
Abstract
Although overall survival from pediatric cancer patients has improved dramatically over the years, enhancements to health-related quality of life (HRQL) among children and adolescents are needed. The negative physical and psychosocial aspects related to the diagnosis and treatments of pediatric cancers not only impact HRQL during active treatment, but also well beyond into survivorship. A review conducted by Fardell et al. (2017) found that overall HRQL was significantly reduced among children with acute lymphocytic leukemia (ALL) during treatment, as well as in the extended posttreatment period particularly with the physical and emotional domains of HRQL. The emotional domains of HRQL typically include negative mood and anxiety. Danhauer et al. (2017) conducted a review of yoga as an intervention during cancer treatments among both pediatric and adult cancer populations, and while they found benefits on a number of measures very few studies focused specifically on children and teens with cancer. Although there are different styles of yoga, most yoga practices include a few main components: physical postures (i.e., asanas), breathing techniques (i.e., pranayama), meditation, and a final relaxation phase (i.e., savasana).
Background
In the general U.S. youth population, anxiety and depression are pervasive problems. Approximately 4.4 million children between the ages of 3 and 17 years have been diagnosed with anxiety and 1.9 million have clinical depression (Ghandour et al., 2018). Although there is little data on the prevalence of anxiety and depression, specifically among pediatric cancer patients and survivors, a study by von Essen et al. (2000) found higher levels of both these symptoms in this population when compared to healthy children. In a recent systematic review conducted by James-Palmer et al. (2020), yoga interventions were found to be effective in reducing both anxiety and depression among children and adolescents. Among the 27 studies, 10 were randomized clinical trials, 17 were cohort studies and a wide range of diagnoses were included (e.g., diabetes, sickle cell disease, cardiac disease, cystic fibrosis, and cancer). The two studies addressing yoga and anxiety among pediatric cancer patients included in the systematic review are also reviewed in the current report (Hooke et al., 2016; Thygeson et al., 2010). Although neither of these studies assessed depression, they both revealed decreases in the severity of anxiety.
Fatigue is a very common symptom in the oncology population that can affect all aspects of HRQL. Among children and teens with cancer, fatigue has been reported as one of the most distressing symptoms both during and following treatments (Nunes et al., 2017). According to the National Comprehensive Cancer Network (NCCN), strategies for helping to ameliorate fatigue among adult oncology patients include regular exercise, as well as psychosocial interventions (NCCN, 2020). Yoga is a practice that can positively impact both the physical and psychological burdens of cancer and has been recommended by the NCCN for individuals affected by cancer-related fatigue (CRF). Although very few studies have focused on the use of yoga in the pediatric oncology population, there have been many studies conducted among adult cancer patients, most of which have been in the breast cancer population. In a Cochrane review of 24 studies assessing yoga interventions among breast cancer patients, it was found that there is sufficient moderate-quality evidence supporting the use of yoga to reduce CRF (Cramer et al., 2017).
Yoga and meditation appear to be gaining popularity among children and teens in the United States as was determined by a 2017 report from the National Health Interview Survey (NHIS). The report showed that the percentage of children using yoga doubled from 2012 to 2017 (3.1% and 8.4%, respectively), whereas the use of meditation went from 0.6% to 5.4% during the same time period (NCCIH, 2018). Because yoga has become more widely accepted among children and teens, it may be an appealing gentle physical exercise, as well as a strategy to address mental well-being, that some pediatric cancer patients can embrace as a way to help them manage treatment-related side effects and the overall burden of cancer on their lives. Considering the known benefits of yoga on HRQL in the adult oncology population and on mental health in other pediatric populations, the goal of this review is to evaluate the current body of literature on yoga as a mind–body therapy for use in pediatric cancer populations.
