
Abstract
This study evaluated the potential impact of an online spiritual care educational program on pediatric nurses’ attitudes toward and knowledge of spiritual care and their competence to provide spiritual care to children with cancer at the end of life. It was hypothesized that the intervention would increase nurses’ positive attitudes toward and knowledge of spiritual care and increase nurses’ level of perceived spiritual care competence. A positive correlation was expected between change in nurses’ perceived attitudes toward and knowledge of spiritual care and change in nurses’ perceived spiritual care competence. A prospective, longitudinal design was employed, and analyses included one-way repeated-measures analysis of variance, linear regression, and partial correlation. Statistically significant differences were found in nurses’ attitudes toward and knowledge of spiritual care and nurses’ perceived spiritual care competence. There was a positive relationship between change scores in nurses’ attitudes toward and knowledge of spiritual care and nurses’ spiritual care competence. Online spiritual care educational programs may exert a lasting impact on nurses’ attitudes toward and knowledge of spiritual care and their competence to provide spiritual care to children with cancer at the end of life. Additional studies are required to evaluate the direct effects of educational interventions patient outcomes.
Introduction
There has been a dramatic increase of interest regarding spiritual care in the context of end-of-life clinical practice. Experts concur that a holistic focus that addresses the needs of the mind, body, and spirit is paramount throughout the disease trajectory (Puchalski et al., 2009). Holistic nursing care embraces the physical, psychological, and spiritual needs of the patient at the end of life, as well as of the family, with a focus placed on providing support, reducing suffering, and enhancing quality of life (Campion, 2011). Yet there are distinct barriers in education that lead many nurses to feel unprepared to address patients’ spiritual needs (Smith & Gordon, 2009).
Education regarding the art of spiritual care must begin with the meaning of spirituality. Creation of an overarching definition of spirituality is extraordinarily challenging due to the unique spiritual needs, values, and beliefs of each individual (Hickey et al., 2008). The construct of spirituality depicts an individual’s personal beliefs, principles, and experiences of transcendence, while also encompassing a search for meaning and purpose in life and death (Emblem, 1992). Spirituality is considered a dynamic, individualized process that unifies the mind, body, and spirit, providing connections with others, God, or a supreme being (Meraviglia, 1999). An important aspect of spirituality for some individuals is religion. Religion, a structured expression of beliefs, doctrines, practices, and rituals held by a community to connect to a higher power, may serve as a means for expression and enrichment of spirituality (Elkins & Cavendish, 2004; Emblem, 1992; McEvoy, 2000).
Spiritual care involves nurses’ facilitation of spirituality through purposeful monitoring and compassionate response to patients’ expressions of spiritual needs, with the goal of assisting individuals to find meaning, connectedness, and peace (Burkhart & Hogan, 2008). The nursing process provides an organizing framework for the provision of spiritual care and includes assessment of spiritual needs, diagnosis, planning, implementation of spiritual care interventions, and evaluation of the efficacy of those interventions (Greenstreet, 1999). While a tremendous amount of work still needs to be done in evaluating the effects of spiritual care for children, research focused on spiritual care in the adult oncology population has found relationships between spiritual care and important patient outcomes, including improved quality of life, enhanced satisfaction with patient care, increased use of hospice services, decreased use of aggressive medical interventions at the end of life, and diminished medical costs (Balboni et al., 2010; Balboni et al., 2011; Williams, Meltzer, Arora, Chung, & Curlin, 2011).
Spiritual care education must inform pediatric oncology nurses about how to best integrate the attributes of spiritual care for a child with cancer at the end of life: Nurses must assess the child’s spiritual care needs, aid the child to find hope, assist the child to express feelings and concerns, guide the child to strengthen relationships, help the child be remembered, and assist the child to find meaning and purpose (Petersen, 2014). Comprehensive spiritual care education must be guided by research, theory, and guidance from the experts. In pediatric oncology, these experts are the children who are at the end of life and their families. Spiritual care education is not consistently provided in nursing curricula, so it is important to investigate efficient, cost-effective ways of providing this education to practicing nurses.
This study addressed a substantial gap in the literature, for there have been no studies to determine the potential impact of a spiritual care educational initiative on pediatric oncology nurses’ attitudes toward and knowledge of spirituality/spiritual care and their perceived competence to provide spiritual care to children with cancer who are at the end of life. In addition, the relationship between nurses’ attitudes toward and knowledge of spirituality/spiritual care and nurses’ perceived spiritual care competence was evaluated.
Materials and Methods
This study employed a prospective, longitudinal design. Participants completed an online educational program. Data were collected at baseline prior to participation in the educational program (Time Point 1), after a participant’s completion of the program (Time Point 2), and 3-months after a participant’s completion of the program (Time Point 3).
Participants
Participants included pediatric nurses who provide direct care to children with cancer. An invitation to participate in the study was sent to members of the Association of Pediatric Hematology/Oncology Nurses (APHON) by e-mail or through in-person invitation from the primary investigator, who attended APHON local chapter meetings. Eligible participants were required to have Internet access and to provide care to children with cancer.
