
Abstract
Keywords
According to the Office of Minority Health at the U.S. Department of Health and Human Services [U.S. DHHS] (n.d.), cancer is the second leading cause of death for most racial and ethnic minorities in the United States. In 2004, 62,499 African Americans, 24,522 Hispanics, 10,863 Asians and Pacific Islanders, and 2,392 American Indians died of cancer in the United States (U.S. DHHS, n.d.). In Asian Americans, cancer is the leading cause of death (Chen, 2005). Although recent U.S. statistics show that the cancer morbidity and mortality rates of Whites have decreased, those of Asian Americans have increased or stayed the same (Chen, 2005). Furthermore, compared with Whites, Asian Americans living with cancer are more likely to suffer from depression (Ell et al., 2005) and Asian Americans report a lower quality of life than Whites (Eversley et al., 2005; Penedo, Dahn, Shen, Schneiderman, & Antoni, 2006). Researchers have reported that the association of poor survival rates with fewer sources of social support was higher for ethnic minorities, including Asian Americans, than for Whites (American Cancer Society, 2008; Freeman, 2003; Morris, Billingsley, Baxter, & Baldwin, 2004).
Internet cancer support groups (ICSGs) have been reported as excellent sources of social support for people living with cancer (Fogel, Albert, Schnabel, Ditkoff, & Neugut, 2003). In this article, “social support” refers to an interpersonal transaction involving emotional concern, instrumental aid, information, or appraisal (i.e., self-evaluation; McLean, 1995). “People living with cancer” are those who have ever had a cancer diagnosis in their lifetime (Moadel et al., 1999). Indeed, studies have indicated that the use of ICSGs increases social support by increasing patients’ personal empowerment, self-esteem, and functional status, and by reducing social isolation, depression, cancer-related trauma, and symptom distress (Fogel, Albert, Schnabel, Ditkoff, & Neugut, 2002; Houston, Cooper, & Ford, 2002; Winzelberg, Classen, & Alpers, 2003). Furthermore, ethnic minorities were reported to receive much greater social support from ICSGs than Whites did (Fogel et al., 2003). However, ethnic minorities were reported to use ICSGs rarely (Hesse et al., 2005; Klemm, Hurst, Dearholt, & Trone, 1999; Pautler et al., 2001). Recent studies also indicated that ICSGs tended to serve highly educated, high-income Whites in the early stages of cancer. Thus, researchers have suggested that to increase their appeal and accessibility (and therefore their use and subsequent social support), culturally competent ICSGs should be developed specifically for ethnic minorities (Im, Chee, Tsai, Lin, & Cheng, 2005; Matsunaga et al., 1996). In this article, “cultural competence” is defined as the acknowledgment and affirmation of cultural sensitivity imbedded in cultural knowledge (Meleis, Lipson, & Paul, 1992).
To develop culturally competent ICSGs for ethnic minorities living with cancer, it is essential to identify what specific factors are predictive of their use of ICSGs. Although there are increasing numbers of studies on ICSGs, very little is known about the predictors that influence the use of ICSGs by ethnic minorities, especially Asian Americans (Hesse et al., 2005; Klemm et al., 1999; Pautler et al., 2001). The currently known predictors of the use of ICSGs include the following: background factors (age, gender, socioeconomic status, and perceived social support), disease factors (site and stage of cancer and treatment modalities), need factors (physiological, psychological, and social requirements for well-being), and Internet use factors (general use of the Internet; Fogel et al., 2002; Hesse et al., 2005; Pautler et al., 2001).
As a first step in developing culturally competent ICSGs for ethnic minorities living with cancer, this article focuses only on Asian Americans living with cancer who were online (ALCO) and compares their use of ICSGs with a reference group—Whites living with cancer who were online (WLCO). The purposes of this study were to explore differences in the use of ICSGs by ALCO and WLCO (with any type and stage of cancer) and determine the factors that influence the use of ICSGs by ALCO and WLCO. Asian Americans are defined here as those having origins in any of the original peoples of the Far East, Southeast Asia, or the Indian subcontinent (U.S. Census Bureau, 2007). ALCO refers to Asian Americans with past or present cancer diagnoses who were familiar with the Internet as a medium of communication and had access to e-mail and the Internet. ALCO were targeted in this study because Asian Americans are reported to use the Internet more than any other ethnic group (Madara & White, 1997; Rainie & Spooner, 2001) and because it has been reported that in ethnic minorities, including Asian Americans, the anonymity of ICSGs provided a comfortable forum to discuss sensitive personal health issues (Campbell et al., 2001; Cline & Haynes, 2001; Eysenbach, Powell, Englesakis, Rizo, & Stern, 2006). We also chose to use an Internet survey in this study to take advantage of the Internet’s capability to reach potential research participants in distant geographic areas quickly (Kollock & Smith, 1999; Strickland et al., 2003). Recruiting ALCO as participants on a national scale was necessary because the number of ALCO in any specific region of the country is limited. The specific aims of this study were as follows:
Aim 1: Explore differences in the use of ICSGs by ALCO and WLCO.
Aim 2: Determine the specific factors that are predictive of the use of ICSGs by ALCO and WLCO.
Conceptual Framework
This study was theoretically guided by the Factors Influencing the Use of Internet Cancer Support Groups (F-ICSG) model. The F-ICSG model was developed using the integrative approach by Im (2005) and based on a systematic literature review and a preliminary study (Im, Chee, Lim, et al., 2007). The F-ICSG model makes several assumptions about online interactions. When the Internet was introduced, many feminist scholars celebrated the anonymous (non-face-to-face) nature of Internet interactions, which they thought might eliminate discrimination based on appearance (e.g., by age, gender, ethnicity, or disability; Featherstone, 2000; Leary, 2000; Turkle, 1995). They thought that individuals who represented themselves through images and symbols could be freer in terms of their identities on the Internet (Waskul, Douglass, & Edgley, 2000). However, this idea has proven problematic, and the Internet is far from granting freedom from constraints or oppression related to embodied identity (Bassett, 1997; Kendall, 1998). Researchers have reported how power relations in the real world, including those regarding ethnicity, are reflected into online interactions (Pitts, 2004). Despite the Internet’s potential as a forum for diverse viewpoints and interests, it has already become dominated by corporate and media interests (Bell & Kennedy, 2000; Cartwright, 2000; Sardar, 2000). From this point of view, the F-ICSG model assumes that the use of ICSGs may reflect current constraints and oppression in the real world. Thus, the model assumes that the lack of use of ICSGs by ALCO comes from their continuous interactions with the real world and from cultural and social biases reflecting the ways that they view the real world.
