
Abstract
Keywords
Introduction
Diabetes mellitus affects approximately 23.5 million individuals in the United States and continues to rise as our society becomes increasingly overweight and sedentary. Of those 23.5 million individuals with diabetes, 11.5 million are women (Centers for Disease Control and Prevention [CDC], 2007). Blacks are more than twice as likely as Whites to have diabetes mellitus, and Black women have the highest overall prevalence of all racial and gender groups (CDC, 2007). Diabetes is associated with complications that include cardiovascular disease, nephropathy, neuropathy, retinopathy, stroke, and mobility limitations, resulting in high direct and indirect personal and societal costs (CDC, 2007).
Physical activity is a cornerstone of diabetes mellitus treatment and can reduce many risks associated with diabetes mellitus. However, the majority of individuals with diabetes mellitus are sedentary (Morrato, Hill, Wyatt, Ghushchyan, & Sullivan, 2007). Participating in regular, moderate-intensity physical activity has been convincingly shown to lower the risk of coronary heart disease, stroke, hypertension, and dyslipidemia and to decrease insulin resistance and depression (Physical Activity Guidelines Advisory Committee, 2008). Even modest increments in physical fitness can reduce the risk of overall mortality twofold (Myers et al., 2002), and these benefits are generally independent of body weight (Physical Activity Guidelines Advisory Committee, 2008). Individuals with diabetes mellitus have a higher prevalence of psychological factors such as depression and anxiety, which may contribute to diminished quality of life (QOL) and inadequate diabetes mellitus self-management. The prevalence of depression is higher in women with diabetes mellitus than in men with diabetes mellitus (Bonnet et al., 2005). Depression has been shown to decrease levels of physical activity (Allan, Johnston, Johnston, & Mant, 2007). Moreover, greater levels of anxiety are associated with physical inactivity (Smits & Zvolensky, 2006). People who are inactive tend to be older (>45 ± 10 years), have higher levels of anxiety and depression, be overweight, have low QOL, and a greater incidence of cardiovascular disease (Panagiotakos et al., 2008). Despite the association of regular exercise with fewer symptoms of anxiety and depression, some studies have shown no causal effect of exercise (De Moor, Boomsma, Stubbe, Willemsen, & de Geus, 2008).
Black women have the lowest reported levels of leisure-time and habitual physical activity among all ethnic groups (CDC, 2004) and higher levels of sedentary behavior than White women (Adams-Campbell et al., 2000). However, little information is available on the physiological, psychological, and behavioral factors associated with lower levels of physical activity in Black women with type 2 diabetes mellitus (T2DM). Therefore, the purpose of this secondary data analysis on Black women with T2DM was to (a) describe their physical activity (activity and inactivity, time watching television, confinement to bed); (b) identify the relationships among physiological (hemoglobin A1c [HbA1c], lipids, blood pressure [BP], waist circumference, and body mass index [BMI]), psychological (somatic anxiety, emotional distress), and behavioral factors (QOL and health care provider support for physical activity); and (c) identify inactivity factors (active vs. inactive, time viewing TV, confinement to bed) associated with demographics, and physiological (HbA1c, lipids, BP, waist circumference, and BMI), psychological (somatic anxiety, emotional distress), and behavioral factors (QOL, health care provider support for physical activity).
Method
Study Design
We examined baseline, cross-sectional data from 109 Black women from African American, Caribbean, and Cape Verdean descent with T2DM who enrolled in an intervention trial (N = 109). The parent study from which data were obtained was a randomized clinical trial conducted to test the effectiveness of a culturally competent intervention of diabetes mellitus self-management education, coping skills training, and care compared with traditional diabetes mellitus education and care of urban, Black women with T2DM in primary care (N = 109). The parent study was powered to detect a change in HbA1c of 1.2% with two groups and four time points during the 24-month follow-up period (α = .05; power = 95%), resulting in 49 participants per group or a total of 98 subjects. To address issues of attrition, 109 women were enrolled. For this current cross-sectional secondary data analysis, we used a descriptive, correlational study design to explore physiological, psychological, and behavioral factors associated with physical activity and T2DM in Black women (N = 109).
Sample and Setting
Participants were recruited from a community health care clinic, private primary care practices, and health fairs in urban settings of southern New England. Inclusion criteria were (a) diagnosis of T2DM confirmed by C-peptide levels, (b) Black American female, (c) 21 to 64 years old, and (d) able to read and speak English. Exclusion criteria were (a) receiving insulin therapy, (b) existence of other serious illnesses (e.g., cancer, multiple sclerosis), and (c) diabetes mellitus–related complications that precluded independence (e.g., visual impairment, end-stage renal disease, lower extremity amputation) or interfered with participation or metabolic outcomes.
Written informed consent was obtained from participants in accordance with study protocols and the human subjects’ research and review committee at the authors’ university. Study data were obtained from all 109 participants in the randomized control trial.
