
Abstract
Many survivors of childhood acute lymphoblastic leukemia (ALL) develop neurocognitive deficits that compromise academic functioning, especially in the presence of sociodemographic risk factors. The extent to which these risk factors coexist for Latino ALL survivors is not well described, but with shifts in U.S. demographics and improved survival in ALL, culturally competent interventions are needed. The Achieving Best Cognitive Successes after Cancer service was designed and implemented by a team representing nursing, medicine, psychology, and social work. Service components include neurocognitve assessment and individualized intervention for treatment-related risks and improving academic success for school-aged ALL survivors. Interventions are child-focused and parent-directed, recognizing that parents are major sources of support and advocates for their children within school systems. The service was designed to be culturally appropriate for the predominantly Latino patient population at our center, based on (1) linguistic competency of children and parents; (2) multicultural and ecological considerations for urban, low socioeconomic status, and migrant populations; (3) literacy barriers; and (4) contextual factors. This report describes methodological considerations and practice implications relevant to the design and implementation of similar culturally competent services for Latino pediatric cancer survivors.
Introduction
Acute lymphoblastic leukemia (ALL) is the most common and one of the most curable form of childhood cancer, with nearly 90% of patients achieving 5-year survival (Howlader et al., 2014). Many childhood cancer survivors are at risk for developing treatment-related long-term complications, such as subsequent malignancies, and problems arising in the cardiac, musculoskeletal, and reproductive systems (Landier, Armenian, & Bhatia, 2015). In childhood ALL, neurocognitive dysfunction that impairs learning is estimated to be the most prevalent late effect, affecting up to 40% of survivors (Buizer, de Sonneville, & Veerman, 2009; Campbell et al., 2007; Peterson et al., 2008). This is attributed principally to adverse effects on the developing brain caused by treatment routinely used in the care of children with ALL, including intrathecal methotrexate, high-dose systemic methotrexate, and cranial irradiation (Cheung & Krull, 2015). These deficits may adversely affect academic achievement, which refers to the extent a person is able to accomplish specific educational goals (Harshman et al., 2012).
In addition to treatment-related causes, sociodemographic factors may contribute to lower academic achievement in ALL survivors. Lower levels of parental education and socioeconomic status (SES) affect language skills development (Farah et al., 2006) and have independent adverse effects on cognitive functioning and academic achievement (Hill, 2012). These risks pose serious challenges to success in school and are known to be overly represented in Latinos (Annie E. Casey Foundation, 2011; Aud, Fox, & Kewal Ramani, 2010). The relative contribution and possible interactive effects of treatment exposure, linguistic, and socioeconomic factors on neurocognitive outcomes for childhood ALL survivors have not been well defined (Patel, Lo, Dennis, Bhatia, & PADRES Contra el Cáncer, 2013); however, the combined effect of these risk factors may pose particularly serious challenges to Latino survivors’ school success. Latinos are also underrepresented in clinical oncology research resulting from language-based exclusion criteria, nonparticipation of Latino potential subjects (Campbell et al., 2007) and difficulties in reporting racial/ethnic categories (Walsh & Ross, 2003). Thus, there is a need for developing culturally competent approaches to both clinical care and research for survivors facing multiple risk factors.
Evidence-informed survivorship care is team based, with nurses and nurse practitioners having key roles in providing safe, comprehensive, and competent care that emphasizes patient-centeredness, early identification of needs, and effective survivor education (Hobbie & Hollen, 1993; Landier, 2009; Ruccione, 2009). Nurses often are the first team members to hear from families about cognitive, academic, and psychosocial difficulties (Moore, Hockenberry, & Krull, 2013), and anecdotal experience suggests families may underreport or report differently to other team members. Unfortunately, it is not uncommon for academic and cognitive difficulties to go undetected or be confused with lack of effort on children’s part by parents and educators alike due to inadequate information about long-term effects (Butler & Mulhern, 2005; Nathan et al., 2007). In part, this is because cognitive deficits often only become evident as academic demands increase with age (Buizer et al., 2009; Nathan et al., 2007). Furthermore, nurses’ awareness about the impact of sociodemographic factors, such as bilingualism and SES, is key to families’ engagement in pediatric survivorship care (Barakat, Schwartz, Szabo, Hussey, & Bunin, 2012). This report examines considerations in designing and implementing culturally competent services and conducting clinical research with Latino pediatric cancer survivors, describes our institutional service for school-aged Latino ALL survivors, provides suggestions that can inform nursing practice, and includes an illustrative case example.
