
Abstract
Pandemics create social dilemmas. Everyone benefits from health behaviors that reduce the transmission of damaging infectious diseases. But people may not want to bear the costs of engaging in health behaviors themselves. Research suggests that if an action (like failing to engage in a health behavior) has consequences for others (i.e., produces externalities), those others will disapprove of the behavior and expect others to also disapprove. In the pandemic context, this argument suggests that norms will support health behaviors. But in situations in which some subgroups are affected by the virus and others are not, norms supporting health behaviors should be weaker. This is because people at risk from a virus are likely to be more supportive of health behaviors than those who are not. And people are likely to expect individuals in groups affected by a virus to support health behaviors more than those who are not affected. We use two online vignette experiments to test this externalities argument in the context of a novel virus. Results partially support the hypotheses. Theoretically, the study contributes to understanding of how patterns of externalities affect normative beliefs and expectations. Substantively, it has implications for messaging about the effects of viruses and the promotion of health behaviors aimed at reducing disease transmission.
Pandemics can create substantial health risks. In recent years, diseases of concern have included Covid-19, HIV, Ebola, Mpox, avian flu, and others. Risks of a pandemic occurring are increasing due to climate change, urbanization, and other factors (e.g., Carlson et al., 2022; Marani et al., 2021; Williams et al., 2023). Experts argue that human behavior plays a role in preventing and managing outbreaks (e.g., Internal Medicine, 2025).
But pandemics are challenging to address in part because an actor’s health behavior decisions affect not just that actor, but also others in the community. In the case of viruses, there are a range of strategies that, depending on the particular virus, might affect disease transmission, such as masking, distancing, vaccination, handwashing, and ventilation. Everyone benefits if community members implement strategies that reduce the transmission of damaging infectious diseases. For example, in the case of an airborne virus everyone is better off if everyone masks. But any individual might prefer to avoid the discomfort, hassle, or other costs of doing so (especially if they do not think they will personally be harmed by the virus) (see, e.g., Diekmann, 2022). When an actor fails to engage in health protective behaviors, they put not only themselves, but others at risk.
Norms may help to encourage health behaviors (e.g., Cislaghi and Heise, 2019; Rimal and Real, 2005; Zhang et al., 2022). Norms are rules governing behavior that are socially enforced (Horne, 2001). When a norm exists people expect that others disapprove of a behavior and will react negatively to those who engage in that behavior. These expectations about the extent to which others think one should or should not engage in a behavior are normative expectations (Bicchieri, 2017). Individuals also hold opinions about whether people should or should not engage in a behavior; these are normative beliefs, and indicate a demand for norms to regulate that behavior (Coleman, 1990).
Where might such normative beliefs and normative expectations come from? One source may stem from the fact that some categories of people may be more vulnerable to a virus than others. That is, the harm caused by a virus may be distributed unevenly, which in turn means that some categories of people are more likely to benefit from health-protective behaviors than others. In this study, we are interested in the patterns of normative beliefs and normative expectations that may emerge depending on the distribution of the benefits created by health-protective behaviors (and the harms that occur when individuals fail to engage in them). We ask: how does the distribution of harm associated with an individual’s failure to engage in a public health behavior affect normative beliefs about the behavior, and normative expectations about how much others approve or disapprove of it? We expect that when people generally are affected, they will support health protective behaviors themselves and will expect others to think the same. If only a minority is affected, most people will not support the behavior and will not expect most others to either. However, when only a subgroup is affected, members of the subgroup will support health protective behaviors, but will not expect people who are outside of the subgroup to do so. Theoretically, the study provides insight into how patterns of externalities affect normative beliefs and expectations. Substantively it suggests that messaging regarding who is at risk from a virus has implications for norms encouraging people to engage in behaviors that prevent the spread of that virus.
Theoretical background
A long-standing theory argues that norms emerge in response to externalities (e.g., Coleman, 1990; Demsetz, 1967; Ullmann-Margalit, 1977). The assumptions underlying this argument are that an “action that has externalities generates interests in the action among those actors who experience the externalities,” and that actors will generally view positively actions that benefit them and view negatively actions that harm them (Coleman, 1990: 249; Opp, 2018). Note that the assumption here is that an individual is interested in externalities that they themselves experience. They will have an interest in those behaviors being regulated in order “to induce the direction that benefits them” (Coleman, 1990: 251). The implication is that people will approve of externality-producing behaviors that benefit them and disapprove of those that harm them. (Note that it is possible that people might also care about externalities that affect others, but this is not our core argument.) Under certain conditions, externality-producing behavior will be sanctioned (Coleman, 1990).
Research has both supported and challenged pieces of this argument. Consistent with the argument, there is experimental evidence that people punish failures to contribute to a group – that is, they react to externalities (e.g., Yamagishi, 1986). Some of this work challenges assumptions about individual rationality and self-interest (e.g., Fehr and Gächter, 2002; Fehr and Gintis, 2007). Other work retains the underlying assumptions and tests implications of the externalities argument. It shows, for example, that people who receive the greatest net benefit from sanctioning can emerge as sanctioners if the personal benefit from doing so is greater than the cost (Przepiorka and Berger, 2016; Przepiorka and Diekman, 2013), and that, depending on relationships between group members, the size of externalities may or may not produce more sanctioning (e.g., Balafoutas et al., 2016; Horne, 2008).
Much of this work focuses on sanctioning. But because the incentives related to sanctioning (e.g., Piskorski and Gorbatâi, 2017) are arguably different from those for internal states, studies of sanctioning do not necessarily tell us much about normative beliefs (demand for norms). To test the effect of externalities on normative beliefs, researchers need to study that association directly (see, e.g., Eriksson et al., 2023 showing that people disapprove of externality-producing behavior). In addition, work on sanctioning also does not necessarily tell us much about normative expectations – a key component of norms (Bicchieri, 2017; for examples of work that focus on normative expectations but that do not specifically address externalities see Dodoo et al., 2020; Horne and Johnson, 2021). Normative beliefs and expectations matter because normative beliefs may be precursors to sanctions (Coleman, 1990) and both normative beliefs and normative expectations may affect behavior even in the absence of sanctions (Andrighetto et al., 2015; Tankard and Paluck, 2016). As such, improved understanding of normative beliefs and expectations fundamentally advances theory on normative social processes.
Here we apply Coleman’s argument to make predictions about how the distribution of externalities affects normative beliefs. In the pandemic context, the externalities argument would predict that when people are at risk from a virus, they will support health behaviors that reduce its transmission. That is, there will be a demand for norms that encourage the health behavior. We also extend the externalities argument to consider normative expectations. We anticipate that people will expect others to act according to their interests -- normative expectations will reflect people’s perceptions of others’ interests in a behavior. Thus, externalities will affect not just people’s normative beliefs, but also their normative expectations. The reduction in the risks of transmission that are associated with a health behavior will produce normative expectations that others approve of the behavior.
But this externalities argument applies most clearly when everyone has the same interests in a behavior. In many instances, however, the effects of a particular behavior may vary depending on the group or category to which people belong. There is much less research on the second situation than the first. Some studies explicitly compare conjoint norms (where the beneficiaries and targets of the norm are the same) to disjoint norms (where the beneficiaries and targets of a norm are different). They show that when norm beneficiaries and targets differ, there may be more free-riding than when norm targets also benefit from the norm enforcement, because obedience provides no benefit to the norm target, and further, that punishment is likely to be more effective when the interests of norm targets and beneficiaries are the same rather than different (Rauhut and Winter, 2017). Research also suggests that when conjoint and disjoint norms are in competition, conjoint norms are likely to be more salient (Teekens et al., 2025). Some work suggests that people’s expectations about the extent to which others will approve or disapprove of a behavior depends on whether those others share the interests of the person affected by the behavior. For example, in Ghana, people expect that men will be more disapproving of a wife’s misbehavior than other women (Dodoo et al., 2020).
The public health arena presents a context in which people may be affected differently by the same behavior (e.g., CDC, 2025a; 2025b). In the case of a virus, it is possible that some people (such as children, the elderly, or immune-compromised individuals) might be more negatively affected by a virus than others – the cost of a virus might be negligible for some people (ranging from no symptoms at all to a slight cold, for example) whereas others may end up with serious illness, hospitalization, and even death. For example, with regard to Covid, Diekmann (2022) points out that some people are more vulnerable to the virus than others. But he does not build on this fact to develop predictions regarding normative expectations and normative beliefs that might emerge in response to the distribution of those vulnerabilities. Other research finds that those who experience higher costs (serious health consequences) would prefer that everyone engage in health protective behaviors and have less trust in those who do not (see e.g., Iacono et al., 2021).
Building on this work, we argue that, to the extent that people benefit from others’ health behaviors, they will approve of people who engage in those behaviors (and disapprove of those who fail to do so). They will also expect people who share their interests to do the same. But those who are not affected by the virus (or are only very mildly affected) would have less reason to support health behaviors and would expect people like them to think similarly. The implication is that there will be different patterns of normative beliefs and normative expectations depending on who is affected by a disease and the health behaviors that reduce its transmission. Below we describe two studies conducted in spring 2025 that examine the effects of patterns of externalities on normative beliefs and normative expectations.
Study 1
We consider first how most people will react if a virus affects everyone or if it affects a subset of immune-compromised individuals. According to the externalities argument, because individuals are at risk if a virus is dangerous for everyone, they will be more supportive of health interventions that reduce transmission than if the virus is only dangerous for a subset of other people. If only a subcategory of the larger group is affected by a virus, then there may be little demand for health behaviors among group members generally and little expectation that people in general support such a norm.
We focus on two health interventions – masking and ventilation. Both are important strategies for reducing transmission of airborne viruses (CDC, 2025c; EPA, no date).
Masking is an individual behavior that has consequences for other group members. Everyone is better off if most people mask, but any individual might prefer not to mask because of costs such as discomfort, the price of masks, etc. (Diekmann, 2022). If a virus has equally negative effects on everyone, then the same people would benefit from and be targets of a masking norm. In such a situation normative beliefs and expectations will support masking. However, if the virus affects a subgroup, but not the majority, then the majority would not benefit from a norm favoring masking. Most people will not support a masking norm and will expect that most others do not support a masking norm either.
Organizations can also help to reduce disease transmission by ensuring that they have good ventilation in their spaces (EPA, no date). We focus in particular on organizations that serve the public such as stores and healthcare facilities. In general, if people are aware that ventilation reduces transmission, then they would prefer that such organizations have good ventilation and expect others to share that opinion. The organization (e.g., stores or healthcare facility) would be the target of the norm and the public (who use the organization’s services) would be the beneficiaries. (Of course, individuals who work at the organization would also benefit.) Given that people will benefit from ventilation, they would support norms favoring ventilation and expect others to do the same. Again, we expect that norms will be more supportive of ventilation when the virus affects everyone (including the individual) than when it affects a subset of people the individual does not belong to. Similarly, people’s expectations that others support ventilation will be stronger when the virus affects everyone.
These predictions are based on the argument that people respond to externalities. But it is unlikely that externalities are the only thing that people respond to; other factors may play a role as well. In particular, political allegiances may matter. Health behaviors in the US have become highly politicized (e.g., Yam, Kikuchi and Pula, 2015). Health behaviors in the context of Covid are a prominent example (e.g., Hart et al., 2020; Stroebe et al., 2021) with, for example, Republicans being more disapproving of masking than Democrats (e.g., Gelfand et al., 2022; see also accounts in the media: Franck, 2020; Peters, 2020; Washington Post, 2020). And the Covid-related political divide seems to have spread to other contexts (e.g., Lacour and Bell, 2024). If people may bring pre-existing beliefs about viruses and health behaviors into the experimental setting, then their political orientation may be relevant.