The F-ICSG model includes mediating factors (predictors) that influence the use of ICSGs, which are essential components to consider in future ICSG development. The mediating factors include the following: (a) health factors, (b) background factors, (c) cultural factors, (d) need factors, and (e) Internet use factors. Health factors are circumstances such as health status, medical and nursing diagnosis, medication use, quality of life, functional status, and etiologic, developmental, and iatrogenic factors. Background factors are descriptors, including age, gender, race, marital status, socioeconomic status, number of children, and number of family members. Cultural factors are defined as those factors that represent one’s cultural background. Need factors are types of perceived psychological and social needs and all types of traditional support for coping with stress, uncertainty, socialization, powerlessness, social isolation, and stigma. Internet use factors include history, comfort with, and pattern of Internet use; type, availability, and quality of Internet resources; previous health-seeking behaviors, both online and offline; and attitudes toward Internet use. In this study, the F-ICSG model was adopted and modified to focus on cultural factors (see Figure 1). Differences in the use of ICSGs by ALCO and WLCO were first determined, and then the specific factors that influenced the use of ICSGs by ALCO and WLCO (a set of 13 selected variables, including health, background, needs, Internet use, and cultural factors) were determined.
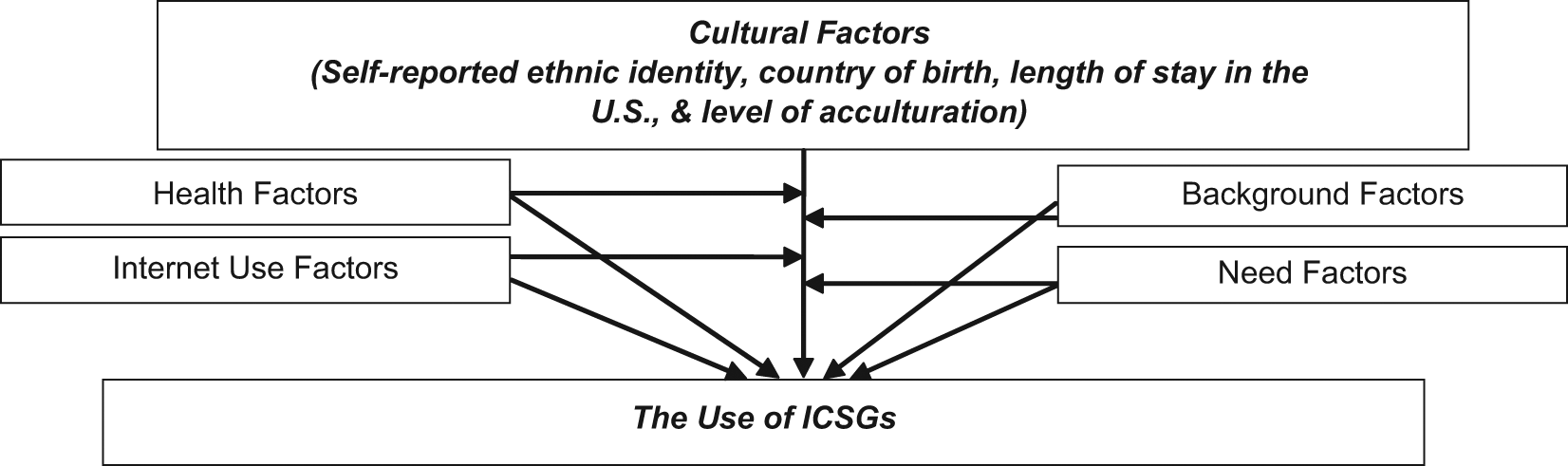
The factors influencing the use of Internet cancer support groups (F-ICSG) model
Method
This study was part of a larger study that used a cross-sectional comparative design with three components: (a) an Internet survey, (b) an expert review, and (c) an online forum. Only the findings from the Internet survey are presented in this article. The study was approved by the Institutional Review Board of the institution where the researchers are affiliated.
Settings and Participants
A total of 60 people living with cancer (30 ALCO and 30 WLCO) who could read and write English were recruited from across the nation using a convenience sampling method. ALCO and WLCO were matched using 1:1 matching on two possible confounding factors: gender and age. Gender and ethnicity have been reported to influence the use of ICSGs by people living with cancer (Im et al., 2005; Klemm et al., 1999; Klemm, Reppert, & Visich, 1998). For all the participants in the larger study (N = 117), appropriate samples were randomly chosen using SAS MACRO MATCH. All the participants self-reported that they were older than 18 years; anyone younger than 18 years was excluded from the study. Children younger than 18 years were excluded because they may not have adequately responded to the questions asked in the study because of their developmental stage. In addition, we assumed that the participants were able to differentiate their culture from others and describe differences in their culture, but children younger than 18 years might not be able to do this developmentally. To recruit participants, two types of recruitment strategies were used. First, ICSGs and Internet communities/groups for Asian Americans and Whites were identified in a search on google.com, and administrators of the first 20 groups/communities in the search results were contacted and asked to post an announcement about the study for their group. Second, informal leaders of communities/groups for Asian Americans and Whites were contacted and asked to announce the study. The announcement included general information about the study, as well as contact numbers, an e-mail address, and the dates on which data would be collected.
