
Abstract
Bone marrow transplant (BMT) units are stressful work environments with high staff burnout, anxiety, and turnover. A qualitative study was undertaken to better understand care for nurses within the context of their clinical practice on a pediatric BMT unit. Understanding care practices for BMT nurses will allow us to design interventions and provide appropriate support for this subspecialty of nurses. Focus groups were held with 24 nurses as key participants, and 2 focus groups with general participants: unit management (N = 2) and caregivers of inpatients (N = 7). Data were analyzed using a thematic analysis. Data were transcribed verbatim and coded to consensus by members of the research team. Five themes emerged from the data: (a) experiencing stressful situations that impede care, (b) growing and developing personally and professionally, (c) providing trustworthy and respectful care, (d) acquiring meaningful coping skills, and (e) sharing with others versus isolation. Stress management, professional development, and interdisciplinary communication were areas that emerged for potential intervention.
When registered nurses (RNs) are dissatisfied or experiencing burnout, there are consequences for the nurse, the unit, and the organization. Work environments that are intensive and stressful place strain on staff that can affect staffing, interprofessional relationships, and patient outcomes (Aiken, Clarke, Sloane, Sochalski, & Silber, 2002). This has been documented in environments such as intensive care units (Mahon, 2014; Sawatzky, 1996), oncology and bone marrow transplant units (Dougherty et al., 2009; Molassiotis & van den Akker, 1995; Spinetta et al., 2000), and emergency departments (Sawatzky & Enns, 2012; Trousselard et al., 2016). According to the U.S. Department of Health and Human Services and the Health Resources and Services Administration (2010), nurses working in these environments account for more than 46% of nurses practicing in the United States. These environments share common characteristics such as, fast pace, potential life threatening situations, exposure to death and dying, and high-risk critical patients (Butler, Willetts, & Copnell, 2015; Molassiotis & van den Akker, 1995; Mukherjee, Beresford, Glaser, & Sloper, 2009; Rashotte et al., 1997; Spinetta et al., 2000). These units are also associated with high staff burnout and turnover, which can affect staffing, quality of care, and patient outcomes (Aiken et al., 2002; Barnard, Street, & Love, 2006; Leiter & Maslach, 2009; Molassiotis & van den Akker, 1995; Mukherjee et al., 2009; Stutzer, 1989).
In order to better understand these environments and the staff that work in them, knowledge pertaining to the unit culture and how the staff provides care for themselves and others is needed. Pediatric bone marrow transplant (BMT) is one such unit, and little is known about pediatric BMT nurses’ views of care and their caring practices. The purpose of this article is to report the findings of a qualitative study that was conducted to discover, describe, and systematically analyze experiences, practices, and care meanings of nurses within the context of their clinical practice on a pediatric BMT unit.
Background
High-stress work environments have been associated with poor psychosocial health outcomes in health care workers. Nurses working in critical care and bone marrow transplant have reported anxiety, emotional exhaustion, and burnout (Bakker et al., 2005; Dunne, 2004; Gallagher & Gormley, 2009; Leung et al., 2012; Meadors & Lamson, 2008; Molassiotis & Haberman, 1996; Molassiotis & van den Akker, 1995). Faragher, Cass, and Cooper (2005) observed a strong relationship between decreased job satisfaction and lowered self-esteem, increased burnout, increased anxiety, and depression in their meta-analysis. The presence of burnout and dissatisfaction has been shown to predict nurses’ intent to leave their job within a year (Aiken et al., 2002). Work-related stress has also been related to staff absenteeism and turnover, which can be costly to the unit and the organization (Molassiotis & van den Akker, 1995). According to Hatcher et al. (2006), replacing an experienced RN costs one to two times their annual salary, and specialty trained RNs have an even higher replacement cost. The authors also stated that in hospitals with greater than 1,000 RNs, the average cost to replace a RN was from $43,667 to $90,000 (Hatcher et al., 2006).
