
Abstract
Introduction
The measurement of health-related quality of life (HRQoL) in patients during an illness experience is an important means to evaluate the quality and outcomes of health care (Bradlyn et al., 1996; Hinds, 1990; Moons, Budts, & De Geest, 2006; Wilson & Cleary, 1995). HRQoL and other factors that contribute to change during the patient’s illness experience are well documented (Eiser, Eiser, & Stride, 2005; Hinds, 1990; Klassen, Anthony, Khan, Sung, & Klaassen, 2011; Sung et al., 2009). However, few studies have specifically addressed factors such as time and duration of therapy that can affect HRQoL in children with cancer during treatment. Although studies have identified factors associated with HRQoL within specific diagnostic groups of childhood cancers, their results are conflicting and preclude the identification of important factors contributing to HRQoL in childhood cancer (Klassen et al., 2011). Moreover, studies reporting the implementation of an intervention to improve HRQoL in children with cancer undergoing curative treatment are limited. Treatment-related HRQoL factors are often difficult to identify in children undergoing curative cancer treatment, due to complexity of the treatment regimen and cancer variability. Furthermore, current systematic reviews include findings from both children undergoing curative treatment and childhood cancer survivors, which further precludes the identification of factors contributing to HRQoL in children undergoing curative treatment (Klassen et al., 2011).
The development of new treatment modalities necessitates the review of recent literature to understand the factors that impact, and the current status of HRQoL in children undergoing curative cancer treatment (Gilbertson, 2004; Miralbell, Lomax, Cella, & Schneider, 2002; Pui et al., 2009). There is limited literature aimed at identifying the factors that influence the reported HRQoL specifically in children undergoing curative cancer treatment. Therefore, we conducted a review of the literature to identify factors that influence the described experience.
Conceptual Framework
Several frameworks explicate the HRQoL of children; however, clarifying the concept of HRQoL in children with cancer is a challenge in HRQoL research (Hinds, Burghen, Haase, & Phillips, 2006; Wallander, Schmitt, & Koot, 2001; Zhan, 2006). One such theory-driven framework was developed by Lach et al. (2006) in the study of the quality of life in children with epilepsy. Subsequently, Klassen et al. (2011) adapted Lach’s model to identify the factors associated with the quality of life of children with cancer and childhood cancer survivors. This adapted model for childhood cancers identified 3 major domains of HRQoL in children that capture the major factors of HRQoL in children undergoing curative cancer treatment. The domains are (1) the biomedical status/level of the impairment domain, which is categorized by disease factors and comorbidities; (2) the intermediate factors domain, which is divided into 3 subdomains—child, family, and community; and (3) the outcome factors related to social, worries, emotional, normalcy, and secrecy domains (Lach et al., 2006). This conceptual model was used as the framework for our review.
Method
Data Sources
A structured review of literature was conducted to identify published studies that explored factors that influence the HRQoL in children undergoing curative cancer treatment. The search strategy was developed and implemented with the support of a medical librarian. A literature search of PubMed, CINAHL, and PychINFO was performed, using health-related quality of life and quality of life as MeSH terms. Other terms often used to describe the dimensions of HRQoL such as “health status” or “functional status” were not included in the search, because the terms health-related quality of life and quality of life have been developed sufficiently and are widely understood to represent a different and a broader concept. The terms were subsequently combined with a subject heading for cancer and limited to children. Articles were initially screened for eligibility on the basis of the title, followed by screening of the abstract, and finally screening of the full text. Bibliographies of full-text articles were also screened for relevant literature that was not identified during the literature search.
Inclusion and Exclusion Criteria
The following inclusion criteria were used to select full-text articles: (1) study participants: children and adolescents ≤18 years, (2) publication date from January 2005 to March 2013, (3) studies published in English, (4) study participants undergoing curative cancer treatment, and (5) the study outcome or dependent variable HRQoL or quality of life. Since the study purpose was to identify quality of life in children undergoing curative treatments, articles were excluded if they examined cancer survivors or children undergoing palliative care with no realistic chances of survival.