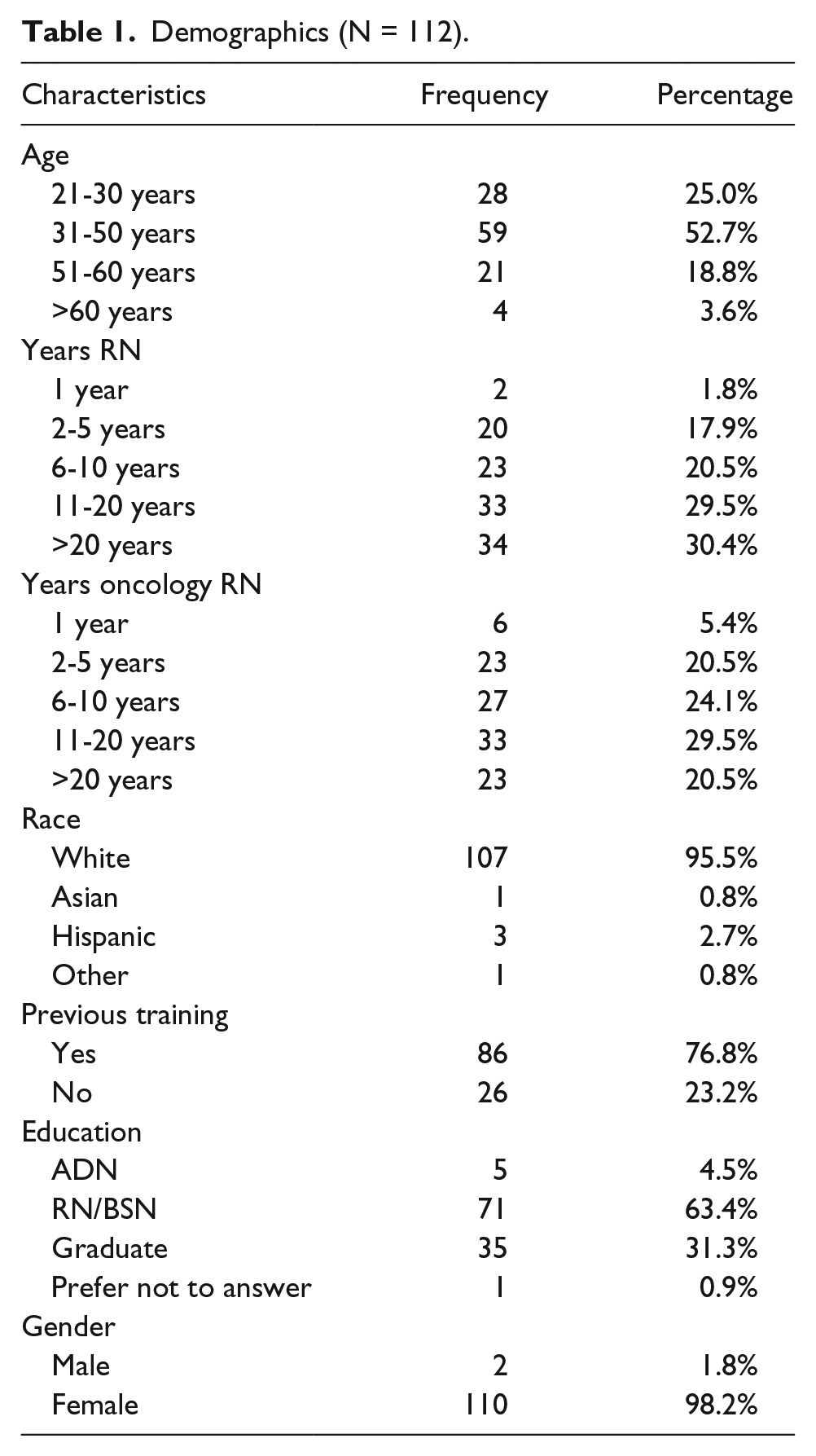
A priori power analysis using G*Power 3 and review of sample calculation tables indicated that a sample size of at least 60 to 80 participants would be optimal to ensure adequate power to detect differences (Faul, Erdfelder, Laang, & Buchner, 2010). The sample size was based on a function of power (.80) with a moderate effect size (.25) of the intervention on dependent variables, an assumption of a .5 correlation between repetitive measures and the α level of .05. Previous longitudinal studies of the effects of spiritual care educational programs experienced rates of attrition of up to 39% (Meredith, Murray, Wilson, Mitchell, & Hutch, 2012; van Leeuwen, Tiesinga, Middel, Post, & Jochemsen, 2008; Wasner, Longaker, Fegg, & Borasio, 2005). Of the 200 nurses who provided written informed consent to participate in this study, 112 participants completed the educational program and the surveys at all 3 time points (44% attrition). Demographic data for these participants are provided in Table 1.
Demographics (N = 112).
Intervention
The intervention involved a 3-hour online self-study program focused on spiritual care of a child with cancer at the end of life, with asynchronous interaction in an online discussion forum. Previous studies demonstrated the efficacy of online administration for spiritual care educational programs (Burkhart, Schmidt, & Hogan, 2011; Ellman et al., 2012). The principal investigator developed the theory-driven spiritual care educational program with the assistance of numerous mentors and content experts. Educational content was based on extensive review of the nursing, medical, and theological literature; content from the National Consensus Conference Report “Improving the Quality of Spiritual Care as a Dimension of Palliative Care” (Puchalski et al., 2009); interviews with spirituality and palliative care experts; and discussion with the children with cancer and their parents.
Content areas of the educational program focused on (1) the definition of spirituality, (2) attributes of spiritual care for a child with cancer at the end of life, (3) goals of spiritual care for children and their families, (4) Fowler’s stages of faith and Erikson’s theory of psychosocial development as guiding frameworks, (5) techniques for therapeutic communication, (6) spiritual assessment tools, and (7) use of the nursing process to guide the provision of spiritual care (Erikson, 1959; Fowler, 1981). Content included readings, videos, discussions, case studies, a poignant blog written by a dying young woman, and extensive online discussions. A voiceover lecture highlighted the report of the Consensus Conference: Improving the Quality of Spiritual Care as a Dimension of Palliative Care (Puchalski et al., 2009). Another voiceover lecture shared the results of a concept analysis on spiritual care of the child with cancer at the end of life, with case studies, a documentary, and videos to examine the attributes of spiritual care through the experiences of children facing the end of life (Petersen, 2014). Video interviews, including “Tales of Hope from a Hospice Chaplain” and “Lessons Learned,” offered enlightening stories of the benefits of spiritual care for children at the end of life from the perspectives of a hospice chaplain and an 11-year old boy who was nearing the end of life. An online documentary, My Last Days: Meet Zac Sobiech, shared the inspiring story of an adolescent’s quest to express his feelings through music, be remembered by his many friends and family, and find meaning in his life and death. To maximize critical thinking, study participants were challenged to apply the knowledge they gained through interactive discussion board postings and reflection exercises.
Instruments
Demographics
Participants provided information regarding their age, gender, race, educational level, previous spiritual care or palliative care education, years of nursing experience, and years of pediatric oncology experience.
Spiritual Care Competence Scale
The Spiritual Care Competence Scale (SCCS), a 27-item 5-point Likert-type instrument, is a reliable and valid measure of nurses’ perceived spiritual care competence (van Leeuwen, Tiesinga, Middel, Post, & Jochemsen, 2009). A higher score indicates a higher perceived level of competence to provide spiritual care to a patient. The instrument has 6 subscales: Assessment and Implementation of Spiritual Care, Professionalization and Improving the Quality of Spiritual Care, Personal Support and Patient Counseling, Referral to Professionals, Attitude Toward Patient Spirituality, and Communication. The scale has shown strong construct validity, with excellent overall reliability (Cronbach’s α of .9; Costello, Atinaja-Faller, & Hedberg, 2012). In previous studies, internal consistency for the instrument subscales ranged from .56 to .82; all 6 subscales were retained during the instrument’s development due to interitem correlations of .25 or more, evidencing a homogeneous instrument (van Leeuwen et al., 2009). In this study population, consistent Cronbach α values were found over all time points for the instrument, with values between .92 and .94, with mean interitem correlations between .30 and .37.