Bone marrow transplant units are high stress environments. Staff working in BMT reported stressors such as the high level of responsibility accompanying working in a technical and intensive environment with various ethical and moral issues, as well as, interpersonal relationships, communication, working with dying patients, short staffing, rotating shifts, and patient acuity (Gallagher & Gormley, 2009; Molassiotis & van den Akker, 1995; Stutzer, 1989). This medically intense and emotionally charged environment often leads to the development of burnout (Barnard et al., 2006; Leiter & Maslach, 2009; Molassiotis & van den Akker, 1995; Stutzer, 1989), and compassion fatigue in health care providers (Meadors & Lamson, 2008), which can, in turn, lead to staff turnover (Molassiotis & van den Akker, 1995).
Burnout can be defined as a physical, emotional and mental state of exhaustion resulting from involvement in work environments that are emotionally demanding over a period of time (Schaufeli & Greenglass, 2001). Burnout is a syndrome that consists of 3 main aspects: depersonalization, emotional exhaustion, and low personal accomplishment (Maslach, Schaufeli, & Leiter, 2001). Research has indicated that anywhere between 62.5% and 100% of staff working in BMT suffer from burnout (Gallagher & Gormley, 2009; Molassiotis & Haberman, 1996; Molassiotis & van den Akker, 1995; Moody et al., 2013; Roth et al., 2011). Roth et al. (2011) found that of 127 pediatric oncologists who thought they had burnout symptoms, 94% had at least moderate burnout and 73% had high levels of burnout. In this same study, pediatric oncologists who did not think they had any symptoms of burnout (N = 222), 66% had at least moderate burnout with 18% having high levels of burnout (Roth et al., 2011). Moody et al. (2013) conducted a mindfulness intervention to reduce burnout in oncology staff (N = 45). In this sample, 100% of staff experienced moderate to high levels of burnout both pre- and postintervention. Although the intervention was not shown to decrease burnout scores, staff subjectively reported feeling less stress and anxiety (Moody et al., 2013).
BMT has evolved as a subspecialty of cancer nursing requiring special knowledge and skills. It is a highly complex and challenging area to work as nurses must coordinate interdisciplinary care activities, complex care and medication regimens, psychosocial support, and patient and family education. Patients become severely immunocompromised as a result of treatment. They suffer through mucositis, and receive frequent blood component transfusions and therapeutic infusions, along with supportive therapies. Patients are also isolated to prevent exposure to infectious contaminants (National Cancer Institute, 2015).
Providing holistic and family-centered care requires that nurses learn to balance the tasks involved in patient care while coordinating and fostering communication between disciplines and with patients and families. These factors combined create challenges for patients, caregivers, and staff working with them. To better propose strategies to improve care and the care environment, more information is needed about the unit culture. This article will discuss results of a qualitative study on the experiences, practices, and care meanings of pediatric BMT RNs. The study aims were to (a) explore staff RN’s beliefs, meanings, expectations, and expressions of care through interviews and observations and (b) to discover meaningful ways to care for RNs working with children receiving a BMT.
Method
A qualitative research study was conducted to explore the experiences, practices, and care meanings of pediatric BMT RNs. A focus group approach was used for data collection to explore the views of nurses about working as a pediatric BMT RN and to observe interactions between participants (Jayasekara, 2012). Key participants were purposefully selected from staff nurses that worked at least part-time on the BMT unit. An effort was made to recruit an equal number of less (<2 years) and more (>2 years) experienced nurses.