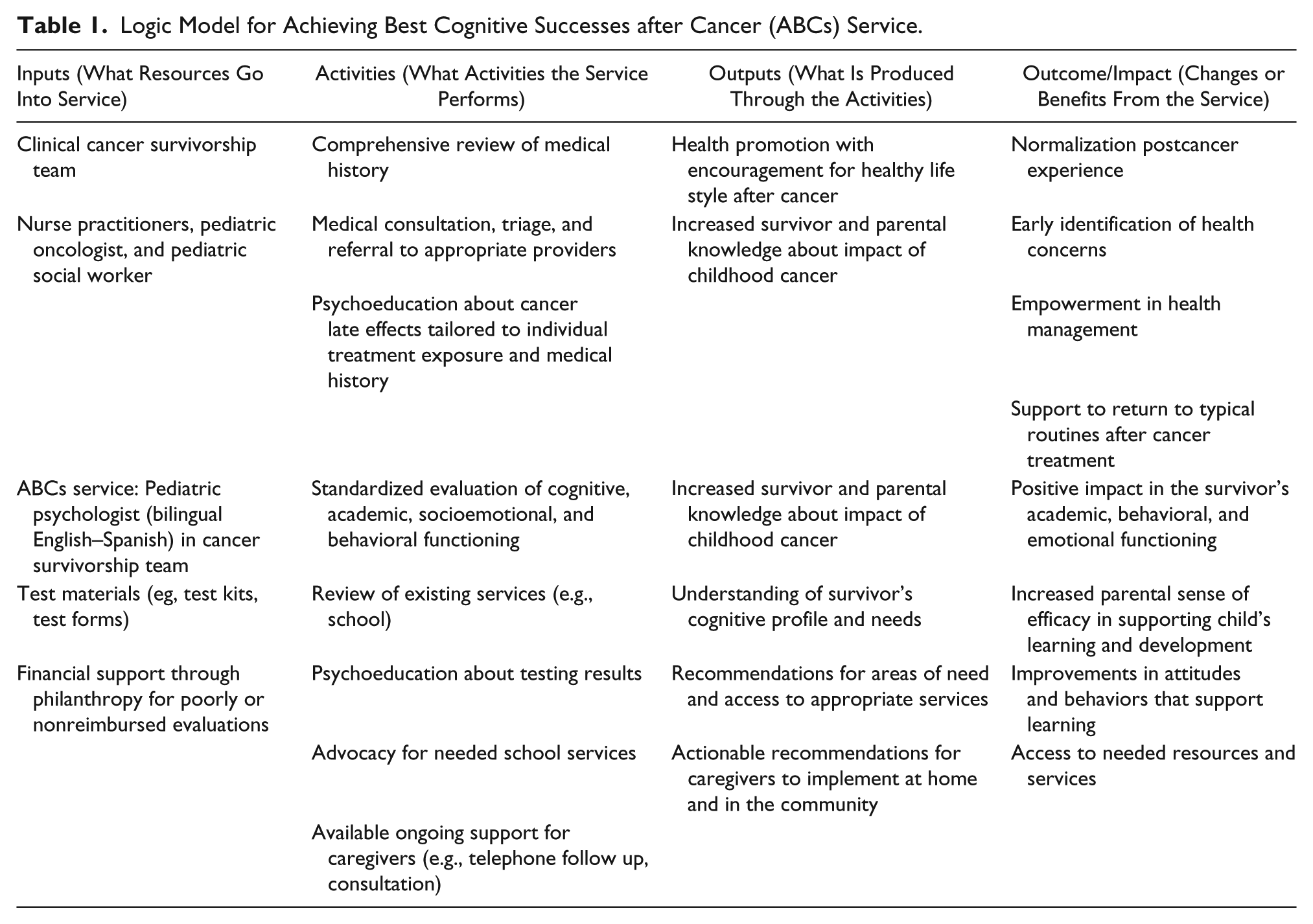
To improve academic success for school-aged survivors of childhood ALL, members of the LIFE Cancer Survivorship and Transition Service at our institution designed a clinical initiative that combines screening, assessment, and intervention, called the Achieving Best Cognitive Successes after Cancer (ABCs) service (see Table 1). The ABCs service is part of standard survivorship care offered to all school-age (5-18 years old) patients treated for ALL or lymphoblastic non-Hodgkin lymphoma (NHL). Relevant clinical data are collected with institutional review board–approved consent, which allows us to conduct outcomes research. The ABCs service uses risk-based screening and standard measures of neurocognitive functioning. The service also includes personalized, parent-directed interventions that enable them to advocate effectively for their child’s needs in school. While the individualized approach of this service is suitable for patients of any race/ethnicity, many of its features are designed to be responsive to the sociodemographic characteristics of our hospital’s predominantly Latino patient population. The service is focused on both the children and their parents, recognizing that parents and family represent a major source of support for children and are advocates within school systems. Additional details of the service and preliminary outcomes have been published elsewhere (Bava et al., 2016), including follow-up rates for completing recommendations to initiate school services, enrichment activities, and mental health referrals, as well as parental learning and satisfaction.
