
Abstract
This article describes changes in central line–associated bloodstream infection (CLABSI) rates among common causative organisms over an 11-year period on a pediatric inpatient unit prior to and following CLABSI reduction strategies. The setting for this descriptive cohort design study was a 32-bed inpatient unit in a tertiary pediatric hospital serving children with immune compromised conditions, including cancer and recipients of hematopoietic stem cell and solid organ transplants. Between January 2006 and December 2016, 265 CLABSIs involving 189 patients were reported. Data were organized into three time periods: 5-year preintervention baseline (2006-2010), implementation of maintenance care bundles (2011-2012), and addition of formalized supportive care practices to the maintenance care bundles (2013-2016). Organisms were categorized into four groups based on the National Health Safety Network organism list. Time-by-class Poisson regression models evaluated changes in CLABSI rates. Characteristics of patients who developed CLABSIs were unchanged. Infections occurred most frequently among patients with hematologic malignancies and neutropenia. Significant log rate decreases in CLABSI rates were observed with the implementation of maintenance care bundles plus enhanced supportive cares compared to preintervention baseline for the following organisms: (1) common commensal organisms (−1.05, p = .005), (2) mucosal barrier injury (MBI) organisms common to the mouth (−.708, p = .007), and (3) other noncommensal/non-MBI pathogens (−.77, p = .005). Rates were unchanged for MBI organisms common to the lower gastrointestinal tract. Central line maintenance care bundles and formalized supportive care practices resulted in sustained decreased CLABSI rates. Additional interventions are needed to reduce CLABSIs involving MBI-associated organisms common to the lower gastrointestinal tract.
Keywords
Introduction
Although central line–associated bloodstream infections (CLABSIs) among children with cancer and other immune compromised conditions have decreased with the implementation of best practice bundles, these infections continue to occur (Bundy et al., 2014; Rinke et al., 2012). For children with cancer, the attributable cost of a CLABSI may be as much as $70,000 with an additional hospital length-of-stay of 21 days (Wilson, Rafferty, Deeter, Comito, Hollenbeak, 2014). Reported mortality rates for children with cancer and those undergoing hematopoietic stem cell transplant who develop bloodstream infections range from 1.5% to 10% (Bochennek et al., 2016; Celebi et al., 2013). Likewise, patients undergoing solid organ transplant face a heightened risk of bloodstream infection, with approximately 29% of adults undergoing liver transplantation experiencing a posttransplant infection (Santos, Hotchkiss, Chapman, & Olsen, 2016).
Mechanisms of Bloodstream Infection
Prevailing frameworks addressing causes of CLABSIs regard these events as breaches in care either during the insertion of the central venous catheter or during its maintenance care that result in the introduction of pathogens into the bloodstream (Agency for Healthcare Research and Quality, 2017; Centers for Disease Control and Prevention [CDC], 2017). The catheter insertion site as well as the catheter hub and needleless connector ports are regarded as potential sites for pathogen entry.
For patients with cancer and those undergoing hematopoietic stem cell transplant, translocation of pathogens across injured mucosal tissue represents an important mechanism of bloodstream infection (Gyarmati et al., 2015; Metzger et al., 2015; Simon et al., 2016; Steinberg, Robichaux, Tejedor, Reyes, & Jacob, 2013). Current pathophysiologic frameworks of mucositis indicate that injury is happening below the level of the epithelium before clinically evident signs and symptoms of injury are present (Sonis, 2009). Generation of reactive oxygen species, DNA strand breakage, and cytokine activation further contribute to tissue damage.
In 2013, the CDC added the mucosal barrier injury (MBI) designation to primary bloodstream infections that meet the clinical criteria of (1) presence of neutropenia and/or graft-versus-host disease and (2) infection involves an organism that is included on the CDC’s master list of organism as being associated with MBI (See et al., 2013). Although these infections include the MBI designation, they remain reportable as hospital-acquired infections.
The CDC revised their criteria for designating secondary versus primary bloodstream infections in 2015 (CDC, 2017). Included in these criteria was the requirement for radiographic evidence of gastrointestinal infection as a cause of secondary bacteremia. As a consequence of these revised definitions, many institutions experienced increases in CLABSI rates because events that previously would have been classified as secondary events were now classified as primary bloodstream infections (Grimes et al., 2016; Huber & Cycan, 2016).