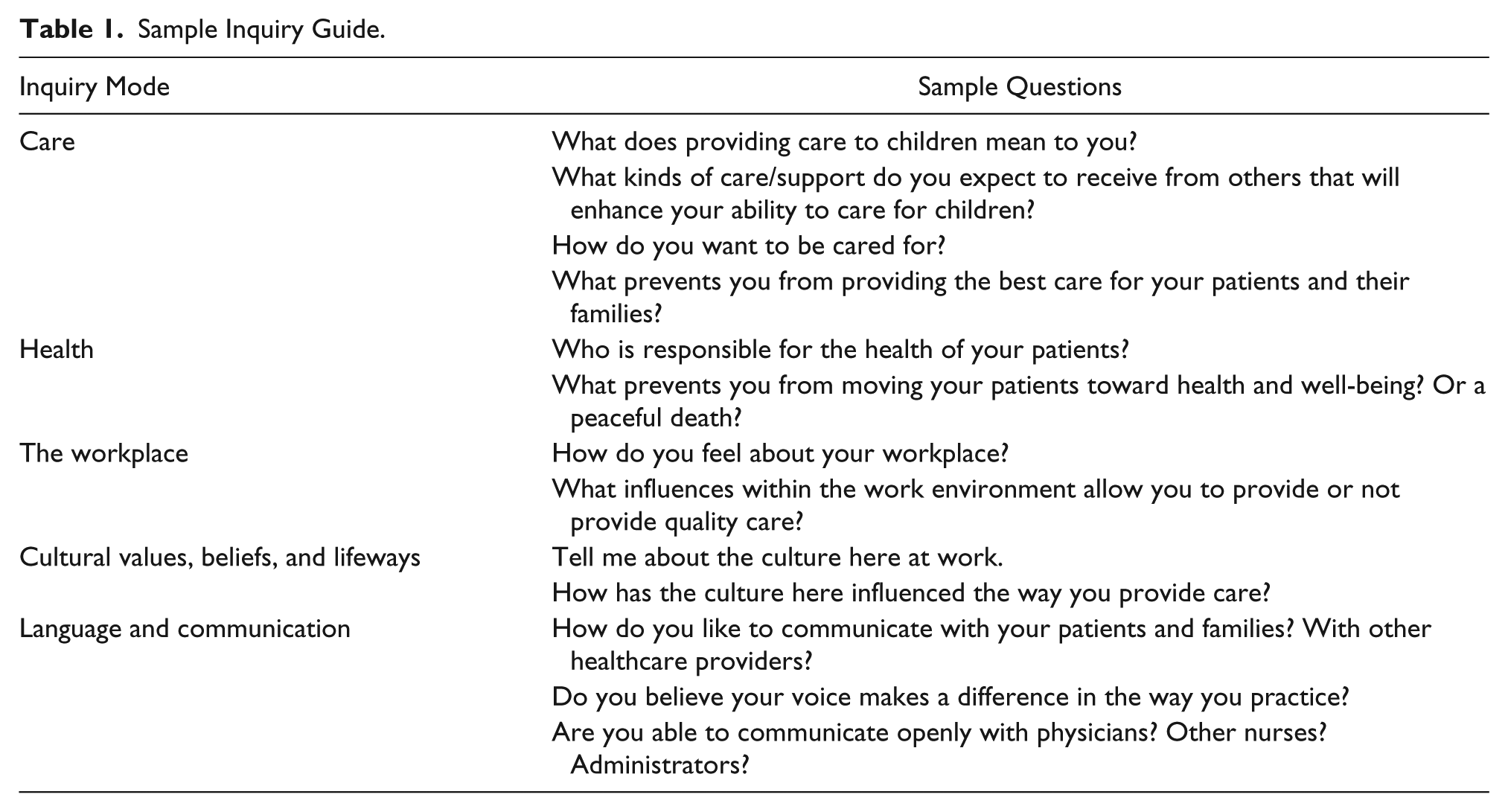
Focus groups were conducted using an inquiry guide developed by the researchers See Table 1 for an example of the inquiry guide. A total of 9 focus groups were conducted with staff nurses using the same moderator (CM), an experienced pediatric BMT RN. Having a moderator who was known and familiar to participants, or a trusted research friend (Leininger, 1998), enhanced trustworthiness and was used as a validation strategy (Creswell, 2013). General participant focus groups were held with managers (N = 2) and parents or caregivers (N = 7) of patients on the BMT unit as a method of triangulation (Creswell, 2013), adding richness and support to key participant data (Leininger, 1998). Observations of activities and interactions within the work environment (contextual data) were collected using a field journal and during focus groups, and were also used for triangulation (Creswell, 2013). Focus group sessions were digitally recorded and transcribed verbatim. Study sessions lasted between 40 and 90 minutes in length.