Logic Model for Achieving Best Cognitive Successes after Cancer (ABCs) Service.
Theoretical Framework
The conceptual framework for the ABCs service is drawn from culture care theory (Leininger, 2002). This theory focuses on the use of research findings to provide culturally congruent, safe, and meaningful care to clients of diverse or similar cultures (Leininger, 2002). A key premise of the theory is that “culture care values, beliefs, and practices are influenced by and tend to be embedded in the worldview, language, philosophy, religion (and spirituality), kinship, social, political, legal, educational, economic, technological, ethnohistorical, and environmental context of cultures” (Leininger, 1997, p. 39). The ABCs framework also incorporates the National Standards for Culturally and Linguistically Appropriate Services in Health and Health Care published by the Office of Minority Health, U.S. Department of Health and Human Services (2015). These standards recognize that culturally competent services are respectful, responsive, effective, and equitable for individuals and families with diverse cultural beliefs, language, and literacy needs. Cultural adaptations represent modifications of standard of care treatment to consider culture, language, and context in a way that is attuned with the values, specific needs, and practices of the population served (Bernal, Jimenez-Chafey, & Domenech Rodriguez, 2009). These adaptations also need to be responsive to within-group variations (e.g., country of origin, years in the United States, history of migration). These considerations apply not only to clinical services but also to research practices.
According to 2010 U.S. Census data, 50.5 million people in the United States are of Latino 1 origin, 42.5 million people speak Spanish at home, and about 32% of Latino children live in poverty (Ennis, Rios, Vargas, & Albert, 2011). Latinos are the third fastest growing segment of the U.S. population. Growth in numbers of Latino health care professionals, including nurses, has not kept pace with Latino population growth. Not surprisingly, Latinos and/or those from diverse backgrounds and their families experience a variety of resultant linguistic and institutional barriers (Peterson-Iyer, 2008). Navigating the health and educational systems can be difficult for parents during and after their child’s cancer treatment. Parents with low general literacy, limited educational attainment, low or non-English proficiency, and/or low SES factors face significant challenges in navigating systems of care (Paasche-Orlow, Parker, Gazmararian, Nielsen-Bohlman, & Rudd, 2005).