Method
A search of the literature for this narrative review was conducted to identify research studies addressing yoga for children and adolescents with cancer between the years 2010 through 2020 using CINAHL, Ovid MEDLINE, PsycINFO, PubMed, and Scopus. The following search terms and/or Medical Subject Headings (MeSH) were entered into the databases: cancer, neoplasm, pediatrics, children, adolescents, and yoga. Search terms were combined using “AND” in the databases and filters were applied for publication date, language, and age. Inclusion criteria included (1) published in English in peer-reviewed journal, (2) study sample included children and/or adolescents, and (3) yoga as the primary intervention. Studies were excluded if the population included cancer patients over the age of 19 years, as well as studies that offered yoga as part of a larger psychosocial or mind–body intervention. For example, studies that had a Mindfulness-based Stress Reduction (MBSR) Program as a broad intervention includes yoga as a component. Due to yoga being one strategy embedded into a larger mind–body intervention, such as MBSR, it would be difficult to discern the impact of yoga specifically on the outcomes. Abstracts were reviewed to identify whether the studies focused specifically on yoga alone as an intervention in children and adolescents with cancer. Upon searching the literature, only eight studies specifically addressed yoga as a single intervention in children/adolescents affected by cancer. The search strategy can be found in the Appendix.
Results
The search process is illustrated in Figure 1 through the PRISMA flow diagram. Eight studies, all of which were nonrandomized studies, were found in the published literature. The results of these eight nonrandomized studies are summarized in Table 1. All reports were pilot and/or feasibility single-arm studies, half of which were conducted entirely while the children were inpatients (Diorio et al., 2015; Fukuhara