The theory we test does not address possible political dynamics in how people respond to externalities. And yet the current political conditions surrounding the health behaviors we study required that we consider the possibility. Given past research on masking and other methods of limiting contagion during Covid, we can expect that Democrats will express more support for masking and ventilation generally than Republicans and that people will expect more support among Democrats generally than Republicans. Addressing these mean level differences in beliefs and expectations is straightforward and does not alter the argument we investigate. Doing so also provides additional information on how health behaviors are perceived in current times.
Of more concern is the possibility that externalities have different effects depending on political orientation. This could arise if political orientation makes participants particularly sensitive to (or dismissive of) information provided in the experimental manipulation, or if groups differ in the extent to which they carry over pre-existing beliefs into a new setting. The investigation of such questions around political dynamics could have important implications for theory as well as policy on public health. That said, the theoretical arguments we investigate do not provide direction that would produce hypotheses about such interaction effects. Moreover, the future pursuit of this line of inquiry would benefit from improved understanding of the arguments about externalities above.
Thus, our focus here is on the effects of the distribution of externalities of a novel virus, but given the politicized nature of the empirical context, we did not think we could ignore political orientation. Accordingly, although we propose no hypotheses regarding the effects of political orientation, we designed our study to allow us to check for differences between Republicans and Democrats and the possibility that externalities differed depending on political orientation. But our theoretically driven hypotheses focus on the effects of externalities. We return to this issue in the Conclusion to suggest important avenues that could be addressed in future research.
Here we propose:
Personal normative beliefs and normative expectations supporting masking will be stronger if a virus has negative consequences for all than if it has negative consequences for a subgroup.
Personal normative beliefs and normative expectations supporting ventilation will be stronger if a virus has negative consequences for all than if it has negative consequences for a subgroup.
Design
Study 1 had a 2 x 2 between-subjects design crossing externalities (the virus affects immune-compromised individuals vs everyone) by political orientation of the study participant (Republican vs Democrat). The manipulation of externalities is the core feature, enabling tests of H1 and H2. Incorporating political orientations of the study participants into the study design allows us to check whether externalities operate differently across political orientation.
Participants and procedures
Participants were recruited via Prolific, an online research hosting site similar to Amazon’s Mechanical Turk, but designed for academic researchers. Research suggests that Prolific produces results comparable to or better than results using other similar platforms (Douglas et al., 2023; Peer et al., 2017). Our study was listed on the Prolific site. We screened for volunteers who were adults (age 18 and older) living in the U.S. In order to assess differences across political orientation, we also screened for those who identified with the Republican or Democratic parties. Those who were interested clicked on the study link. They completed a consent form. They were randomly assigned to one of the experimental conditions and each participant read only one version of the vignette. They then answered questions about it, responded to a manipulation check, and provided some sociodemographic information.
Power analyses suggested a sample size of 88 per cell to detect moderately small effect sizes (Cohen’s d = .30, or f = .15, and assuming p = .05 and power = .80). We slightly oversampled. Our final sample consisted of 389 participants. Eleven percent failed the manipulation check in the immune-compromised condition; four percent failed in the everyone condition. Results are generally consistent whether those who failed the manipulation checks are excluded or not. We report the results of analyses for the full sample (Aronow et al., 2019; Mize and Manago 2022).
The sample was 56% female and 73% white. Mean years of education were 15.25 years (SD = 2.04). Average age was 40.82 (SD = 13.31). In addition to screening for political orientation, we asked participants with which party they most identified. Half (51%) of the sample identified as Democratic and half (49%) as Republican. This measure was very close to the prescreen measure. We conducted analyses using this measure (rather than the prescreen) – results are comparable regardless of the indicator used.
Vignette conditions