Demographic Information
Demographic data included age, education, income, and marriage status (single and living alone, single and living with partner, married, divorced, widowed). Participants also provided information on current prescription medications, over-the-counter medications, and vitamins. A self-reported health history included the following: (a) diabetes mellitus complications of kidneys, eyes, and/or feet problems; (b) hypertension; and (c) dyslipdemia. Participants were also asked (a) if they had ever been told by a health care provider that their weight was a health problem; (b) if yes, they circled all items (joints, blood pressure, diabetes mellitus, heart, other) that they had been told were affected by their weight; (c) were they ever told to lose weight as part of a treatment or health maintenance plan; and (d) if they smoked.
Physiological Measures
Hemoglobin A1c
HbA1c, a routine measure of the average blood glucose for a previous 3-month period, was estimated in samples of participants’ venous blood using the Glyc-Affn Assay (Isolab, Inc., Akron, OH). This method measures all glycohemoglobin; thus, glycosylated hemoglobin variants, such as sickle cell, are deleted.
Lipid levels
Lipids measured included total cholesterol, triglycerides, low-density lipoprotein (LDL), and high-density lipoprotein (HDL). This lipid profile was obtained from samples of venous blood after at least an 8-hour fast.
Blood pressure
Blood pressure was measured as systolic and diastolic pressure recorded with a standardized mercury manometer. Participants were seated in a chair with back supported, arms bared, and supported at heart level, wearing an appropriate size cuff, and at rest for 5 minutes before the first reading was taken. For 30 minutes before readings, participants refrained from smoking or caffeine intake. Systolic BP was recorded at the first appearance of sound (Phase 1) and diastolic BP on sound disappearance (Phase 5) separated by 5 minutes and averaged to obtain systolic BP and diastolic BP.
Body mass index
BMI was calculated from participants’ weight (kg) divided by the square of their height (m). Weight was converted to kilogram after being measured to the nearest quarter pound using a standard balance beam scale. Height was converted to meter after being measured without shoes and socks to the nearest quarter inch using the same scale.
Waist circumference
Waist circumference was measured by research staff trained to use the following procedure: (a) place tape measure around participant’s bare abdomen, 1 inch above the umbilicus; (b) pull tape measure taut without pinching the skin; (c) instruct participants to relax and exhale; then (d) measure waist.
Psychological Measures
Emotional distress
Diabetes mellitus–specific emotional distress (denial, worry, frustration, anger, interpersonal distress, and other emotions associated with psychological adjustment to diabetes mellitus) was measured using the 25-item Problem Areas in Diabetes(PAID) Questionnaire (Polonsky et al., 1995). Items are rated on a 6-point Likert-type scale. Scores range from 25 to 100, with higher scores reflecting higher levels of distress. High levels of internal consistency have been demonstrated with alpha coefficients ranging from .93 to .95 (Polonsky et al., 1995). Concurrent validity has been established with generalized distress, fear of hypoglycemia, and adherence to several self-care behaviors (Polonsky et al., 1995).
Anxiety
Anxiety was measured using the Somatic Anxiety subscale of the Crown–Crisp Anxiety Index (Crown & Crisp, 1966). This standardized, self-rating 8-item inventory has two to three levels of possible responses to each question. Scores can range from 0 to 16, with higher scores indicating higher levels of phobic anxiety. The Crown–Crisp Index has been validated in psychiatric outpatient clinic settings and found to discriminate patients with anxiety disorders and agoraphobia from healthy controls (Burgess, Mazzocco, & Campbell, 1987).
Behavioral Measures
Quality of life
QOL was measured with the Medical Outcomes Study Short-Form-36 (SF-36; Ware & Sherbourne, 1992). This 36-item self-report instrument uses a Likert-type scale to assess eight health concepts on eight subscales. For this study, only three subscales were used: (a) limitations in physical activity due to health problems (physical function), (b) bodily pain, and (c) vitality (energy and fatigue). Scores range from 0 (low functioning) to 100 (maximum functioning). Transformed scores were used, with higher scores indicating higher QOL for each subscale. The alpha coefficients for the eight scales have ranged from .78 to .93 (Ware & Sherbourne, 1992).
Health Care Provider Support for Exercise
Health care provider support for exercise was measured using the exercise subscale of the Modified Health Care Climate Questionnaire, which measures the extent to which providers elicit and acknowledge patients’ perspectives and support their initiatives, while minimizing pressure and control (Williams, Rodin, & Ryan, 1998). The exercise subscale contains six items that are rated on a 7-point Likert-type scale ranging from strongly disagree to strongly agree. This questionnaire has been used in studies of weight loss and smoking cessation, with Cronbach’s α of .92 and .96, respectively (Williams et al., 1998). Factor analysis has shown a one-factor solution measuring perceived autonomy support (Williams et al., 1998).