et al., 2020; Geyer et al., 2011; Thygeson et al., 2010). The sample size ranged from 6 to 29 participants. The children ranged in age from 5 to 19 years and diagnoses included ALL, acute myelogenous leukemia, lymphoma, central nervous system (CNS) tumors, a mix of solid tumors, and one patient with Fanconi’s anemia requiring a bone marrow transplant. Four of the studies included a parent and/or caregiver and reported on one or more HRQL measures of those individuals, such as anxiety (Fukuhara et al., 2020; Geyer et al., 2011; Orsey et al., 2017; Thygeson et al., 2010). Five of the eight were U.S. studies, whereas the other three were conducted in Canada. All yoga sessions were led by individuals trained to teach yoga, but only one study mentioned that the instructors were trained in therapeutic yoga and only one of them indicated that the yoga instructor had specialized training for a pediatric cancer population (Orsey et al., 2017).
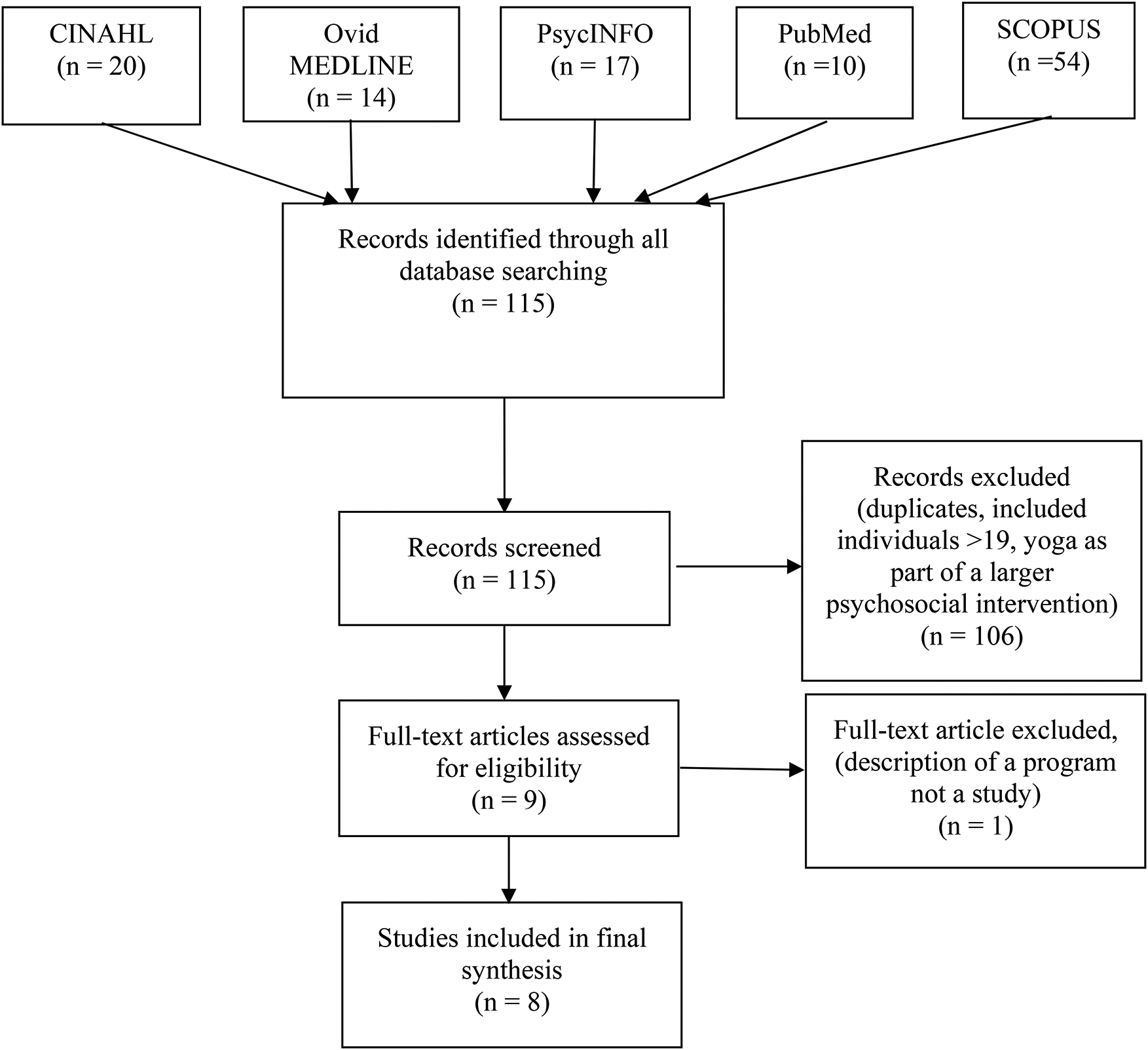
PRISMA flow diagram illustrating the review process.
Nonrandomized Studies of Yoga in the Pediatric Oncology Population.
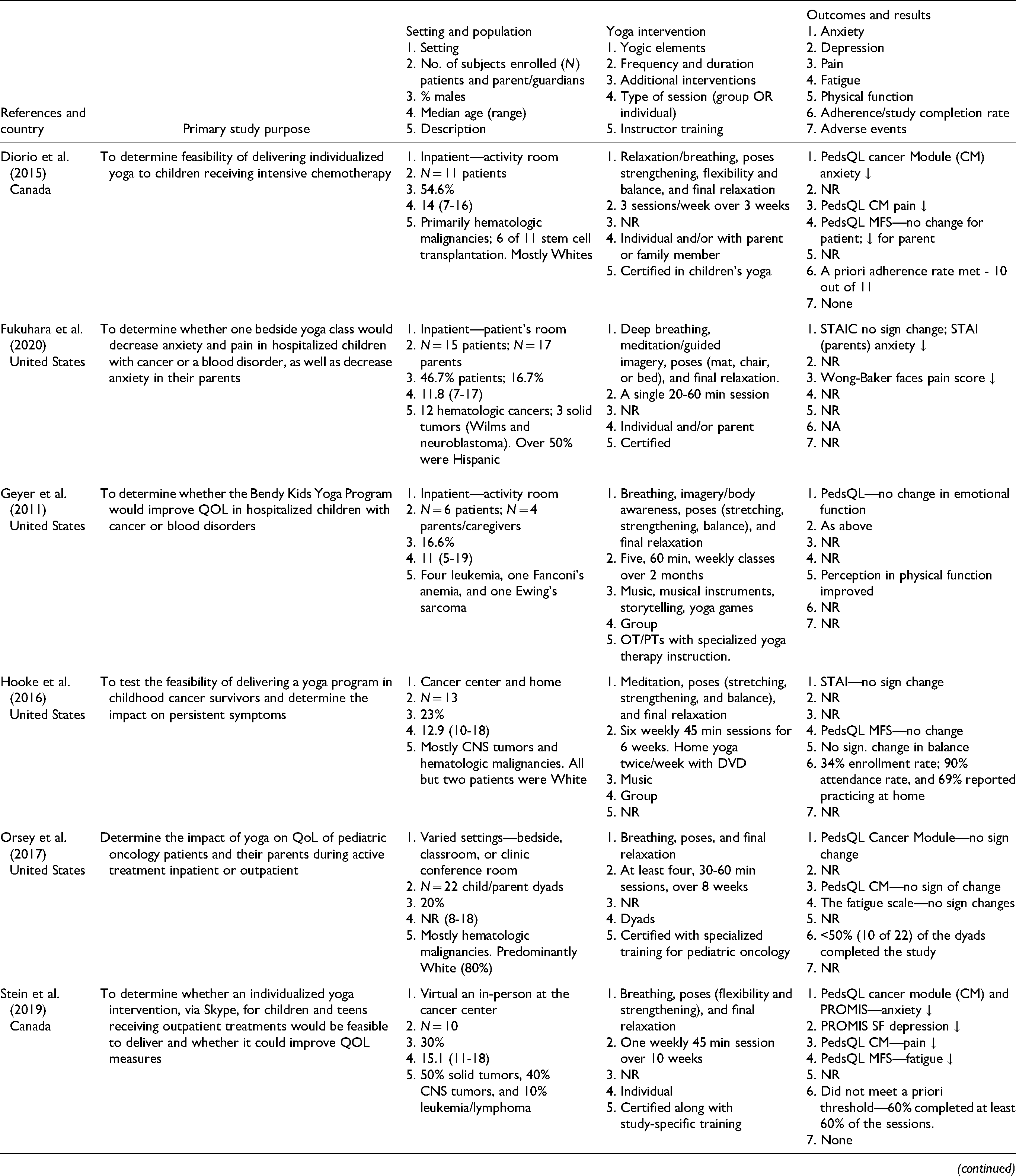
Note. NA = not applicable; NR = not reported; ROM = range of motion; STAI = State-Trait Anxiety Inventory; STAIC = State-Trait Anxiety Inventory for children; PedsQL CM = Pediatric Quality of Life Cancer Module; PedsQL MFS = Pediatric Quality of Life Multidimensional Fatigue Scale; PROMIS SF = Patient-reported Outcomes Measurement Information System short forms; QOL = quality of life; CNS = central nervous system.
Yoga interventions varied widely, but all included physical postures, breathing techniques, and the final relaxation, whereas some also incorporated meditation and imagery (Geyer et al., 2011). In all but one study (Wurz et al., 2014), it was reported that a combination of meditation and/or breathing exercises, physical poses, and final relaxation was included as part of the intervention. The intervention