Participants first read a description of a novel virus (the manipulated phrases are italicized below): Assume there is a novel virus that has spread around the world. Human beings have no immunity to this new virus. The virus is airborne meaning that it is transmitted primarily through the air. The virus is [harmless for most people, but is] dangerous for [people who are immune compromised/all Americans], with a risk to [immune compromised individuals/everyone] of serious long-term disability and death. Because the virus is airborne, mask wearing can significantly reduce its transmission. If you wear a mask you reduce your own risk. You also reduce the risk to others.
At this point, the participants answered questions about masking. Then they read the following text: So far we have talked about masks. Masks are one strategy for reducing the rate of disease transmission. Good ventilation in buildings can also significantly reduce the risk. This can be achieved economically by using portable air filters.
After reading the above statement, participants answered questions about ventilation in organizations “like stores, health care facilities, etc.”
Measures
To assess personal normative beliefs, we asked participants about whether they thought everyone should wear masks (0 = definitely should not; 10 = definitely should). To measure normative expectations, we asked about participants’ expectations that most others would think everyone should wear masks (0 = definitely should not; 10 = definitely should). We asked parallel questions about normative beliefs and expectations regarding ventilation. Higher scores mean more support or expected support for masking or ventilation. In order to check whether our results were consistent regarding expectations about Republicans and Democrats we asked about people’s normative expectations regarding support for masking and ventilation among Republicans and Democrats. And we solicited the sociodemographic information identified above. 1
Results
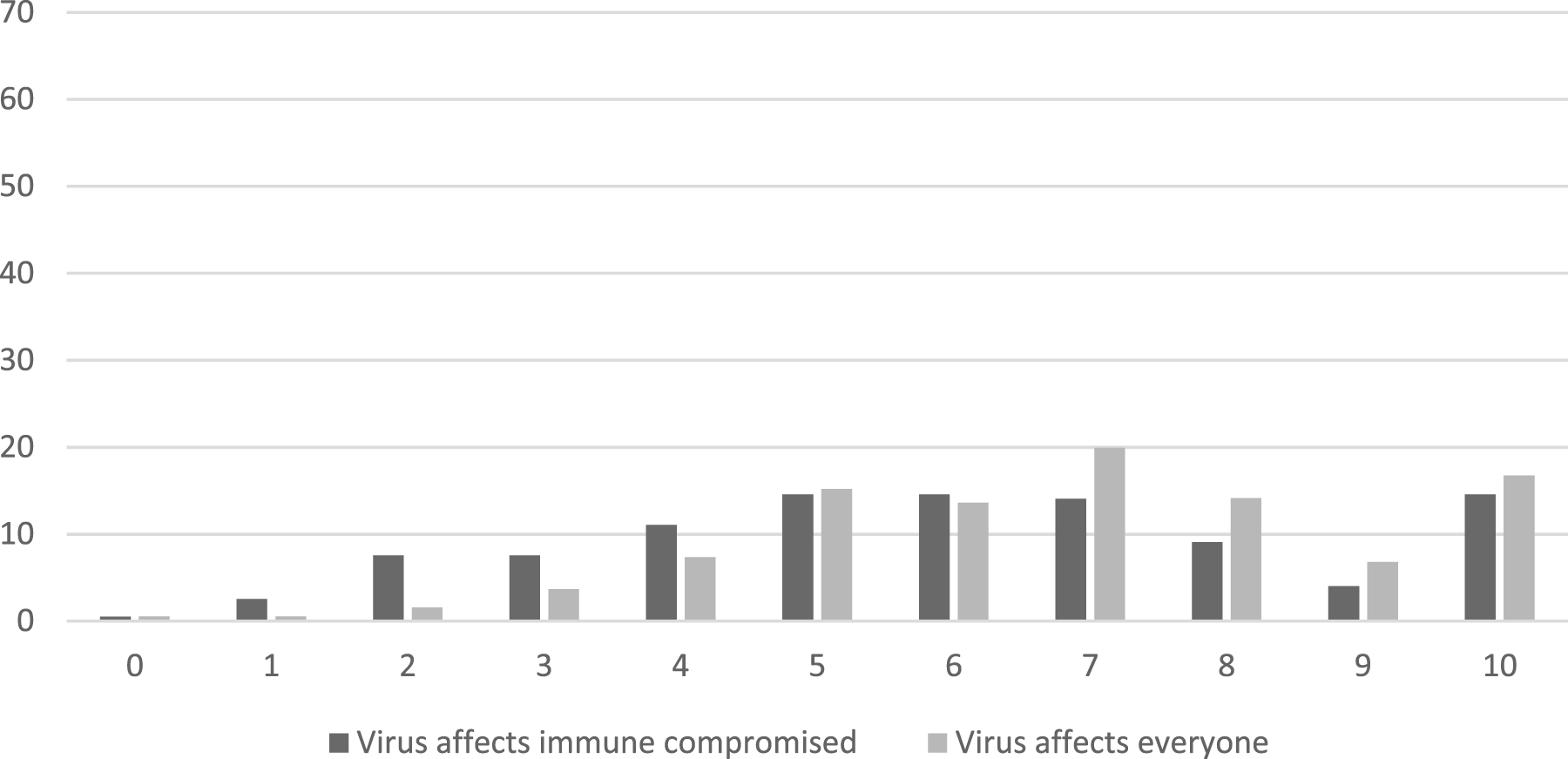
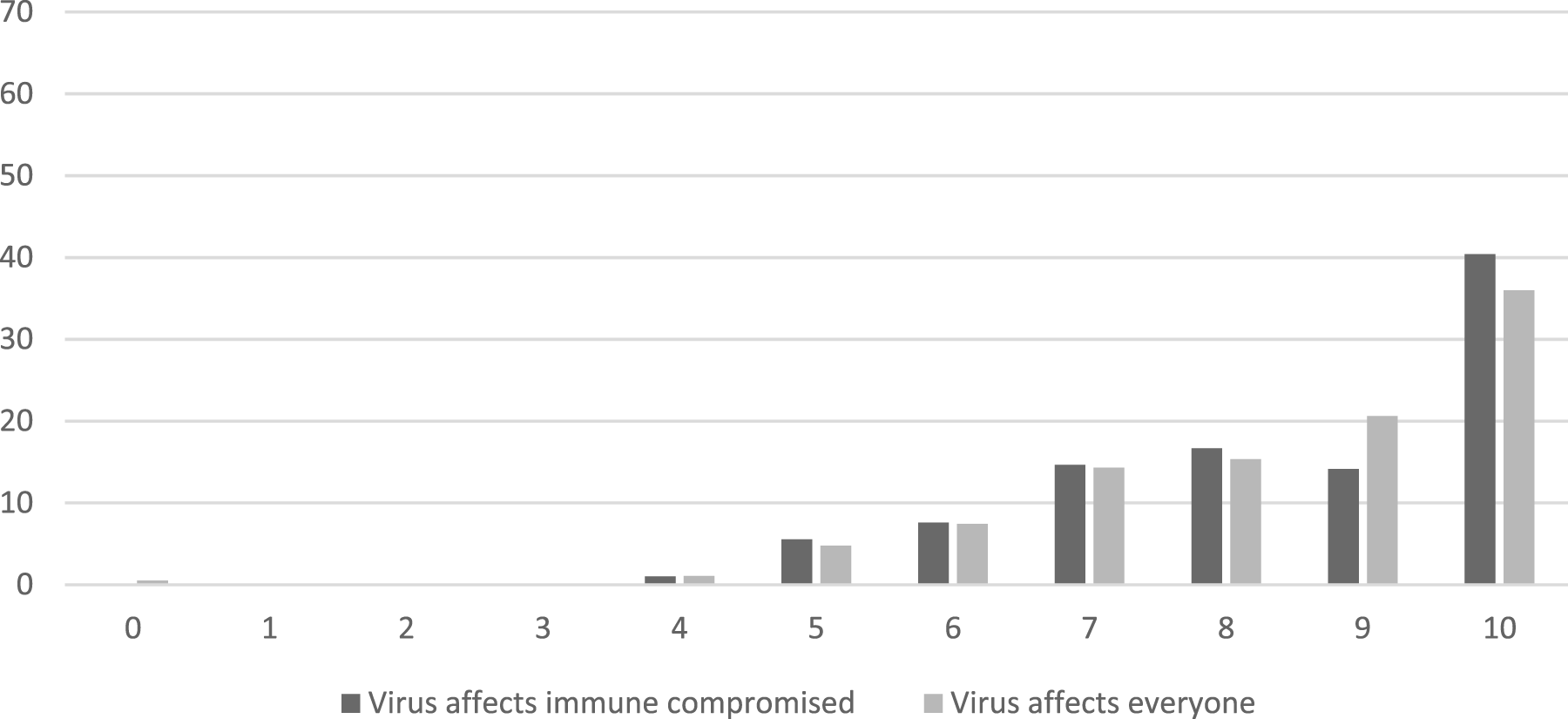
Figures 1 and 2 report the distribution of participant responses about masking by experimental condition. Personal and normative beliefs about masking in the study were somewhat correlated (r = .29) but also clearly distinct. Participants were generally supportive of masking and expected others to be as well. As shown in Figure 1, less than five percent of participants selected zero (“definitely should not”) for their own beliefs, regardless of which experimental condition they were in. In contrast, nearly half to two-thirds of participants selected 10 (“definitely should”) to indicate their own support of masking, depending on whether the virus affected a subgroup or everyone. Participants’ personal normative beliefs are more approving of health behavior than what they expect of others. Figure 2 indicates that relatively few participants expected that others would think people definitely should mask, instead expecting more moderate levels of support (i.e. ratings of 5-8) than shown for beliefs in Figure 1. Distribution of normative beliefs suporting masking by experimental condition (Study 1). Distribution of normative expectations about support for masking by experimental condition (Study 1).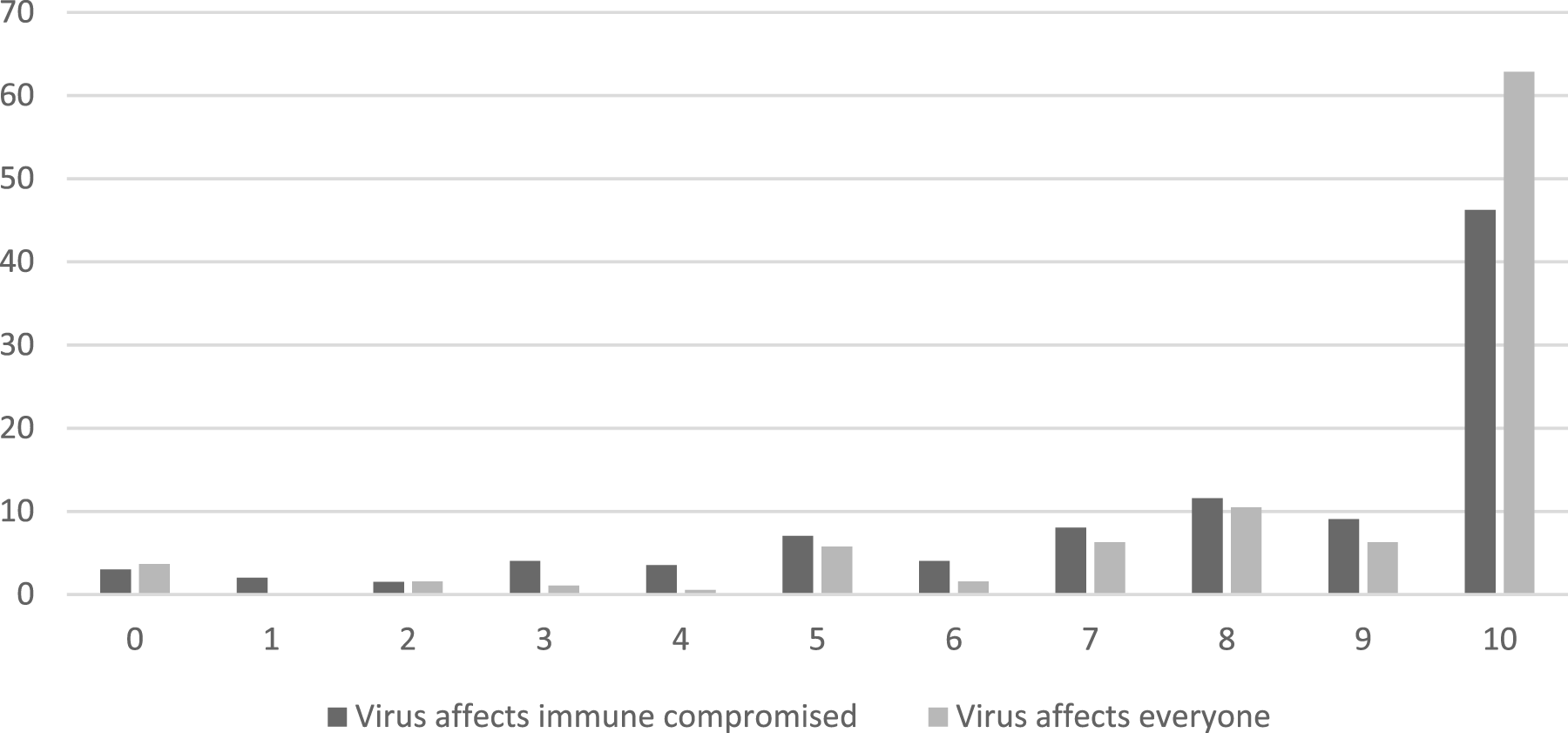
Norms about mask wearing and ventilation.
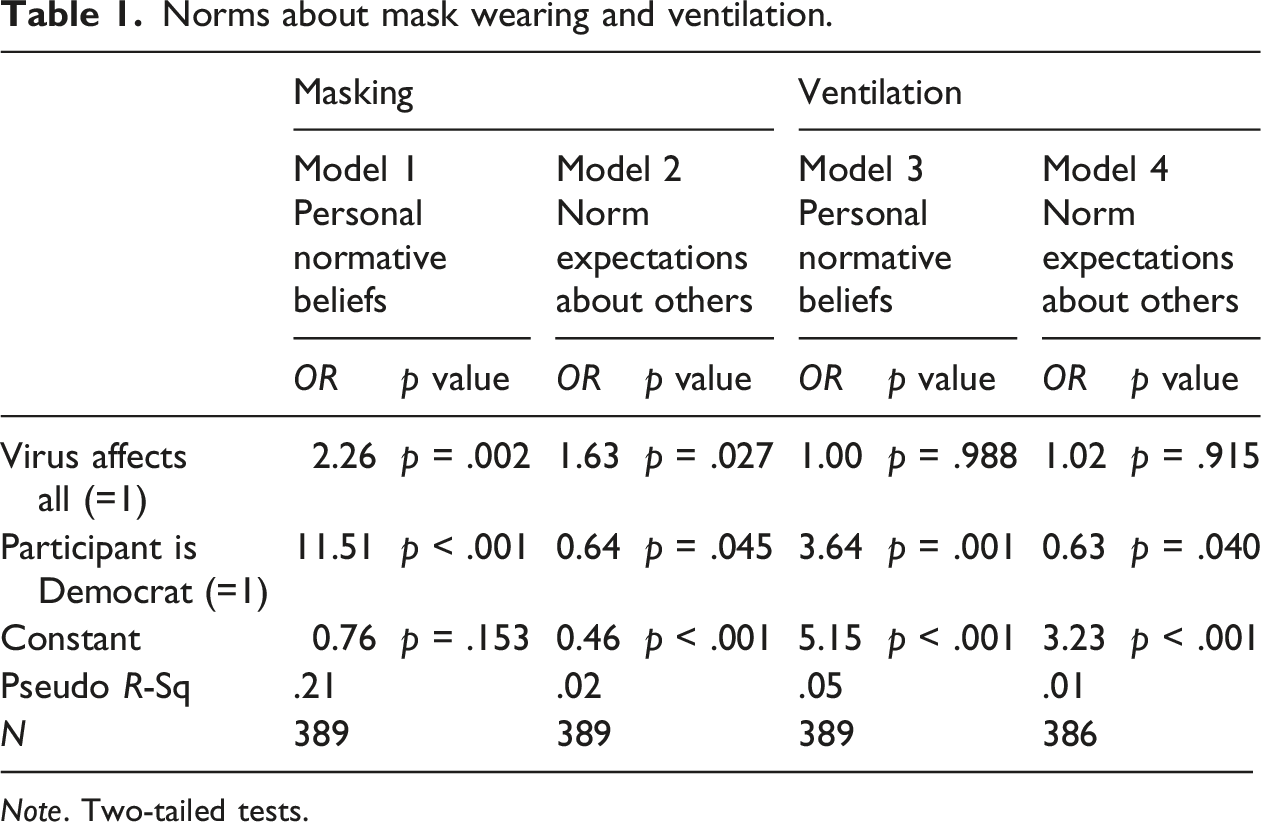
Note. Two-tailed tests.
As predicted by Hypothesis 1, individuals’ personal normative beliefs (Model 1, Table 1), and their normative expectations about what most others support (Model 2, Table 1), were more supportive of masking when everyone was affected by the virus than when only immune-compromised individuals were affected. Democrats were more favorable toward masking than Republicans (Model 1, Table 1) but expected others to be less supportive than did Republicans (Model 2, Table 1).
Figures 3 and 4 report the distribution of participant personal normative beliefs and normative expectations about ventilation by experimental condition. Again, normative beliefs and expectations were somewhat correlated (r = .48). Participants were highly supportive of ventilation, especially in their personal normative beliefs, but also in what they expected others to support. In both, participants’ own support and their expectations about others’ support registered almost exclusively in the top half of the scale (5-10). Distribution of normativel beliefs supporting ventilation by experimental condition (Study 1). Distribution of normative expectations about support for ventilation by experimental condition (Study 1).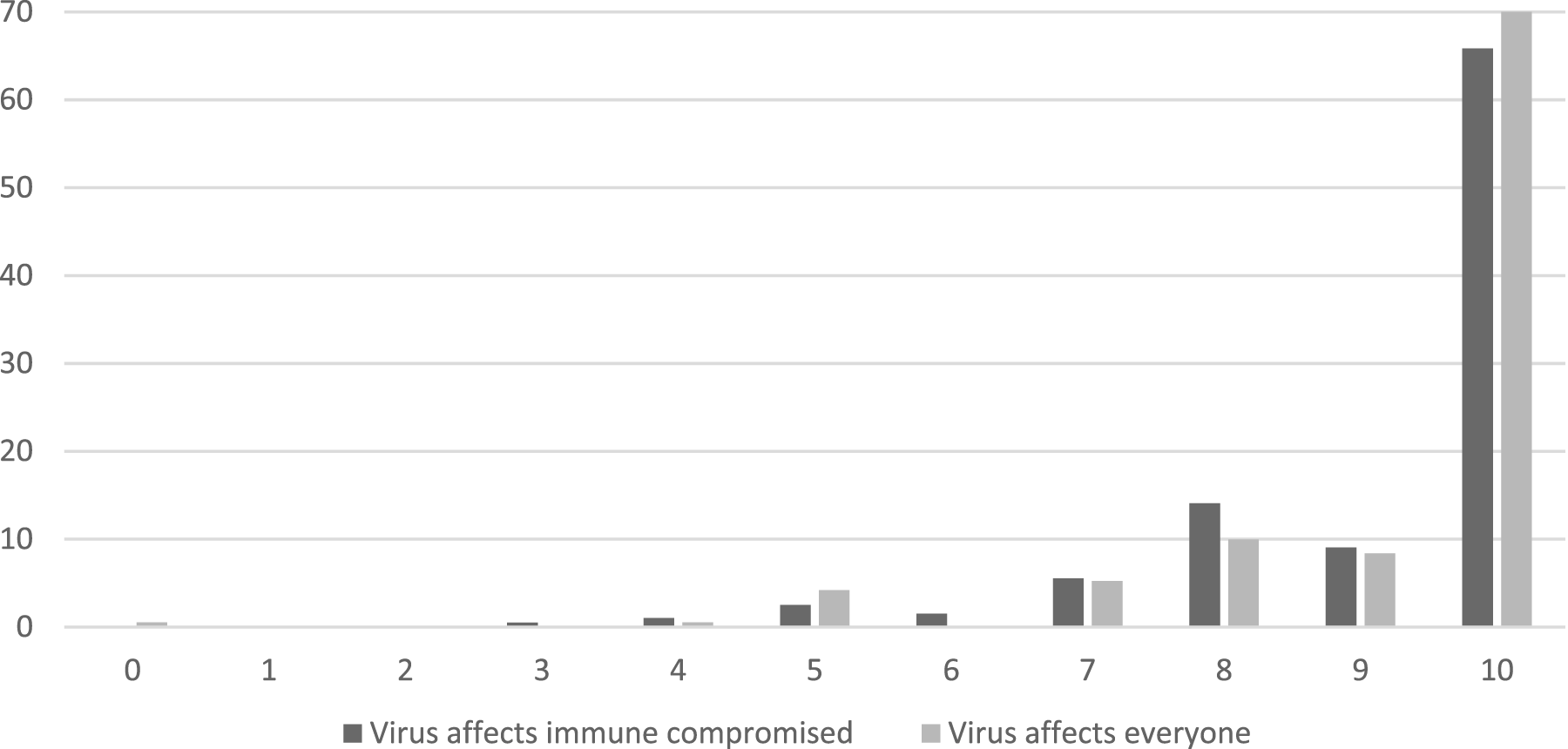
Again, we dichotomized responses into low (0-7) and high (8-10) support and estimated logistic regression models to test the hypotheses. 4 In contrast to the findings regarding masking, the experimental manipulation had no effect on personal normative beliefs or normative expectations about others (Models 3 and 4, Table 1). It is possible that because organizations rather than individuals directly experienced the costs of compliance, individual normative beliefs and expectations did not take those costs into account. It may be that if an outside actor is able to reduce externalities, individuals want them to do so. That is, it may be that any externality at all, regardless of its distribution, may be enough to trigger support for good ventilation. The higher support in Figure 3 for ventilation compared to masking in Figure 1 is consistent with this possibility. Again, we find that Democrats were personally more supportive of ventilation than were Republicans (Model 3, Table 1). They also had lower expectations about others’ support than Republicans (Model 4, Table 1).