Organisms and Infection Risk Factors
Among patients with cancer, those with hematologic malignancies are at heightened risk for bloodstream infection (Metzger et al., 2015; Rhee, Heung, Chen, & Chenoweth, 2015; Thurman, Abbott, Liu, & Larson, 2017). Approximately 20% of children with acute lymphoblastic leukemia and over 60% of children with acute myelogenous leukemia will experience at least one episode of bacteremia (Ammann et al., 2015; Sung, Lange, Gerbing, Alonzo, & Feusner, 2007). Gram-positive organisms, particularly coagulase-negative staphylococci and viridans group streptococci, predominate as leading causes of bacteremia (Gaur et al., 2013; Kelly et al., 2011; Lewis et al., 2014; Nielsen et al., 2016; Sung et al., 2007). For children with hematologic malignancies and those undergoing hematopoietic stem cell transplants, viridans group streptococcal infections most frequently occur during periods of neutropenia and are associated with significant morbidity, including septic shock and the need for intensive care services. Organisms associated with the lower gastrointestinal flora, specifically Escherichia coli, Enterococcus species, and Klebsiella species, are also important causative organisms. In the hematology/oncology/transplant population, these organisms are frequently associated with infections meeting MBI criteria (Metzger et al., 2015). Of note, vancomycin-resistant enterococci may be increasing as a source of CLABSIs (Kelly et al., 2011).
Overview of Strategies to Reduce Infections
To date, strategies to reduce CLABSIs have emphasized preventing the introduction of outside pathogens. Similar to efforts to reduce CLABSIs in critically ill adults, best practice maintenance care bundles for central venous catheters have been implemented across multiple pediatric hematology/oncology/transplant settings (Duffy, Rodgers, Shever, & Hockenberry, 2015; Rinke et al., 2012). Results of a national quality improvement initiative among inpatient hematology/oncology/transplant centers found that implementation of best practice maintenance care bundles resulted in a 28% decrease in CLABSIs (Bundy et al., 2014). This study did not, however, report differences in CLABSI rates based on organism. The use of a central venous catheter care team with the goal of ensuring standardization of best care practices was deemed feasible but did not result in a significant decrease in CLABSIs (Secola et al., 2012).
The use of chlorhexidine (CHG) bathing to reduce CLABSIs in critically ill adults has had mixed results (Climo et al., 2013; Noto et al., 2015). Reported decreases in CLABSI rates have been largely driven by decreases in coagulase-negative staphylococci while decreases in CLABSI rates involving organisms common to the lower gastrointestinal tract have not been observed (Climo et al., 2013). Likewise, in critically ill children, per-protocol analyses identified significant decreases in bacteremia involving coagulase-negative staphylococci with the use of CHG bathing in children with and without central venous catheters (Milstone et al., 2013). No differences were observed in bacteremia events involving yeast or gram negative bacteria.
Among the pediatric hematology/oncology/transplant population, a single-site study comparing a 7-month baseline to a 7-month trial of CHG bathing on an inpatient pediatric oncology unit did not demonstrate differences in bloodstream infection rates (Raulji, Clay, Velasco, & Yu, 2015). Rates of hospital-acquired infections from other sources such as the urinary tract or respiratory tract also did not differ. This site reported a decrease in hospital-acquired infections among patients 12 years and older (p = .009) but not among other age-groups. Another pediatric hematology/oncology/transplant unit reported decreased CLABSI rates involving coagulase-negative staphylococci and viridans group streptococci following implementation of formalized supportive care protocols with increased attention to daily hygiene (Linder, Gerdy, Abouzelef, & Wilson, 2017).
To date, most institutions have reported changes in CLABSI rates over a relatively short period of time such as a 6-month intervention period. Additionally, evidence addressing sustained decreases in CLABSI rates over longer periods of time in both adult and pediatric settings is limited. Because CLABSIs are uncommon events, examination of a longer time range may provide a more meaningful perspective and analysis of progress in reducing events and provide direction for additional focused interventions.
Purpose
This article presents changes in CLABSI rates among common causative organisms over an 11-year period on a pediatric inpatient unit that provides care for children with immune compromised conditions. This time period includes a 5-year preintervention baseline (2006-2010) and 6 years following the introduction of intentional CLABSI reduction efforts. The intervention period is further divided into two time periods: (1) the implementation of the Children’s Hospital Association’s best practice central line maintenance care bundles (2011-2012) and (2) the addition of formalized supportive cares in addition to the best practice maintenance care bundles (2013-2016). The formalized supportive cares included daily soap-and-water bathing, twice daily oral care, and out-of-bed activity three times each day (Linder, Gerdy, Abouzelef, & Wilson, 2017).