Physical Activity
Physical activity was measured by three items from the six-item Modifiable Physical Activity Questionnaire (MAQ; Kriska et al., 1990). The MAQ is a structured interview that measures leisure activity, occupational activity, inactivity, and total activity. Test–retest reliability has ranged from .35 to .92 in a population of Pima Indians (Kriska et al., 1990). The MAQ has been validated by correlations between its activity measure and total energy expenditure using the Caltrac activity monitor ranging from .50 to .80 (p < .05; Kriska et al., 1990). For this study, we used three MAQ items: (a) type of physical activity engaged in >10 times in the past year, (b) how many hours/day usually spent watching television, and (c) >1 week spent confined to a bed or chair in the past year due to injury, illness, or surgery.
Data Analysis
Data were entered into Microsoft Access by research staff using a double-entry system, with verification of accuracy by comparing data sets. Frequency distributions and appropriate summary statistics for central tendency and variability were used to describe demographic and clinical data. These calculations were made using SPSS (Version 15). The relationship between physiological, psychological, and behavioral factors was explored using Spearman correlation coefficients due to nonnormal distribution of some data. Baseline comparisons were made between active and nonactive groups, <2 hours and >2 hours of television viewing per week, as well as no and ≥1 week confinement to bed in the last year by t tests or χ2 analyses.
Results
Of the 109 participating women, most were low income and obese, with a mean age of 48 years, and had suboptimal control of lipids, HbA1c, and blood pressure (Table 1). Participants had diabetes mellitus on average for 5 ± 8 years, and the majority was single living alone (45) with only 28 married, 8 single and living with a partner, 24 divorced, and 3 widowed. A minority of women reported taking hypertensive medications (31%), lipid-lowering medications (13%), over-the-counter medications (3%), and vitamins (11%). Participant self-reported the following diabetes mellitus complications and medical-related conditions: kidney disease (61%), eye disease (24%), foot problems (47%), hypertension (31%), and high lipid levels (37%). Twenty-seven women were told their weight was a health problem (25%). Participants reported being told their weight was affecting their joints (17%), BP (50%), diabetes mellitus (66%), and heart (26%). A minority of women were told to lose weight as part of their treatment plan (15%). One fourth of the participants (n = 27, 25%) reported a smoking history, with 25 of those women currently smoking.
Participant Characteristics (N = 109)
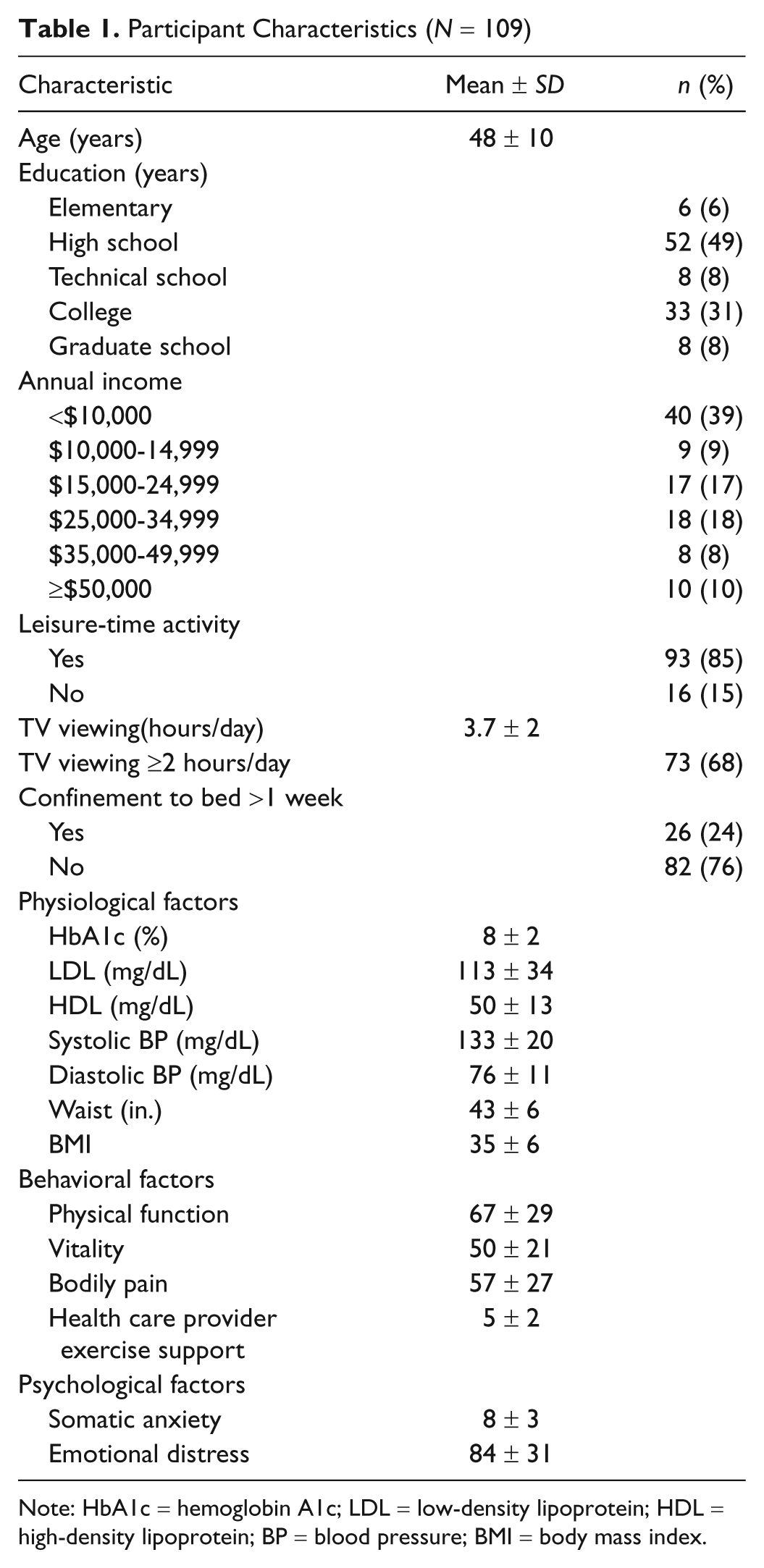
Note: HbA1c = hemoglobin A1c; LDL = low-density lipoprotein; HDL = high-density lipoprotein; BP = blood pressure; BMI = body mass index.