Spirituality and Spiritual Care Rating Scale
The Spirituality and Spiritual Care Rating Scale (SSCRS) is a 17-item instrument that employs a 5-point Likert-type scale to explore nurses’ attitudes toward and knowledge of spirituality and spiritual care. The SSCRS has 4 factor-based subscales: Spirituality, Spiritual Care, Religiosity, and Personalized Care. The tool has exhibited an acceptable level of reliability, with documented Cronbach’s α values between .64 and .71 for the overall instrument (McSherry et al., 2002; Wallace & O’Shea, 2007). Reported reliability coefficients for the subscales range between .65 and .77 (McSherry et al., 2002). In this study population, consistent Cronbach α values were found over all time points for the instrument, with values between .78 and .81 and mean interitem correlations between .22 and .26.
Procedures
University institutional review board approval was obtained prior to initiation of the study. Prior to data collection, the principal investigator obtained written, informed consent from participants after screening for eligibility. The study involved minimal risk to participants; the researcher was aware of the potential risk for participants’ spiritual distress due to the emotional subject content, so a hospice chaplain was available for consult. Strict confidentiality and anonymity were maintained through use of the university’s password-protected online course management system to administer the program. De-identified subject data were entered into a secure, encrypted computer for analysis using SPSS version 21.0. On completion of instruments at all 3 time points, a participant received a $50 gift card by e-mail to show appreciation for their time.
Data Analyses
Descriptive statistics were run on demographic factors. When inferential analyses were employed, pairwise deletion was used for missing data, thereby maximizing power and sample size for each analysis (Pallant, 2010). As a result, sample size for each subsequent analysis varied. One-way repeated-measures analysis of variance (RM-ANOVA) evaluated the effect of the online spiritual care educational program on nurses’ perceived spiritual care competence, as measured by the SCCS. Scores on the SCCS were compared at 3 time points: Time Point 1 (baseline before a participant’s completion of the program); Time Point 2 (immediately after a participant’s completion of the program); and Time Point 3 (3 months after a participant’s completion of the program). The Kolmogorov-Smirnov test of normality and the normal Q-Q plots indicated a normal distribution of the data. The assumption of sphericity was violated in this specific analysis, but the multivariate statistics from the analysis could safely be used since multivariate statistics do not require an assumption of sphericity. As a result, the multivariate Greenhouse-Geisser results were used to determine statistical significance in this analysis (Pallant, 2010).
RM-ANOVA was employed to evaluate the potential impact of the online spiritual care education program on nurses’ attitudes toward and knowledge of spirituality/spiritual care, as measured by the SSCRS. Scores were compared at 3 time points: Time Point 1, Time Point 2, and Time Point 3. Review of the Kolmogorov-Smirnov test of normality and the normal Q-Q plots indicated that the assumption of normality was met for this analysis. The assumption of sphericity was also met.
A bivariate linear regression was performed to evaluate if the amount of change in nurses’ perceived spiritual care competence (as measured by the SCCS) over time could be predicted from the amount of change in nurses’ perceived knowledge and attitudes toward spirituality/spiritual care (as measured by the SSCRS) over time. Change scores were calculated to show the difference in scores from Time Point 2 to Time Point 1. Preliminary data screening indicated that scores on both variables were normally distributed. A scatterplot showed a reasonably linear relationship between variables, with a bivariate normal distribution. There were 3 bivariate outliers noted on the scatterplot, and the analysis was run with and without the outliers, showing congruent results. Results are reported from the analysis with outliers removed.
Partial correlations were completed to explore the relationship between change scores in nurses’ level of knowledge and attitudes toward spirituality/spiritual care (as measured by the SSCRS) and change scores in nurses’ level of spiritual care competence (as measured by the SCCS) while controlling for (1) overall years of experience as a nurse or (2) years of experience in pediatric oncology. Preliminary analyses were completed to ensure that there were no violations of the assumptions of normality, linearity, and homoscedasticity.
Results
Pediatric Oncology Nurses’ Level of Spiritual Care Competence
A one-way RM-ANOVA compared the mean scores of nurses’ perceived level of spiritual care competence, as measured by the SCCS at Time Point 1, Time Point 2, and Time Point 3. There was a statistically significant difference in level of spiritual care competence over time, Wilks’s Λ = .36, F(1.643, 97) = 127.78 (p < .0005; see Table 2). The multivariate partial η2 of .57 evidenced a very large effect over time on nurses’ perceived level of competence to provide spiritual care to children with cancer at the end of life (Cohen, 1988). While the statistically significant F test indicated that the null hypothesis was rejected and that there were statistically significant differences in the mean scores of the dependent variable across the 3 time points, it did not specify where the difference was specifically found. To deconstruct the differences and make more precise conclusions, post hoc (a posteriori) comparisons were completed. Because 3 analyses were run to compare means scores at the 3 time points of data collection, a Bonferroni-adjusted significance level of .017 (0.05/3) was calculated, with the ultimate goal of conservatively minimizing the risk of Type I error (Pallant, 2010). Statistically significant differences were found between participants’ mean scores on the SCCS from Time Point 2 to Time Point 1, from Time Point 3 to Time Point 1, and from Time Point 3 to Time Point 2. See Table 3 for the pairwise comparisons.
One-Way RM-ANOVA SCCS Total Score.