As we noted at the outset, it is important to examine the robustness of our findings in ways that take into consideration the recent, highly political, pandemic experience in the U.S. In addition to recruiting participants favoring the two major U.S. political parties, we supplemented our measures of normative expectations, which ask about how much most others would approve of a behavior, with similar measures asking separately about most Republicans and most Democrats. We report those results in the Appendix Table A and summarize them briefly here. They generally show that Democrats expected most Republicans to be less supportive of masking and ventilation, but did not expect Republicans to respond to the experimental conditions. (However, this lack of effect for Republicans was seen only when treating high as 8-10; the experimental conditions had a statistically significant effect when using an alternative cut point). Participants expected Democrats to support masking more when the virus affected all adults than when it affected only immune-compromised individuals. These patterns add to the portrait of political differences documented in Table 1, that Democrats are personally more supportive of masking and ventilation, but are less likely to expect others to be. As noted above, political affiliation did not interact with the virus condition to shape normative beliefs or expectations.
Discussion
The results for masking are consistent with the hypotheses and suggest that norms supporting health behaviors are stronger when everyone is at risk than when only a minority is at risk. The results for ventilation do not support the hypotheses. This may be because individuals do not directly bear the costs of engaging in that health behavior (organizations do). In both cases the experimental effects are consistent across participants from the two major U.S. political parties.
The theoretical argument assumes that the distribution of the externality drives interest in regulation of the related behavior. But in the data above, it is also possible that the number of people affected by the externality (the spread of the harm), rather than the distribution of the externality (the harm to the actor and group members generally versus a small subgroup), had an effect. In other words, participants may have held stronger normative expectations of masking when the virus affected everyone than if it affected the immune-compromised either because most participants were not personally vulnerable in the latter case or because regardless of whether they were, the number of people affected was considerably larger. So, it is not clear from Study 1 whether the distribution of externalities or the number of people affected drove more supportive norms.
Study 2
To examine this question, we conducted a second study focusing only on masking that relied on age to distinguish who was affected by the virus and who was not. Study 2 had a 3 x 2 between-subjects design crossing externalities by political orientation of the study participant (Republican vs Democrat). The three externalities conditions were: adults in their 50s and older (50+) were affected by the virus, adults in their 40s and under (40-) were affected by the virus, and all adults were affected by the virus. This age grouping (50+ vs. 40-) roughly cuts the adult population in half. All participants were 50 or over. In addition to examining personal normative beliefs, we also distinguish between normative expectations about those affected by the virus and those not affected. In other words, participants ages 50+ expressed their normative beliefs, their expectations about adults 50 and over, and their expectations about adults 40-. As in Study 1, we blocked on participant political orientation.
We expect that if the externalities argument is correct, then participants’ normative beliefs will be more supportive of masking when it benefits the subgroup they are in, and will be less supportive when masking only benefits a subgroup they are not in (with those two subgroups similarly sized). Normative expectations will follow the same pattern. Thus, people (who are 50+) will have stronger beliefs supporting masking, and expect others 50+ to be more supportive of masking, when the virus affects adults 50+ than when it affects adults 40-. They will expect adults 40- to be less supportive when the virus affects adults 50+ than 40-.
What if the virus either affects the subgroup the participant is in, or affects everyone? If people care primarily about their personal consequences, they will be equally supportive of masking if the virus affects only people 50+ and if it affects all adults – because they personally will benefit either way. But if participants care about the number of people affected (the spread of the harm), then they will be more supportive of masking if the virus affects all adults. To the extent that people see others as self-interested, they will expect those 50+ to be equally supportive if the virus affects all adults or if it affects only 50+, and they will expect those 40- to be more supportive when the virus affects everyone (including 40-) than if it affects only those 50+.
Accordingly, we hypothesize:
Personal normative beliefs and normative expectations about people 50+ will be more supportive of masking if the virus affects people 50+ than if it affects people 40-. Normative expectations about those 40- will be less supportive.
Harm to Individual: Personal normative beliefs and normative expectations about people 50+ will be equally supportive of masking if the virus affects all adults and if it affects 50+. Normative expectations about people 40- will be more supportive of masking if the virus affects all adults than if it affects only people 50+.
Spread of Harm: Personal normative beliefs will be more supportive of masking if the virus affects all adults than if it only affects people 50+.
Participants and procedures
Participants and procedures were the same as for Study 1 except that we recruited only participants who were age 50 and older. Power analyses again suggested a sample size per cell of 88 per cell to detect moderately small effect sizes (Cohen’s d = .30, or f = .15, and assuming p = .05 and power = .80). We slightly oversampled. Our final sample included 594 participants. 5 We included a manipulation check. In the 50+ condition, nine percent failed the manipulation check. In the 40- condition eight percent failed. And in the all adults condition, 15 percent failed. We report the results for the full sample (Aronow et al., 2019; Mize and Manago, 2002). Results are the same whether those who failed the manipulation check are included or not.
Mean participant age was 59.08 (SD = 7.11). Their mean years of education were 15.92 (SD = 2.20), or about four years of college. Fifty-nine percent of participants were female and 79% were white. Fifty percent identified most with the Democratic party and 50% with the Republican party.
Vignette manipulations
The manipulated phrases are italicized below: Assume there is a novel virus that has spread around the world. The virus is airborne, meaning that it is transmitted primarily through the air. The virus has little effect on adults in their [40s and younger/50s and older]. But it is very dangerous for adults in their [50s and older/40s and younger]. Adults in their [50s and older/40s and younger] are likely to be hospitalized. Their risk of dying is high. If they survive they are likely to have serious long-term problems. Because the virus is airborne, mask-wearing can significantly reduce its transmission. If you wear a mask you reduce your own risk. You also reduce the risk to others. Assume there is a novel virus that has spread around the world. The virus is airborne, meaning that it is transmitted primarily through the air. [The virus is] very dangerous [for all adults]. [Adults of all ages] are likely to be hospitalized. Their risk of dying is high. If they survive they are likely to have serious long-term problems. Because the virus is airborne, mask wearing can significantly reduce its transmission. If you wear a mask you reduce your own risk. You also reduce the risk to others.
Measures
As in Study 1, to assess personal normative beliefs, we asked participants about whether they thought everyone should wear masks (0 = definitely should not; 10 = definitely should). To measure normative expectations, we asked about participants’ expectations that most others 50+ and most others 40- would think everyone should wear masks (0 = definitely should not; 10 = definitely should). Again, we also asked about participants’ expectations about most Republicans and most Democrats (results for expectations about Republicans and Democrats are in the Appendix).
It is possible that 50+ individuals who have younger family members might react more negatively to the 40-condition than one might expect based on their own age alone. In order to account for the possibility that people might be closely tied to vulnerable individuals, we asked participants if any members of their household were adults 40-. We included measures of the sociodemographic characteristics identified above. We also included the manipulation check mentioned above.
