
Abstract
Introduction
If trends do not change, demographic predictions indicate that the Spanish population will age and that, by 2050, 30% of the population will be older than 65 years, the highest rate in the world (Population Reference Bureau, 2009). An aging population implies a considerable number of people requiring care (Durán-Heras & García-Díez, 2005; Julia, 2003) and, in a welfare state, it is the government’s responsibility to ensure the quality of that care (Consejo de Europa, 1998). However, in Spain, only 5% of the population received home help provided by the Social Services in 2005 (Durán-Heras & García Díez, 2005; Spanish Institute of the Elderly and Social Services [IMSERSO], 2005), and as there are no planned services for dependency (Ministerio de Trabajo y Asuntos Sociales [MTAS], 2004), the responsibility for care and support of the elderly falls on the family (Plá-Julián et al., 2004).
At present, Spanish society continues to regard the care of ill relatives as the family’s legal and moral obligation, and it is the family that continues to assume the greater part of this care (IMSERSO, 2005). Thus, it is estimated that 86% of the elderly are cared for in their homes by their families (IMSERSO, 2005). However, the new social and family structures emerging in Spain do not facilitate informal social support systems, and many families are unable to care for their elderly relatives (Plá-Julián et al., 2004).
When the families find themselves unable to provide care they seek assistance in the job market, transferring caregiving duties to people who are unconnected with the family circle (Gallart Fernández-Puebla, 2004; Plá-Julián et al., 2004). Thus, a gradual shift from family caregiving to paid caregiving is taking place, and a new understanding of caregiving is emerging. In this context, women immigrants create a new caregiving structure in developed countries, as they are increasingly providing care for the elderly (Navarro, 2002). In Spain, this group now constitutes 43% of paid caregivers (Gallart Fernández-Puebla, 2007).
Indeed, since the mid-1980s, Spain has become a host country for immigrants and has witnessed an increase in the flow of female economic immigrants, mostly of Latin American origin (Vicente & Setién, 2005), who are attracted by employment opportunities in the domestic and caring sector and the common language (Catarino & Oso, 2000; Parella-Rubio, 2003). From the employer’s point of view, Latin American female workers are preferred over other immigrants because of stereotyped traits such as being patient and affectionate, which are highly sought-after qualities in caregivers for the dependent elderly (Colectivo Ioé, 1999; Parella-Rubio, 2003). They are also perceived to be docile and pleasant. Paradoxically, such stereotypes also have a negative effect on these workers as they may be consequently regarded as slower and less productive (Parella-Rubio, 2003).In 2001, Spain received 24% of all immigrants arriving in the European Union, the highest rate in this zone (Vicente & Setién, 2005). This immigration process is linked to a growing demand for foreign domestic workers to fill the void left by native Spanish women within the domestic service and caregiving sector (Catarino & Oso, 2000; Parella-Rubio, 2003). Consequently, 7 out of 10 work permits were requested for domestic work (Vicente & Setién, 2005). However, Spain has a long tradition of undocumented immigration as the restrictions imposed by the Spanish Immigration Law enacted in 1986 (Ley de Extranjería) has meant that “from then on, migration to Spain was predominantly undocumented” (Anderson, 2000, p. 57).
Nowadays, a significant number of immigrants working in domestic services are illegal, suffering poor labor conditions and living on the fringes of the regularized labor market (Vicente & Setién, 2005). Their irregular situation and the need for money to send back to their families force these immigrants to accept exploitative conditions (Parella-Rubio, 2003). A study conducted in Madrid found that the working conditions of these women were inadequate because of long hours, isolation, low pay, and paternalistic employee–employer relations (Colectivo Ioé, 1999). These women have clearly migrated for economic reasons and the very survival of their families often depends on their wages (Parella-Rubio, 2003; Vicente & Setién, 2005). They are recruited via their own migration networks and intermediary agencies in Spain (Parella-Rubio, 2003).
Live-in domestic service is increasing in demand but native Spanish women are unwilling to accept it. On their arrival, immigrant women readily accept this form of employment as it offers certain advantages for them, including accommodation and a promise from their employer to regularize their legal status (Parella-Rubio, 2003). However, live-in conditions tend to be exploitative and once regularized they do not necessarily improve. Current Spanish regulation for domestic work merely establishes minimum requirements, largely leaving the employer to define labor relations as he sees fit. Hence, immigrant women must adhere to the hours and demands set by their employer (Parella-Rubio, 2003).