Cultural values also affect family interactions with medical settings. Cultural values influence clinical needs and conceptualizations of illness and cure (Gray, Szulczewski, Regan, Williams, & Pai, 2014). While there is within-group variation in cultural values often influenced by conditions such as ethnic identity, degrees of acculturation, and region or country of origin (e.g., most Latinos in Los Angeles immigrated from Mexico and Central America), there are some broadly shared cultural values often observed among Latinos (Gloria & Segura-Herrera, 2004; Santiago-Rivera, Arredondo, & Gallardo-Cooper, 2002). A primary value that impacts the context for patients’ medical care is familismo, which is a collectivist value characterized by strong ties and loyalty to family relations, including the idea that the family’s needs take priority over the individual’s needs (Santiago-Rivera et al., 2002). Family is a natural source of social, physical, and emotional support; its composition can be flexible and include nonrelated members. Personalismo is characterized by a style of communication and interaction highly attuned to positive interactions and social skills where relationships are prioritized over tasks (Santiago-Rivera et al., 2002). Simpatía (sympathy, warmth) refers to a warm, friendly attitude, which includes reciprocal respect with social conversations often preceding engagement in tasks (Gloria & Segura-Herrera, 2004). Simpatía has been found to influence coping style for Latina mothers of children with cancer (Johns et al., 2009). Confianza (trust, confidence) implies the establishment of a trusting relationship as well as familiar and personal interactions. Confianza facilitates disclosure and discussion of difficult topics with health care providers. Latinos value respeto (respect), which includes interacting with deference toward authority and avoiding conflict (Santiago-Rivera et al., 2002). These cultural values were foundational to ABCs design and implementation.
Overall cultural adaptations and content strategies (Barrera, Castro, Strycker, & Toobert, 2013) aimed at making the ABCs service responsive to the population included: (1) staff with linguistic competency in Spanish; (2) multicultural and ecological considerations for low SES and immigrant populations; (3) knowledge and awareness of literacy barriers; and (4) consideration of contextual factors, such as immigration policy. Additional design considerations included minimizing burden imposed on patients/families and providers, as well as maximizing impact with limited resources. For example, our neurocognitive assessment battery was designed to be both sufficiently comprehensive and concise. We relied on the reinforcement of the service goals by team nurses. Cultural adaptations included having a bilingual/bicultural psychologist responsible for recruitment and all ABCs interactions to facilitate the development of trust over time. Specific considerations and implications for nursing practice are threaded throughout the methodology section and nurses are encouraged to apply these considerations in their survivorship practice.
Methodology
Service Design
The process of service design mirrored the growing consensus that developing culturally enhanced interventions improves health outcomes and participation (Barrera et al., 2013). However, this process can be challenging, for example, there were limited options available for appropriate validated and reliable outcome measures for the population we serve. When necessary, nonstandardized surveys and informational materials were developed with sociodemographic considerations in mind. For example, attention was given to parental issues limiting their ability to assist with homework, such as not speaking English and lacking formal education. Delivering a service tailored to the unique needs of diverse families poses possible challenges to fidelity, as one size cannot fit all. We focused on the flexibility needed to increase the clinical applicability of the intervention with standardized components rather than adhering to a strictly manualized approach, which was particularly important when addressing the varying needs of Latino families.
Recruitment
The ABCs service and the psychologist responsible for delivering it were introduced to potential participants by well-respected members of the cancer survivorship clinic team, typically the nurse practitioners. Recruitment encouraged inclusion of extended family members or close friends in the intervention or consenting process (familismo). Self-selection was a recruitment challenge at times. It was sometimes difficult to engage families where cognitive assessment was perceived as a threat or when children did not have academic difficulties. In addition, we were not able to offer financial compensation to partially reimburse costs of participation. We recommend transportation costs be included where funding is available for similar research and clinical care initiatives.
Service Delivery
It was crucial for the clinician to interact in a professional, yet warm, and friendly manner (simpatia). Establishing trust (confianza) was important to address potentially sensitive topics, such as (1) parental knowledge of the educational U.S. system; (2) language or literacy barriers; (3) feelings of stigma related to special education services; and (4) fears when interacting with schools due to immigration status. These conversations were held after the ABCs provider had met with families at least twice in person to establish trust, reviewed completed parental questionnaires, and observed families’ needs and language use. Some families had familiarity and trust regarding research through their prior experience with cancer clinical trials.