Results
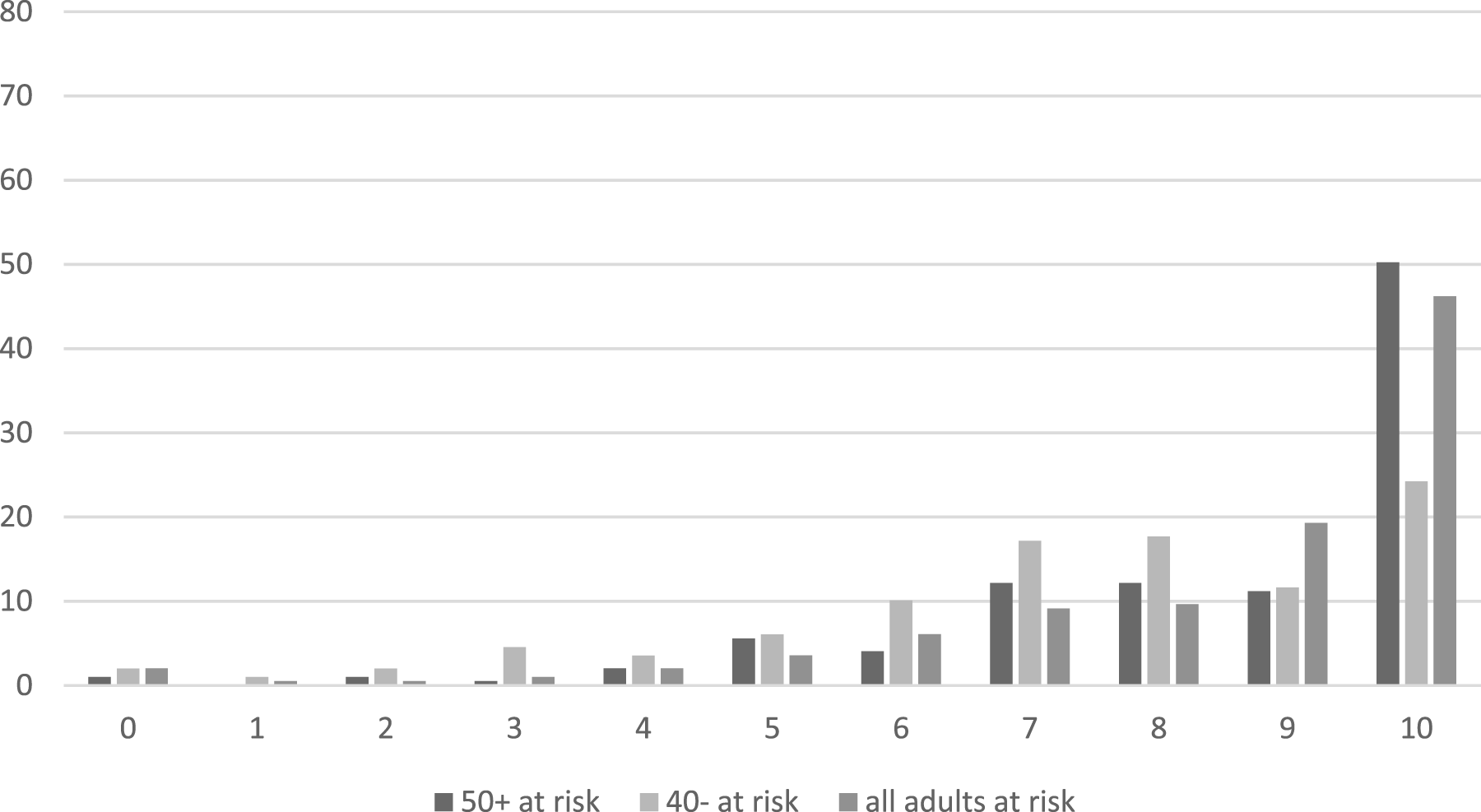
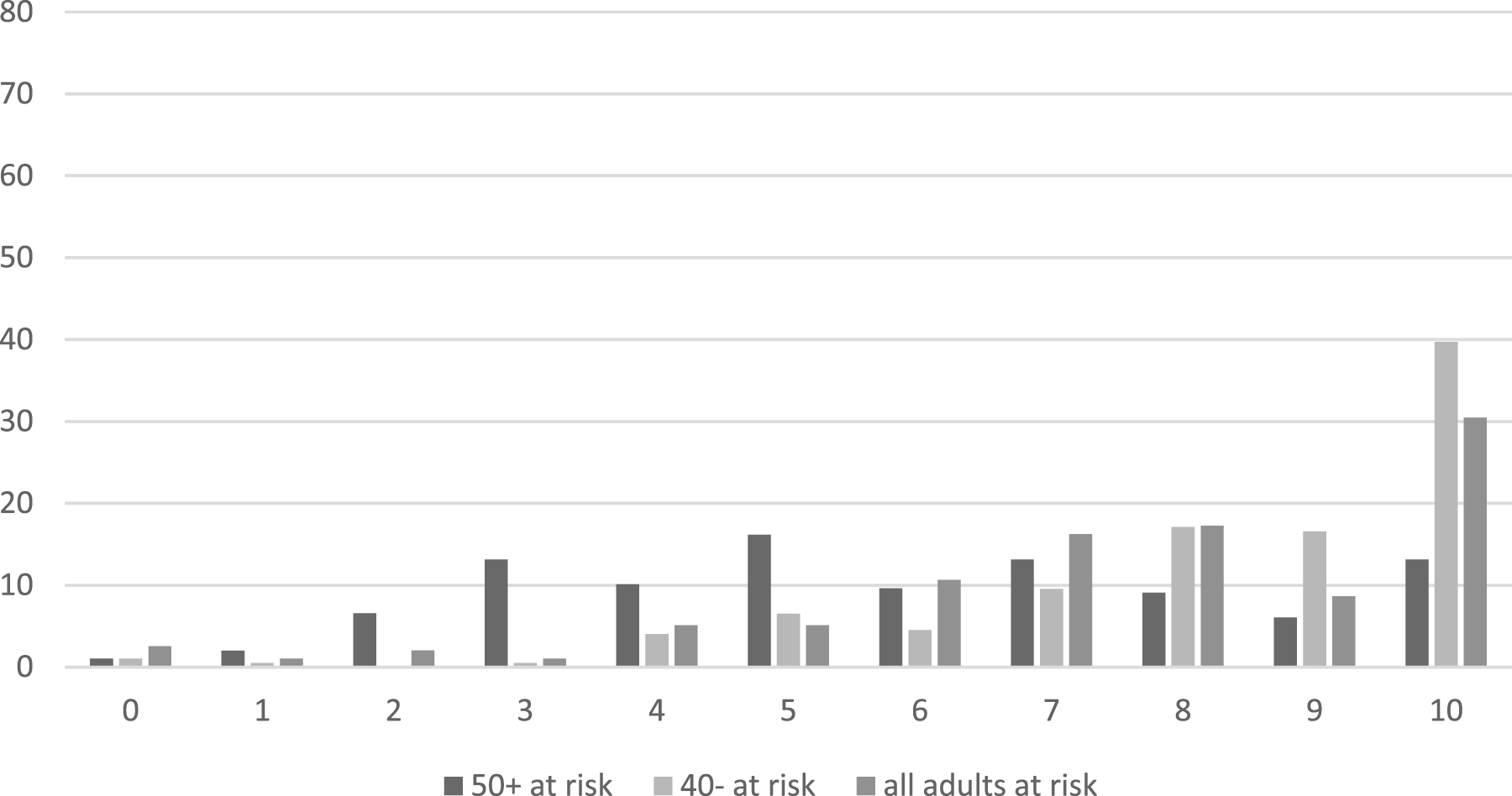
Figures 5–7 report the distribution of participants’ responses across the experimental conditions. Personal beliefs were correlated with normative expectations about other adults 50+ (r = .62) and with normative expectations about adults 40- (r = .46). The two normative expectations measures were also correlated, but less strongly (r = .39). DIstribution of normative beliefs supporting masking by experimental condition (Study 2). Distribution of normative expectations about those 50+ that support masking by experimental condition (Study 2). Distribution of normative expectations about those 40- that support masking by experimental condition (Study 2).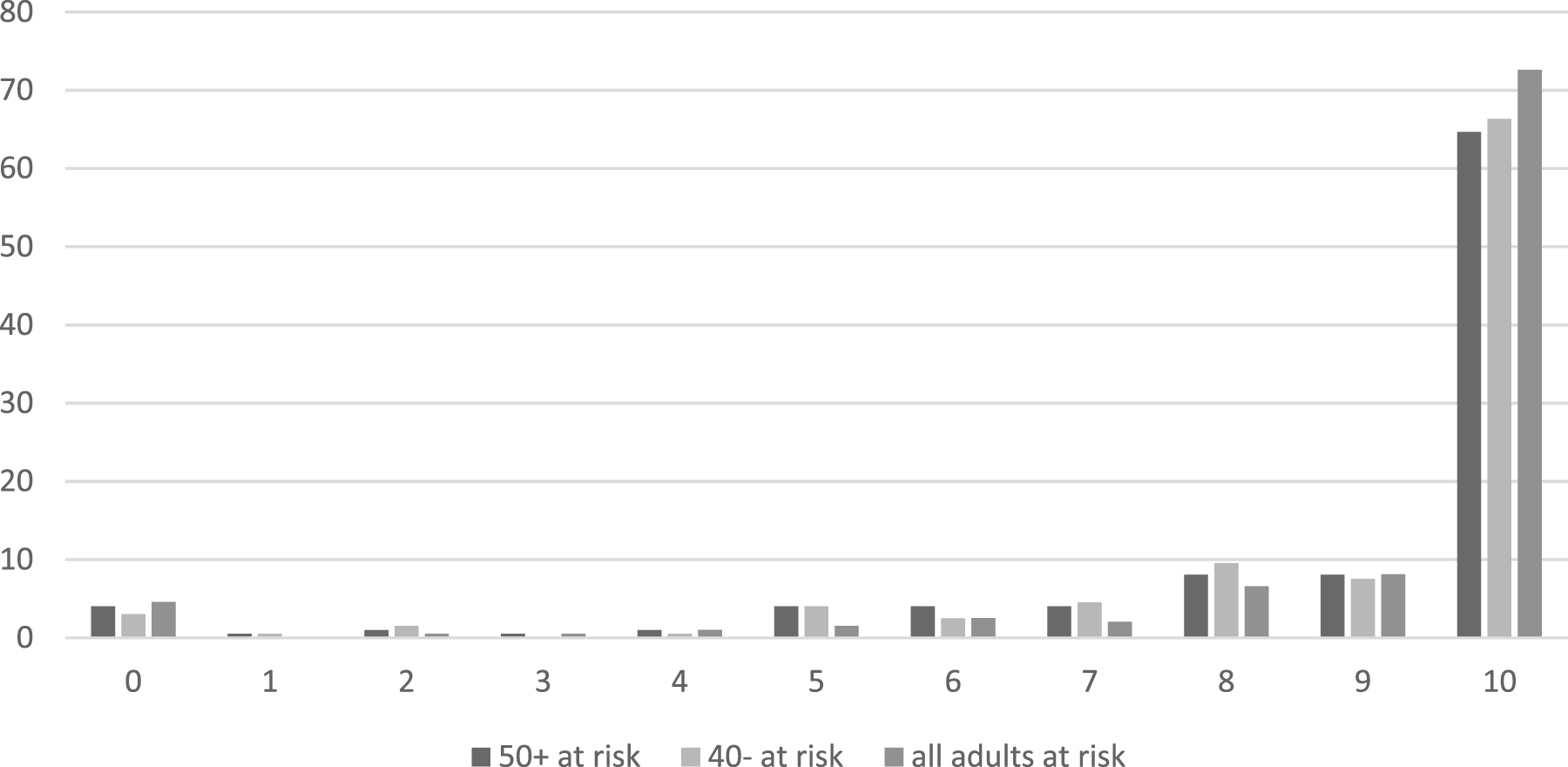
Participants were personally very supportive of masking, regardless of who was affected by the virus (Figure 5). Less than 10% of ratings were in the bottom half of the scale (i.e., 0, definitely should not, to 4). Across conditions, 65-73% strongly supported masking (i.e., responding with a rating of 10). There is little variation in participants’ personal normative beliefs across the experimental conditions (Figure 5). Over two-thirds of the sample in each condition strongly supported masking.
The distribution of ratings for normative expectations (Figures 6 and 7) was more spread out, with larger percentages of respondents using middle values on the rating scale. Still, expectations leaned supportive, with a majority of respondents expressing normative expectations in Figures 6 and 7 in the top half of the ratings scale. In contrast to normative beliefs, the experimental manipulation does seem to matter for expectations, both for other 50+ year olds (Figure 6) and for those 40- (Figure 7).
OLS regressions showing the effects of comparing a condition in which people 50+ are affected by the virus and one in which people 40- are affected by the virus.