Physical Activity and Inactivity, Television Viewing, and Confinement to Bed
Most women (n = 93, 85%) reported some leisure-time physical activity, with the majority preferring walking for physical activity (n = 65, 60%; Table 2). They viewed TV on average for 3.5 hours/day. During the previous year, 26 women (24%) reported confinement to bed for an average of 3 to 4 weeks.
Participants Leisure-Time Activities (N = 109)
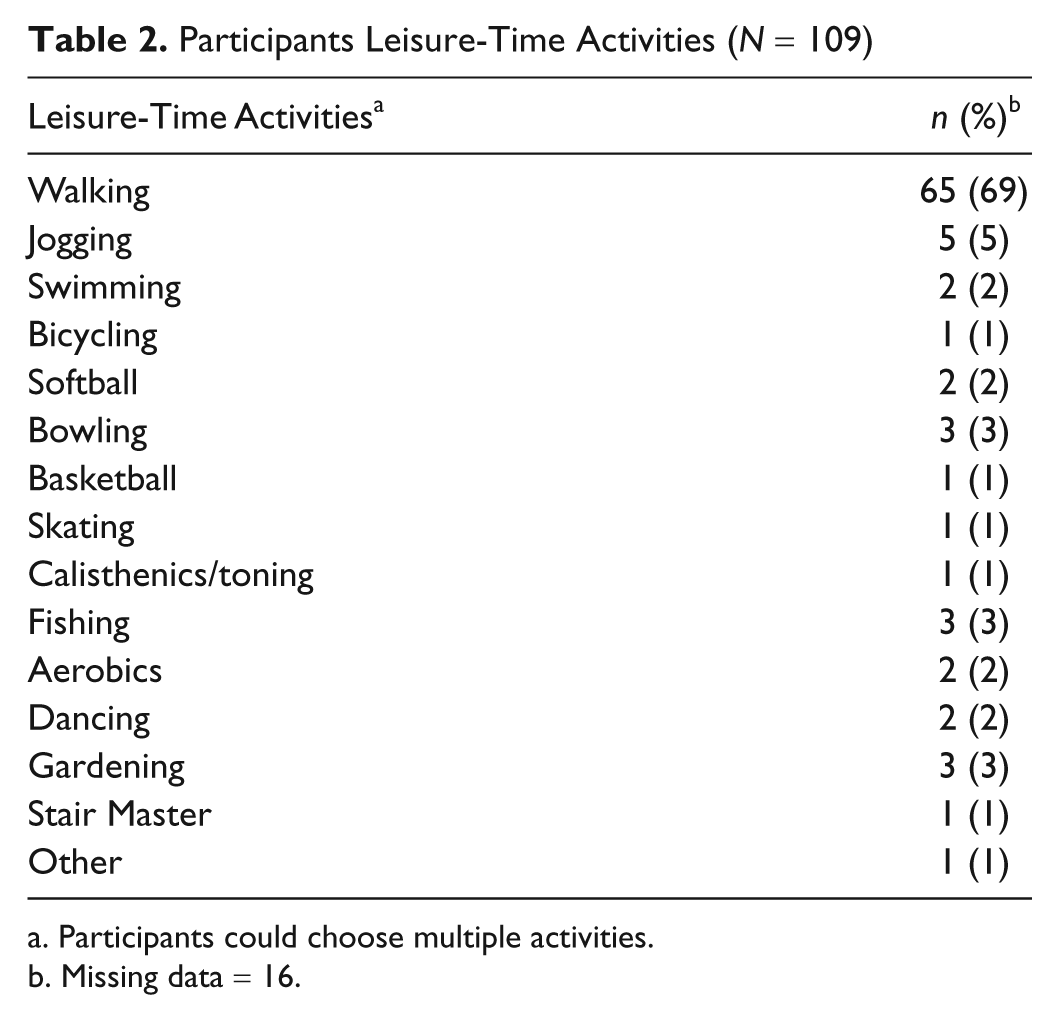
Participants could choose multiple activities.