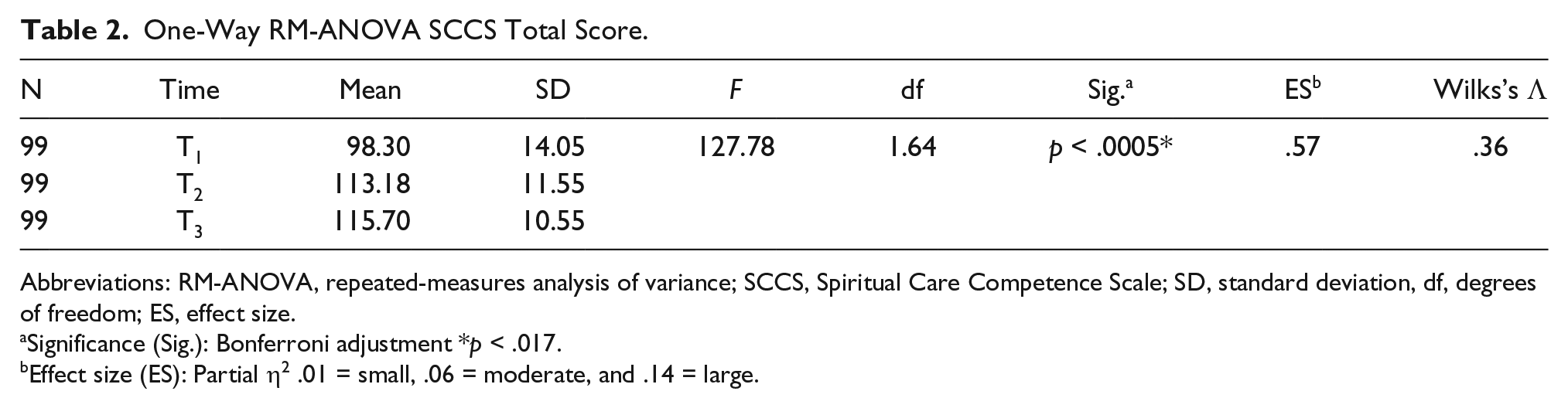
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SCCS, Spiritual Care Competence Scale; SD, standard deviation, df, degrees of freedom; ES, effect size.
Significance (Sig.): Bonferroni adjustment *p < .017.
Effect size (ES): Partial η2 .01 = small, .06 = moderate, and .14 = large.
One-way RM-ANOVA SCCS Total Score Pairwise Comparisons.
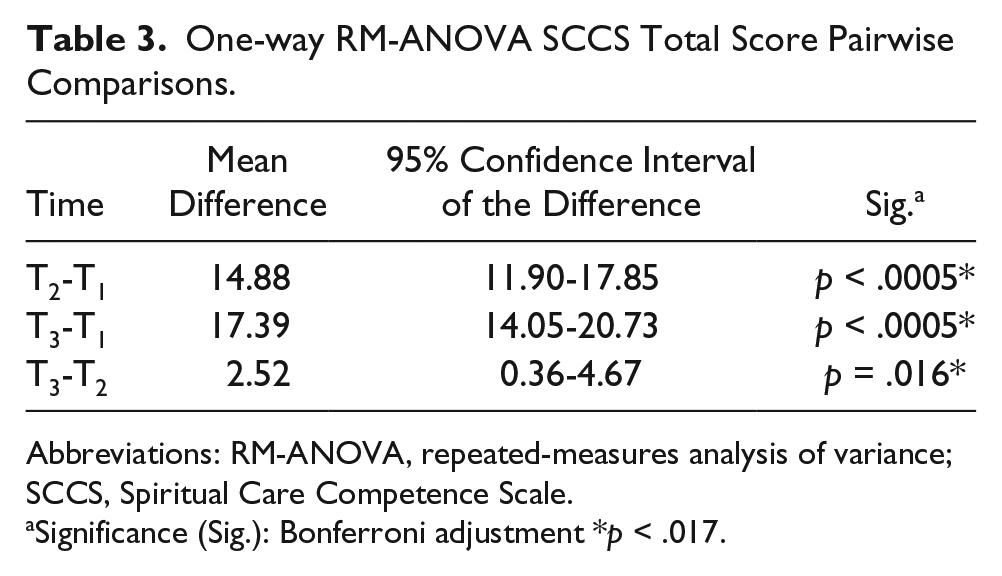
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SCCS, Spiritual Care Competence Scale.
Significance (Sig.): Bonferroni adjustment *p < .017.
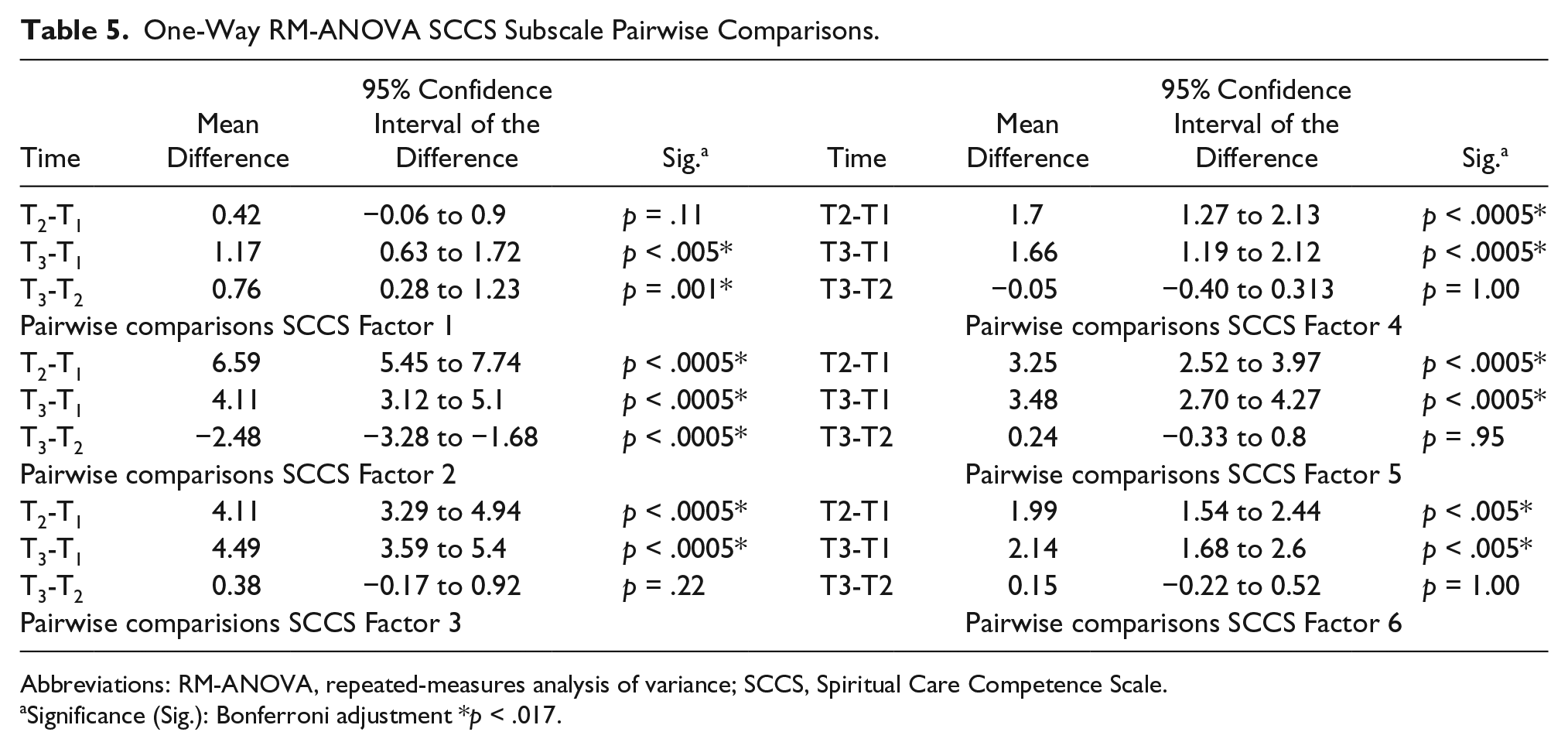
One-way RM-ANOVA analyses were conducted for the 6 SCCS subscales, with statistically significant differences found across time for all 6 subscales, with moderate to very large effect sizes noted. See Tables 4 and 5 for the results for the SCCS subscales and the resultant pairwise comparisons.