Thus, immigrant caregivers usually work as live-in caregivers, spending 24 hours a day with the dependent person (Berjano, Simó, & Ariño, 2005a). Although initially employed as caregivers, it is also common for these women to eventually become tacitly responsible for domestic work, as their employers endeavor to resolve all domestic chores for a little more money (Berjano et al., 2005a; Gallart Fernández-Puebla, 2007). The higher the level of dependency, the harder these women work, frequently suffering from stress and the burden of care (Gallart Fernández-Puebla, 2007), which is understood as the negative impact of caregiving on the caregiver’s health. As live-in caregivers, these women have little chance of building social relationships beyond their caregiving environment. Thus, the absence of social networks, among other factors, adds to their burden of care (Gallart Fernández-Puebla, 2007).
Furthermore, immigrants are living in a place to which they do not belong and are in the process of adapting to a reality that is completely new to them. The migratory process often entails sacrificing significant emotional ties, such as those with family and friends (Plá-Julián et al., 2004). Adapting to the host country and a new social environment implies further losses in terms of national identity (Plaza del Pino, Plaza del Pino, & Martínez-Gálvez, 2005) and social class (Salazar-Parreñas, 2001). This adjustment, known as acculturation, can be stressful (Negy, Schwartz, & Reig-Ferrer, 2009) and has a negative effect on health (Lassetter & Callister, 2009).
Previous studies on the cultural differences in caregiving have reported mixed and inconsistent findings regarding the burden of care (Janevic & Connell, 2001; Montoro-Rodríguez & Gallagher-Thompson, 2009). On one hand, a review of published research suggested that minority groups, including Latin Americans, may not have more available support than whites (Janevic & Connell, 2001). On the other hand, in a recent study, female Latin American caregivers reported lower levels of burden than non-Hispanic White caregivers as well as higher levels of emotion-focused coping mechanisms (Montoro-Rodríguez & Gallagher-Thompson, 2009). Regarding paid immigrant caregivers, a study in Spain found that they have a similar burden to family caregivers and that the level varies according to contextual factors such as the support they receive from social networks, the level of dependency of the person cared for, and the working conditions (Gallart Fernández-Puebla, 2007).
Frequently, the immigrants are not recognized as caregivers, but are referred to as domestic workers or as informal family support (IMSERSO, 2005; Plà-Juliàn et al., 2004). Although they classify themselves as the “primary caregivers” (IMSERSO, 2005), they are considered as help and respite for other caregivers (IMSERSO, 2005). Consequently, their need for rest is not fully recognized. In terms of the burden of care, immigrant caregivers are even more vulnerable than family caregivers (Gallart Fernández-Puebla, 2007, Plá-Julián et al., 2004). They are present but unseen. One feature of the invisibility of these workers is the scarcity of studies on caregiving by immigrant women (Gallart Fernández-Puebla, 2007, Plá-Julián et al., 2004).
In contrast, research studies in recent years have paid much attention to the mechanisms employed by family caregivers in order to cope with the demands of caregiving, and have reported on a variety of cognitive, problem solving, and stress reduction techniques, such as keeping some time aside for oneself, seeking distractions, or maintaining interests that are unrelated to caregiving (Ekwall, Sivberg, & Hallberg, 2007; Grant & Whittell, 2003; Nolan, Grant, & Keady, 1996; Salin, Kaunomen, & Astedt-Kurki, 2009). However, the means employed by immigrant women to cope with the burden of care remains unknown.
This article presents the category “turning to one’s own world,” which emerged during a study whose aim was to identify the strategies employed by immigrant caregivers to relieve the burden of care. This forms part of a wider project concerning relief from the burden of care among those in vulnerable situations (de la Cuesta-Benjumea et al., 2006).
Method
This is a qualitative research study conducted in Alicante and Elche (Spain). A total of 17 immigrant women participated, all of whom provided home care to extremely dependent people for more than 5 hours a day (Table 1). A combination of purposive and snowball sampling (Morse, 1989) was used to identify those immigrant caregivers with the widest and richest experience of home-based caregiving.