Sample Inquiry Guide.
Data were analyzed using a thematic analysis (Leininger, 1998; Vaismoradi, Turunen, & Bondas, 2013). First, code words were identified from the raw data using line-by-line coding. Codes were then categorized into patterns, and patterns into themes and subthemes with the assistance of the NVivo© Software Package. Data were coded to consensus by members of the research team at each level of analysis. This study was approved by the institutional review board. All participants reviewed the study information sheet and provided verbal consent prior to participating (written consent waived by the institutional review board).
The setting for this study was the BMT unit within a large Midwestern children’s hospital. The unit specializes in BMTs for oncologic, hematologic, metabolic, and immunologic disorders and attracts patients from around the globe. The length of stay ranges from several weeks to well over a year. Parents are involved in the care of their child and are often at the bedside 24 hours per day.
Results
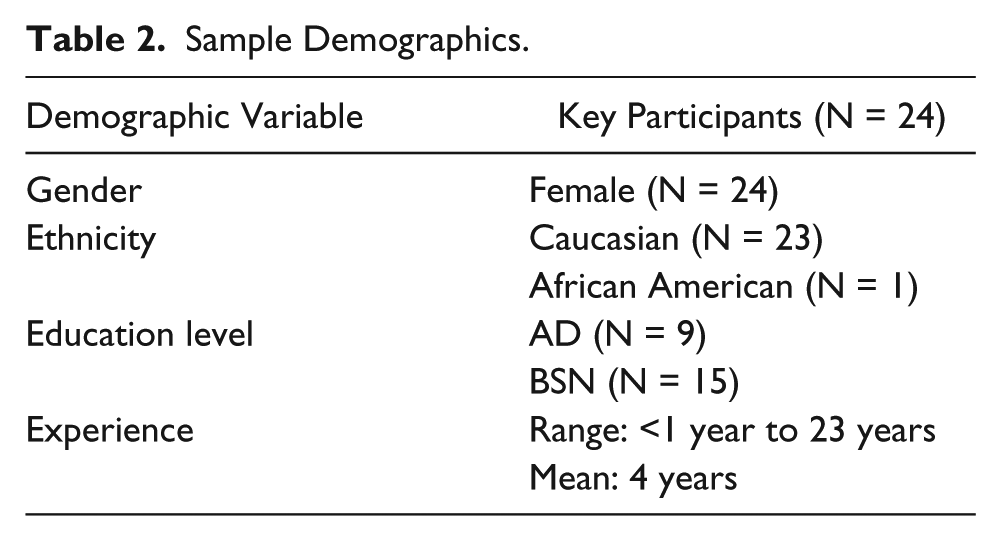
All staff RN participants (N = 24) were female and with an equal number of more (>2 years) and less (≤2 years) experienced nurses. Six mothers and one father participated in the caregiver focus group. Table 2 lists participant characteristics.
Sample Demographics.
Five themes emerged from the data: care for nurses within the culture of a pediatric BMT unit means (a) experiencing stressful situations that impede care, (b) growing and developing personally and professionally, (c) providing trustworthy and respectful care, (d) acquiring meaningful coping skills, and (e) sharing with others versus isolation.
Theme: Experiencing Stressful Situations That Impede Care
Words used to describe working in the environment were “stressful,” “hard,” “challenging,” and “rewarding.” Nurses in this study experienced stress from multiple sources while providing care for others. One source of stress BMT RNs identified was performing multiple tasks that detracted from their ability to offer emotional and spiritual care. This was especially difficult for less experienced nurses who were still learning how to manage their time. This was also mentioned in both the manager and parent/caregiver focus groups. One participant remarked, It would be interesting to know what that impact would have on a patient length of stay and recovery if you have one-on-one nursing. If they would feel that much more cared for, or that much more in an environment where you can heal better? And you’re not missing things because you are busy with another patient.