Results
Figure 1 presents a flowchart of the process used to identify studies that met the inclusion criteria. The initial search identified 1333 studies, of which 753 were excluded on the basis of titles. Of the 580 remaining studies screened, 492 were excluded on the basis of the abstract review. Thus, 88 full-text studies were analyzed, of which 26 met all the inclusion criteria. The final 26 studies (Table 1) included in this review represent work conducted in 16 countries, with a majority of studies (17) occurring in the United States. Study sample size ranged from 20 to 411 children and adolescents. HRQoL factors were categorized based on our conceptual framework into 5 domains: cancer, cancer treatment, child, family, and community factors.
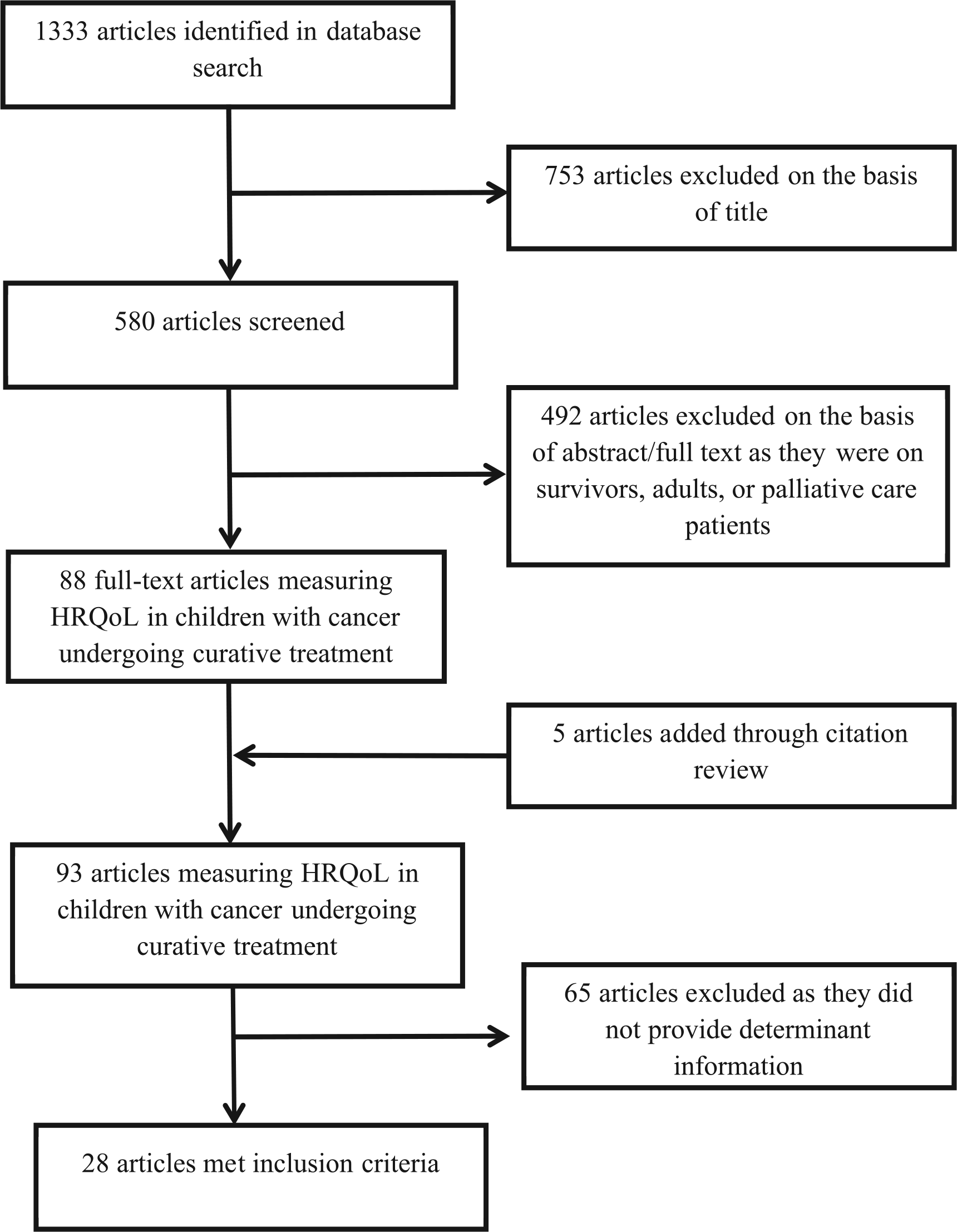
PRISMA flow diagram of the research process for the literature review. HRQoL, health-related quality of life; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Study characteristics for publications included in the review.