Method
Design
This study used a descriptive cohort design. This study is guided by a practice-based evidence approach that emphasizes the use of data from routine clinical practice to identify the most effective and efficient practices in routine care (Horn et al., 2015; Horn & Gassaway, 2007). A practice-based evidence approach is particularly useful when best practices are not well established. Data can then be used to guide iterative decision making as part of quality improvement initiatives.
Setting
The setting was a 32-bed inpatient unit serving children with immune compromised conditions at a free-standing tertiary children’s hospital in the Intermountain West of the United States. The majority of the unit’s patient population includes children with cancer and hematologic conditions as well as those undergoing hematopoietic stem cell transplant. The unit also serves children undergoing kidney and liver transplantation. Over the past 11 years, the unit has averaged approximately 6,400 central line days each year. The unit averages approximately 1,300 admissions and 6,800 patient days per year. More than 85% of these days are attributed to patients with cancer or those undergoing hematopoietic stem cell transplant. Patients treated by the oncology service whose treatment results in prolonged and profound neutropenia (e.g., acute myelogenous leukemia) remain inpatient during the count recovery period. Antibacterial prophylaxis was not routinely prescribed for these patients during the time periods represented in these analyses.
Data Sources
CLABSIs
All positive blood culture events meeting National Health Safety Network (NHSN) criteria to be classified as CLABSIs from January 1, 2006, to December 31, 2016, were included. All events were reviewed by the hospital infection preventionist and were classified based on NHSN criteria in place at the time of the event. All CLABSIs, including those designated as MBI events from 2013 to 2016, are included.
Central Line Days
The unit’s central line days were calculated based on data reported by the hospital’s continuous improvement department. The hospital maintains a central line database that tracks central venous catheters from the time of placement to the time of removal. This database can be queried to provide a summary of each individual unit’s central line days. At the present time, the system is unable to provide a summary of central line days based on admitting service.
Patient Characteristics
Patient characteristics were extracted from review of the medical record to characterize the sample. Variables included the patient’s age at the time of the CLABSI, diagnosis, gender, admitting service, diagnosis, presence of relapsed disease, and neutropenia (absolute neutrophil count < 1.0/µL) at the time of the CLABSI.
Procedure
Ethical Considerations
Institutional review board approval with a waiver of informed consent was granted to support the review of individual CLABSI cases.
Retrospective Review
A retrospective review of CLABSI events occurring between 2006 and 2010 was conducted prior to the initiation of intentional CLABSI reduction strategies to provide a baseline for comparison.
Continuing Review
As part of the unit’s ongoing efforts to reduce CLABSIs, individual cases are reviewed with the hospital infection preventionist and summarized as they occur.
Data Preparation and Analysis
Data were entered into Excel spreadsheets in preparation for analysis. Data were organized into three key time periods associated with the implementation of unit-based CLABSI-reduction strategies. These included (a) 2006 to 2010: a 5-year preintervention baseline for comparison; (b) 2011 to 2012: implementation of the Children’s Hospital Association best practice maintenance care bundles; and (c) 2013 to 2016: implementation of formalized supportive care practices in addition to the maintenance care bundles.
CLABSI rates per 1,000 central line days were calculated for each of the three time periods as were rates for individual organisms. Exact binomial 95% confidence intervals were calculated for each rate.
Organisms were grouped based on the source of the organism using the NHSN master organism list (NHSN, 2017). Organisms listed on the mucosal barrier injury (MBI) tab of the master organism list were further divided into those organisms common to the mouth and those common to the lower gastrointestinal tract. The four groups of organism included in the analyses were (a) common commensal organisms (e.g., coagulase-negative staphylococci), (b) MBI organisms common to the mouth (e.g., viridans group streptococci), (c) MBI organisms common to the lower gastrointestinal tract (e.g., Klebsiella spp.), and (d) other pathogens that are not designated as common commensal or MBI-associated organisms (e.g., Pseudomonas spp.).
Patient characteristics were assessed for comparability across the three time periods (preintervention [2006-2010], bundles [2011-2012], and bundles + formalized supportive cares [2013-2016]) using chi-square tests. Poisson regression (with log [catheter line time] as offset) was used to compare CLABSI rates for the individual organisms and organism groups using post hoc Tukey HSD (honest significant difference) tests to compare across the three time periods.
All analyses were performed using R software (3.4.3) with results considered statistically significant if p < .05.