Missing data = 16.
Relationships Between Physiological, Psychological, and Behavioral Factors
Correlations were explored among the following baseline variables: HbA1c, total cholesterol, triglycerides, LDL, HDL, systolic BP, diastolic BP, waist circumference, BMI, vitality, physical function, somatic anxiety, diabetes mellitus emotional distress, and health care provider exercise support (Table 3). HbA1c was positively associated with diabetes emotional distress (r = .22, p = .02) and inversely associated with HDL cholesterol (r = −.25, p = .01). Waist circumference was inversely associated with vitality (r = −.23, p = .02) and bodily pain (r = −.25, p = .01). Physical function was positively associated with vitality (r = −.58, p < .001) and bodily pain (r = .58, p < .001) and negatively associated with somatic anxiety (r = −.39, p < .001) and emotional distress (r = −.50, p < .001). Vitality was negatively associated with bodily pain (r = −.64, p < .001) and somatic anxiety (r = −.56, p < .001). Bodily pain was negatively associated with somatic anxiety (r = −.43, p < .001). Last, health care provider support for exercise was associated with vitality (r = .19, p = .04) and inversely associated with emotional distress (r = −.26, p = .01).
Correlations Among Physiological, Psychological, and Behavioral Variables (N = 109)
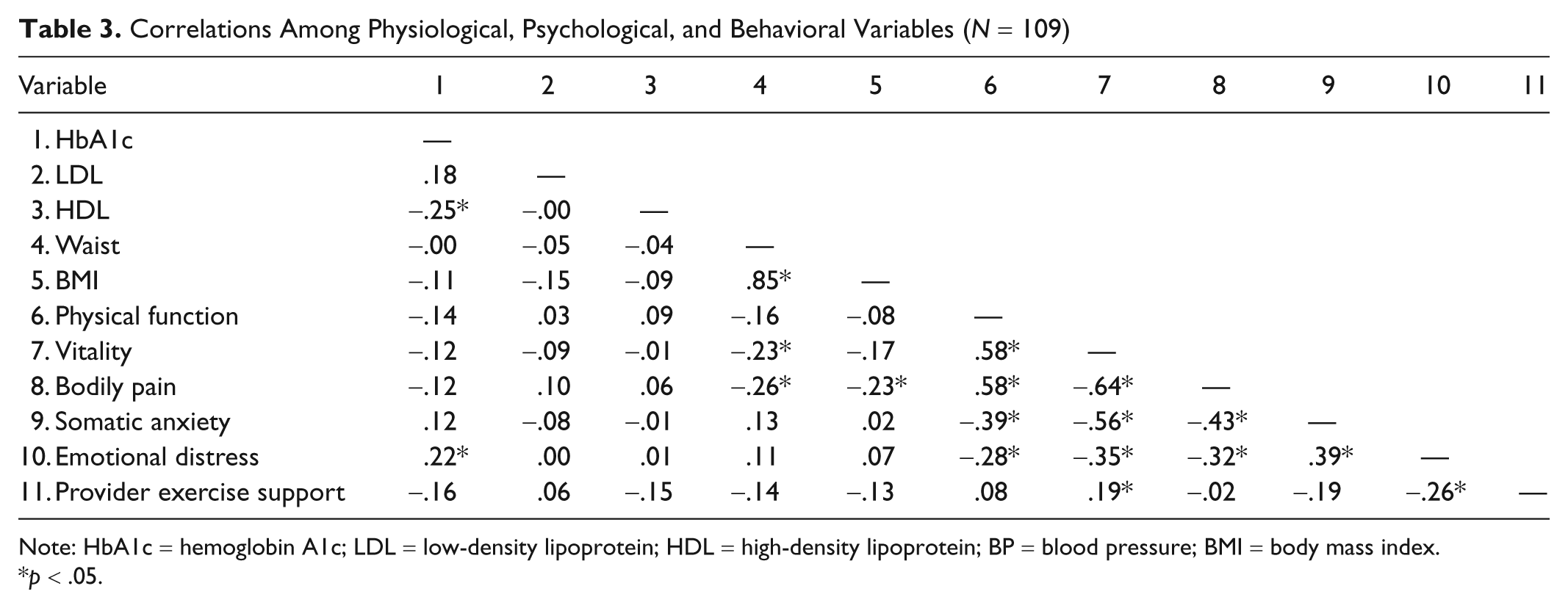
Note: HbA1c = hemoglobin A1c; LDL = low-density lipoprotein; HDL = high-density lipoprotein; BP = blood pressure; BMI = body mass index.
p < .05.
Factors Associated With Inactivity
Women who were active (n = 93) and inactive (n = 16) were compared on physiological, psychological, and behavioral variables (Table 4). Inactive women had greater BMI (t = 2.58, p = .01), waist circumference (t = 3.25, p = .00), lower total bodily pain (t = −2.39, p = .02), and lower vitality (t = −2.35, p = .02) than active women. Active and inactive women did not differ significantly in HbA1c, systolic BP, diastolic BP, LDL, or HDL cholesterol.