Another source of stress for the BMT RNs was serving in multiple caregiver roles while trying to provide care, maintain therapeutic relationships, and maintain boundaries. Families are isolated and many are from out of town, and often the medical and nursing teams are the only people who shared their journey. As one participant described it, “You’re the only ones that technically kind of know what their world is like, which we really do because a lot of the family members will say.” The shared journey sometimes led to a blurring of the line between a professional and personal relationship. Another nurse participant stated, It is hard to define the line, because they need to know that you’re the professional nurse that is taking care of their kid, but at the same time it’s therapeutic to almost get in that friend role but not to be in a social relationship, it’s a very delicate line.
This was confirmed in both general participant focus group sessions. Nurses also described being substitute parents to children who were left in the hospital alone as emotionally difficult and an added stressor in daily care.
The third source of stress the BMT RNs identified was not being heard by physicians, management, and parents. Less experienced RNs remarked that they felt their assessments or inputs were not taken as seriously as more experienced colleagues, which undermined confidence and occasionally led to nurses questioning when to approach the medical team with concerns. Less experienced RNs felt they needed to prove themselves before they were accepted as part of the team. The RNs sometimes felt they were not valued members of the care team and described not feeling validated or having positive reinforcement for accomplishments by management. Not being heard by parents usually involved unit rules that are in place for patient safety such as visitor restrictions, hygiene practices, and therapy participation. Parents would sometimes attempt to gain control by undermining the RNs and pitting them against each other and the medical team, which led to conflict and discord.
Theme: Growing and Developing Personally and Professionally
Participants described being a novice nurse just out of orientation and learning how to complete tasks, learn new skills, manage time, and seek out resources. They also described transitioning to a more experienced nurse, trusted with high-risk and higher acuity patients. This sometimes caused anxiety about their ability to provide good care and uncertainty in their technical skills that was gradually reduced with experience. One novice nurse remarked “I mean you feel good about yourself when you get to work that day and you have a difficult patient. It makes you feel like people have confidence in you.” Experienced RN participants discussed learning how to teach another nurse to provide meaningful care and taking on more responsibilities within the unit and the organization as areas of professional growth. Participants saw these as important responsibilities that could be stressful but also rewarding.
Participants appreciated opportunities for learning and professional development. Some of the opportunities nurses in this study identified were learning new technical skills while providing patient care, in-services on new medications, learning about different cultures, disease specific information, and spontaneous teaching moments such as patient-centered daily rounds with the interdisciplinary team.
Caring for patients and families from multiple cultural backgrounds and family structures served as sources of personal and professional growth. Nurses talked of learning about new cultures and how to work that knowledge into their practice. One participant stated, “Because we do pull from all over the world, you have this opportunity to meet people from all over the world and be introduced to cultures you have very little exposure to and work that into your practice.”
Nurses talked of “bearing witness” to suffering and the privilege of caring for someone during what is likely to be one of the hardest times in their lives and helping to make the burden more bearable. As one nurse put it, You’re loving somebody at one of the hardest times in their life. It’s not the easy love, it’s not the chocolate and let’s go do something fun like go to the movies, it’s the really- I have diarrhea on the floor, my hair’s falling out, my skin, my body’s basically betraying me and I need you to stand with me while I go through this. So when you see that, it will stop you.
Theme: Providing Trustworthy and Respectful Care
Providing trustworthy and respectful care was important to BMT nurses and was accomplished through staff, physician, and patient communication, and through a positive nursing presence. Communication and attitude were the 2 essential elements of trustworthy and respectful care nurses identified. Managers and parents corroborated that communication and attitude were important in nursing care. Effective communication between nurses, nurses and other healthcare team members, and nurses and families establishes therapeutic relationships that are built on trustworthy and respectful care. If trust or respect is broken, it can create conflict and damage relationships not just for that member of the team but for all the others that follow.
You’re just that critical of a link so when you have somebody there that doesn’t really care about it is, having the attitude that that’s not my job, or I’ve never had this patient before. Those words should be a strike out. It really does impact that care for that family and they’ll remember that. There’s no way around it. And it sets up that next person that comes in to have to undo because it can be a total trust issue because you’ve broken that trust and now someone else has to come in and repair it.