Demographic Characteristics of Participants (N = 17)
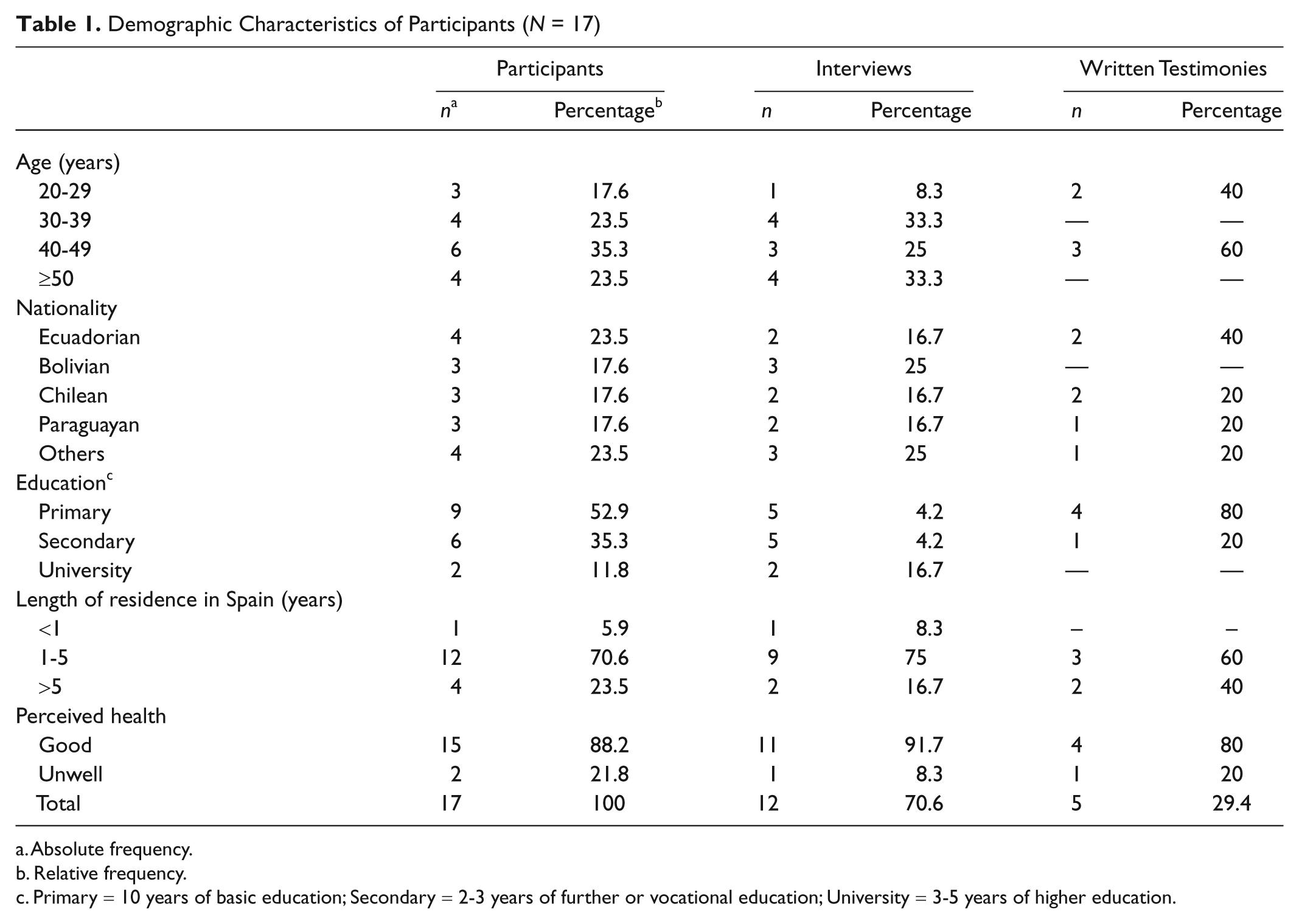
Absolute frequency.
Relative frequency.
Primary = 10 years of basic education; Secondary = 2-3 years of further or vocational education; University = 3-5 years of higher education.