Results
Patient Characteristics
Table 1 summarizes demographic and clinical characteristics of patients who developed CLABSIs during each time period. Between 2006 and 2016, 265 CLABSI events were identified in 189 individual patients. Twenty of these events involved two or more organisms, and 289 total organisms were identified. No significant differences in patient characteristics were present across each of the three periods. CLABSIs most frequently occurred in children with hematologic malignancies who were being treated for a primary diagnosis of cancer by the oncology service. Fifty-two patients experienced two or more CLABSIs (range two to five). Within this subgroup of patients with repeat CLABSIs, 44 (85%) had a diagnosis of leukemia. Of note, no patients with sarcoma developed a CLABSI following the introduction of best practice bundles.
Patient Characteristics.
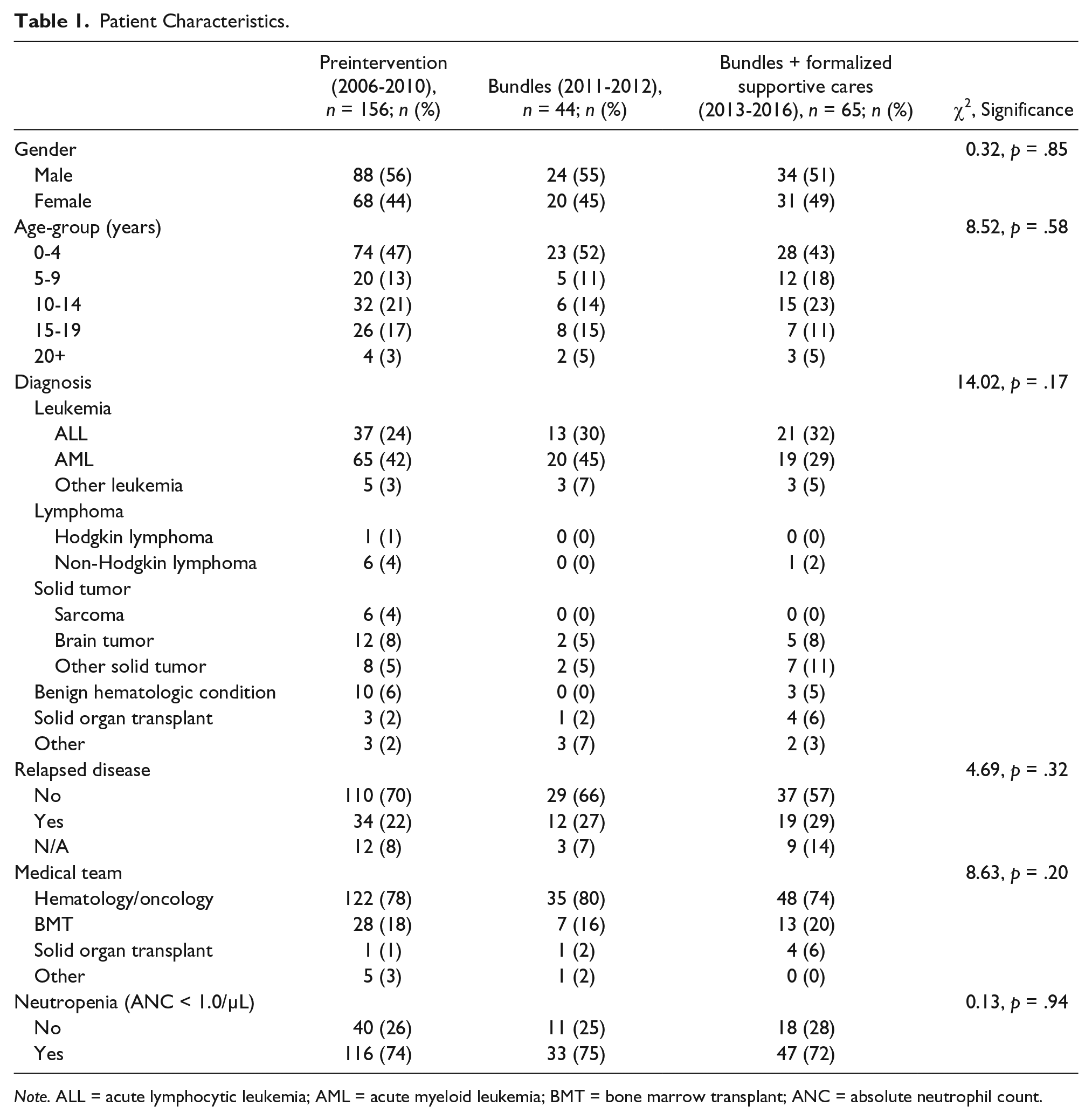
Note. ALL = acute lymphocytic leukemia; AML = acute myeloid leukemia; BMT = bone marrow transplant; ANC = absolute neutrophil count.