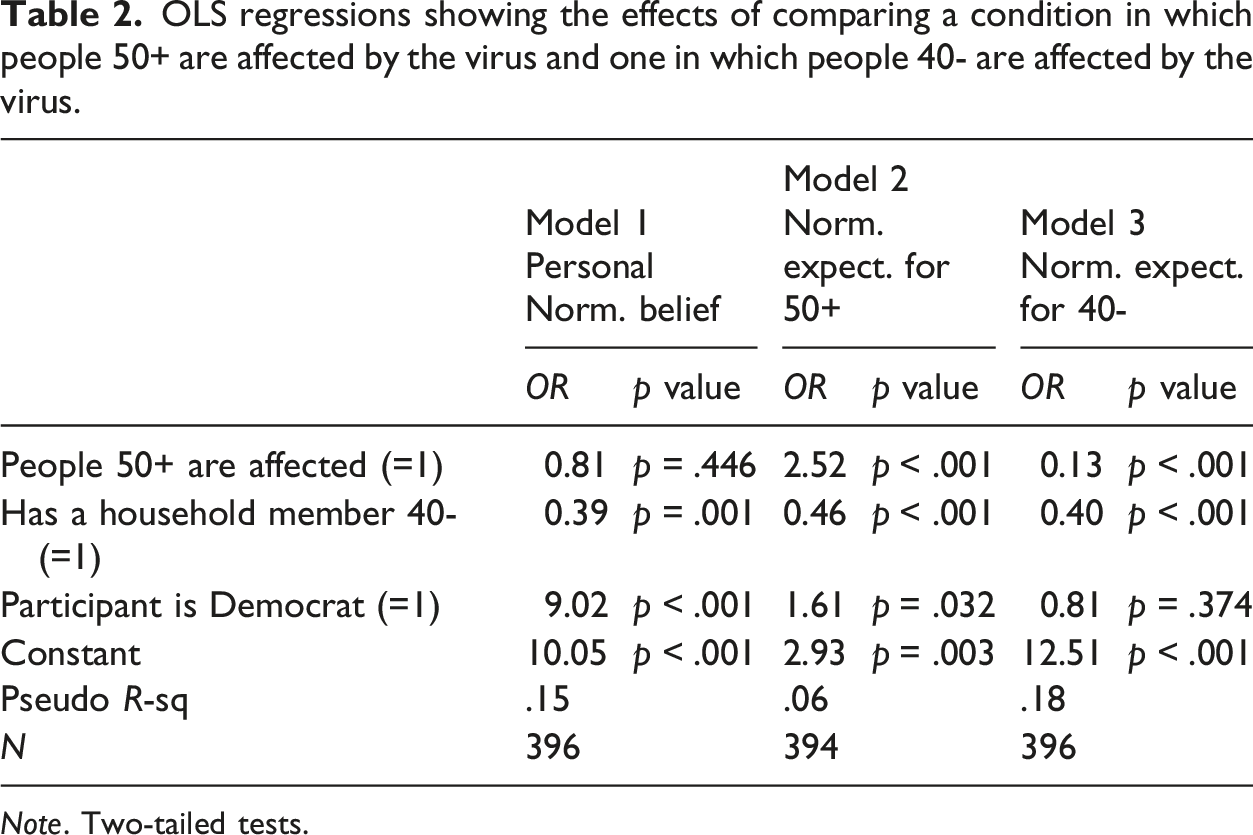
Note. Two-tailed tests.
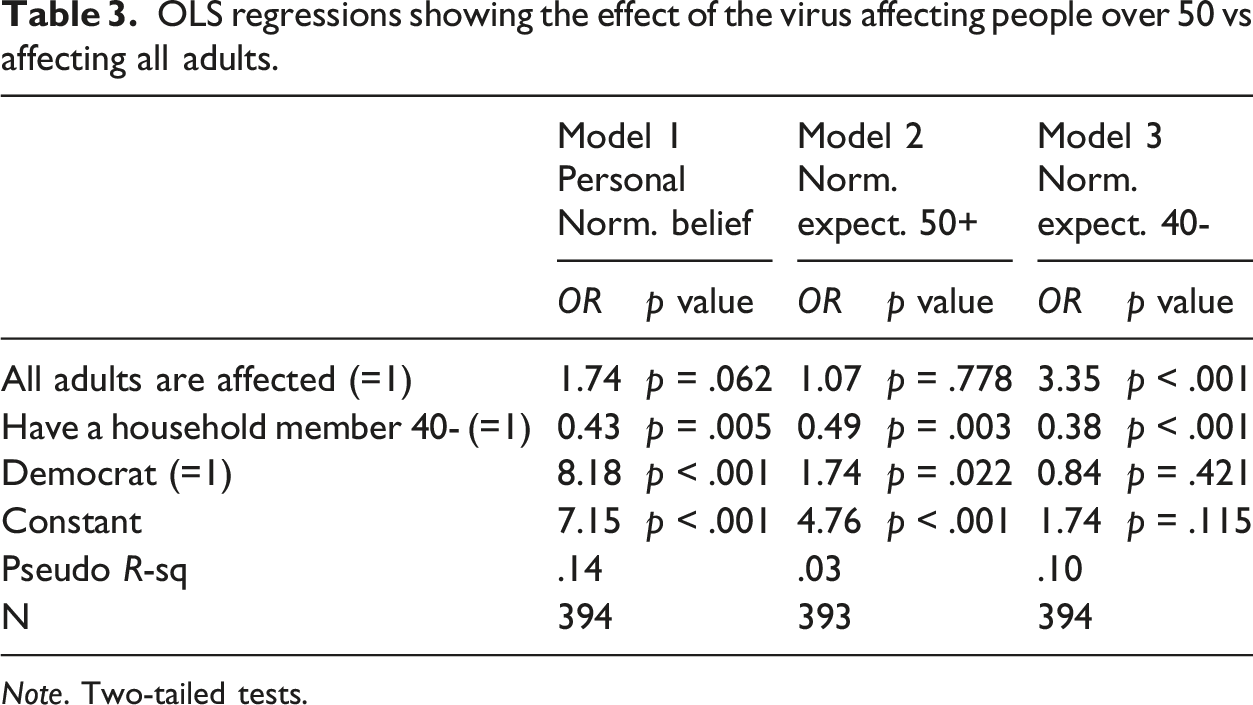
OLS regressions showing the effect of the virus affecting people over 50 vs affecting all adults.
Note. Two-tailed tests.
Table 2 reports the results of logistic regressions examining the effect of the experimental manipulation of the virus affecting 50+ or 40- adults on responses. 6 We also include participant political orientation and whether a household member was 40- as predictors. Hypothesis 3 predicts that people in this sample of 50+ year olds will have higher levels of support for masking, expect others over 50 to have higher levels of support for masking, and expect those 40- to have lower levels of support for masking, when the virus affects people 50+ than when it affects people 40-. The results for participants’ personal normative beliefs do not support the hypothesis. Instead, we see that the effect of the experimental condition is statistically insignificant (see Model 1, Table 2). The results for expectations about reactions of people 50+ and 40- do support the hypothesis, however. In both cases the coefficient representing the experimental condition is statistically significant and in the predicted direction (see Models 2 and 3, Table 2). Thus, the results regarding personal normative beliefs are inconsistent with our externalities argument, but the results for normative expectations about others are consistent.
With regard to the covariates, we find that those who have a household member 40- are less personally supportive of masking and expect others (both others 50+ and others 40-) to be less supportive as well. Democratic participants were also personally more supportive of masking than Republicans and expected others 50+ to be so as well, but there is no statistically significant effect of participant political orientation on expectations about others 40-. Again, we examined participants’ expectations about Republican and Democratic others in the different age groups (Appendix Table B). Results were largely consistent with those for expectations regarding other adults.
Hypothesis 4 makes predictions about support for masking when those over 50 are affected by the virus versus when all adults are affected. In both cases, participants were in the group affected by the virus; the numbers of people more generally affected differed, however. In one condition, the participant and their subgroup were affected; in the other, the participant and both subgroups were affected. Hypothesis 4a predicts that people will react similarly to both conditions – because in both conditions they would benefit from masking. Hypothesis 4b predicts an alternative – that people may be more supportive of masking when all are affected than when just 50+ are affected.
Table 3 reports the results of logistic regression models examining these hypotheses. The experimental effect compares the case of all adults affected to only those 50+. The effect of the experimental conditions on normative beliefs is significant only at the p < .10 level, and this result is not robust across sensitivity tests 7 (see Model 1, Table 3). 8 It is possible that there is an effect here that we are not clearly detecting. Participants expected others over 50 to be equally supportive, appearing to assume that others were reacting in self-interested ways.
As predicted by Hypothesis 4a, participants also expected those age 40- to be more supportive when the virus affected everyone than when it affected only those 50+. This result is consistent with the idea that people will expect others’ support for masking to be self-interested.
Similar to the models comparing the other two virus conditions, those that compare the virus affecting all adults with those 50+ document that participants with household members 40- are less supportive of masking and expect others, both older and younger adults, to be so as well. Also similar to the earlier results, participants who were Democrats were more supportive of masking and expected others 50+ to be more supportive as well (Models 1-2 in Table 3). Participant party affiliation did not shape expectations about adults 40- however (Model 3, Table 3). 9 Results for expectations regarding Republican and Democratic others across these age groups (vs. more generally adults in these age groups) were largely consistent (Appendix Table C).
Discussion
The results of Study 2 partially support the externalities argument. In comparing reactions when the virus affects people 50+ versus 40-, personal normative beliefs are inconsistent with our externalities argument. Participants are equally supportive of masking whether the virus affects their age group or the other age group. Expectations about others generally support the externalities argument, however. People expect others’ support to vary across the experimental conditions in ways that map onto exposure to externalities. When comparing people 50+ to all adults, the results for normative beliefs are less clear, but again, the results for normative expectations are consistent with the externalities argument. People in a group affected by the virus support masking regardless of the size of the group, and expect others to think the same.
Conclusion
We conducted two studies to test the effects of the distribution of externalities on normative beliefs and expectations. The results of Study 1 on masking are consistent with the externalities argument in that support for masking and expectations of others’ support are higher when the virus affects everyone (including the participant) than when it affects a subpopulation (not including the participant). Yet it is not clear whether this result is due to the effect of the externality on the individual (as the theory would predict) or due to the numbers of people potentially affected. The results for ventilation also suggest that when organizations bear the costs of a health behavior, the distribution of externalities does not affect support for those behaviors. Normative beliefs and expectations about ventilation are supportive regardless of who is at risk from the virus.
To further examine the effects of externalities in the context of masking we conducted a second study, designed to distinguish between the distribution of externalities and the numbers of people affected. The results of Study 2 partially support the externalities argument made here. When comparing situations where the virus affects people 50+ or 40-, externalities affect normative expectations. This finding suggests that participants think that others are self-interested actors. However, their own opinions diverge. Individuals are equally supportive of masking when the virus affects their own subgroup and when it affects a different subgroup. This finding might mean that individuals incorporate others’ well-being into their own preferences. Or it might mean that individuals are not behaving instrumentally – for example, instead considering the deservingness of people who impose harm on others. Future research on normative beliefs is needed to address these possibilities.
When comparing situations where the virus affects people 50+ to one in which the virus affects all adults, the results for expectations are again consistent with the externalities argument. Participants expected that others 50+ would support masking when their subgroup was affected and when both subgroups were affected – suggesting that they expected others to focus on the consequences of masking for their own well-being. The results for normative beliefs are less conclusive, however, showing a significant effect, but only at the p < .10 level. It is possible that in the 50+ condition, participants may have thought a group that included everyone 50 and over was large enough to support mask wearing. If so, then increasing the size of the group that was already seen as large, may have led to minimal, if any, increase in support for masking. One way to check the possible impact of the size of the actor’s group, would be to reduce the size of the group to which the individual belongs. As a practical matter, in the virus context it is difficult to identify characteristics that would produce a smaller group, while also retaining the ability to recruit a sufficient number of participants. For example, if we said that only immune-compromised individuals are affected by the virus, it would be difficult to recruit a sample of immune-compromised individuals to participate in the study.
The results of the two studies together show strong support for the externalities argument in the context of normative expectations. The evidence for personal normative beliefs shows that externalities matter, and also suggests that, at least under some conditions, people’s normative beliefs may reflect how externalities affect others at least as much as they reflect their own experience with externalities. Future research should further explore the mechanisms responsible for these patterns.
Further, the results from Study 1 suggest that the distribution/spread of an externality may not affect normative beliefs and expectations if an organization rather than individuals bear the costs of addressing externalities. Future research should examine whether this pattern is unique to organizations or whether the effect would be the same for any third party who takes on the costs of reducing harmful externalities. The findings here also suggest that people may consider the burden of reducing externalities – and may be more supportive of an externality-reducing behavior if the costs to them of the behavior are low (see, e.g., Horne, 2001; Horne et al., 2018).