Access to participants was obtained through nongovernmental immigrant organizations and health service personnel from various health centers. The study was approved by the University of Alicante Ethics Committee. All participation was voluntary and fully informed. To preserve anonymity, pseudonyms are used in the text below.
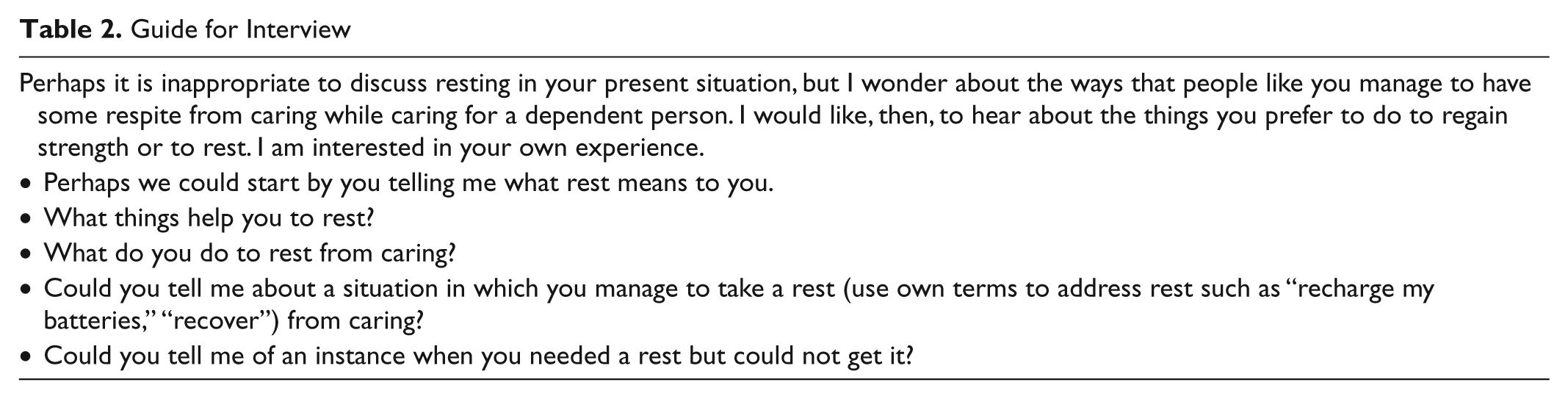
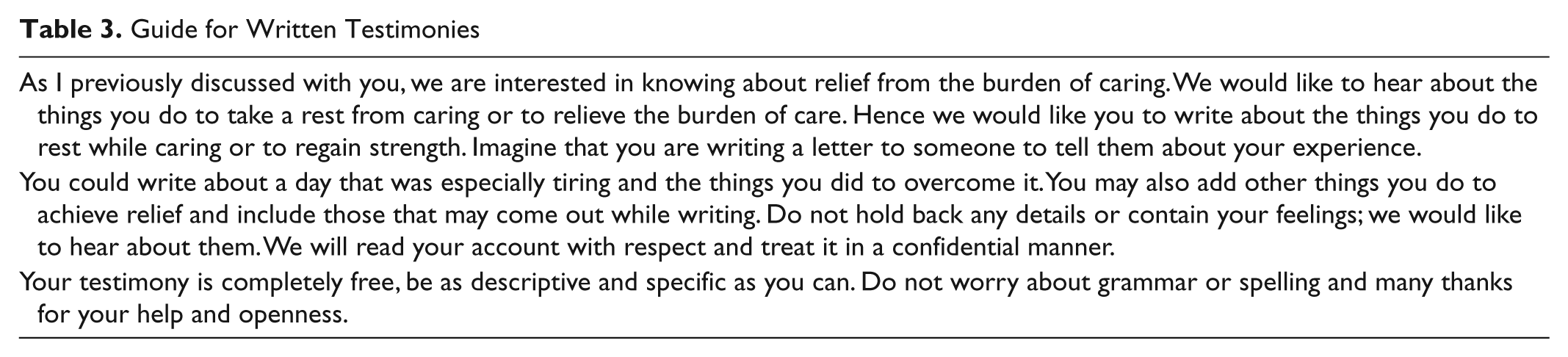
Data were obtained between November 2006 and May 2008. Participants were invited to be interviewed and to write a testimony as a means to enrich data. Knowing that some participants could be reluctant to speak in an interview because of their illegal status, written testimony was offered as an alternative. Participants either chose the interview or the written testimony (see Table 1). In total, 12 semistructured interviews were conducted and 5 written testimonies collected. The interviews lasted from 45 to 60 minutes, and were recorded and transcribed in their entirety. Most of the interviews took place in the caregiver’s place of work. Interviews were conducted as a guided conversation. The meaning of rest, the conditions under which participants achieve it, and the strategies they use to seek relief were all discussed (Table 2). The written testimonies were requested as a strategy to enrich data due to the reflective nature of writing. Participants were told the aim of the testimony and had the chance to clarify their doubts with researchers. We provided the writing materials to produce the testimony and a guide to elaborate it (Table 3).