We used the NOETHER estimation (Hamilton & Collings, 1991) to calculate the sample size necessary to address Aim 1 using Wilcoxon rank-sum tests at an alpha level of .05; at least 23 participants per group were needed to detect a statistically significant difference. Nonparametric regression analyses (Aim 2) are potentially useful for small samples (Rutherford & Yakowitz, 1991). The minimum sample size required for nonparametric regression tests is 50 (Zhang & Lu, 2008). Because this was a pilot study, we chose a reasonable sample size that could be recruited during the given period of funding.
Instruments
The Internet questionnaire included self-administered questions on background factors, cultural factors, health factors, the Support Care Needs Survey-34 Short Form (SCNS-34SF; to measure need factors), the 2003 Health Information National Trends Survey (HINTS) subscale on Internet usage (to measure Internet use factors), and the Use of Internet Cancer Support Groups (UICSG) Questionnaire (to measure the use of ICSGs).
Background factors
Eleven questions on age, gender, education, religion, marital status, employment, degree of difficulty in paying for basics (a proxy for socioeconomic status), and availability of perceived social support described participants’ background factors. The question on the degree of difficulty in paying for basics was chosen for this study to measure socioeconomic status because cancer patients rarely answered the question about their family income in previous studies (Im, Chee, Guevara, et al., 2007).
Cultural factors
Cultural factors were measured using questions on self-reported ethnic identity, country of birth, the length of stay in the United States, and the level of acculturation. Self-reported ethnic identity was measured using the ethnic identity question required in the National Institute of Health’s guidelines. The length of stay in the United States was measured in months and/or years. The level of acculturation was measured using five questions about foods, music, customs, language, and close friends using a Likert-type scale of 1 to 5 (1 = exclusively one’s own ethnic group, 5 = exclusively American). These five questions were adopted from among the questions on the Suinn–Lew Asian Self-Identity Acculturation Scale (Suinn, Ahuna, & Khoom, 1992) to reduce potential participant burden, and modified to measure the degree of acculturation in multiple ethnic groups (Im, Chee, Guevara, et al., 2007). In the data analysis, the scores of these five questions were totaled and used to represent the level of acculturation. The validity and reliability of the original Suinn-Lew Asian Self-Identity Acculturation Scale have been supported in Asian populations (Suinn et al., 1992). The reliability of the modified five questions was also well supported in more than 10 studies of multiple ethnic groups in the United States (Im, Chee, et al., 2008). The reliability of the questions used in this study was high (Cronbach’s α = .82).
Health factors
Health factors were measured using seven items on general health, diagnosis of cancer, length of time since diagnosis, primary site and stage of cancer, previous and current medical treatments (e.g., radiation therapy, chemotherapy, surgery, or hormone therapy), and medication use.
Support Care Needs Survey-34 Short Form
The SCNS-34SF was developed by consecutively removing the items from the original Cancer Needs Questionnaire with the lowest magnitude of need until the minimal criteria for an acceptable short-form version was extracted (Sanson-Fisher et al., 2000). The SCNS-34SF includes 34 items, consisting of five domains of need (11 items on psychological needs, 9 items on health information needs, 6 items on physical needs, 5 items on support needs, and 3 items on communication needs). Respondents rate each item on a 5-point scale (1 = no need to 5 = high need for help). Individual item scores are summed to obtain a total score (the SCNS score), which ranges from 34 to 170, with higher scores indicating greater needs. The short-form version showed acceptable construct validity and internal reliability, a capacity to reproduce the original mean factor scores with a precision of 75% or more, nonsignificant differences between mean factor scores on the long- and short-forms, and acceptable sensitivity and specificity on the short-form (Lattimore-Foot, 1996). In a study by Crossich, Schofield, and McLachlan (2004), Cronbach’s alpha coefficients for all the domains ranged from .77 to .94, and most of the a priori predictions regarding the convergent and contrasting groups’ construct validity were well supported. In this study, the reliability (Cronbach’s alpha coefficient) of this scale was .96.
The 2003 Health Information National Trends Survey subscale
The 2003 HINTS questionnaire provides an assessment of how the general population accesses and uses current communication channels to obtain health information, and it collects baseline data on cancer knowledge, attitudes, and behaviors (Ling, Klein, & Dang, 2006). Items on the 2003 HINTS questionnaire were created by an interdisciplinary team of communication researchers and were vetted by members of the external research community. All items were cognitively tested in a 150+ person field-test and used in a national survey in 2002 (Ling et al., 2006). The HINTS includes 14 modules, each with several subsections. Only the subsection that included the 14 questions on general Internet use was used for this study. Total scores of the questions were calculated and used as a composite score representing general Internet use. The reliability and construct validity of the HINTS questionnaire were well established by the national survey (Hesse et al., 2005; Rutten, Squiers, & Hesse, 2006; Viswanath et al., 2006). In this study, the reliability (Cronbach’s alpha coefficient) of this scale was .63. When an instrument has a short scale, a .50 value for Cronbach’s alpha coefficient is usually acceptable (Kehoe, 1995).
The UICSG Questionnaire
Eight questions on the UICSG were developed for this study because no other instrument was available. Detailed information about the instrument can be found elsewhere (Im, Lee, & Chee, 2011). Briefly, questions were developed based on the qualitative findings of a previous study (Im, Chee, Lim, et al., 2007) and the subsection on general Internet use included in the 2003 HINTS questionnaire. These questions were then validated by a panel of four experts (Im et al., 2011). The questions are about the use of ICSGs, the frequency of using ICSGs, access to ICSGs, reasons for using ICSGs, usefulness of ICSGs, and the likelihood of using ICSGs in the near future. These questions were selected based on a theoretical construct developed through a systematic literature review. Each item uses either a 5-point Likert-type scale or a dichotomous scale. A total score was calculated by summing the individual scores of all the items; thus, the total score was a composite score representing the use of ICSGs. The content validity of the questions was supported in a review by eight experts (mean agreement on a 1-5 scale = 4.25, SD = 0.46). In this study, the reliability (Cronbach’s alpha coefficient) of this scale was .74.