One-Way RM-ANOVA SCCS Subscales: Comparison of Baseline Scores (T1), Scores After Completion of Intervention (T2), and Scores 3 Months After Completion of Intervention (T3).
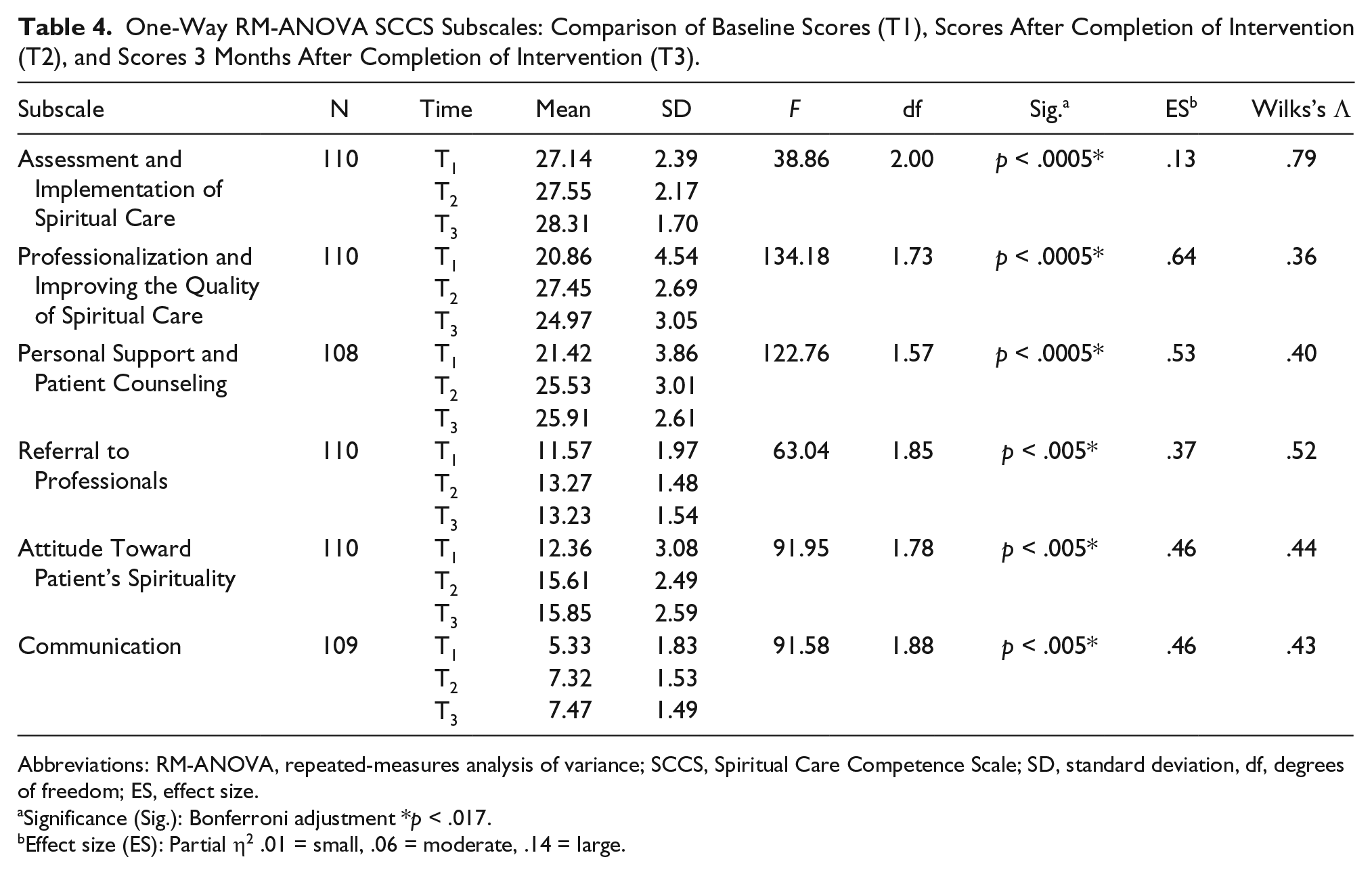
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SCCS, Spiritual Care Competence Scale; SD, standard deviation, df, degrees of freedom; ES, effect size.
Significance (Sig.): Bonferroni adjustment *p < .017.
Effect size (ES): Partial η2 .01 = small, .06 = moderate, .14 = large.
One-Way RM-ANOVA SCCS Subscale Pairwise Comparisons.
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SCCS, Spiritual Care Competence Scale.
Significance (Sig.): Bonferroni adjustment *p < .017.