Inactivity Factors Associated With Physiological, Psychological, and Behavioral Factors
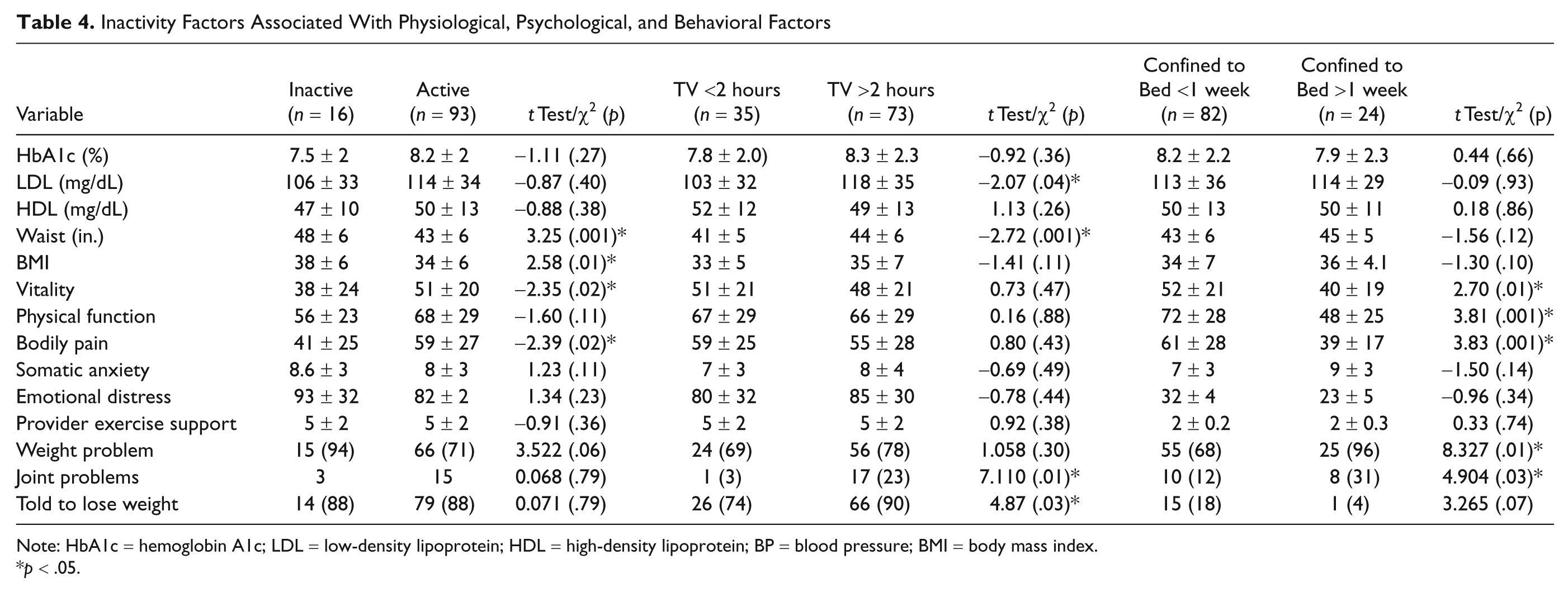
Note: HbA1c = hemoglobin A1c; LDL = low-density lipoprotein; HDL = high-density lipoprotein; BP = blood pressure; BMI = body mass index.
p < .05.
The same physiological, psychological, and behavioral variables were used to compare participants who watched TV <2 hours/day (n = 35) with those who watched ≥2 hours/day (n = 73; Table 3). Women watching TV ≥2 hours/day had significantly higher LDL levels (t = −2.07, p = .04) and waist circumference (t = −2.72, p = .00) than those who watched TV <2 hours/day. Women watching TV ≥2 hours/day and <2 hours/day differed significantly in only two of the self-reported diabetes mellitus and weight-related health history problems. Joint problems related to weight was reported significantly more in woman watching TV ≥2 hours/day than those watching TV <2 hours/day (χ2 = 7.110; p = .01). Similarly, women who watched TV ≥2 hours/day were significantly more likely to be told by their health care provider to lose weight than women watching TV <2 hours/day (χ2 = 4.87, p = .03).
Women confined to bed >1 week (n = 26) in the last year were compared with those who had not been confined to bed for >1 week in the last year (Table 4). Women who reported being confined to bed had significantly lower QOL scores on the physical function (t = 3.81, p = .00), vitality (t = 2.70, p = .00), and bodily pain (t = 3.83, p = .00) subscales than women who reported no confinement to bed. Additionally, among the women reporting >1 week of confinement to bed in the last year, 40% had no leisure-time activity (were inactive), whereas only 22% of those were participating in some type of leisure-time activity. This difference was not statistically significant (p = .11). Women with joint problems related to their weight were significantly more likely to report confinement to bed (31%) for more than a week in the last year than those not confined to bed (p = .07). Of the self-reported diabetes mellitus and weight-related complications, two factors were significantly different. Women reporting >1 week of confinement to bed in the last year were more likely to be told that their weight was a problem by their health care provider (χ2 = 4.87, p = .03) and to have joint pain (χ2 = 7.110, p = .01) than women reporting <1 week of confinement to bed in the last year.