Data Collection Procedures
A website conforming to the Health Insurance Portability and Accountability Act and the SysAdmin, Audit, Networking, and Security/Federal Bureau of Investigation recommendations was developed and published on an independent, dedicated website server consisting of five Pentium-based computers. The website included an informed consent form, Internet survey questions, and online forum sites. When potential participants visited the project website, the opening page explained the purpose of the study, and visitors were asked to click to enter the “informed consent form.” Informed consent was obtained via the Internet by asking potential participants to click the “I agree to participate” button. When they clicked the button, they were queried to verify that they met the inclusion criteria (age, literacy, Internet access, and ethnic identity). Those who met the inclusion criteria were automatically connected to the Internet survey web page, where they were asked to answer the questions on sociodemographic characteristics, cultural factors, and self-reported disease status, as well as complete the SCNS-34SF, the HINTS subscale, and the UICSG Questionnaire. Although a participant entered his or her answers, four or more random questions that the participant had already answered were repeated to check for consistency in his or her answers for the purpose of identity verification.
Data Management and Analysis
The Internet survey data were directly saved in ASCII format and were analyzed using the Statistical Analysis System Version 8.1 (SAS Institute, Cary, NC). Participants for whom 10% or more data were missing were not included in the data analysis. To describe the characteristics of the research participants, the data were analyzed using descriptive statistics, including frequency, percentage, proportion, mean, standard deviation, range, skewness, kurtosis, and 95% confidence intervals. In this study, a nonparametric approach was chosen because the key variables were not normally distributed. The normality tests showed that skewness and kurtosis of the UICSG, general Internet use, and SCNS scores for each ethnic group ranged from −1.83 to 0.05 and from −1.21 to 2.89, respectively. In general, normal distributions have zero skewness and zero kurtosis. Thus, Wilcoxon rank-sum tests and nonparametric multiple regression analyses were conducted. In addition, the appropriateness of the variables was checked for regression analyses. Tolerance of the age variable was less than .10, which indicates possible multicollinearity. Thus, age was excluded in the multiple regression analyses. “Level of acculturation” and “length of stay in United States” were measured only for those who were not born in United States; thus, for those who were born in the United States, mean substitutions were used for these variables