Guide for Interview
Guide for Written Testimonies
We carried out the analysis concurrently with data collection, using grounded theory procedures (Strauss & Corbin, 1998). We used open coding to identify codes indicating the participants’ rest strategies. Then, through a process of constant comparison and axial coding, we assembled the codes into the turning to one’s own world category, which is divided into four subcategories: (1) virtual outings, (2) going to a private place, (3) making those they care for their own, and (4) deciding to go home. We drafted memos and consulted the literature to aid conceptualization and to guide theoretical sampling (Strauss & Corbin, 1998).
The category presented here emerged from the data, and it was saturated and validated with the study participants during field work. This research, therefore, adheres to the validity canons of grounded theory (Strauss & Corbin, 1998).
Results
Turning to one’s own world describes a means of seeking relief from the burden of care that immigrant caregivers shoulder. This type of rest is bound to the status of being an immigrant, that is to say, of living in a foreign country far from family and severed from one’s own world.
For immigrant caregivers, caring is both their primary source of income and the means by which they maintain their families’ economic well-being. During the interviews, they described how they had left their families, friends, and children behind in their country of origin, as to emigrate with them would have implied enormous legal difficulties and an obstacle to securing work as a caregiver, an occupation that requires total availability in terms of working hours and is sometimes precarious. These caregivers reported having given up everything, even their time, as one caregiver states,
El día que fui contratada, perdí mi ritmo de vida para adquirir otro, el de mis patronos. (The day I was employed, I lost my own pace of life in order to acquire another, that of my employers.)
1
There is no rest from caregiving for immigrant caregivers, despite the burden it represents for them. Consequently, they seek alternatives that provide a respite, a pause that enables them to endure the arduous task of caregiving. Data analysis showed that caregivers turn to their own world by (1) virtual outings, (2) going to a space of their own, (3) making those they care for their own, and (4) deciding to go home. These alternatives function as escape mechanisms from the world of caregiving in which they find themselves, and each is described more fully below.
Virtual Outings
Thanks to telecommunication technologies that cross boundaries, caregivers can reach out to their countries, families, and friends. They are transported over the telephone line from their present location to their place of origin and are momentarily no longer immigrants. As a result, their energy levels are replenished, as one caregiver affirmed when asked what she did to rest: “salgo a llamar a Bolivia, a la semana dos o tres veces” (I go out to make a call to Bolivia, two or three times a week).
The locutorio is a place where immigrants can make calls using public telephones and contact their families over the Internet. Here caregivers reach out virtually to their families and children, attempting to maintain a dialogue and a maternal relationship with the latter: “At least, I would get out to talk on the phone with my son” said Paula. By communicating with their families, these immigrants temporarily forget all the sacrifices that being far away involves. Their aim is to achieve a brief respite, to stay alive, and to be able to carry on. As one participant said,
Hablar telefónicamente con mi marido, con mis hijos, así ya vengo contenta . . . de esa forma es como yo hago para respirar un poco, verdad, y mantenerme viva para seguir adelante. (Talking on the phone with my husband, with my children, that’s when I come back happy . . . This is what I do to give myself a breathing space, right, and keep myself alive in order to carry on.)