Overall CLABSI Rates
Table 2 presents a comparison of overall CLABSI events and rates across each of the three time periods. Overall, CLABSI rates decreased by an expected log rate of −1.48 (p < .01), that is, the CLABSI rate was e−1.48 = 0.23 times less following implementation of the bundles plus supportive cares compared with the preintervention period. Post hoc Tukey tests identified significant differences in rates only between the 5-year preintervention period and following implementation of enhanced basic supportive cares in addition to best practice bundles (z = −3.43, p < .01).
Comparison of CLABSI Events and Rates.
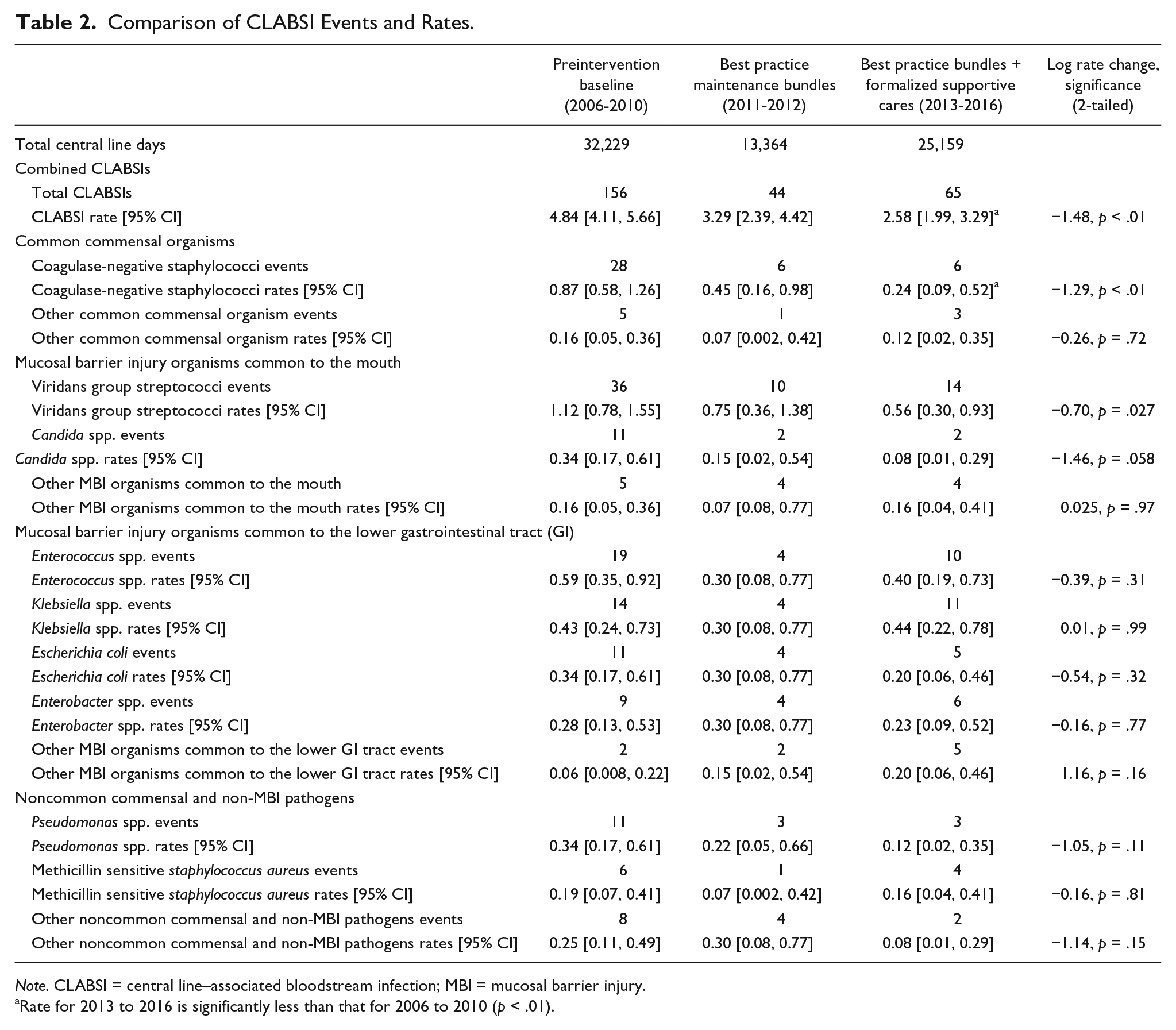
Note. CLABSI = central line–associated bloodstream infection; MBI = mucosal barrier injury.
Rate for 2013 to 2016 is significantly less than that for 2006 to 2010 (p < .01).