Abbreviations: ALL, acute lymphoblastic leukemia; OS, osteosarcoma; NHL, non-Hodgkin lymphoma; CNS, central nervous system; AML, acute myeloid leukemia; HL, Hodgkin lymphoma; KPS, Karnofsky Performance Scale; Dx, diagnosis; Dexa, dexamethasone; Pts, Patients; QoL, quality of life; RMS, rhabdomyosarcoma; CTX, chemotherapy; XRT, radiotherapy; IQ, intelligence quotient; TACQOL, TNO-AZL Questionnaire for Children’s Health-Related Quality of Life; SES, socioeconomic status; BT, brain tumors; GCT, germ cell tumors; CML, chronic myeloid leukemia; HB, hemoglobin; Ewing, Ewing sarcoma; CAM, complementary alternative medicine; CHQ, Children’s Health Questionnaire; POQOLS, Pediatric Oncology Quality of Life Scale; SCT, stem cell transplant; EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Core 30; PedsQL, Pediatric Quality of Life Inventory.
The review identified that HRQoL was quantified by a variety of instruments, including 5 generic and 5 cancer-specific questionnaires. The most common instrument used in studies was the PedsQL Generic Core Scale version 4.0, (N = 13), followed by the Children’s Health Questionnaire (N = 3) and the DISABKIDS Chronic Generic Module (N = 2), the Lansky Performance Scale (N = 1), and the TNO-AZL Questionnaire for Children’s HRQoL (TACQOL; N = 1). The most common cancer-specific instrument used in studies was the PedsQL Cancer Module version 3.0 (N = 11), followed by the PedsQL-Brain Tumor Module (N = 2), the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ C-30) (N = 2), the Minneapolis-Manchester Quality of Life Instrument (N = 1) and the Ecocultural Family Interview–Cancer (N = 1).
Cancer Factors
The most frequently studied cancer factor was cancer diagnosis. Fourteen studies were identified as assessing the influence of cancer diagnosis on HRQoL by comparing cancer diagnoses in cohorts of children with various cancer diagnoses (af Sandeberg et al., 2010; Baggott et al., 2011; Barakat et al., 2010; Eiser et al., 2005; J. M. Erickson et al., 2011; Hinds et al., 2009; Hullmann, Wolfe-Christensen, Meyer, McNall-Knapp, & Mullins, 2010; Kuhlthau et al., 2012; Landolt, Vollrath, Niggli, Gnehm, & Sennhauser, 2006; Pek et al., 2010; Shankar et al., 2005; Sung et al., 2009; Tremolada et al., 2011; Zareifar et al., 2012). The results of these studies varied widely, with 7 studies describing cancer diagnosis as having a significant influence on the child’s HRQoL (af Sandeberg et al., 2010; Hinds et al., 2009; Landolt et al., 2006; Pek et al., 2010; Shankar et al., 2005; Sung et al., 2009; Zareifar et al., 2012).
Two studies compared the HRQoL between cancer diagnoses and reported that children with acute lymphoblastic leukemia (ALL) had higher HRQoL scores than those with solid or central nervous system tumors (Baggott et al., 2011; Sung et al., 2009). However, another study reported that children with ALL experienced lower physical HRQoL during early treatment when compared to children with brain tumors (Landolt et al., 2006). Across studies that utilized the PedsQL-Generic scale, 1 study identified children with osteosarcoma as having the poorest HRQoL (Hinds et al., 2009).