in the multiple regression analyses. When only a few valid responses are available to predict a larger number of missing responses, mean substitutions are usually recommended (Stommel & Wills, 2003). Because of the small sample size, and to determine the predictive variables, stepwise multiple regression analyses were performed with health factors, background factors, cultural factors, need factors, and Internet use factors. To control for Type І errors in the stepwise regression analyses, we used the true stepwise procedure (Myers & Well, 2002). Only the variables that had valid beta coefficients were included in the nonparametric multiple regression analyses.
Findings
Characteristics of the Participants
Most of the participants reported their education level as high (college graduates or higher). About 72% of the participants were married or partnered, and 40% were employed. The mean family income level (1 = totally insufficient to 4 = more than sufficient) was 2.77 (SD = 0.98). About 47% of the ALCO were born outside the United States; mean residence time in the United States was 25.27 years (SD = 10.03). The mean score for the level of acculturation was 16.50 (SD = 2.95), ranging from 12 to 22. The mean level of social support (perceived availability of social support: 1 = none of the time to 4 = most of time) was 3.48 (SD = 0.72). The mean general health score was 3.38 (SD = 1.24; 1 = very unhealthy to 5 = very healthy). About 37% of the participants were breast cancer patients and the mean length of time since their diagnosis was 3.33 years (SD = 4.56). About 32% of the participants currently had Stage ІІ cancers. About 53% of the participants had undergone radiation therapy, 67% had chemotherapy, 68% had surgery, and 35% had hormone therapy. About 33% of the participants were currently taking pain medications. The sociodemographic characteristics of the participants are summarized in Table 1.
Sociodemographic Characteristics of Participants (N = 60)
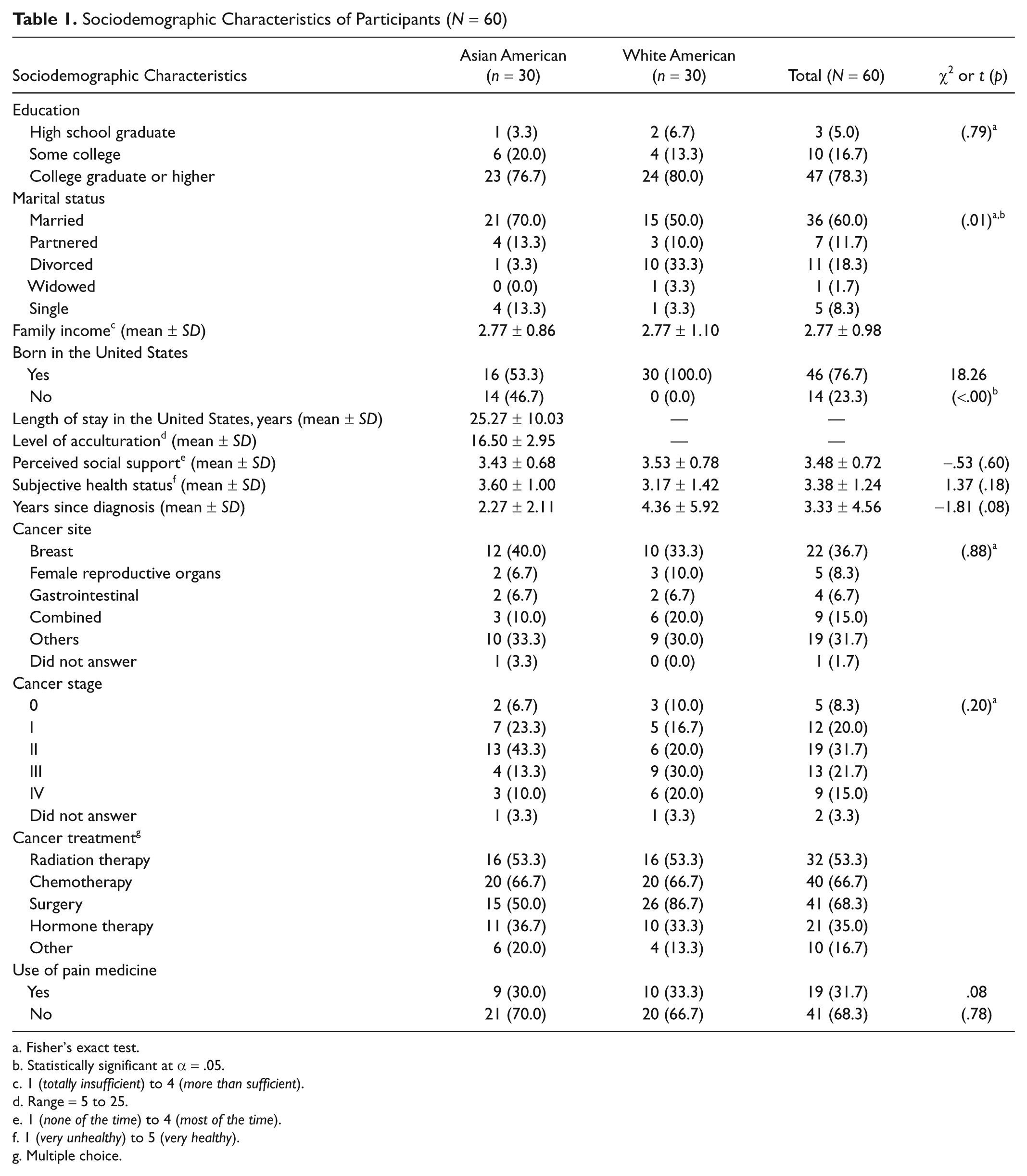
Fisher’s exact test.
Statistically significant at α = .05.
1 (totally insufficient) to 4 (more than sufficient).
Range = 5 to 25.
1 (none of the time) to 4 (most of the time).
1 (very unhealthy) to 5 (very healthy).
Multiple choice.
The Use of Internet Cancer Support Groups
The mean UICSG score across ethnic groups was 5.88 (SD = 2.05). The UICSG scores for ALCO and WLCO were significantly different (p < .03). The mean score for general Internet use across ethnic groups was 11.48 (SD = 2.23; see Table 2).
Differences in the use of ICSGs, General Internet Use, and Needs for Help Between ALCO and WLCO (Wilcoxon Rank-Sum Test); N = 60
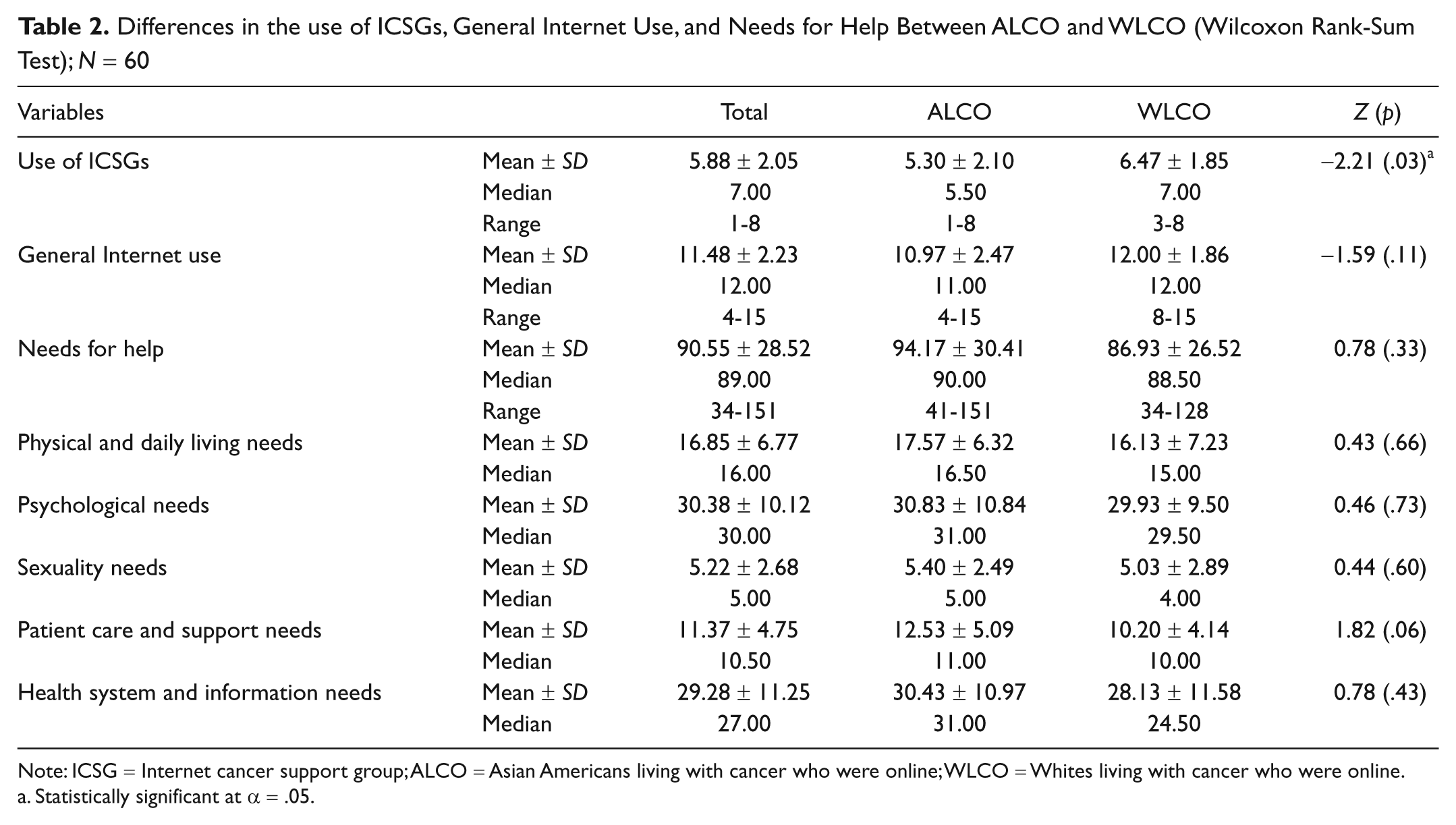
Note: ICSG = Internet cancer support group; ALCO = Asian Americans living with cancer who were online; WLCO = Whites living with cancer who were online.