dose ranged from single sessions (Fukuhara et al., 2020; Thygeson et al., 2010) to twice-weekly yoga for 60 min for over 12 weeks (Wurz et al., 2014). Diorio et al. (2015) did not report on the length of time for each yoga session, but they were offered 3 times/week for 3 weeks. Among the studies conducted in the hospital setting, two were tailored and individually delivered with or without a parent/caregiver (Diorio et al., 2015; Fukuhara et al., 2020) and two were held in groups (Geyer et al., 2011; Thygeson et al., 2010). The study by Hooke et al. (2016) included home sessions with the use of a recorded DVD by the same yoga instructor and Stein et al. (2019) included individual virtual sessions (i.e., Skype).
With regard to outcome measures, the general Pediatric Quality of Life (PedsQL) questionnaire Acute Cancer Module and the PedsQL Multidimensional Fatigue Scale (MFS) were the most consistently utilized scales across studies. The State-Trait Anxiety Instrument (STAI), and/or the child version (STAIC) were used by three of the investigators (Fukuhara et al., 2020; Hooke et al., 2016; Thygeson et al., 2010). In addition to the use of the PedsQL, Stein et al. (2019) used the Patient-reported Outcomes Measure Information System (PROMIS) short form to assess anxiety, depression, fatigue, and anger. Only one study used the Wong-Baker Pain Scale (0–10) to subjectively measure physical pain (Fukuhara et al., 2020). Wurz et al. (2014) measured both subjective physical activity (Godin Leisure-Time Exercise Questionnaire) and objective physical function (e.g., range of motion, sit and reach, etc.). With regard to feasibility data, enrollment rates were reported by Hooke et al. (2016), Stein et al. (2019), Thygeson et al. (2010), and Wurz et al. (2014) with the last three studies also reporting on completion rates. The study by Stein et al. (2019) was the only study that collected video data for use in reviewing sessions for quality, as well as safety.