Three studies examined the influence of cancer stage/risk and HRQoL in children undergoing curative cancer treatment (de Vries et al., 2008; Penn et al., 2008; Sitaresmi et al., 2008), of which 1 study reported that, at the end of the therapy, children treated on the high-risk arm had significantly lower HRQoL and cognitive problems compared to children on the non–high-risk arm (de Vries et al., 2008).
Only 3 studies included time in treatment or time since diagnosis as a factor influencing HRQoL (Baggott et al., 2011; Barakat et al., 2010; de Vries et al., 2008), with 1 study finding lower HRQoL domain scores in children with ALL at the end of treatment in comparison with 1 year after the initiation of treatment (de Vries et al., 2008). Several studies reported a lower HRQoL in children after diagnosis, intensification, or changes in treatment (Hinds et al., 2009; Penn et al., 2008; Sung et al., 2009; Tremolada et al., 2011). Other studies found a gradual HRQoL improvement in children as they progressed through treatment, with highest HRQoL reported immediately after completion of treatment (Erickson et al., 2011; Houtrow et al., 2012; Penn et al., 2008).
Only 1 study assessed the longitudinal changes in HRQoL during curative cancer treatment (Peeters et al. 2009). In this study, 96 patients treated for ALL were followed over 3 time points during treatment. Time significantly influenced HRQoL, with higher HRQoL being reported as time progressed during treatment, especially in the physical and mental functional domains. These findings were not associated with patient age; children with ALL reported a lower HRQoL than that of the general age-matched population. Less commonly assessed cancer factors included relapse status (Baggott et al., 2011), tumor location (Kuhlthau et al., 2012), hydrocephalus (Penn et al., 2009), and prognosis (Sung et al., 2009).
Cancer Treatment Factors
Six studies assessed type of treatment (chemotherapy, radiotherapy, surgery, or any combination; de Vries et al., 2008; Durmaz et al., 2011; Kuhlthau et al., 2012; Penn et al., 2008; Sung et al., 2009; van Litsenburg et al., 2011). Radiotherapy was a determining factor in 3 studies, but it was not compared to other modalities (Houtrow et al., 2012; Kuhlthau et al., 2012; Penn et al., 2008). Two studies described the HRQoL of children undergoing proton radiotherapy treatment; however, the HRQoL of these children was not compared with that of patients receiving conventional radiotherapy (Houtrow et al., 2012; Kuhlthau et al., 2012). Another study identified radiotherapy to correlate with lower HRQoL in children with brain tumors during the first year of diagnosis in comparison to children who did not receive radiotherapy (Penn et al., 2008). Three studies explored the influence of chemotherapy on HRQoL, of which two found that chemotherapy was negatively correlated with HRQoL in children undergoing curative treatment for cancer (Kuhlthau et al., 2012; Penn et al., 2008). One study found surgery to significantly contribute to a worse HRQoL in children with cancer compared to children who did not receive surgery (Sung et al., 2009).
Treatment intensity was measured in 5 studies (Barakat et al., 2010; Kuhlthau et al., 2012; Landolt et al., 2006; Sitaresmi et al., 2008; Sung et al., 2009), with 3 finding it to be a significant factor contributing to lower HRQoL in children with brain tumors (Kuhlthau et al., 2012), children receiving intensive and complex therapy (Landolt et al., 2006), and children with leukemia during the intensive stage of treatment (Sitaresmi et al., 2008). The remaining 2 studies did not find a significant association between intensity of treatment or total number of treatment combinations (chemotherapy+ radiation + surgery + bone marrow transplantation) and HRQoL (Barakat et al., 2010; Sung et al., 2009).