Individual Organisms
Among individual organisms, significant expected log rate decreases were present only for coagulase-negative staphylococci and viridans group streptococci. For coagulase-negative staphylococci, the expected log rate decrease was −1.29 (p ≤ .01), that is, the CLABSI rate was e−1.29 = 0.28 times less following implementation of the bundles plus supportive cares compared the preintervention period. For viridans group streptococci the expected log rate decrease was −.70 (p = .03), meaning the CLABSI rate was e−.7 = 0.497 times less following implementation of the bundles plus supportive cares compared the preintervention period. Of note, the expected log rate decrease for Candida species approached significance with an expected log rate decrease of −1.46 (p = .058), that is, the CLABSI rate was e−1.46 = 0.23 times less following implementation of the bundles plus supportive cares compared the preintervention period. Post hoc Tukey tests identified significant differences in rates of infection with coagulase-negative staphylococci between the preintervention period and following implementation of enhanced supportive cares (z = −2.87, p = .011). Although decreases in rates of infection involving Candida and Pseudomonas species did not reach statistical significance, the observed decreases were clinically important.
Organism Groups
Table 3 presents a comparison of CLABSI events and rates based on the four groups of organism. Expected log rate decreases were significant for three of the groups: common commensal organisms, MBI organisms common to the mouth, and other pathogens that are not considered common commensal or MBI-associated organisms (p < .01). Additionally, CLABSI rates were significantly less during 2013 to 2016 (bundles + formalized supportive cares) compared with 2006 to 2010 (preintervention comparison) for both common commensal organisms (z = −2.80, p = .014) and MBI organisms common to the mouth (z = −2.69, p = .019). CLABSI rates were unchanged for MBI organisms common to the lower gastrointestinal tract.
Log Rate Changes by Organism Group.
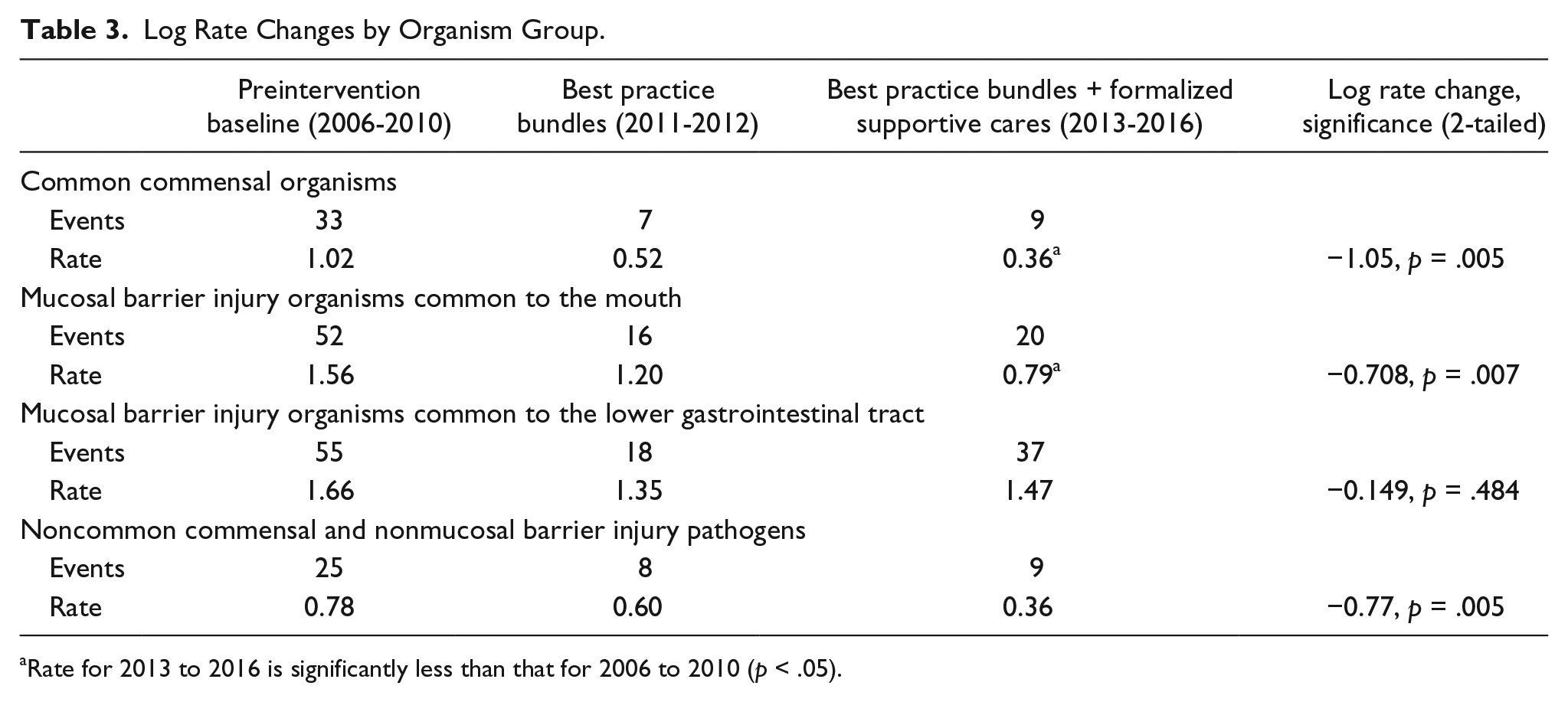
Rate for 2013 to 2016 is significantly less than that for 2006 to 2010 (p < .05).