In addition, as noted above, the results from Study 2 show that people’s normative expectations seem to assume that others care about externalities to the extent that they themselves are affected, whereas people’s normative beliefs (demand for norms) tend to support health behaviors regardless of who is affected. These findings suggest some level of pluralistic ignorance — people support health behaviors more than they expect that others do (Miller, 2023). Situations where sub-groups are affected differently by a behavior may foster pluralistic ignorance because there is more conflict between altruistic motivations (which would support health behaviors regardless of who is affected) and instrumental motivations (which would support health behaviors that benefit the individual more than those that benefit others). Pluralistic ignorance may lead people to engage in health behaviors more (because they think if others do not then their own actions are more important), or to engage in health behaviors less (because they do not think they will receive positive responses from others). Future research should explore the effects of pluralistic ignorance on norm-related behaviors.
The findings have policy implications. The results of Study 1 suggest that norms supporting health behaviors are stronger when everyone is seen as at risk than when only a subgroup is seen as at risk, and that the numbers of people potentially affected may matter. The implication is that when health experts talk about subgroups being vulnerable, they are weakening health behavior norms. In the case of Covid, for example, the Centers for Disease Control and Prevention (CDC) consistently identifies categories of people who are more at risk from long Covid. But those categories include women, Hispanic/Latin individuals, people who had more severe Covid, people with underlying health conditions (such as being overweight), and people who are not vaccinated (CDC, 2025b). Given that there are more women than men in the U.S. and the large numbers of overweight individuals as well as large numbers of unvaccinated individuals, it seems that the majority of Americans are at higher risk of long Covid. But the communications suggesting that only vulnerable groups need to worry send the message that only a few are vulnerable and most people do not need to be concerned – the kind of communication that this study shows weakens health behavior norms.
This study was conducted after people had experienced the Covid-19 pandemic during which masking became highly politicized. We find that Democrats are generally more supportive of masking and efforts to improve ventilation than Republicans. This is not surprising given the politicization of health behaviors during Covid (e.g., Calvillo et al., 2020; Hart et al., 2020; Stroebe et al., 2021). But this does not necessarily mean that we would expect the effects of the experimental conditions to differ for Republicans and Democrats. For example, if we assume that Republican normative beliefs oppose masking while Democratic normative beliefs support it, and that both groups are committed to their existing beliefs, then we would expect to see no effect of the experimental conditions for either group. That is, the political nature of masking may have blunted the effects of externalities. Nonetheless, we found effects. To the extent that participants brought normative beliefs about masking into the experimental setting, our results likely understate the effects of the distribution of externalities – our study provides a conservative test of the theoretical argument. In addition, if Republican and Democratic participants differed in their attachments to prior normative beliefs or had different beliefs about the risks posed by viruses and the effectiveness of masking (therefore differing in their perceptions of externalities associated with masking), then we might expect them to react differently to the experimental manipulations. But although the personal beliefs of Republicans and Democrats anchored differently on the scale, we did not find that externalities affected them differently. We also found that, compared to Republicans, Democrats had lower expectations about others, particularly about Republicans (see Appendix) suggesting that Democrats may be more “judgy” than Republicans (see Horne and Johnson, 2021 for evidence that Democrats had lower expectations of Republicans than Republicans themselves did). However, we note that because our study does not use a representative sample, it is possible that Republicans and Democrats generally might not behave like people in our study. Future research could test the theory with representative samples and could examine the effects of externalities on norms in more and less politicized contexts. Future research could also investigate the possibility that existing beliefs tied to political affiliation are carried over into new settings and shape norm emergence and compliance. If so, then public health messaging about new diseases and behaviors may be less effective than hoped.
Existing opinions not tied to political party might have affected behavior in the experiment. But random assignment of participants distributed such opinions across the experimental conditions. Observed experimental effects are thus independent — though they could be smaller or larger under other historical conditions. It is also possible that other pre-existing opinions interacted with the experimental conditions in ways we are not able to assess here.