Pediatric Oncology Nurses’ Attitudes Toward and Knowledge of Spirituality and Spiritual Care
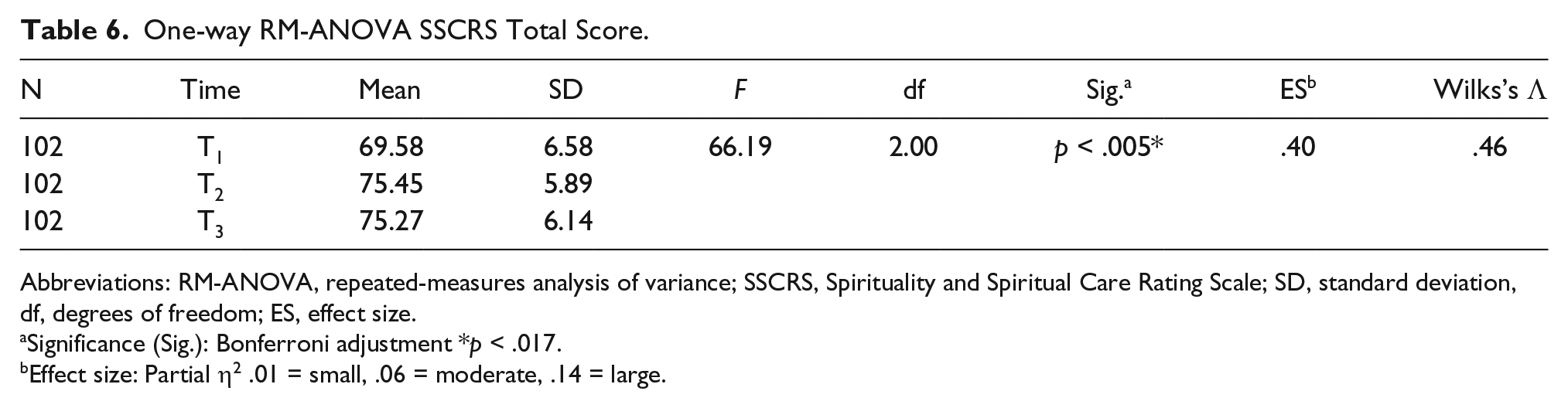
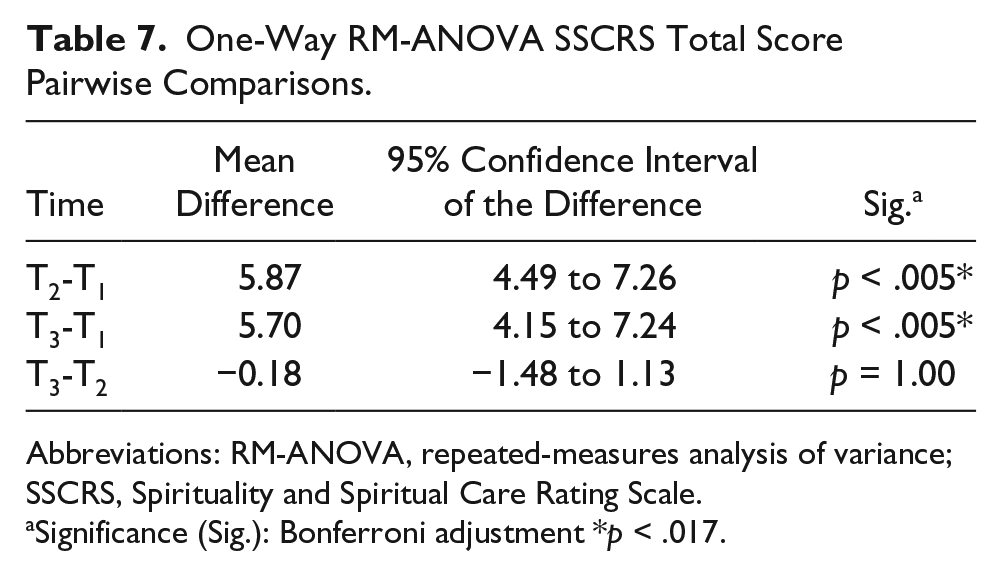
A one-way RM-ANOVA was conducted to compare mean scores on nurses’ perceived attitudes toward and knowledge of spirituality/spiritual care, as measured by the SSCRS at Time Point 1, Time Point 2, and Time Point 3. There was a statistically significant difference over time, Wilks’s Λ = .46, F(2, 100) = 66.19 (p < .0005; see Table 6). The multivariate partial η2 of .40 evidenced a very large effect on nurses’ level of knowledge and attitudes toward spirituality and spiritual care (Cohen, 1988). To identify where the differences were located and make more precise conclusions, post hoc comparisons were conducted. A Bonferroni-adjusted significance level of .017 (0.05/3) was calculated to conservatively minimize the risk of Type I error (Pallant, 2010). Statistically significant results were identified in the differences in mean scores on the SSCRS from Time Point 2 to Time Point 1 and from Time Point 3 to Time Point 1. See Table 7 for the pairwise comparisons.
One-way RM-ANOVA SSCRS Total Score.
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SSCRS, Spirituality and Spiritual Care Rating Scale; SD, standard deviation, df, degrees of freedom; ES, effect size.
Significance (Sig.): Bonferroni adjustment *p < .017.
Effect size: Partial η2 .01 = small, .06 = moderate, .14 = large.
One-Way RM-ANOVA SSCRS Total Score Pairwise Comparisons.
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SSCRS, Spirituality and Spiritual Care Rating Scale.
Significance (Sig.): Bonferroni adjustment *p < .017.