Child Factors
Age was a frequently assessed factor that influences HRQoL in children and adolescents undergoing curative cancer treatment. Sixteen studies assessed age and HRQoL (af Sandeberg et al., 2008; af Sandeberg et al., 2010; Baggott et al., 2011; Barakat et al., 2010; de Vries et al., 2008; Eiser et al., 2005; Hullmann et al., 2010; Kuhlthau et al., 2012; Landolt et al., 2006; Penn et al., 2008; Shankar et al., 2005; Sitaresmi et al., 2008; Sung et al., 2009; Tremolada et al., 2011; Zareifar et al., 2012). However, these studies provided limited evidence for the nature of the association between age and HRQoL. Only 5 studies found age to be significantly associated with HRQoL during treatment (af Sandeberg et al., 2010; Shankar et al., 2005; Sitaresmi et al., 2008; Sung et al., 2009; Tremolada et al., 2011). Young children generally reported higher procedural anxiety and treatment anxiety than did adolescents (Sitaresmi et al., 2008), whereas older children reported higher social HRQoL and communication than did younger children (af Sandeberg et al., 2008). Two studies reported a higher HRQoL with age (Barakat et al., 2010; Sitaresmi et al., 2008), whereas 1 study (Sung et al., 2009) found that younger age was associated with higher reported HRQoL. 11 studies found no association between age and HRQoL in children (af Sandeberg et al., 2008; Baggott et al., 2011; Barakat et al., 2010; de Vries et al., 2008; Eiser et al., 2005; P. Erickson, 2004; Hullmann et al., 2010; Kuhlthau et al., 2012; Landolt et al., 2006; Penn et al., 2008; Zareifar et al., 2012). Notably, however, 4 studies reported that the differences between parent proxy-reports and child self-reports of HRQoL were influenced by age of the child (Barakat et al., 2010; Kuhlthau et al., 2012; Penn et al., 2008; Speyer et al., 2009).
Gender was examined frequently in our review. However, of the 16 studies that examined the influence of gender and HRQoL, only 4 identified gender as a significant factor. In these studies, female gender was consistently associated with a lower HRQoL (af Sandeberg et al., 2010; Landolt et al., 2006; Shankar et al., 2005; Sung et al., 2009).
Three studies assessed the impact of race on HRQoL (Baggott et al., 2011; Kuhlthau et al., 2012; Shankar et al., 2005), of which only one study found an association between race and HRQoL in children undergoing curative cancer treatment (Shankar et al., 2005), reporting that non-white children had lower HRQoL than white children.
Other less frequently assessed factors were related to the child functional status, including the child’s IQ status, functional independence (Kuhlthau et al., 2012), position in family (Sitaresmi et al., 2008), functional status (Landolt et al., 2006), and personality traits (De Bolle et al., 2008). Of these factors, higher IQ score, higher functional independence, higher functional status scores, and lower neuroticism scores were significant predictors of higher HRQoL.
Family Factors
Ten studies explored the association between family factors and HRQoL in children undergoing curative treatment. These factors included mothers’ quality of life (Eiser et al., 2005), parental age (Barakat et al., 2010; Hullmann et al., 2010; Sung et al., 2009), parental gender (Sung et al., 2009), parental education (Hullmann et al., 2010; Sitaresmi et al., 2008; Sung et al., 2009), marital status (Sung et al., 2009), parental depression (Penn et al., 2008), parental work (Sung et al., 2009), parental chronic condition (Sung et al., 2009), parental anxiety (Penn et al., 2008), family’s socio-economic status (Landolt et al., 2006; Penn et al., 2008; Sitaresmi et al., 2008; Sung et al., 2009; Zareifar et al., 2012), sociodemographic risk (Barakat et al., 2010), number of siblings (af Sandeberg et al., 2010; Sung et al., 2009), family roles (Barakat et al., 2010), parental care (Barakat et al., 2010), parental overprotection (Barakat et al., 2010; Hullmann et al., 2010), family burden (Houtrow et al., 2012), perceived child vulnerability (Hullmann et al., 2010), parental psychological adjustment (Landolt et al., 2006), family function (Barakat et al., 2010; Penn et al., 2008), family coping and impact (Penn et al., 2008), family support (Penn et al., 2008), and first parenting experience (Sung et al., 2009). Of these family-related factors, 2 studies described better family functioning, involved parental care and bonding to be associated with higher physical domain HRQoL (Barakat et al., 2010; Penn et al., 2008). Family resources were the strongest predictor of psychosocial HRQoL (Barakat et al., 2010), with higher family socioeconomic status and annual income being significantly associated with higher HRQoL in children with cancer (Penn et al., 2008; Tremolada et al., 2011). Children whose mothers reported a higher quality of life had a higher HRQoL themselves (Eiser et al., 2005). Higher parental overprotection and perceived child vulnerability were related to a lower HRQoL in the parent proxy-report of the child (Barakat et al., 2010; Hullmann et al., 2010; Tremolada et al., 2011). Perceived child vulnerability was a negative factor that resulted in parental overprotection and a lower reported HRQoL (Hullmann et al., 2010).