In the two studies that evaluated anxiety using the STAIC (Fukuhara et al., 2020; Thygeson et al., 2010), anxiety levels were reduced although not statistically significant. However, Thygeson et al. (2010) found the STAI scores were significantly lower following the yoga intervention among teens (p = .04) and parents (p < .001). In the study by Fukuhara et al. (2020), anxiety scores decreased among patients, but differences were not statistically significant. Scores for parents or guardians did change significantly on both STAI state and trait scores (p < .001; p = <.01, respectively) following a single yoga session. Hooke et al. (2016) found that teen scores on the STAI were not statistically significant following a 6-week yoga intervention, but there was a decrease in anxiety among the children (p = .04). The PedsQL was used in five studies to measure multicomponents of quality of life (Diorio et al., 2015; Geyer et al., 2011; Orsey et al., 2017; Stein et al., 2019; Wurz et al., 2014). In the studies by Orsey et al. (2017) and Wurz et al. (2014), improvements in patient’s total scores were found (p = .006 and p = .02, respectively). Geyer et al. (2011) revealed statistically significant improvements in physical function (p < .016) as reported by the patients. The PedsQL Acute Cancer Module subscales of worry revealed slight worsening in the studies by Diorio et al. (2015) and Stein et al. (2019). Wurz et al. (2014) included a few objective physical measures that showed statistically significant improvements in overall physical functioning (p = .01) and hamstring flexibility (p = .02). A change in pain scores using the Wong-Baker Pain scale was statistically significant (p = .045) indicating a reduction in pain following a single yoga session (Fukuhara et al., 2020).
Among the studies reporting on feasibility as a primary outcome (Diorio et al., 2015; Stein et al., 2019; Wurz et al., 2014), two met their a priori thresholds (Diorio et al., 2015; Wurz et al., 2014). Diorio et al. (2015) defined feasibility as the ability to deliver at least 60% of the planned yoga sessions in at least 70% of participants and 10 of 11 participants met the threshold. The studies by Hooke et al. (2016) and Thygeson et al. (2010) both reported on enrollment and adherence rates, but Hooke et al. (2016) also provided data on retention rate, which was not relevant for the study by Thygeson et al. (2010) because the intervention was a single session. Hooke et al. (2016) had a 34% enrollment rate, however the retention was 72% with 90% of participants attending all in-person sessions and 69% engaging in at least one weekly session at home using the DVD provided. Three studies did not report on feasibility data (Fukuhara et al., 2020; Geyer et al., 2011; Orsey et al., 2017). For those studies that assessed acceptability, qualitative feedback from participants was very positive (Diorio et al., 2015; Orsey et al., 2017; Stein et al., 2019; Thygeson et al., 2010). Themes related to both physical and psychological benefits and included statements, such as “yoga was fun,” “relaxing and calming,” “increased stamina,” “reduced need for pain and/or nausea meds,” and expressions that yoga was an “escape” from the difficulties of cancer. One teen from the study by Thygeson et al. (2010) stated that yoga, “calmed all my worries and helped strengthen some of my muscles.” Diorio et al. (2015) also noted that feedback from parents was positive in terms of the physical and psychological benefits for themselves and their children, but that there was a questionnaire burden from the four assessment points included in the study design. In the study by Stein et al. (2019) which was conducted in part online, one participant stated, “I loved the Skype sessions because I was in the comfort of my own home, so I felt more comfortable doing yoga.” Although the safety of the interventions was not discussed in most of the studies, it was noted that no adverse effects were reported (Diorio et al., 2015; Stein et al., 2019; Wurz et al., 2014).
Discussion
The purpose of this review was to evaluate the limited data that exists on yoga as a therapeutic mind–body intervention in the pediatric oncology population. All studies used nonrandomized single-arm designs and most were feasibility and/or pilot studies. The data supports the feasibility and safety of delivering yoga interventions to children and teens with cancer in both the inpatient and outpatient settings and looks promising for ameliorating some symptoms and improving physical function. However, the efficacy cannot be determined based on the small sample sizes and variability in interventions and measurement tools used to assess the many psychosocial and physical facets of quality of life. As previously mentioned, Danhauer et al. (2017) conducted a review of yoga as an intervention during cancer treatments among both pediatric and adult cancer populations. Their review included four of the eight studies discussed in this current paper (Diorio et al., 2015; Geyer et al., 2011; Thygeson et al., 2010; Wurz et al., 2014). Since the time of the previous review, three additional studies on yoga during active treatment have been published. The study by Hooke et al. (2016) was not included in the review by Danhauer et al. (2017), because the focus was on cancer survivors with persistent symptoms posttreatment.