Statistically significant at α = .05.
Factors Influencing the Use of Internet Cancer Support Groups
The significant factors influencing the use of ICSGs included “self-reported ethnic identity” (p < .01), “born in the United States” (p < .05), and “general Internet use” (p < .05; see Table 3). However, in the nonparametric regression analyses for each ethnic group, no statistically significant predictors of the use of ICSGs were identified (see Table 4).
Predictors of Use of ICSGs for All Participants (Nonparametric Multiple Regression); N = 60
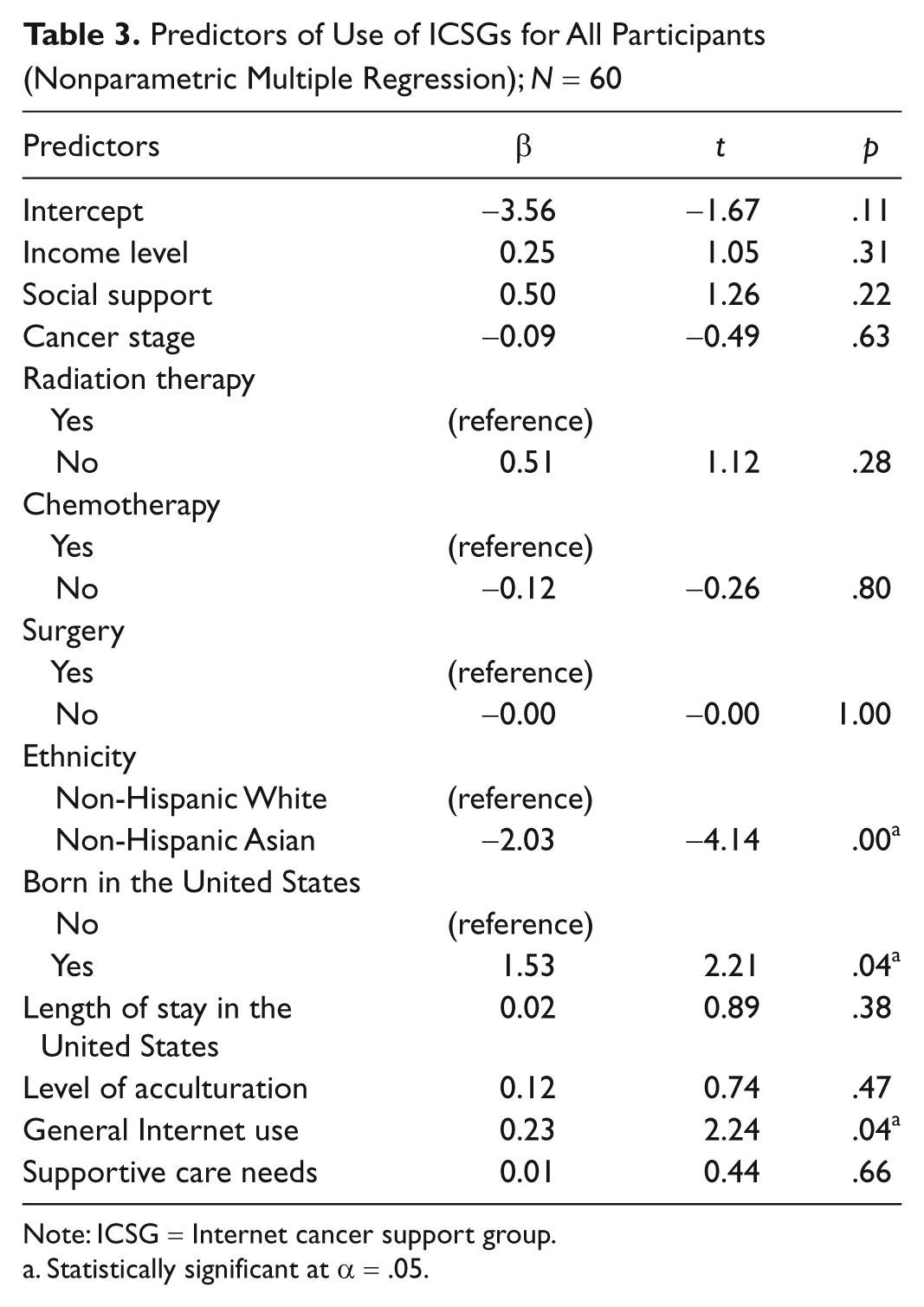
Note: ICSG = Internet cancer support group.
Statistically significant at α = .05.