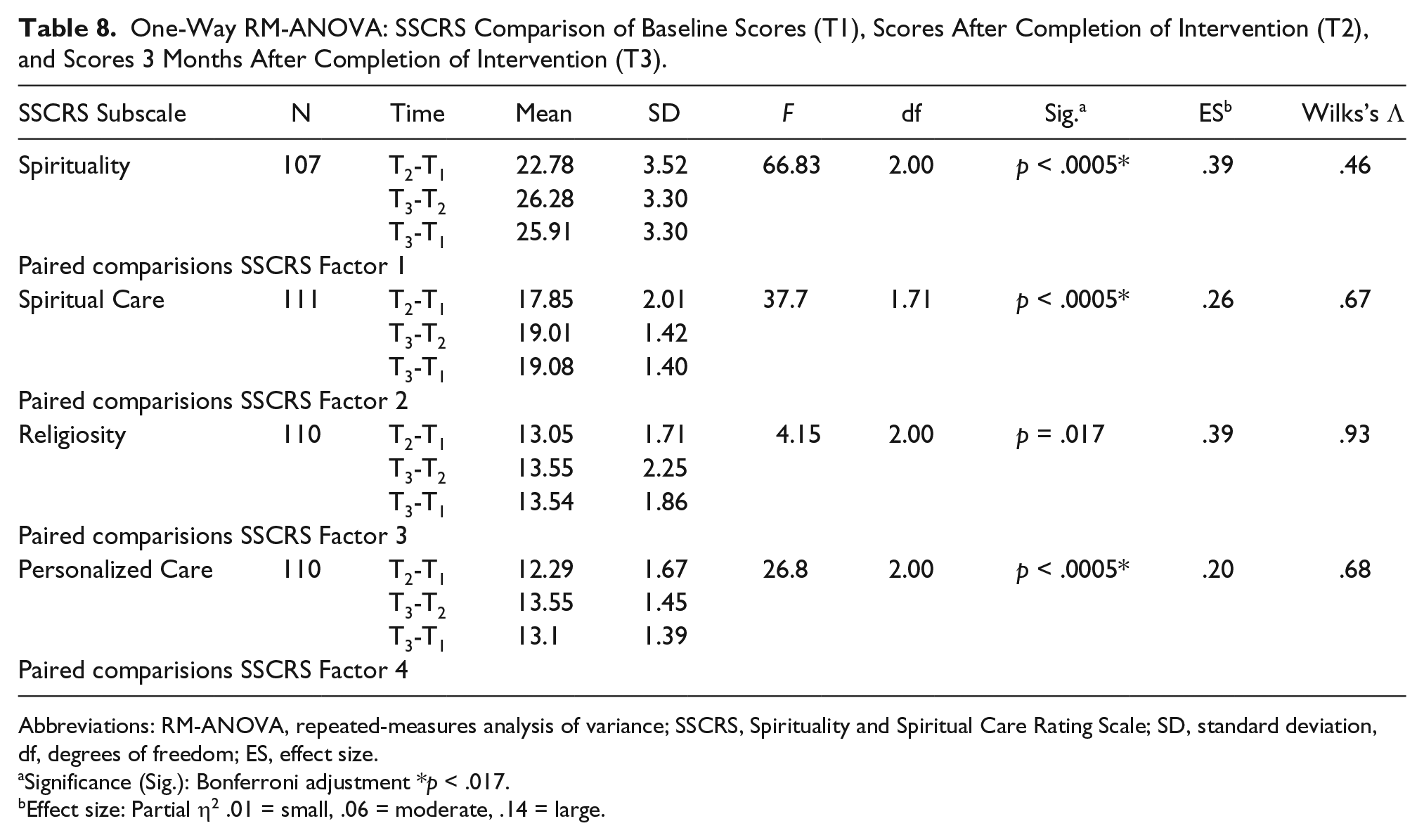
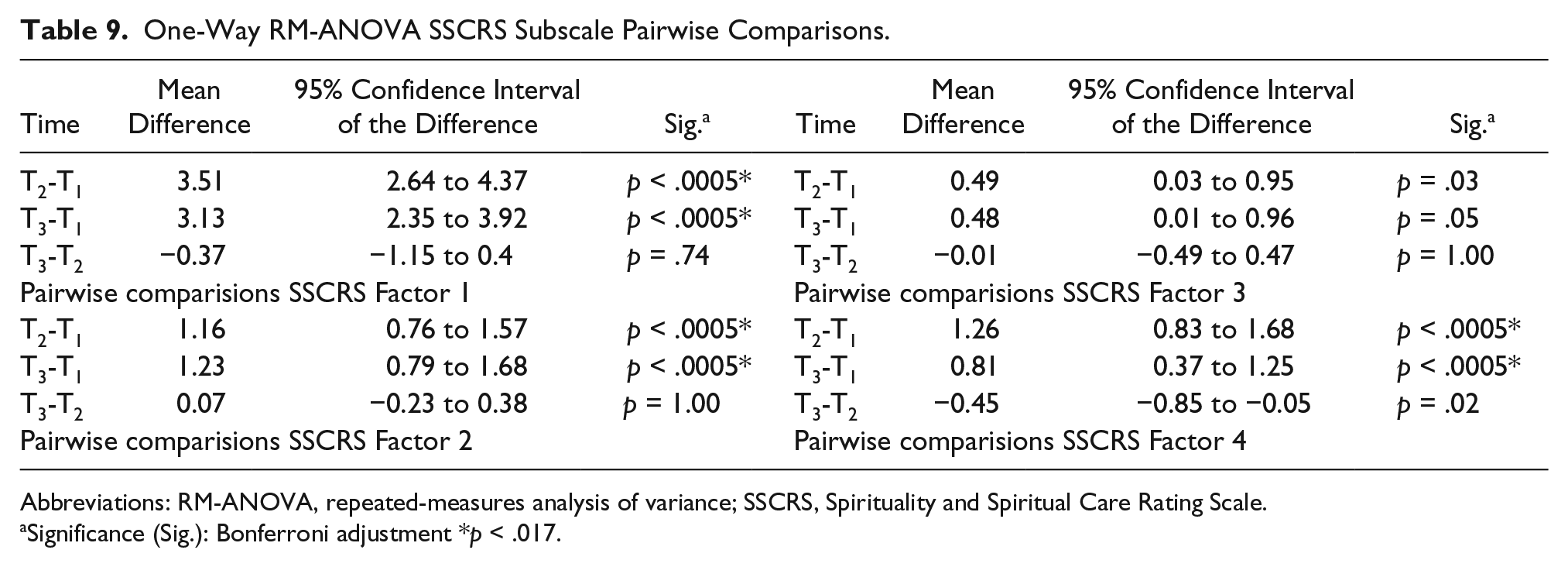
One-way RM-ANOVA analyses were also conducted for the SSCRS subscales, with statistically significant differences identified over time for 3 of the 4 subscales (Spirituality, Spiritual Care, and Personalized Care). The mean difference in scores on the Religiosity subscale, with a p = .017, was just outside of the conservative significance level of p < .017. See Tables 8 and 9 for the RM-ANOVA results and pairwise comparisons for the SSCRS subscales.
One-Way RM-ANOVA: SSCRS Comparison of Baseline Scores (T1), Scores After Completion of Intervention (T2), and Scores 3 Months After Completion of Intervention (T3).
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SSCRS, Spirituality and Spiritual Care Rating Scale; SD, standard deviation, df, degrees of freedom; ES, effect size.
Significance (Sig.): Bonferroni adjustment *p < .017.
Effect size: Partial η2 .01 = small, .06 = moderate, .14 = large.
One-Way RM-ANOVA SSCRS Subscale Pairwise Comparisons.
Abbreviations: RM-ANOVA, repeated-measures analysis of variance; SSCRS, Spirituality and Spiritual Care Rating Scale.
Significance (Sig.): Bonferroni adjustment *p < .017.