During this contact with their family, the participants experience respite from their absence. For a moment, the family is close; briefly they are present in each other’s lives. Thus, talking with them, they feel and receive their family’s affection across the miles as if nothing had changed, and this gives them strength:
Me encanta hablar con ellos, con mi nena especialmente, que ella habla ahora y que ella me dice cosas, entonces ya para mi es algo que me dice “hola mami, te quiero mucho”, ya es muchísimo, ya para mi, entonces . . . bueno, eso me da fuerzas. (I love speaking with them, especially with my little girl, who talks now and tells me things. It means so much to me that she says “hello mommy, I love you a lot,” it means so very much, and so for me . . . well, it gives me strength.)
This form of escapism enables these women to continue being mothers at a distance, so they achieve rest by being able to care for their children:
Hago una escapada y me voy a hablarles por teléfono, que, cómo están, que si rindió . . . estoy pendiente también de que tal rindió, si pasó los exámenes. (I slip out to speak to them on the phone, find out how they are, and how they’re getting on . . . I’m waiting to see how one got on in their exams.)
Circumstances do not always permit a visit to the locutorio, and so sometimes caregivers conjure up the family’s presence in their thoughts, which also helps them rest:
A mi, lo que me ayuda a descansar . . . pensar en mis hijos, si me echan de menos, si les falta algo, si comen o no comen, si están enfermos. (What helps me to rest . . . is thinking about my children, whether they miss me, whether they need anything, if they are eating or not, if they are unwell.)
Caregivers are reunited with their families during these mental escapes, remembering them, speaking to them, and feeling their presence. Although separated by thousands of miles, the family is present in the caregivers’ thoughts, as a virtual presence which they can easily visit at any time by simply thinking about them.
Going to a Private Place
Caregivers have parallel homes and spaces of their own in which to rest. On their days off, they go back to the flats they share with other immigrants or to the homes of relatives or friends. They take a break, seeking closeness and actual physical contact with their own world, with what is truly theirs as Esther said, “Cuando yo voy es a despejar la mente, a dormir en la casa de mis hijos” (When I leave, it’s to clear my head, to sleep in my children’s house).
The prospect of an encounter with what is truly theirs is something caregivers look forward to. From the moment they make such a decision, the way they perceive their situation changes and their anticipation makes the same place and atmosphere feel different:
Cuando yo iba caminando, para tomar el autobús, eh, para traerme acá (a su casa), yo ¡uy!, ya respirando de otra manera, el mismo aire de ir y volver, pero respirando de otra manera. (When I was walking to catch the bus, to bring me here (to her house), I, well, I breathed differently, the same air going in and out, but I was breathing differently.)
In their private place, caregivers feel that they regain some of the things they have sacrificed, and are once again in control of their own time. In their own homes, it is they who decide what they want to do and when, they are not accountable to anyone, and no one is going to bother them. Here they achieve what a participant defined as real rest:
No, descanso real lo he tenido ahora aquí, que volví a estar en mi casa. Eh, que si, que las niñas están estudiando y que yo, hay un momento en que quiero asear, hago limpieza. Aquí nadie nos molesta, me canso, me voy a recostar a la cama. (No, a real rest is what I’ve just had here, now, when I came back home. Uh, yes, the girls are studying and me, there comes a moment when I want to clear up, and I clean. Here, nobody bothers us, if I get tired, I go and lie down on the bed.)
The participants also seek a space of their own without leaving their place of work. They go to their bedroom; to the space that one way or other they feel is theirs and have made their own. In these little areas of the house, they manage to separate themselves from their caregiving duties. There the caregiver can clear her head, relax, and switch off to later return once more to the caregiving tasks:
Me voy y me acuesto un rato en mi dormitorio, en mi cama, o veo un poco la tele, ya ahí me espabilo un poco ¡estoy desconectada! . . . y ya luego me levanto, y empiezo otra vez. (I go and lie down for a while in my bedroom, on my bed, or I watch a bit of TV, and I perk up a little because I’ve disconnected . . . then I get up and start again.)