A strong emphasis on key Latino cultural values provided opportunities to personalize the intervention. For example, reviewing survey answers with families contributed to personalismo and allowed tailoring of communication style. Conversations were held in an open and normalizing manner, including acknowledging the differences in education systems between other countries and the United States. The need for these families to learn and navigate the health care system after their child’s diagnosis with cancer was often used as a parallel for learning about survivorship and the U.S. school system. While immigration status of parents was never questioned, some parents disclosed their concerns as part of accessing educational services for their children. Skill building was tailored to parental knowledge (e.g., how to apply knowledge of late effects to educational rights at schools), contextual considerations (e.g., available resources in a community), and individual factors (e.g., education level, bilingual skills, and general health, and computer literacy). Families also learned negotiation skills and how to access community services. In addition, the service emphasized skills to promote learning at home, even when parents were not able to assist directly with homework content (e.g., setting homework routines, encouraging work habits, monitoring and restricting amount of screen time). For the survivors’ neurocognitive assessment, measures of formal English and Spanish language proficiency were included. Survivors’ language proficiency was integrated into the interpretation of overall results and recommendations provided to parents. Using a strength-based approach, cognitive benefits of bilingualism were discussed with families where appropriate. Parents were encouraged to use family members or friends (eg, comadres) to master advocacy skills needed within the school system. This strong sense of collectivism was manifested by many participants who expressed their desire to participate in future research in order to help other families.
Retention Strategies
Strategies to support participation included consideration of SES factors affecting attendance, such as reliance on others for transportation. The service was delivered in the fewest possible number of appointments to minimize “no shows” and family burden, such as excessive transportation costs and missed school and work. Whenever possible, flexible scheduling was offered to accommodate family needs. Families were encouraged to coordinate ABC visits with other scheduled medical appointments. Parental preference for appointments during school vacation time, days off from work, and holidays were accommodated.
Language and Literacy
Study forms were translated into Spanish and Spanish-language resources were used when available. Regardless of language preference, reading assistance was offered to parents when needed. All reading materials were supplemented with oral instruction. Parents who lacked computer literacy were given assistance to access web-based information. The ABCs service design was informed by awareness of the stigma associated with low literacy and lower levels of formal education that may make it difficult for parents to be forthcoming (e.g., some parents from Latin American regions had the experience of being removed from school to help support their families through working or providing childcare). It was not uncommon for parents with a sixth grade education or less to avoid answering questions about their own education or to delay in filling out forms. Parents were offered templates and assistance when they expressed a lack of confidence in making written requests for enhanced school services on their own.