Discussion
Black women with T2DM enrolled in this study were sedentary and overweight/obese, with low QOL scores on vitality, physical function, bodily pain, and high levels of diabetes mellitus-related emotional distress and somatic anxiety. Health care provider support for physical activity was positively associated with vitality and inversely associated with diabetes mellitus–related emotional distress. Moreover, diabetes mellitus–related distress was associated with metabolic control. These psychological, behavioral, and physiological variables and their relationship to inactivity are important for understanding the complexity of issues that need to be addressed in changing physical activity behavior in Black women with T2DM.
Inactivity was examined from three different perspectives: (a) reports of preferred leisure-time activity, (b) time spent viewing TV, and (c) time confined to bed in the last year. The majority of Black women with T2DM in this study preferred walking for leisure-time activity, consistent with previous reports (Sharpe et al., 2008). Inactive women had significantly greater waist circumferences, BMI, and bodily pain than active women. Moreover, 17% of all participants reported problems with joint pain. This relationship of overweight/obesity and bodily pain was also found in the NHANES III (Nelson, Reiber, & Boyko, 2002) and may be related to the prevalence of mobility limitations in adults with diabetes mellitus. For example, 59% of adults with diabetes mellitus in 2003 had a mobility limitation such as walking a quarter of a mile (34%), climbing 10 steps (29%), standing for 2 hours (36%), and/or stooping, bending, or kneeling (41%; CDC, 2004). The highest prevalence (56%) of mobility limitations, among all race/ethnicity and gender groups studied, was found in Black women (CDC, 2004). These mobility issues may be related to diabetes mellitus–associated comorbidities such as obesity, depression, blindness, peripheral neuropathy, peripheral arterial disease, visual impairments, and cardiovascular diseases (Volpato et al., 2002). Furthermore, obesity and knee osteoarthritis increase the likelihood of walking limitations and can contribute to decreases in leisure-time physical activity (Stenholm, Sainio, Rantanen, Alanen, & Koskinen, 2007). More research is needed to explore the specific causes of mobility issues in Black women with diabetes mellitus.
Time spent viewing television has been shown to detract from engaging in leisure-time physical activity such as walking (Bennett, Wolin, Askew, Puleo, & Emmons, 2006). The women in our study watched TV on average 3.50 hours/day, similar to a recent report that women of all ethnicity viewed TV on average 3.3 hours/day and Black individuals (both men and women) had the highest rates of television viewing (4.1 hours/day) among all multiethnic groups studied (Bennett et al., 2006). Other data show that in 2007 women averaged watching television 2.25 hours/day on weekdays and 2.69 hours/day on weekends, with Black or African Americans (all ages) watching more TV (weekday 3.11 hours/day; 3.62 hours/day weekend) than Whites (weekday 2.37 hours/day; weekend 3.02 hours/day) or Hispanics/Latinos (weekdays 2.52 hours/day; weekends 2.94 hours/day; Bureau of Labor Statistics, n.d.). Television viewing has been shown to decrease physical activity levels by approximately 520 pedometer-measured steps/day, and every hour of television viewing/day decreases by 16% the likelihood of meeting the 10,000 steps/day threshold (Bennett et al., 2006). Thus, time spent viewing television is an important variable to consider when designing physical activity interventions in Black women with T2DM.
We found that women who watched television ≥2 hours/day differed significantly from those who watched <2 hours/day in terms of being told to lose weight, having joint problems, LDL, and waist circumference. These findings echo reports that television viewing time is associated with many negative health markers such as obesity (Jakes et al., 2003), lower muscle/knee strength, cardiorespiratory fitness (Duvigneaud et al., 2008), and cardiovascular risk factors (Jakes et al., 2003). All these variables are markers of cardiovascular disease in individuals with diabetes mellitus.
An unexpected finding of our study was that 24% of women reported confinement to bed within the previous year. Moreover, 40% of inactive women versus 22% of active women reported confinement to bed in the last year, although the proportions were not significantly different. This finding could not be compared with the literature, as no comparable studies were found. The high levels of bed rest found in our study could be due to several diabetes mellitus–related comorbidities. For example, extreme bed rest has been associated with increased insulin resistance in muscle and liver (Blanc et al., 2000), and sedentary behavior in the form of bed rest might reduce glucose disposal via skeletal muscle. To verify this high percentage of Black women reporting confinement to bed, further research is needed to determine the nature of confinement to bed and to identify its physiological effect on glucose levels and insulin resistance.