Community Factors
Three studies addressed the association of community factors and reported HRQoL in children undergoing curative cancer treatment (af Sandeberg et al., 2008; Stevens et al., 2006; Tremolada et al., 2011). Two of these studies examined the difference in HRQoL between children treated at home versus those treated in a hospital setting (Stevens et al., 2006; Tremolada et al., 2011). Stevens et al. (2006) found that HRQoL in the early stages of treatment was higher in children treated at home; however, these children reported higher distress as treatment progressed. Tremolada et al. (2011) reported higher HRQoL in children whose parents had developed a trusting relationship with the staff. af Sandeberg et al. (2008) identified a positive correlation between school attendance and higher HRQoL in children undergoing curative cancer treatment.
Discussion
Information regarding factors that influence the HRQoL in children undergoing curative cancer treatment is limited. This review of literature attempts to collect and identify patterns of influential factors on HRQoL in this population. We found that for children and adolescents with cancer, cancer diagnosis and cancer treatment most frequently influence HRQoL, which is consistent with results from a previous report (Klassen et al., 2011). Previous literature reviews combined children under curative cancer treatment and childhood cancer survivors, with identified factors being different between the groups (Eiser et al., 2005). This review identifies factors that influence HRQoL during treatment and includes cancer diagnosis, female gender, age, treatment intensity, type of treatment, and time since diagnosis. These factors can assist clinicians and researchers to develop and incorporate interventions to improve patient-reported outcomes in children with cancer.
Although few studies have assessed family and community factors, we found that these factors significantly influence HRQoL. The small number of studies assessing family and community factors can be attributed to the difficulty in obtaining data related to family and community demographics. In addition, most studies focus on treatment and cancer factors, which can be easily documented within the context of the cancer experience in a clinical setting. However, in our review, the results from studies evaluating family and community factors highlight the importance of evaluating the influence of these factors on the HRQoL of children undergoing curative cancer treatment. This trend of negligible reporting of family and community outcomes is consistent with another review (Klassen et al., 2011).
Although not part of the study aim, we identified studies that described interventions to improve HRQoL in children undergoing curative cancer treatment. Five studies reported the effectiveness of interventions, including treating patients at home versus a hospital setting (Stevens et al., 2006), adapting physical activity (Speyer et al., 2009), employing Chinese alternative medicine (Shi, Tian, Zhu, Wang, & Qin, 2011), engaging in creative arts therapy (Madden, Mowry, Gao, Cullen, & Foreman, 2010), and increasing school attendance (af Sandeberg et al., 2008). All these studies identified their respective interventions as factors significantly influencing HRQoL in children with cancer. Our previous study has shown that establishing a sense of normalcy and ability to perform usual activities can help children undergoing curative cancer therapy develop a better treatment experience (Momani et al., 2014). Thus, interventions that help establish this sense of normalcy—being at home, physical activity, and school attendance—are recommended to improve the HRQoL of children most vulnerable to low HRQoL during curative cancer treatment. Such interventions may be most valuable when implemented early in treatment when children experience the lowest HRQoL.