Discussion
CLABSIs remain an important subset of infections for children with cancer and other conditions resulting in immune compromise. To date, interventions have emphasized the prevailing model of CLABSIs as resulting from organisms entering the bloodstream as a consequence of breaches in care. Despite these efforts, CLABSIs continue to occur. The addition of formalized supportive cares in addition to the best practice maintenance care bundles contributed to sustained significant decreases in the overall CLABSI rate at this institution; however, rates of infection involving MBI organisms common to the lower gastrointestinal tract did not decrease. The examination of data over an 11-year period provided important insights into the characteristics of patients who develop CLABSIs as well as organisms involved in CLABSI events.
Patient Characteristics
The clinical characteristics of patients who acquired CLABSIs over the 11-year period remained unchanged. Patients with leukemia continued to comprise the largest diagnostic group who developed CLABSIs, specifically during periods of prolonged and profound neutropenia. These patients also more frequently developed subsequent infections relative to other diagnostic groups. This project also identified subsets of patients at particularly low risk for infection, specifically, patients with sarcoma.
Organism Characteristics
Although overall CLABSI rates decreased over the 11-year period, the only two organisms for which significant rates of decrease were observed were coagulase-negative staphylococci and viridans group streptococci. Because these two groups of organisms have historically been the most common organisms involved in CLABSIs, decreasing the rates of infection involving these organisms has driven the decrease in the overall CLABSI rate. Despite overall decreases in the rate of viridans group streptococci, rates of infection involving this organism group remained the highest relative to other organism species.
Grouping the organisms into classes based on the NHSN’s master organism list supported additional examination of organisms involved in CLABSIs based on their potential source of introduction into the bloodstream. Decreases in rates of CLABSIs resulting from common commensal organisms, MBI organisms common to the mouth, and non-MBI/noncommon commensal organisms were observed. These decreases suggest current successes of interventions targeted at reducing the introduction of organisms through enhanced maintenance care of the central venous catheter and patient hygiene efforts targeted at reducing the concentration of bacteria on the skin and in the mouth.
Consistent with previously reported studies (Climo et al., 2013; Milstone et al., 2013), the rate of infection involving MBI organisms common to the lower gastrointestinal tract remained unchanged across the 11-year period. This lack of responsiveness to interventions to date supports current evidence that CLABSIs involving these organisms in patients with neutropenia likely represent a distinct subset of infection associated with translocation of organisms across injured mucosal tissue (Metzger et al., 2015; See et al., 2013). As such, these infections will require additional intervention strategies.
Clinical Implications
Results of this study provide guidance in directing interventions for ongoing efforts to reduce CLABSIs in pediatric hematology/oncology/transplant patients. Although past attention has been given to standardizing care across individual units and institutions, emphasizing more targeted interventions to selected subgroups of patients, specifically patients with leukemia, may provide a more meaningful approach. A recent study has demonstrated the safety and efficacy of administering levofloxacin to patients with leukemia during the induction period as antibacterial prophylaxis (Wolf et al., 2017). Such an approach may offer potential benefit to oncology service patients who remain hospitalized for count recovery during periods of profound and prolonged neutropenia and warrants investigation. Likewise, patients who are at particularly low risk for an infection may be able to avoid additional interventions such as CHG bathing and prophylactic antibiotics from which they are less likely to benefit.
The use of practice-based evidence techniques that emphasize a more rigorous description of unit-based data can support institutions in refining interventions targeted at the hematology/oncology/transplant settings. Treating CLABSI-MBI events as a distinct subset of infection with a distinct pathophysiology can help shift the paradigm of regarding hematology/oncology/transplant units as underperforming units. Reporting CLABSI rates with MBI events removed in addition to the overall CLABSI rates can further help to provide a more meaningful comparison across other units within and across institutions.