Making Those They Care for Their Own
Some participants in the study, faced with the impossibility of actually being with their real family, convert their workplace into new homes and families who they can be with and rest. Thus, the people they care for become their family, their grandparents, parents or children, and they in turn become a member of the family:
Me ayuda (a sobrellevar el peso) a una cosa, que no sé, que es que esta familia me trata como si fuera su hija y que yo les trato como si fueran mis abuelos y que nos entendemos mejor y muy bien, que no es una cosa como si fuera una familia que ha contratado una cuidadora, y yo soy una cuidadora y ellos mis jefes, nosotros estamos como si fuéramos una familia. (One thing that helps me (to cope with the burden), I don’t know, is that this family treats me like a daughter and I treat them as if they were my grandparents, and we understand each other better, very well. It’s not like a family that’s employed a caregiver, where I’m a caregiver and they’re my bosses, it’s as if we were a family.)
It could be said that immigrant caregivers cling to those around them in order to achieve rest and the strength to help them carry on. As one participant expressed,
Yo estaba ahí con Felipe la hora y la hora se me pasaba rápido . . . aferrándome a él, yo salí adelante . . . con Felipe hablaba de todo…él era mi apoyo, como yo no salía, no le veía nadie, no conocía a gente ni nada, él era como un padre para mí. (I would be there with Felipe for an hour, and the hour flew by . . . depending on him for support, I was able to carry on . . . I talked about everything with Felipe . . . he was my source of support, as I didn’t go out, I didn’t see anyone, I didn’t know anyone or anything, he was like a father for me.)
Consequently, caregivers achieve a respite which enables them to continue caregiving. The family ties they create are solid, and it is not unusual for caregivers to spend their free time with the people they provide care for, and even to go back to visit them once they have left their job, just as they would do with their own family. Nevertheless, the families and homes where they work are substitutes, and so at times they do not achieve the same level of rest, as pointed out in the interviews:
Eh, fui a ser dueña de casa de otra casa pero que no era mi casa y atendiendo a otra persona, entonces, eh, eh, que si, si se descansa, ¡si!, No te puedo decir que no, pero se descansa de una manera diferente a como nuestro descanso en nuestro hogar. Sin trabajar, o trabajando, pero llegar a descansar. ¡Es diferente el descanso! (Uh, I went to be housekeeper at another house but which wasn’t my house and attending to another person, well, um, yes, yes, you rest, yes. I can’t say you don’t, but you don’t rest in the same way as you do in your own home.)
Even so, taking those they care for as their own genuinely helps immigrant caregivers to achieve moments of rest, which would not be possible without this emotional bond. Without leaving their workplace, they “turn to their own world” simply by considering the people they care for as their own family.
Deciding to Go Home
When none of the previous strategies proves to be effective, it becomes necessary for the caregiver to see her friends and family again in the flesh, in the real physical world, in order to regain strength and to rest. They decide to return and be reunited with their family and friends, with those who they had left behind to go to Spain, as Gloria put it, “Pues sólo me ponía a llorar y decidí . . . y me fui (a su país) por un mes.” (I couldn’t stop crying so I decided . . . and went [to her country] for a month).
Over time, exhaustion from caregiving increases, and immigrant caregivers need to physically touch the reality that they dream about constantly. Virtual encounters, rekindled memories, and substitute families no longer sustain them; they lack energy and decide to return to their country in search of what is theirs, of everything that they miss so much:
Me hacía falta ver a mi familia . . . comprobar por mis propios ojos . . . para darme cuenta que, lo que ya había escuchado por teléfono no era mentira. (I needed to see my family . . . to see with my own eyes . . . to see that what I had heard on the telephone wasn’t a lie.)
The idea of returning to familiarity, returning to “that which is one’s own”, provides the strength necessary to continue working in a country which is “not one’s own”, as the above participant explained during the interview. Caregivers immediately feel relief from the burden of care; the mere idea of returning provides them with relief.
Discussion
In recent years, an increasing number of people are being employed in Spanish homes to provide care for the elderly, and have become an important resource for families in need of care for their dependents. A significant number of these workers are immigrants (Berjano, Simó, & Ariño, 2005b) who do not have real access to the support systems usually available to family caregivers, and are considered as simply providing a form of rest for others. Those who work on a live-in basis suffer loneliness and social isolation, and miss their family and friends, which can lead to psychosomatic illness (Jiménez-Blasco & Redondo-González, 2007). Most of the women caregivers are mothers and consequently worry about their children, left behind in their countries of origin to be cared for by relatives. This concern is added to the daily burden of care that they suffer (Rodríguez, 2007).