Studies investigating yoga interventions for children and teens with various diagnoses are increasingly being reported in the literature, and many have been found to reduce both anxiety and depression. In a recent systematic review by James-Palmer et al. (2020), yoga interventions resulted in lower levels of anxiety and depression regardless of health condition. James-Palmer et al. (2020) included 27 studies, 10 of which were randomized clinical trials. Health conditions ranged from children with known mental health issues to those with diagnoses such as diabetes, cancer, cardiac disease, sickle cell disease, and cystic fibrosis. Although it was noted that the majority of the studies in the review by James-Palmer et al. (2020) were of low methodological quality, mostly due to the nature of the designs (e.g., lack of randomization, lack of reporting on feasibility, etc.), ∼70% showed some improvements in symptoms of anxiety and/or depression. Among the 16 studies reporting on feasibility, there was a completion rate of ∼84%. Very few investigators included data on adherence rates and safety, which in addition to a more rigorous study design, would be important for future studies to include. Results from the systematic review by James-Palmer et al. (2020) are encouraging and findings from the current review on yoga among children with cancer also reveal decreases in anxiety levels as well as moderate to high completion rates, although limited due to the small number of studies reviewed and the lack of randomization.
Several randomized clinical trials (RCTs) assessing the effects of yoga among adult oncology populations in active treatment have shown significant improvements in various outcome measures, such as anxiety, depression, sleep, pain, fatigue, nausea, and overall quality of life (Danhauer et al., 2017). Another review of 29 RCTs by Danhauer et al. (2019) focused on symptom management and yoga among adult oncology patients both in active treatment and/or posttreatment. Overall, findings revealed improvements in the symptoms of fatigue, stress/distress, sleep, and cognition. Although most of the studies have been conducted among breast cancer patients/survivors, there are single studies on patients with lymphoma, colorectal, and prostate cancer, as well as several studies which included a mix of different diagnoses. As a result of the mounting evidence showing significant improvements from yoga on various quality of life measures in breast cancer patients, the Society for Integrative Oncology (SIO) has recommended yoga as an evidence-based intervention for anxiety, depression, fatigue, sleep, and overall HQOL (Greenlee et al., 2017). In the future, it is possible that yoga may be recommended as an evidence-based therapy for other oncology patients, including pediatric oncology patients, but additional studies are needed.
In addition to improvements for patients’ HQOL as noted above, there could possibly be cost savings if yoga is incorporated more broadly into oncology care. Although the literature is scant in this area, there is a report addressing cost analysis of delivering yoga as part of a larger integrative approach to cancer care on an adult oncology inpatient unit. It was determined that compared to a control cohort group, those receiving the integrative approach used less medications for side effects such as pain, nausea, and anxiety, which led to lower medication costs (Kligler et al., 2011). This is an area worth further investigation to help gain support from clinicians, hospital administrators, researchers, and funding sources. The growing body of evidence from RCTs on the benefits of yoga in adult oncology patients has provided an opportunity to further explore this intervention in pediatric oncology.
Although the preliminary data in pediatric oncology points to improvements in some symptoms/side effects, RCTs with more rigorous designs are needed before efficacy can be determined. Based on their previous pilot work, Diorio et al. (2016) designed an individualized yoga program with low-, moderate-, and high-intensity versions, as well as a safety monitoring approach, for children hospitalized for either intensive chemotherapy or hematopoietic stem cell transplantation (HSCT) that could be incorporated into a clinical trial for the purpose of increasing mobility and providing relaxation during prolonged hospitalization. This could be a model for other inpatient oncology yoga studies for children and teens focused on additional symptoms and treatment-related side effects. Recognizing the safety of therapeutic yoga intervention in this very vulnerable subpopulation (e.g., children undergoing intensive cancer treatments) should allay some fears about concerns for injuries. Factors such as the training of the yoga instructors and the recognition of comorbidities in children involved in a yoga intervention are also important to consider in helping to assure safety in a study. Because therapeutic yoga is typically a gentle form of exercise, the threshold for conducting a study among the pediatric population is generally low.