Conflict between the nurses and members of the medical team also affects the ability to provide respectful and trustworthy care. Nurses identified the following as sources of conflict: questioning decisions or orders, moral or ethical differences, being stuck in the middle between medical team and family, and occasional demeaning or bullying behavior. When nurses questioned medical decisions often it was for clarification or a better understanding. Reactions from the medical team were either supportive of questions and provided explanations or education as needed, or taken as questioning of the prescriber’s judgments or decisions leaving nurses feeling penalized for asking questions. The moral and ethical conflicts brought up in the interviews mainly surrounded the transition from curative treatment to palliative care.
Bone marrow transplant RNs found that negative attitudes among co-workers caused discord and disruptions in patient care. There were several core characteristics that emerged from the data that collectively were termed the positive nursing presence. The positive nursing presence incorporates a positive attitude, professional behavior, open communication, and accountability for yourself and other members of the care team. One participant said, It is really a much better day when you have those relationships and you feel like you are here with a group. Like “How’s your day? Did you get lunch?” And you can just feel it. Sometimes, I can walk on the floor and I can feel it as I walk through the door, what the energy is. So my argument is, why would you not want that every day?
Theme: Acquiring Meaningful Coping Skills
Nurses identified several coping skills they utilized to help manage working in the BMT environment. Having a sense of humor was used as a way to relieve stress and tension. Humor was also used often when reminiscing about past patient encounters both in focus group sessions and on the unit. Several nurses talked about not taking things personally, especially in nurse–family relationships. As one nurse said, “I think not taking it personal in a wide variety of things. Not taking it personal in the sense of how the parents feel and when they have a bad day and they take it out on you.”
Participants also talked about taking a step back, or gaining perspective. “You think you’re having a bad day but you just have to take a step back and think about what’s going on. They don’t choose to be, well I mean nobody chooses that but it’s very humbling.” Several nurses talked about seeing it from the family’s point of view and “walking in their shoes,” which allowed them to gain new perspective. The other side of this is emotional attachment as the nurse and family spend time together and try to enter into a relationship together. Several nurses discussed using emotional distance as a coping mechanism, a way to protect themselves so they could continue to come back to the workplace. “Sometimes you can’t let yourself get close to every single person. You have to protect yourself, you have to.”
Nurses also sought out social support structures both on the unit and outside of the workplace. The social support has to be a positive relationship that builds into the nurse, otherwise it was considered time consuming and another stressor. “And it’s not even just having someone to talk to, it’s just having a life out of here to balance it all, to get your mind off of it.” Nurses also sought outside interests such as volunteer work, physical activities, hobbies and travel as ways to cope, take a break and gain a different perspective.
Theme: Sharing With Others Versus Isolation
Nurses described trying to talk to others about work and getting responses like “why don’t you quit,” wondering how someone could work with kids getting a BMT, or even refusing to listen. This lead to nurses being socially isolated in their job roles. One nurse described it as follows: Do you know how some people that aren’t nurses or aren’t in the medical field, you can’t even explain to them, possibly explain to them what you do in a day. It’s not like- no one would ever understand it.
Nurses felt they were able to share with others who had similar experiences. Those who lacked shared experiences, such as family and friends, had difficulty relating to and sympathizing with BMT RNs. Nurses reported criticism when they attempted to find humor in serious situations, and friends and family were unable to understand their desire to continue working in a stressful environment with sick and dying children. This inability to share with those outside the work environment created a sense of isolation. Nurses reported that in order to cope they shared personal experiences with other staff on the unit who had similar experiences and were able to sympathize and bring clarification when necessary. Sharing with coworkers, or reminiscing, also served as a mechanism nurses used to cope with losing a patient and served as an informal debriefing.
Discussion
Nurses in this study described the BMT unit work environment as stressful which is consistent with current literature. Stressors for BMT nurses identified in the literature include technology, palliative/end-of-life care, interpersonal relationships, moral/ethical concerns, intensive care environment, and patient acuity (Gallagher & Gormley, 2009; Molassiotis & van den Akker, 1995; Stutzer, 1989). Nurses in this study discussed these stressors in the context of how they affected the care they were providing.