The case example of “Cesar” (Table 2) illustrates the implementation of the ABCs service and how it was guided by the National CLAS Standards (Office of Minority Health, U.S. Department of Health and Human Services, 2015).
Case Example: “Cesar.”
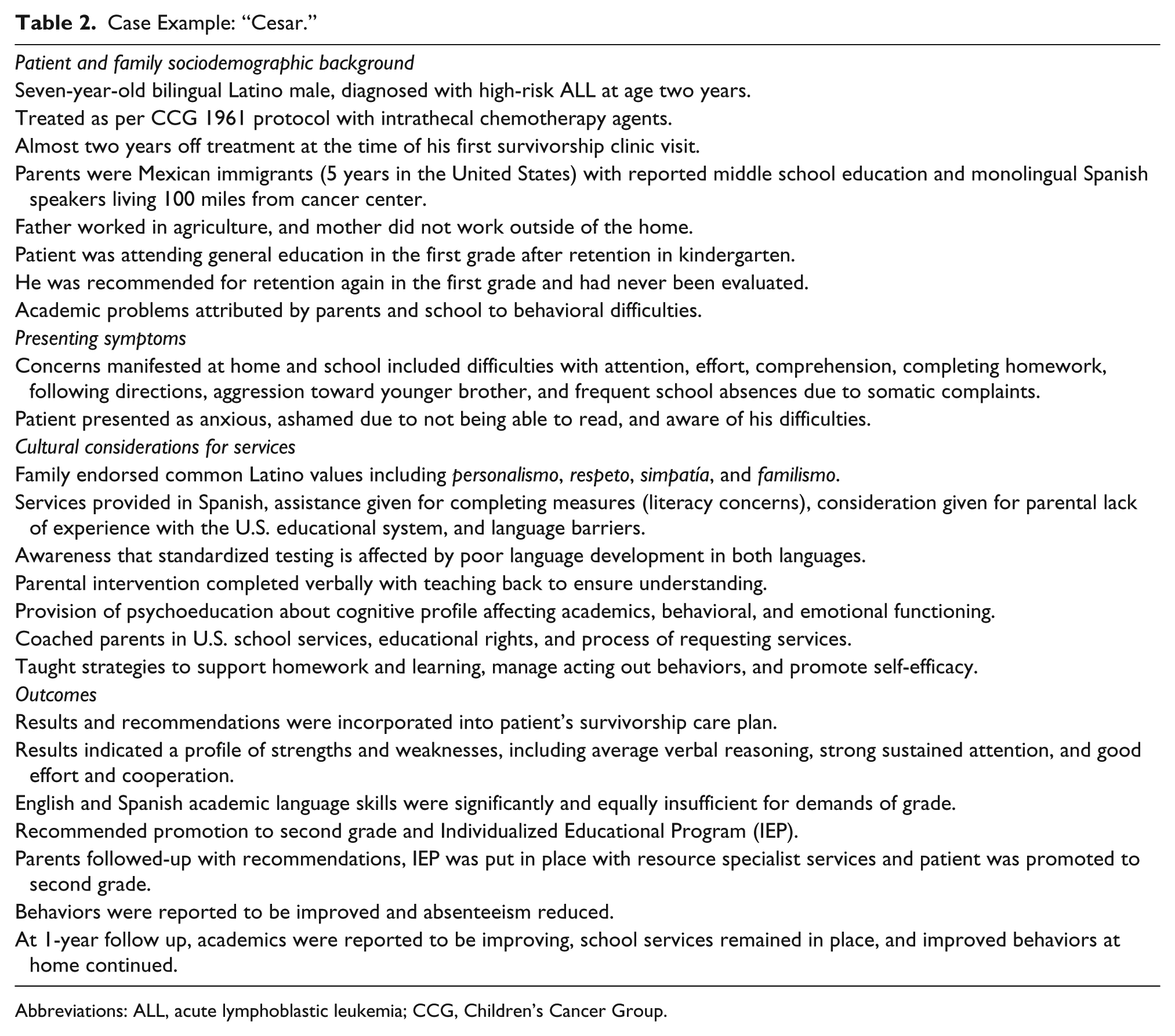
Abbreviations: ALL, acute lymphoblastic leukemia; CCG, Children’s Cancer Group.
Discussion
There is consensus that cultural factors influence pediatric cancer care and that culturally competent interventions can reduce health disparities to improve patient outcomes (Gray et al., 2014). Despite increasing numbers of Latino ALL patients, operationalizing cultural competence remains challenging. We developed our service with the goal of improving academic outcomes and reducing disparities affecting Latino childhood ALL survivors. In addition to conducting neurocognitive assessment, we provided parental education about the long-term effects of pediatric cancer treatment on academic achievement, how to navigate the school system, and the benefits of increased parental involvement. This approach enhanced parents’ sense of efficacy to advocate and problem-solve. The improvement in parents’ skills benefited their child’s educational and socioemotional well-being through the frequent completion of recommended actions (Bava et al., 2016).
As with many other efforts to integrate clinical research and care, we faced challenges regarding intervention design, maximizing resources, issues of reimbursement, sampling considerations, and selecting measures. Intertwined with these factors were overarching considerations for ensuring cultural and linguistic competency in order to extend the benefits of our service to the predominantly Latino patient population we serve. We found that we needed to account for parental language proficiency, literacy in English and Spanish, educational attainment, and SES, as these factors often influenced parents’ ability to support their children academically. As recommended in the CLAS standards (Office of Minority Health, U.S. Department of Health and Human Services, 2015), our linguistically competent service addressed language barriers and low literacy as key for obtaining appropriate services within the school system. We used frequent comprehension checks and verbal review, along with periodic phone check-ins, to ensure families understood and followed through with recommendations.
Clinical services and research designs that better match the needs of Latino populations are critical to increasing participation, engagement, and retention. Nurse practitioners were essential in the introduction of the service, psychoeducation about long-term effects, and follow-up care with Latino families. They reflected the cultural values incorporated into service delivery so that families experienced a personal connection, trust, and respect while learning how to address their child’s needs. These considerations align with the theory of cultural care, which asserts that “culturally congruent or beneficial nursing care can only occur when individual, group, family, community or institutional care value, expressions, or patterns are known and used explicitly in appropriate and meaningful ways” (Leininger 1997, p. 39).
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
Funding in support of this clinical service and related research was generously provided by the Larry and Helen Hoag Foundation.