead the planning and implementation of a qualitative study, such as conducting focus groups with parents of children who have died of cancer to evaluate their perspectives on their child’s death care (eg, place of death and after-death care). Also, the DNP education can also position the advance practice nurse to foster collaborative clinical relationships with interdisciplinary team members to identify and enroll eligible subjects and the research expertise to facilitate planned focus groups and to lead the analysis of collected focus group data.
Initiate Interdisciplinary Health Care Team Communication
The DNP-prepared advanced practice nurse can establish and build a respected relationship with the health care team members and provide a valued skill set (ie, advanced research and technology knowledge) during the care of all patients (Dennison, Payne, & Farrell, 2012). Hence, the DNP educational training on effective communication with interdisciplinary teams can also foster collaborative team building with members of the health care team to better serve pediatric oncology patients during inpatient and outpatient care and when receiving referrals for care from other clinical services (eg, PC support teams, hospice care). Through dialogue with members of the health care team, the DNP-prepared nurse can identify specific health care concerns of patients and families that surface during direct clinical practice and then apply research to address those concerns. For example, a child dying of a brain tumor at home on hospice care may have progressive, intractable seizures and no intravenous access. In this clinical situation, the DNP-prepared advanced practice nurse could engage in focused discussions about evidence-based recommendations with the hospice nurse, the attending physician, members of the hospice team, and the parents of the child regarding the appropriate medication escalation and route of administration. The DNP-prepared advance practice nurse could also advocate for the use of the rectal route as acceptable for pain management or for the child to be hospitalized for a central venous access device to facilitate the administration of medications. Another example is a child with hydrocephalus secondary to a progressive brain tumor. The DNP-prepared advanced practice nurse would be well positioned to facilitate team discussions with members of neurosurgery and other oncology team members regarding the prognosis and evidence based symptom management of expected and often distressing symptoms (eg, headache, uncontrolled increased intracranial pressure). The DNP-prepared advanced practice nurse could also lead interdisciplinary team discussions about the child’s prognosis, parental preferences related to the location of EOL care, and recognized quality-of-life indicators related to pain and comfort of the dying child.
The DNP-prepared advanced practice nurse is prepared to foster interdisciplinary communication with other health care team members (eg, primary oncologists, advanced practice nurses, front-line nurses, social workers, psychologists, clergy members, child life specialists, etc) to foster focused discussions to share ideas, questions, or concerns in order to stimulate interest in research (eg, exploring symptom-management trends in pediatric oncology, testing behavioral and symptom management interventions during PC/EOL, exploring grant opportunities; Dennison et al., 2012; Rew, 2011). The DNP-prepared advanced practice nurse is also well prepared to plan effective communication to better probe other health care team members about their experiences, compare these experiences to the literature, raise questions about anecdotal clinical observations, and identify gaps in the literature. Planned dialogue among interdisciplinary team members can provide leadership opportunities and recognition for the DNP-prepared advanced practice nurse to enhance the quality of care for children dying of cancer and their families.
Patient Advocate and Policy Developer
The DNP-prepared advanced practice nurse who is caring for children with cancer can be a voice that offers timely recommendations that adhere to newly approved and existing health care policies that may foster quality health care practices for pediatric oncology patients during PC/EOL. Fostering interdisciplinary discussions to plan PC/EOL care for all patients is an example of a strategy to enhance institutional compliance of current health care policy, such as the 2013 American College of Surgeons standards, which purports an interdisciplinary team approach in the delivery of comprehensive PC (Muehlbauer, 2013). Another example is being a resource to update the team about cutting edge PC/EOL publications, such as the 2014 Institute’s proposed core components of quality EOL care (IOM, 2014). The specialized care required for children with cancer encompasses holistic care to meet their acute and long-term health care needs (Yard, 2009). For example, the DNP-prepared nurse can be well positioned to foster team initiation of early discussions about PC/EOL options with parents of children with cancer who have a poor prognosis. The DNP-prepared advanced practice nurse who has clinical experience in PC/EOL will especially be prepared to advocate for timely discussions with patients and families about PC/EOL support, using advanced research and clinical expertise, collaboration with the attending physician, as well as the nursing relationship with the patient and family (Arland et al., 2013). An example of a strategy to foster development of an institutional patient care policy is for the DNP-prepared advanced practice nurse to hold a faculty meeting or departmental grand rounds to demonstrate examples of effective PC/EOL discussions using role-play activities and then have an open discussion with the entire medical/nursing staff to promote early and effective PC/EOL discussions with parents of pediatric oncology patients with a poor prognosis. Also, the DNP-prepared advanced practice nurse could participate in state and national policy planning teams to inform pediatric discussions about new press releases, such as 2014 National Institutes of Health–National Institute of Nursing Research campaign titled, “Early Palliative Care Conversations Matter” (National Institute of Nursing Research, 2014), and the available evidence-based resources on the National Institutes of Health Web site related to this campaign.
Implications for Practice
Health care system business plans in pediatric oncology should include DNP-prepared advanced practice nurses and highlight the unique contributions these professionals can offer. The business plans should (a) document the DNP-nurse candidate’s advanced technology skills and knowledge of how to critically appraise published evidence-based research for possible translation into clinical practice; (b) document proposed time allotted for clinical practice and scholarship (or research) activities (eg, 80% clinical practice role, 20% research role); (c) define the DNP-prepared nurse’s role, responsibilities, and proposed salary; and (d) describe the significance of recruiting an advanced practice nurse with a DNP degree in a collaborative practice (Barry, 2009; Mackey & Estala, 2008). The DNP-prepared advanced practice nurse must also propose future research to gather data on the reduced-cost-yet-improved care for children dying of cancer by an expert doctor of nursing practice. The multidisciplinary care for a child with progressive cancer requires immense coordination. The nurse with a DNP degree combines all of the valued roles of the advanced practice nurse to foster and promote quality care for children with cancer and also during EOL care. Because of proposed advanced educational mandates for advanced practice nurses, the number of DNP-prepared nurses will continue to increase over time. DNP-prepared nurses should prove valuable for their advanced skills in technology, research, and interdisciplinary communication that will better position them to advocate for monitoring and fostering the delivery of quality care to pediatric patients with cancer throughout the spectrum of their cancer trajectory (eg, cancer treatments, symptom management, psychosocial support, and during PC/EOL).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.