Relationship Between Change in Nurses’ Perceived Attitudes Toward and Knowledge of Spirituality/Spiritual Care and Change in Nurses’ Perceived Spiritual Care Competence
A linear regression evaluated the relationship between change in nurses’ perceived attitudes toward and knowledge of spirituality/spiritual care and change in nurses’ perceived spiritual care competence. The relationship between the total change scores (calculated from Time Point 1 to Time Point 2) in nurses’ attitudes toward and knowledge of spirituality/spiritual care and the total change scores in nurses’ level of spiritual care competence (calculated from Time Point 1 to Time Point 2) was statistically significant: r = .32, p = .001. This positive correlation indicated a moderate relationship and signified that an increase in the amount of change in nurses’ attitudes toward and knowledge of spirituality/spiritual care was associated with an increase in the amount of change in nurses’ perceived spiritual care competence over time. The regression equation was Y′ = 11.93 + 0.62X. The r2 for this equation was .10, with 10% of the variance in change score for nurses’ perceived spiritual care competence predictable from the change score of nurses’ perceived knowledge and attitudes toward spiritual care. The 95% confidence interval for the slope to predict the dependent variable from the independent variable was 0.25 to 0.99.
A partial correlation was run to test for the impact of participants’ number of years of nursing experience on the correlation between change in nurses’ perceived attitudes toward and knowledge of spirituality/spiritual care and change in nurses’ perceived spiritual care competence. There remained a moderate, positive partial correlation between change scores of nurses’ perceived spiritual care competence and change scores of nurses’ perceived knowledge and attitudes toward spirituality/spiritual care when controlling for participants’ number of years of experience as a nurse, r = .31, p = .002. An inspection of the zero-order correlation (r = .32) indicated that controlling for participants’ number of years of experience as a nurse therefore had a very minimal effect on the strength of the relationship between these 2 variables.
There was a moderate, positive partial correlation between the change scores in nurses’ perceived attitudes toward and knowledge of spirituality/spiritual care and the change scores in nurses’ perceived spiritual care competence when controlling for participants’ years of experience in pediatric oncology, r = .32, p = .001. An inspection of the zero-order correlation (r = .32) indicated that controlling for participants’ number of years of experience in pediatric oncology had no effect on the strength of the relationship between these 2 variables.
Discussion
Professional nursing organizations and accrediting bodies readily acknowledge the importance of addressing patients’ spiritual needs (American Nurses Associations, 2010; International Council of Nurses, 2006; Joint Commission on Accreditation of Healthcare Organizations, 2004; North American Nursing Diagnosis Association, 1999). Still nurses often fail to integrate spiritual care into the overall care of patients and their families. Reasons cited include a lack of knowledge about the effect of quality spiritual care on health outcomes, a failure to recognize patients’ spiritual needs, and a lack of understanding of the best ways to provide spiritual care (Sulmasy, 2006). Spiritual care education for practicing nurses and nursing students is critical if barriers to providing quality spiritual care are to be overcome and national end-of-life care guidelines are to be met. It is through first educating pediatric nurses about how to provide spiritual care to children with cancer at the end of life and their families that future work may be done in investigating the effects of spiritual care on important patient care outcomes, including quality of life, patient satisfaction, use of hospice services, initiation of aggressive medical interventions at the end of life, and medical costs. By assessing and meeting the spiritual needs of children and their families, nurses minimize their spiritual suffering and ensure that potential coping strategies are not lost (O’Shea et al., 2011).
Findings from this study demonstrate the potential impact of an online educational program on pediatric oncology nurses’ perceived attitudes toward and knowledge of spirituality and spiritual care and their level of spiritual care competence. The findings of statistically significant gains over the 3 months after participants’ completion of the educational program interestingly point to the potential importance of application and integration of spiritual care education principles into practice. Statistically significant differences were noted on the SCCS and the SSCRS from Time Point 2 (immediately after a participant’s completion of the program) to Time Point 3 (3 months after a participant’s completion of the program). As a result, the true effects of spiritual care educational programs may need to be reevaluated after allowing time for new knowledge and skills to become fully integrated into practice.
Limitations of the study include use of a convenience sample, lack of a control group, potential for self-report bias and self-selection bias, reliance on self-report of perceptions rather than behavioral measures of effect, and the risk of testing effect with repeated administration of the same instruments. Looking forward, it is important to shift to longitudinal studies that measure retention of effects from spiritual education initiatives over extended periods of time. In addition, it is vital for researchers to comprehensively examine the effects of spiritual care education on nurses’ actual provision of spiritual care in the clinical environment, with reliable and valid measures of resultant patient and family outcomes. To further advance the science, researchers must consider multisite collaborations that will enable the use of randomized controlled trials, for control groups can minimize potential biases and maximize control of potential confounding variables (Meredith et al., 2012; Taylor, Mamier, Bahjri, Anton, & Petersen, 2008).
Spiritual care is a key aspect of comprehensive nursing care for children and their families, from the beginning to the end of life, across all dimensions of the illness trajectory. Spiritual care educational initiatives are crucial if the spiritual domain is to be adequately incorporated into daily patient care. It is by addressing the spiritual needs and available resources that we may ultimately close the gap between theory and practice and maximize the opportunity for dying children and their families to find peace at the end of life.
Footnotes
Acknowledgements
The authors express their sincerest thanks to the Association of Pediatric Hematology/Oncology Nurses for allowing us to recruit participants from organization membership. We are thankful to Barb Ruggeri, Medical College of Wisconsin Librarian, and Martha Jerme, Marquette University Librarian, for their expertise and assistance in conducting several comprehensive literature reviews required to complete this work!
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Cheryl Petersen’s doctoral program and dissertation research were supported in part by the following scholarships and grants: The American Cancer Society Doctoral Degree Scholarship in Cancer Nursing (Grant #9124356-DSCN-13-269-01-SCN); The American Cancer Society Graduate Scholarship in Cancer Nursing Practice (Grant Number 121693-GSCNP-11-238-01-SCN); Marquette University Arthur J. Schmitt Leadership Fellowship; Tylenol Future Care Scholarship; Nurses’ Educational Funds Doctoral Scholarship; Oncology Nursing Society Graduate and Doctoral Scholarships; Hospice and Palliative Nurses’ Association Doctoral Scholarship; Southeastern Wisconsin Research Consortium’s Building Bridges Conference Grant; Marquette University’s Frenn Service Award Grant; and Sigma Theta Tau: Delta Gamma At-Large Grant.