For nurses, interpersonal conflict with patients and families was often attributed to the stress the families were experiencing due to treatment and complications. Interpersonal conflict with the medical team coincided with some of the moral and ethical concerns nurses in this study identified, such as when to prepare patients and families for the transition to palliative, or end-of-life, care from curative treatment. In a study with intensive care unit nurses, apathetic and incompetent nursing staff was seen as the biggest threat to good and safe care, and moral and ethical issues ranked as the highest stressor for these nurses (Sawatzky, 1996). Other interpersonal conflict between disciplines in this study involved ineffective communication and respect for the nurse as a professional.
Sabo (2011) found similar results with her phenomenological study of meaning in BMT nursing. Nurses in this study talked about professional development and learning and growing in their clinical practice. Sabo (2011) called this being comfortable in one’s own skin. Competency for nurses in this study progressed in a pattern that matches Benner’s stages of clinical competence (Benner, 1984). Nurses in this study explored bearing witness to suffering, which was also seen in Sabo (2011)’s investigation. A theme that emerged in Sabo (2011)’s investigation was RNs’ need to feel supported, which incorporated being heard, education, and personal care. The results of the current study were similar, with participants discussing coping mechanisms they used, personal and professional growth, and sharing versus isolation.
Sabo’s (2011) theme navigating uncertainty involved the process of trying to establish and maintain relationships with patients and families. Nurses in the current study also discussed relating to patients and families when they shared about maintaining boundaries and therapeutic relationships. Similarly, nurses working in intensive care units in the Netherlands reported providing good and safe care was dependent on building a bond of trust with their patients and families (Wassenaar, van den Boogaard, van der Hooft, Pickkers, & Schoonhoven, 2015). The bond of trust was developed by ensuring physical safety, nurses’ attitude and expertise, explaining and informing families about care and what to expect, and by developing a relationship with families (Wassenaar et al., 2015). Many of these concepts were comparable to BMT nurses’ views, such as developing expertise and having a good attitude as necessities to providing good care, which suggests a similarity between BMT and intensive care nursing. The analogous findings in these studies on a specialized population of nurses suggest that results may be transferable to other BMT nurses, and potentially to intensive care nurses.
Limitations
The unit this study was conducted on is unique in that it has 24 dedicated pediatric BMT beds with resources such as donor partnerships, child life specialists, music therapists, holistic health specialists, and care resources that other BMT units may not have available. A large portion of patients have immune disorders and the majority of the nursing staff are new graduate nurses, which also contributes to the uniqueness of the unit; however, as addressed earlier, Sabo (2011) had similar results in her study with BMT nurses working on an adult unit.
Implications for Practice
Stress management, professional development, and interdisciplinary communication have emerged as areas to target for care interventions for this group of nurses. Education on stress management and relaxation techniques, resilience, and the impact of stress on health could be beneficial for this group of nurses. Interdisciplinary communication is essential to safe and effective patient care. Nurses highly valued authenticity, positivity, and accountability in relationships with their coworkers and felt it impacted their ability to function as a team and cope with the interpersonal challenges of the environment. Mentors and leaders within the care environment can help change the unit culture by modeling behaviors and attributes the “positive nurse presence” embodies.
Conclusions
Understanding the culture of pediatric BMT nurses and the environment in which they work, promotes the ability to care for them in ways that are meaningful. For this population of nurses that includes recognizing the stress involved in care and stressors specific to the environment. It also includes providing opportunities to grow and learn as a person and a professional, respectful and trustworthy care with positive attitude and open communication, awareness of coping skills, and opportunities to share their experiences with others who relate. Stress management, professional development, and interdisciplinary communication are potential targets for interventions to provide meaningful care for pediatric BMT nurses.
Footnotes
Acknowledgements
We would like to express our gratitude to all the staff and parents who so openly shared their experiences with us. A special thanks to Stella Davies, Laura Flesch, and Mary Ellen Meier for their support of this work.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded in part by the Carolyn Stoll Research Fund through the Division of Patient Services at Cincinnati Children’s Hospital.