Predictors of Use of ICSGs by Ethnicity (Nonparametric Multiple Regression); N = 60
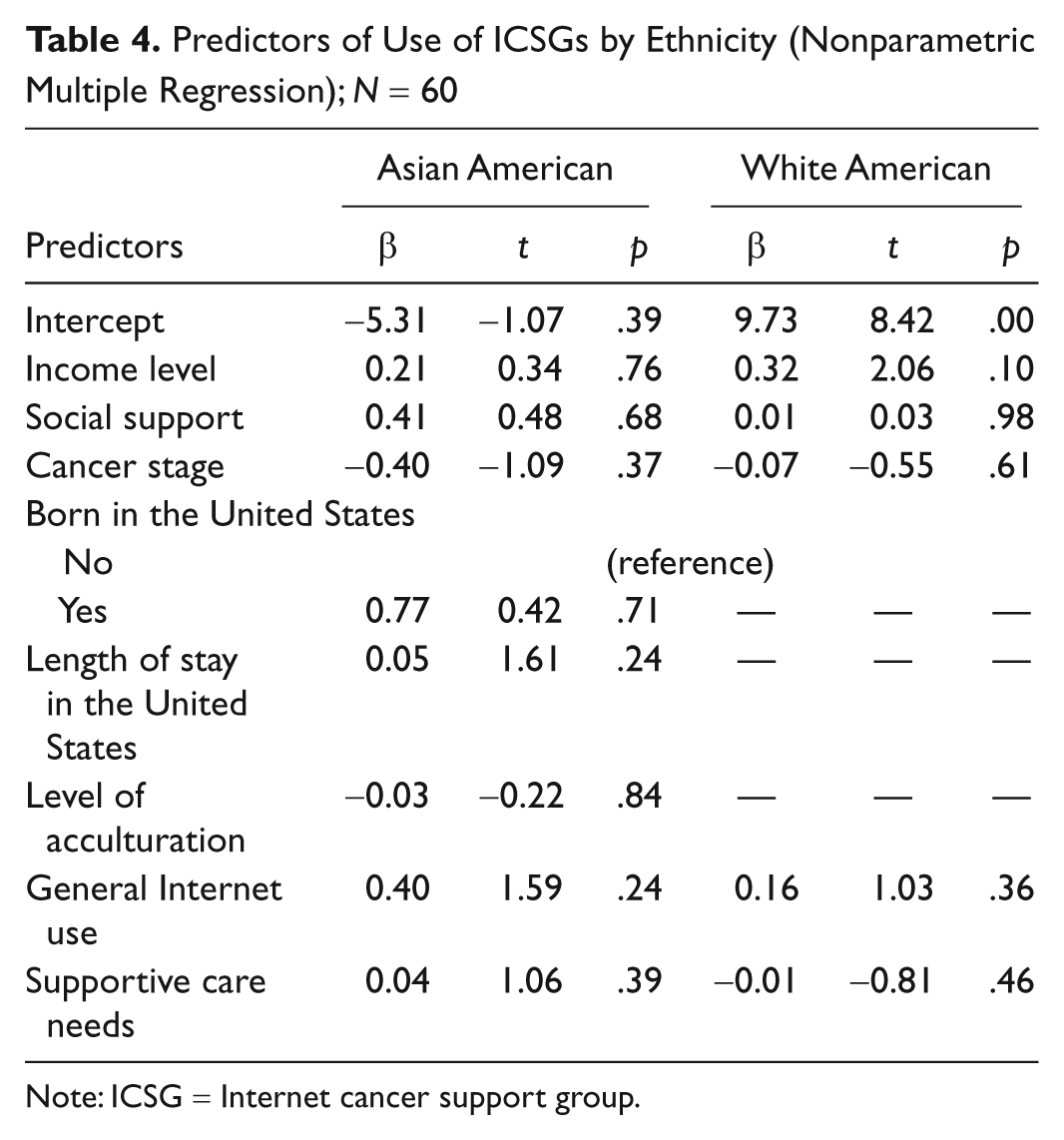
Note: ICSG = Internet cancer support group.
Discussion
The findings of this study show ethnic differences in the use of ICSGs: ALCO were less likely to use ICSGs than WLCO. The differences may stem from differences in cultural attitudes toward cancer between ALCO and WLCO. Indeed, the literature indicates that Asian Americans tend to stigmatize cancer (Im, Liu, Kim, & Chee, 2008; Simpson, 2005), which could influence ALCO’s use of ICSGs. In other words, ALCO might not want to disclose their cancer even on the Internet interactions because of the stigma attached to cancer in Asian culture. Although researchers have asserted that the anonymity of ICSGs could provide a comfortable forum to discuss sensitive health issues, including cancer (Campbell et al., 2001; Cline & Haynes, 2001; Eysenbach et al., 2006), this might not work for Asian Americans.
Although there were differences in the use of ICSGs between ALCO and WLCO, there were no ethnic differences in general Internet use and in the needs for help. In other words, ALCO had a similar rate of general Internet use and similar needs for help as WLCO, but the rate of use of ICSGs by ALCO was lower than that of WLCO. This finding may indicate that ICSG use by ALCO does not stem from differences in their general use of the Internet or in their needs for help.
These findings are partially consistent with the current literature, which indicates that ICSGs tended to serve highly educated, high-income Whites in the early stages of cancer, and that there were ethnic differences in ICSG use (Hesse et al., 2005; Klemm et al., 1999; Pautler et al., 2001). Shaw et al. (2006) reported that being White and having a higher energy level predicted higher volumes of writing by active participants in ICSGs. A recent analysis by Im et al. (2005) indicated that only 24 out of the 546 ICSGs examined were intended specifically for ethnic minorities, but minority participation in those 24 ICSGs was minimal. The HINTS by the National Cancer Institute also indicated that ethnic minorities rarely used ICSGs, although when they did use them, they received greater perceived benefits than Whites (Hesse et al., 2005).