An important trend in recent HRQoL research is the emphasis on child self-reported HRQoL measures. Eighteen studies in our review included child self-reported HRQoL measures. Some of the reviewed studies also highlighted the significant differences between parent-proxy reports of children’s HRQoL and the children’s self-reporting of their HRQoL. Four studies in our review identified older age as a predictor of larger differences between self-reported and proxy-reported HRQoL (Barakat et al., 2010; Kuhlthau et al., 2012; Penn et al., 2008; Speyer et al., 2009). Furthermore, levels of agreement vary across different HRQoL domains and can be influenced by the parents’ own quality of life (Cremeens, Eiser, & Blades, 2006). These documented differences between self-reported and proxy-reported HRQoL measures, in addition to the development of age-appropriate HRQoL scales, may explain the increase in studies that rely on self-reported measures either solely or in addition to parent-self reported measures.
The use of consistent instruments for HRQoL and cancer-related symptoms is important in building a consensus of factors that influence HRQoL in children undergoing curative treatment. Adapting a consistent measurement of HRQoL will also assist in drawing comparisons between studies and patient populations. The PedsQL instruments have been reported as reliable and valid in children and provide a population norm that can be used to compare the HRQoL of children with cancer and school-age children. However, these instruments do not allow for comparison of HRQoL assessment of childhood cancer survivors into adulthood. More recently developed instruments such as the National Institute of Health’s Patient Reported Outcomes Measurement Information System (PROMIS) offer standardized, valid, and clinically feasible HRQoL assessments that may be used across all ages and feasible for comparison across time (Garcia et al., 2007; Hinds et al., 2012).
Our review identified limitations of the research on HRQoL in children undergoing curative cancer treatments. The studies included in our review identified factors related to HRQoL in specific pediatric diagnoses (dexamethasone in ALL, radiotherapy in CNS tumors). Most studies only described HRQoL with a cross-sectional design and did not consider the important factor of change over time. Most studies had small sample sizes, making it difficult to identify significant results or analyze data with an advanced analytical approach. This review also highlights the inconsistency in the use of instruments for measuring factors that influence HRQoL, which limits the ability to compare and interpret findings across studies. As an example, the most frequently used generic instrument, the PedsQL-Generic, identifies 4 domains of HRQoL—physical, social, emotional, and school—whereas other HRQoL instruments do not consistently include the same domains. This discrepancy can hinder the understanding of factors that impact HRQoL in children undergoing curative cancer treatment. Also, assessments of demographics were not consistent across studies. Studies variably assessed age at diagnosis, age at completion of therapy, or included a description of age without a specific timing. Similarly, some studies measured time since diagnosis, whereas others measured time since end of chemotherapy. Socioeconomic status was also not consistently measured across studies. Finally, our review only included studies conducted after 2005, with the intent of studying HRQoL associated with treatment modalities introduced over the past decade. This approach aimed at capturing the effect of current treatment modalities and approaches that differ significantly from earlier treatments for children with cancer. Our focus on children undergoing curative cancer treatment excluded patients with relapsed disease and those at the end of life, as factors that influence HRQoL in this population may be different from children undergoing curative cancer treatment.
Conclusion
In this review of the measurement and assessment of HRQoL in children undergoing curative cancer treatment, we found that treatment and cancer factors were the most significant factors to influence HRQoL. Demographics, time, community, and family factors were also important contributing factors to HRQoL but were less frequently measured in children undergoing curative cancer treatment. Our review suggests wide variability in reporting and identifying factors that influence HRQoL in children with cancer. Better designed studies with large sample sizes are required to understand the dynamic nature of HRQoL in children undergoing curative cancer treatment.
 Continuing Education Credit
Continuing Education Credit
The Journal of Pediatric Oncology Nursing is pleased to offer the opportunity to earn pediatric hematology/oncology nursing continuing education credit for this article online. Go to www.aphon.org and select “Continuing Education.” There you can read the article again or go directly to the posttest assessment. The cost is $15 for each article. You will be asked for a credit card or online payment service number.
The posttest consists of 11 questions based on the article, plus several assessment questions (e.g. how long did it take you to read the article and complete the posttest?). A passing score is 8 out of 11 questions correct on the posttest and completion of the assessment questions yields one hour of continuing education in pediatric hematology/oncology nursing for each article.
The Association of Pediatric Hematology/Oncology Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.