This study is limited in ways that could be addressed in future research. It looks at normative beliefs and expectations, not at behavior. We cannot tell from the data here what the implications are for norm compliance. Moreover, in this study, the externalities are known to the participants. This serves a strategic goal of isolating the key features under study. But many situations of interest may involve additional factors such as varying knowledge of externalities and even the possibility of misinformation about externalities. In the recent Covid-19 context, people over- and under-estimated the consequences and risks of contracting the disease. Misinformation circulated. Public health experts note the role such misinformation will likely play in complicating efforts to combat the next pandemic (Internal Medicine, 2025). The effects of externalities probably depend on people having shared understanding of what those externalities are. In addition, investigation into who pays the cost of engaging in health behaviors may be useful. Our participants in Study 1 may have assumed that organizations would bear the cost of improvements to ventilation, without considering whether those costs would be passed on to individuals.
Finally, the study relies on samples from Prolific. Such samples are more diverse than student body samples but are not representative of the U.S. population. Therefore, we cannot generalize from our results regarding overall support for health behaviors, nor those regarding Republicans and Democrats. The study also focuses on the U.S. It is possible that there might be variation across countries, given different experiences with COVID-19. In addition, effects might differ given other societal characteristics. Eriksson and colleagues find, for example, that the strength of norms focusing on harm to others varies depending on how collectivist or individualist a society is. This work suggests that we might expect the effects of externalities to differ across societies (Eriksson 2024; see also Eriksson et al., 2026).
Researchers argue that norms emerge in response to externalities. Theoretically, the findings here support the view that externalities matter, but also suggest that sometimes externalities have an effect, at least in part, because individuals consider the impact of externalities on others. It also appears that when there are no compliance costs, the distribution of externalities does not matter – people want compliance no matter who is affected. Looking at situations in which the effects of behaviors on different groups of people vary may provide opportunities to disentangle mechanisms beyond what can be observed in situations where individuals all share the same interests. Substantively, the study has implications for public health communications. Communications that emphasize harms to vulnerable groups are likely to produce weaker norms than communications suggesting that risks are widespread.
Footnotes
Ethical considerations
The study was reviewed by the Washington State University IRB and determined to be exempt from review (Certificate of Exemption: IRB#20783-001) on November 25, 2024. Participants provided informed consent by reading a consent form online and clicking on a link indicating their consent.
Funding
We appreciate the research support of the Department of Sociology at Washington State University.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data and syntax are available at Johnson, Monica Kirkpatrick, 2026, “Replication Data for: Horne and Johnson's Externalities and Norms in the Context of a Novel Virus,” Harvard Dataverse, V1, https://doi.org/10.7910/DVN/227BLE UNF:6:XRc+TDRYgkEQFhEU4U0PUQ== [fileUNF] (Johnson, 2026).
Notes
Appendix
Effects of the Study 1 experimental conditions on expectations about Republicans and Democrats. Note. Two-tailed tests. Participants expected lower support from Republicans than Democrats, and as a result the dichotomization of high support captures a much smaller group for the former. Expectations about Republicans’ support for masking did not reach significance with this dichotomization (high = 8-10), with only 12% of cases expected to support, but does if high support is expanded to include 7-10.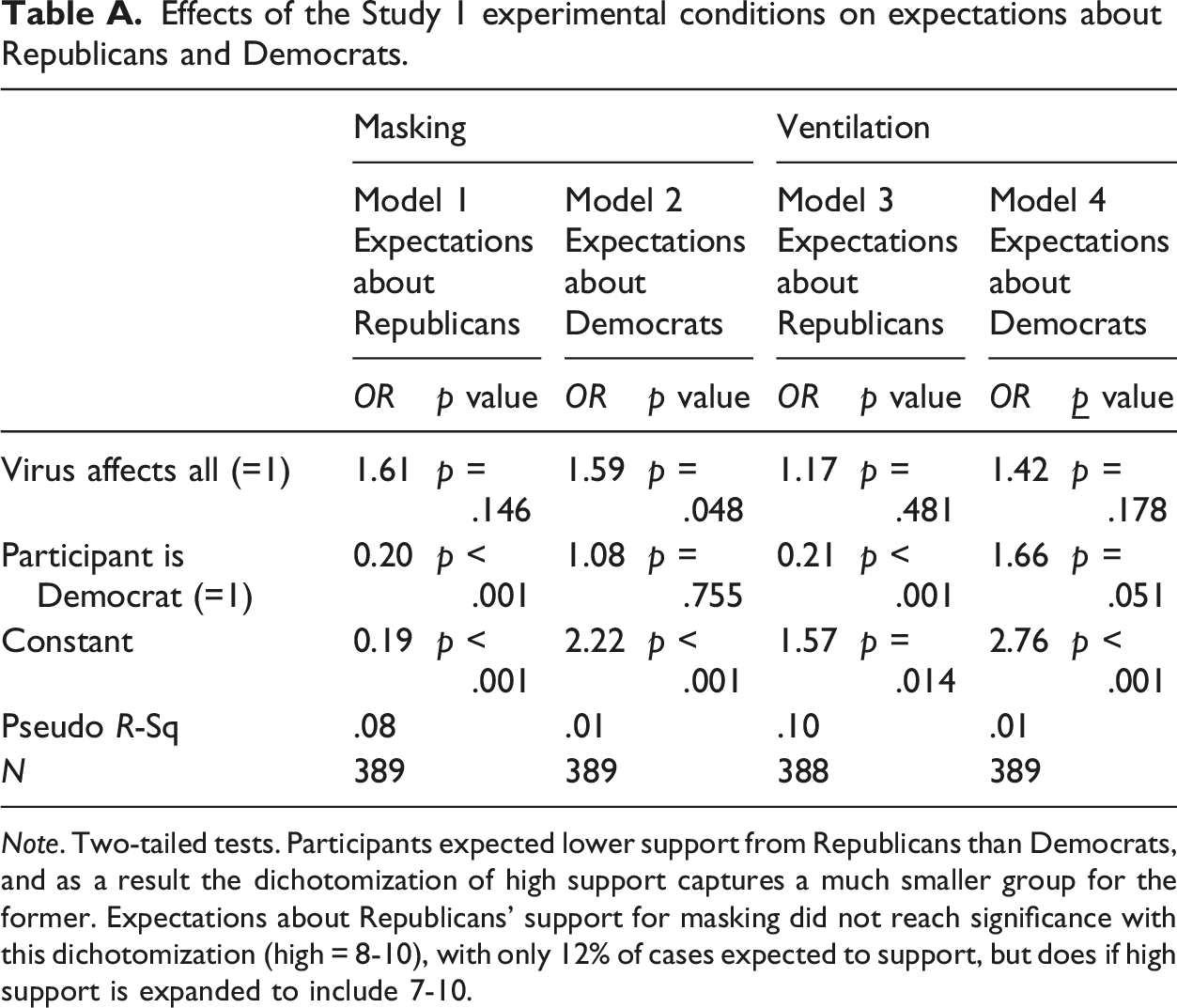
Masking
Ventilation
Model 1
Model 2
Model 3
Model 4
OR
p value
OR
p value
OR
p value
OR
Virus affects all (=1)
1.61
p = .146
1.59
p = .048
1.17
p = .481
1.42
p = .178
Participant is Democrat (=1)
0.20
p < .001
1.08
p = .755
0.21
p < .001
1.66
p = .051
Constant
0.19
p < .001
2.22
p < .001
1.57
p = .014
2.76
p < .001
Pseudo R-Sq
.08
.01
.10
.01
N
389
389
388
389
Effects of the Study 2 experimental conditions on expectations about Republicans and Democrats (comparing virus affects 50+ to virus affects 40-). Note. Two-tailed tests.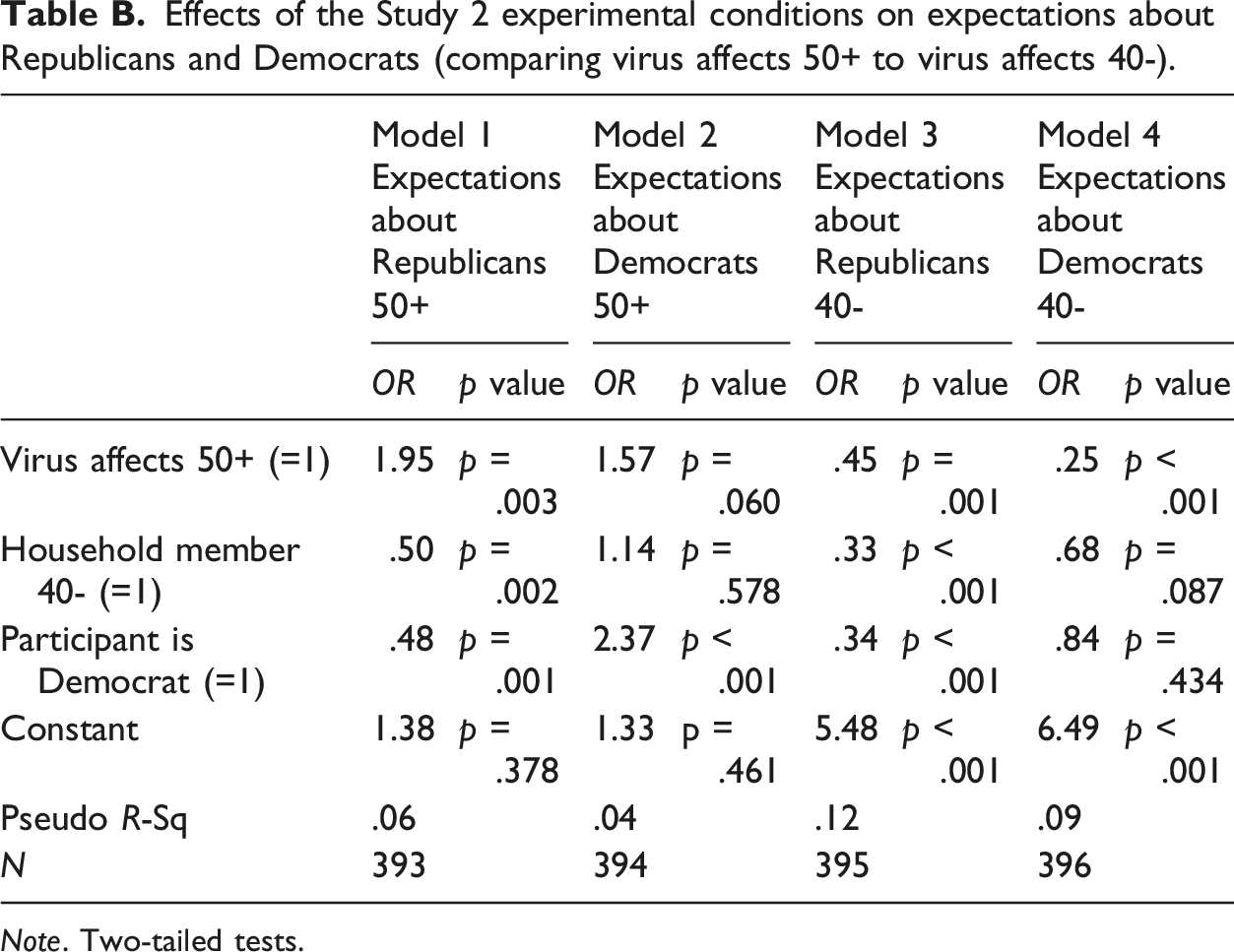
Model 1
Model 2
Model 3
Model 4
OR
p value
OR
p value
OR
p value
OR
p value
Virus affects 50+ (=1)
1.95
p = .003
1.57
p = .060
.45
p = .001
.25
p < .001
Household member 40- (=1)
.50
p = .002
1.14
p = .578
.33
p < .001
.68
p = .087
Participant is Democrat (=1)
.48
p = .001
2.37
p < .001
.34
p < .001
.84
p = .434
Constant
1.38
p = .378
1.33
p = .461
5.48
p < .001
6.49
p < .001
Pseudo R-Sq
.06
.04
.12
.09
N
393
394
395
396
Effects of the Study 2 experimental conditions on expectations about Republicans and Democrats (comparing virus affects 50+ to virus affects all). Note. Two-tailed tests.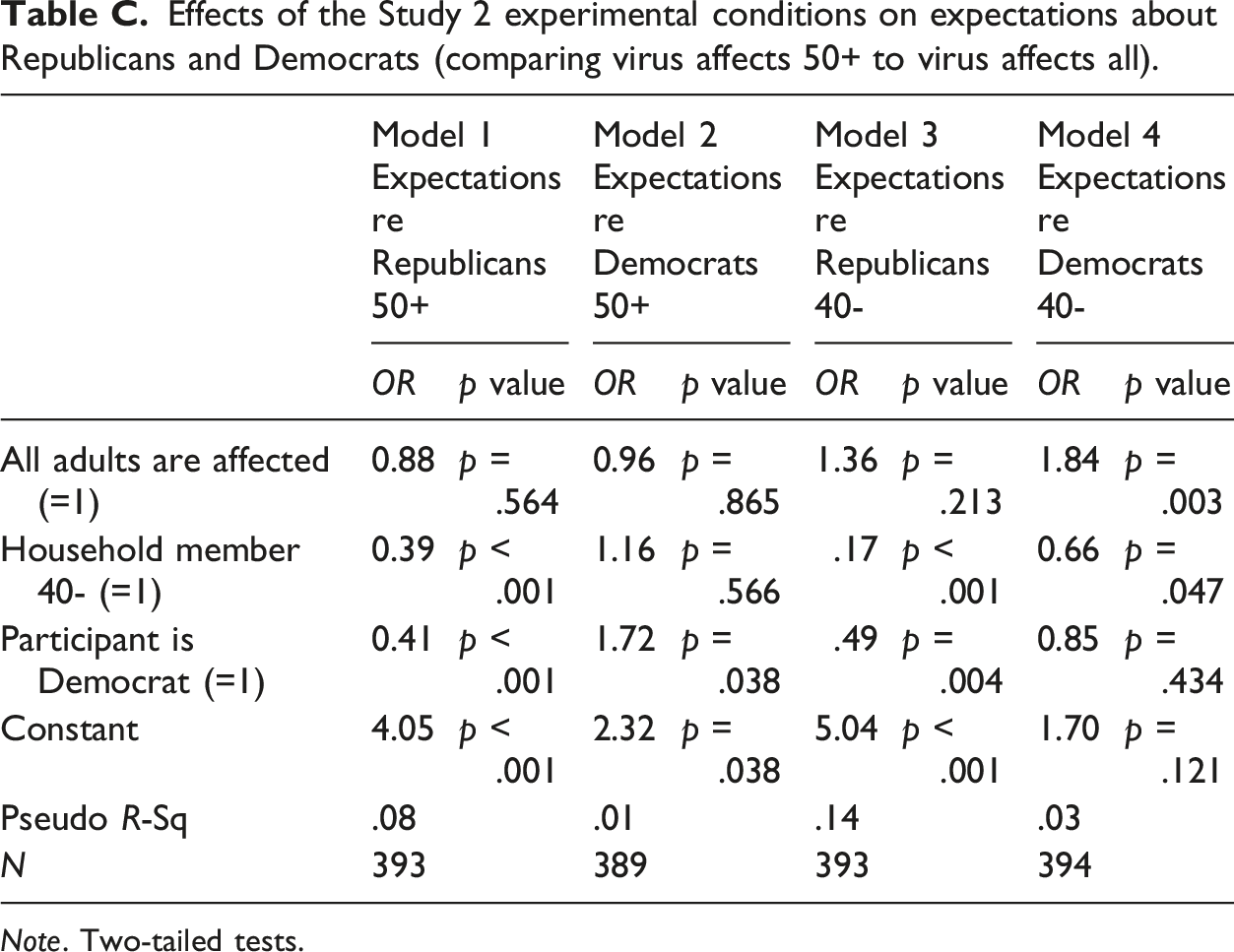
Model 1
Model 2
Model 3
Model 4
OR
p value
OR
p value
OR
p value
OR
p value
All adults are affected (=1)
0.88
p = .564
0.96
p = .865
1.36
p = .213
1.84
p = .003
Household member 40- (=1)
0.39
p < .001
1.16
p = .566
.17
p < .001
0.66
p = .047
Participant is Democrat (=1)
0.41
p < .001
1.72
p = .038
.49
p = .004
0.85
p = .434
Constant
4.05
p < .001
2.32
p = .038
5.04
p < .001
1.70
p = .121
Pseudo R-Sq
.08
.01
.14
.03
N
393
389
393
394
Effects of the experimental conditions comparing 50+ to all adults for Republicans only (comparing virus affects 50+ to virus affects all). Note. Two-tailed tests.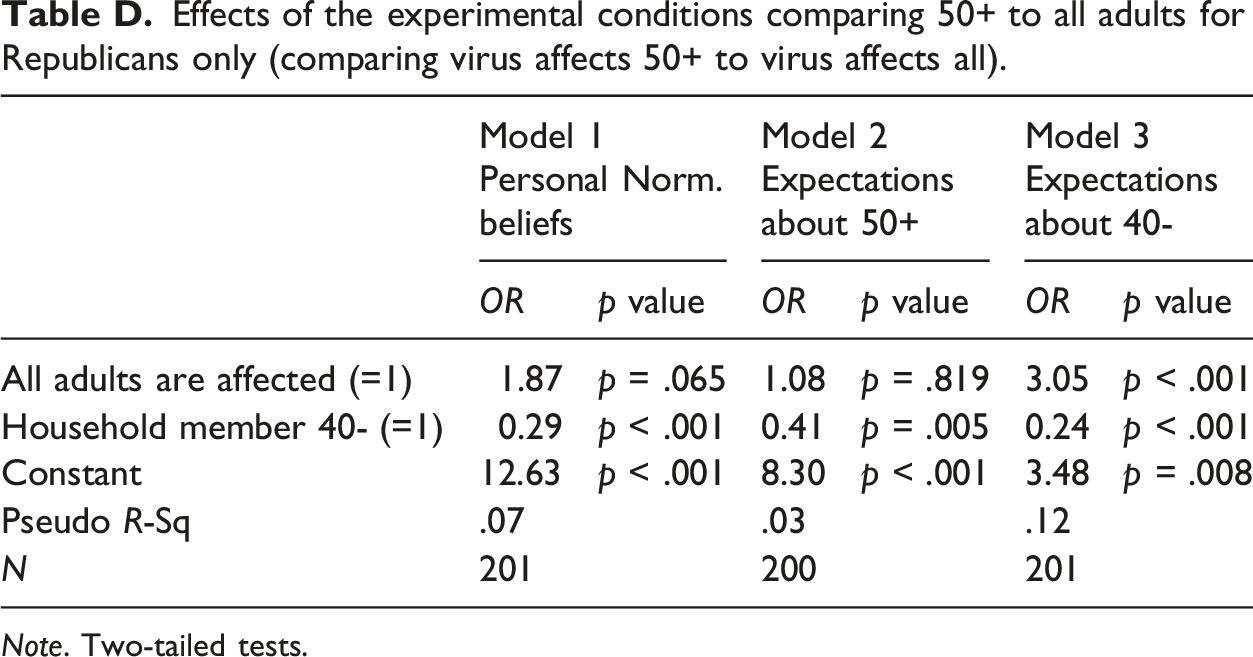
Model 1
Model 2
Model 3
OR
p value
OR
p value
OR
p value
All adults are affected (=1)
1.87
p = .065
1.08
p = .819
3.05
p < .001
Household member 40- (=1)
0.29
p < .001
0.41
p = .005
0.24
p < .001
Constant
12.63
p < .001
8.30
p < .001
3.48
p = .008
Pseudo R-Sq
.07
.03
.12
N
201
200
201