Limitations
Limitations of this project include data from a single institution. The scope of the patient population served by this institution may not be reflective of other settings, therefore, the results may have limited generalizability. Additionally, variations in institutional supportive care practices across institutions such as hospitalization during the count recovery period and the use of antibacterial prophylaxis during periods of prolonged and profound neutropenia may further contribute to variation in reported CLABSI rates across institutions. In 2016, this center adopted more stringent blood culture practices ensuring that two blood culture samples were obtained from patients developing new fevers and increasing the volume of blood obtained with each specimen. This practice change increased the potential for more CLABSIs to be identified, particularly those involving common commensal organisms and viridans group streptococci in which the same organism grew from both cultures.
Institutional mechanisms for reporting central venous catheter days during the time period reported in this article do not support further delineation of central line days based on patient diagnosis or admitting service. This limits the ability to complete more refined analyses of CLABSI rates among specific patient populations served by the unit.
A potential limitation of the analyses presented in this article is the additional delineation of MBI organisms. These organisms were attributed to either the oral cavity or lower gastrointestinal tract based on review of its primary location as part of the human host flora. For additional clarity in comparing trends over time, CLABSI rates for each major organism genus were provided to support comparisons.
Surveillance definitions for CLABSIs continue to be refined by the CDC. As a consequence, an event meeting criteria to be defined as a CLABSI in a given year may or may not have been classified as a CLABSI in a previous or subsequent year.
A limitation of the analytic approach is that it assumes immediate change as a result of the intervention and does fully address changes in variation and correlation following implementation of the intervention. Emerging statistical approaches, such as a robust interrupted time series model (Cruz, Bender, & Ombao, 2017) are designed to address these limitations and can be implemented in future longitudinal analyses.
Directions for Future Research
Directions for future research include ongoing attention to understanding individual patient characteristics. Within this study, nearly one third of patients experienced more than one CLABSI and 85% of patients with repeat infections had leukemia. Exploration of both disease-related and patient-specific characteristics may further support stratification of patients based on risk and guide more targeted interventions.
The lack of change in CLABSI rates involving MBI organisms common to the lower gastrointestinal tract emphasizes the crucial need for additional research and the development of interventions targeted at reducing this subgroup of infections. Regardless of whether these events are viewed as hospital-acquired, they represent an important source of morbidity for pediatric hematology/oncology/transplant patients. Areas of current interest include gastrointestinal dysbiosis, which can occur as a consequence of the illness and nutritional deficits, as well as exposure to chemotherapy, radiation, and antibiotic therapy (Galloway-Pena et al., 2016; Taur & Pamer, 2016). Failure of systemic immune responses, such as in the context of prolonged and profound neutropenia further contribute to infection risk. Polymorphisms in individual genes may further convey an increased risk of bacterial translocation in the context of an altered microbiome (Rayes et al., 2016).
Interventions targeted at reducing injury to the oral mucosa are also needed. Despite current improvements, MBI organisms common to the mouth remain an important source of infection, particularly in the context of profound and prolonged neutropenia. Low level laser light therapy has been proposed as means to promote the integrity of the oral mucosa, which may be protective against infection and has been reported to be tolerated by children (Eduardo et al., 2015; Migliorati et al., 2013).
As future studies are reported, attention needs to be given not only to reporting changes in overall CLABSI rates but also to changes in rates of infection involving specific organisms. Decreases in more common causative organisms such as coagulase-negative staphylococci can mask a lack of change in CLABSI rates involving other organisms (Climo et al., 2013). Such additional detail in reporting can provide a more meaningful evaluation of organisms for which a given intervention is or is not effective. Additional studies reporting the sustained effectiveness of interventions across time are also needed.
Conclusion
Results of this study emphasize ongoing challenges in reducing CLABSIs in pediatric hematology/oncology/transplant patients. Patients with hematologic malignancy, specifically leukemia, are most frequently affected by CLABSIs. While strategies to date resulted in decreases in some groups of organisms, rates of infection involving MBI organisms common to the lower gastrointestinal tract remained unchanged over an 11-year period. Study results emphasize the need for more specific, targeted interventions that address the underlying pathophysiology of these infections.
Footnotes
Authors’ Note
Andrew Wilson is also affiliated to PAREXEL International Corporation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The pre-intervention retrospective review of CLABSIs between 2006-10 was supported by a grant from the Utah Organization of Nurse Leaders.