Although future studies with randomized controlled designs and larger sample sizes are warranted to further explore this important area, additional elements of study design that need to be addressed are consistency in reporting on psychometrics of the instruments used to measure concepts, such as anxiety, depression, fatigue, and pain. For example, it was found in a review of studies using instruments to measure anxiety among children receiving chemotherapy and/or an HSCT that none of those focused on HSCT included reliability and validity data (Lazor et al., 2017). The review by Lazor et al. (2017) also found that there was some consistency across studies for the use of specific measures of anxiety in this population; the most commonly used was the STAI in 46 of 78 studies. One benefit of this is that it can be used among teens and parents, and the STAIC version can be utilized with children.
Only one of the studies included data on objective physical function (Wurz et al., 2014), in addition to subjective emotional well-being and HQOL. The findings for statistically significant improvements in some physical function and flexibility measures warrant further study with objective measures of physical health in addition to perceived physical function. Geyer et al. (2011) found significant improvements in perceived physical function, which may suggest the possibility for objective improvements as well. However, from the studies on yoga in adult oncology populations that included any objective physical fitness outcomes (e.g., actigraphy), only one of five studies showed statistically significant improvements (Danhauer et al., 2019). Relevant factors to take into consideration for the measurement of physical fitness parameters would be the type of yoga intervention and the dose of yoga (i.e., number of sessions per week, length of study, and adherence).
There were a wide range of interventions with respect to the frequency and duration of the yoga sessions, as well as with the length of time for the study. This with the fact that symptoms across studies were measured with a variety of measurement tools, makes it very challenging to compare data on symptom outcomes such as anxiety, depression, fatigue, and pain. However, several studies showed some reductions in anxiety scores among children, teens, and/or parents (Diorio et al., 2015; Fukuhara et al., 2020; Hooke et al., 2016; Stein et al., 2019; Thygeson et al., 2010), fatigue (Stein et al., 2019), and pain (Diorio et al., 2015; Fukuhara et al., 2020). The majority of studies utilized either the PedsQL with or without the Acute Cancer Module or the STAI general version for teens and parents and the children's version (STAIC) for those younger than 13 to measure anxiety.
Among these eight studies, there was also variation in the settings where yoga was being offered, mostly inpatient settings. Although there is a need for further studies in the inpatient setting especially when children and teens are expected to be hospitalized for long periods of time, such as for HSCT, there is also a need for studies in the outpatient and/or home setting. Offering either individualized or group yoga online following some inpatient and/or outpatient instruction would be an area of study worth investigating. Considering that many pediatric patients travel far distances for their cancer care, an online yoga program may be more feasible than sessions offered at the hospital or clinic setting and may be beneficial for lingering physical symptoms as well as for mental health (Stein et al., 2019).
From the data presented, it appears as though yoga is both safe and feasible to deliver in the pediatric oncology population, although RCTs are needed. Pediatric oncology nurses may be well poised to help educate patients and their families, as well as colleagues, about the potential benefits of yoga in reducing treatment-related side effects and improving the overall quality of life.
Summary
Considering the many distressing physical and emotional symptoms and/or treatment-related side effects among pediatric oncology patients and findings from the literature on the benefits of yoga, this is an important topic to further explore. Yoga is increasingly being utilized by adults affected by cancer and also by children and teens in general. As a therapeutic mind–body strategy, yoga has been found to not only alleviate suffering from effects of cancer and treatments, but it may also help instill a sense of personal control over one's physical, emotional, and spiritual health. Adult cancer yoga programs are becoming more prevalent in cancer centers across the country and will continue to expand into the pediatric oncology setting as more data reveals the advantages and safety of this gentle mind–body practice. However, future studies, including RCTs in pediatric oncology patients should provide more thorough descriptions of yoga intervention protocols, including setting, dose, and outcome measures, as well as other factors that may affect the acceptability of yoga in this special population. Designing yoga interventions with consistency in mind will help lead to a stronger body of evidence.
Footnotes
Appendix
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.