Quality of life scores in this study were lower than U.S. norms and for those with T2DM (Ware, Snow, Kosinski, & Gandek, 1997). Of particular interest is that QOL scores on the bodily pain and vitality subscales were significantly lower for women reporting no leisure-time physical activity than women who were active. Similarly, women reporting >1 week confinement to bed within the last year had significantly lower QOL scores on bodily pain, vitality, and physical function than women not confined to bed within the last year. Lower QOL has been associated with several chronic health conditions such as congestive heart failure, hypertension, macrovascular or microvascular complications, hyperglycemia, depression, psychological perceptions of diabetes mellitus, poor social support, coping style, insulin use, increasing age, osteoarthritis, female gender, and lower education (Kleefstra et al., 2005; Wexler et al., 2006).
In this study, vitality and bodily pain were associated with waist circumference and BMI, similar to results from a study of 5,145 overweight and obese adults with T2DM (Rejeski et al., 2006). Most interestingly, greater BMI was related in that study to lower physical capacity scores, for example, vitality and total bodily pain, in individuals with lower metabolic equivalent capacities, an objective measure, but this relationship was absent for individuals with higher metabolic equivalent capacities (Rejeski et al., 2006). It is unknown whether physical activity in our study participants was limited by bodily pain and poor vitality or if these QOL measures were affected by comorbidities related to obesity and T2DM. However, 17% of our participants reported joint problems, and of those, 31% reported confinement to bed >1 week in the last year and 23% reported watching TV >2 hours/day.
The effects of low vitality in this population might be buffered by support from health care providers. We found that women’s vitality was positively correlated with health care provider support. Similarly, patient provider support was found by structural equation modeling (Maddigan, Majumdar, & Johnson, 2005) to have a direct impact on exercise adherence, which directly influenced QOL. Thus, health care providers have considerable potential to help these women by offering specific support to safely engage in physical activity that may in turn improve vitality and decrease total bodily pain from obesity or other diabetes mellitus–related comorbidities.
Our study sample had much higher levels of diabetes mellitus–related emotional distress (84 ± 31) than reported in comparable studies using the PAID survey in women with diabetes mellitus (18.6-51.6; Whittemore, D’Eramo Melkus, & Grey, 2005) and in African Americans (15.59 ± 1.78; Spencer et al., 2006). We also found that diabetes mellitus–related emotional distress was positively related to HbA1c, in contrast to some studies in African American populations (Miller & Elasy, 2008; Spencer et al., 2006), but consistent with other studies in women (Whittemore et al., 2005) and Caucasian populations (Polonsky et al., 1995). These mixed results might be explained by the women in our study being not only of African American descent but also Caribbean and Cape Verdean. Despite the high levels of diabetes-related emotional distress found in this study, the inverse relationship between emotional distress and health care provider support was encouraging. Providers need to be aware of the psychological stress associated with diabetes mellitus and the need for interventions to minimize this stress, possibly leading to improvements in metabolic control.
The women in our study had a moderate amount of anxiety that was positively associated with physical function and bodily pain. Individuals with diabetes mellitus have a 20% overall age-adjusted prevalence of a lifetime diagnosis of anxiety compared with an 11% prevalence in people without diabetes mellitus (Li et al., 2008). Furthermore, women with diabetes mellitus have a higher prevalence of anxiety (25%) than men with diabetes mellitus (15%; Li et al., 2008). However, anxiety has been shown to be decreased by physical activity/exercise, which also improves physical function and decreases bodily pain (Physical Activity Guidelines Advisory Committee, 2008). However, few physical activity interventions are effective for Black women with T2DM, and recent research suggests that physical activity interventions must be specifically tailored to be effective in this population (Whitt & Kumanyika, 2002).
Limitations
Our findings, although informative, must be interpreted in light of some limitations. First, the study design was cross-sectional, precluding determination of the directionality of relationships between inactivity/activity and other variables such as emotional distress and anxiety. For example, emotional distress could lead to inactivity, or conversely, inactivity could lead to emotional distress. Moreover, the relationship could be bidirectional, or inactivity might be caused by a common antecedent that was not examined. Second, activity/inactivity was not measured objectively, and subjective measures are affected by recall bias. Third, participants had difficulty completing the MAQ, and therefore, we were unable to quantify the time, intensity, and duration of participants’ physical activity. Last, the sample size was small, increasing the risk that important relationships may have been missed and limiting our ability to conduct a multivariate analysis.
Conclusion
In conclusion, these results indicate that physical activity in Black women with T2DM was associated with TV viewing time and confinement to bed. Since the majority of these women preferred walking as their physical activity, interventions should promote walking and address TV viewing time. Moreover, interventions should incorporate health care provider support for physical activity and counseling that addresses bodily pain, vitality, emotional distress, and anxiety. In addition to physiological outcomes, anxiety, emotional distress, vitality, and physical function are important behavioral factors to account for in developing, implementing, and evaluating physical activity interventions in Black women with T2DM.
Footnotes
Acknowledgements
We would like to acknowledge Vanessa Jefferson, MSN, FNP, and Susan Langerman, MSN, FNP, for their contributions in recruiting participants and data collection.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article:
National Institute of Health Grant R01NR05341 and T32 NR 008346-06.