Our findings that there were no ethnic differences in the participants’ general use of the Internet or in their needs for help, however, are quite different from findings reported in the literature; thus, this study contributes new information to the current literature. Indeed, the literature indicates ethnic differences in the general use of the Internet by people living with cancer. For example, James and Rice (2002) reported that the use of Internet information was uniformly low among ethnic minorities. The HINTS also reported significant ethnic differences between Hispanics and non-Hispanics in their general use of the Internet (Hesse et al., 2005). In addition, previous studies have reported specific ethnic differences in the needs for help of people living with cancer. Whites tended to place the highest priority on their own individual needs and wanted to have control over their own bodies and lives, whereas cancer patients in some cultures (e.g., Asian and Hispanic cultures) tended to emphasize the needs of their families (familism; Pinquart & Sörensen, 2005). Thus, Asian cancer patients tended to have lower scores on needs assessments than those from other ethnic backgrounds (Im, Chee, et al., 2008; Lipson & Dibble, 2005). Also, ethnic minorities living with cancer tended to present with later stage disease than Whites, so their physical needs were frequently different from that of Whites as well (Delgado, Lin, & Coffey, 1995; Eley et al., 1994). Ethnic minorities reported greater informational, practical, supportive, and spiritual needs than Whites (Moadel, Morgan, & Dutcher, 2006).
This discrepancy between the findings of this study and those of previous studies may reflect that the participants in this study were a select group of people living with cancer. Although ALCO were matched with WLCO in terms of their gender and age, the majority of participants were highly educated and married with high incomes. Previous Internet surveys indicated that cancer patients recruited through ICSGs tended to be middle aged, female, well educated, and middle class (Im, Chee, Liu, et al., 2007). Furthermore, because all the participants in this study, regardless of their ethnic identity, were recruited via the Internet, their general use of the Internet may be similar across the ethnic groups.
The low rate of use of ICSGs by ALCOs in this study was also related to cultural factors, which adds new information to the current literature. Indeed, in this study, “self-reported ethnic identity” and “born in the United States” were significantly correlated with the use of ICSGs across ethnic groups when other factors were controlled. Previous studies on the relationship between cultural factors and general Internet use have also strongly suggested an association between these factors and the use of ICSGs by people living with cancer (Barry, 2001; Tsai, 2001; Ye, 2005). Tsai (2001) reported that Internet and e-mail access facilitated the transition of immigrant families, and the transitions they made as immigrants to a new country caused them to rely on Internet and e-mail access. Ye (2005) found a positive relationship between acculturative stress and Internet use, and reported that immigrants had three motivations for using the Internet: information seeking, relaxation/entertainment, and social utility. Barry (2001) reported that Arabic immigrants to the United States used the Internet and it was an effective vehicle for addressing the concerns of Arab immigrants.
It may be hasty, however, to draw these conclusions because very few studies have explored the relationships between cultural factors, including self-reported ethnic identity, country of birth, length of stay in the United States, and level of acculturation, and the use of ICSGs. In fact, the relationships between cultural factors and general Internet use have not been adequately explored (Barry, 2001; Tsai, 2001; Ye, 2005). Furthermore, in this study, no significant predictors were found to influence the use of ICSGs by either ethnic group, which may be because of the small number of samples in each group. In addition, these findings should be interpreted carefully for several reasons, most of which stem from the inherent nature of a pilot study. First, the sample size for this study was small because of feasibility issues inherent in a pilot study. Second, the participants might have been a select group of ALCO and WLCO; in fact, they tended to have high incomes and college educations, and as a whole, were not representative of the diversity among Asian Americans. In this study, ALCO included only the following Asian subethnic groups: Chinese (10), Filipino (5), Japanese (4), Korean (2), Persian (1), Indian (1), and not specified (7). In addition, cultural factors were operationalized as only several variables, which may not have been comprehensive enough to represent all the cultural factors that may influence the use of ICSGs by ALCO. In addition, the number of questions used to measure the level of acculturation was limited to five to reduce the participants’ burden.
The findings must also be interpreted carefully because of the possibility that the instruments might lack cultural sensitivity. Indeed, recent studies have reported issues related to the appropriate use of instruments that were developed for a specific ethnic group in a different ethnic group (Bergh et al., 2005; Closs & Briggs, 2002; Deschamps, Band, & Coldman, 1988). The instruments used in this study have rarely been tested in different ethnic groups of people living with cancer, especially ALCO. Thus, for a better understanding of these findings, the cultural appropriateness and adequacy of the instruments used in this study should be further examined and established.
Conclusions
Although no significant ethnic differences in general Internet use and the needs for help were found, the findings of this study strongly indicate ethnic differences in the use of ICSGs. The findings suggest that cultural factors could explain the ethnic differences in the use of ICSGs. Based on these findings, we conclude this article with the following recommendations for future research and practice with ALCO.
First, health care providers and researchers who wish to develop ICSGs for ALCO or WLCO should take into consideration the ethnic differences and influencing factors in the use of ICSGs. Most importantly, cultural factors should be incorporated into the design and structure of ICSGs for ALCO. For example, because the findings of this study indicated that the country of origin was a significant predictor of the use of ICSGs by ALCO, an ICSG for ALCO could be developed and constructed based on the country of origin (e.g., for U.S.-born, China-born, etc.). We believe that doing so would help increase participation by ALCO in ICSGs.
Second, further studies with a larger number of ALCO and WLCO should be conducted to confirm the findings reported in this article. As discussed above, one of the major limitations of this study was the small sample size. With a larger number of ALCO and WLCO, future studies could provide a clearer picture of the factors influencing the use of ICSGs by ALCO and WLCO.
Finally, the instrument that we used to measure the use of ICSGs should be further developed, refined, and tested in people of different ethnicities living with cancer. Because no instrument is currently available to measure the use of ICSGs, a new instrument was developed for this study based on a previous study (Im, Chee, Lim, et al., 2007) and the 2003 HINTS questionnaire. Thus, the instrument itself should be further examined and refined with a diversity of people living with cancer.
Footnotes
Acknowledgements
We acknowledge the efforts made by Dr. Young Ran Lee and Ms. Chia-Chun Li who helped the recruitment, data collection, and data analysis process.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
This study was funded by the Expedited Proposal-Enhancement Grant (EP-EG) program, the Center for Health Promotion Research (a National Institutes of Health–funded research center, NINR, P30 NR05051).