Previous studies have revealed the negative effects that immigration has on health: a general deterioration, the presence of coronary disease, altered blood pressure, and depression (Lassetter & Callister, 2009). The well-being of groups with strong collectivist values, such as Latin Americans, is particularly affected by the lack of social support (Phillips & Crist, 2008). To the vulnerability of being a caregiver is added the fact of being an immigrant, which puts these women in an extremely vulnerable situation (IMSERSO, 2005).
This study found that “turning to one’s own world” is a means by which immigrant caregivers seek rest. It reveals their need to be reunited with their family and friends in order to relieve the burden of care and to find the strength to help them continue with their caregiving duties. Studies on migration have highlighted the key role that family and friends play in helping one another to find work and housing (Bertaux, 1993), and this study shows that the same is true for relieving the burden of care, describing how family ties are created through the caregiving relationship with people who would otherwise be strangers. Whereas, the public telephone constitutes a means for immigrants to raise their children (Rodríguez, 2007), this study also shows that it is a means whereby the caregiver relieves her burden of care.
While the category “turning to one’s own world” adds to the repertoire of respite activities described in the literature (Chappell, Colin Reid, & Dow, 2001; Stoltz, Willman, & Udén, 2006; Teitelman & Watts, 2004), it also highlights the importance for immigrant caregivers to be close to their families. Indeed, for caregivers, respite is a process of escaping from the caregiver world and into their own world where they feel free from the responsibilities and worries of caregiving (Strang & Haughey 1998). This study shows that for immigrant caregivers, this world frees them from an arduous task and puts them in touch with their families.
The limitations of this study are related to the situation and profile of the participants. As the participants are live-in caregivers, mostly of Latin American origin, it is possible that the perspectives reported here are limited. Likewise, the fact that they have been resident in Spain for less than 5 years could imply that their rest strategies differ from those used by immigrant caregivers who have resided here longer. Discussing rest in the caregivers’ actual workplace posed other limitations. It was necessary to probe deeply before the participants would open up and provide details of their resting strategies, as they may have felt that they were talking about something illegitimate.
Conclusions
Immigration has become a complex issue in caregiving (de la Cuesta-Benjumea, 2003). Not only must nurses deal with patients from other countries and provide culturally congruent care (Leininger, 1991), but they must also relate to immigrant caregivers who have different practices and experience from those of the professionals and their patients, as they come from different cultural backgrounds (de la Cuesta-Benjumea, 2003). This is an area of special interest for transcultural nursing. Diverse cultures are converging in family caregiving, which means that nurses must be adaptable, and in some cases, act as cultural mediators between patients, their caregivers, and the health system.
This study shows that feeling the presence of their family and friends helps immigrant caregivers to achieve rest. Therefore, it is obviously necessary to work toward integrating and normalizing the work and family situations of the immigrant caregivers, who are forming an increasing part of our society. This should be carried out both by official bodies and by the people and organizations which come into contact with these immigrant workers. Feeling that they form part of a society with rights and obligations, would help them to regain something of what they left behind and to relieve the burden of care.
The participation of immigrant caregivers in family care has increased. Consequently, they should receive special attention from health professionals as they form part of the caregiving system, while at the same time constituting the recipients of care. They should not, therefore, be excluded from nursing studies and interventions. It is essential to reduce the burden of care among immigrant women in Spain in order to improve their quality of life and health. Only then will they be able to continue providing care (Gallart Fernández-Puebla, 2004).
Health professionals must recognize immigrant caregivers as actual caregivers and address them as such when in home visits or consultations. They are not domestic workers. Professionals must also include them as a target population in health promotion and preventive activities. Specifically, nurses should involve immigrant caregivers in workshops and other educational activities as well as taking them into account in interventions to relieve the burden of care. Nurses occupy a unique position by influencing families who employ such caregivers. They are able to improve caregivers’ working and living conditions and inform employers about their need for rest. In addition, health professionals should recognize the meaning that immigrant caregivers attach to the burden of care and respite, so that they may undertake actions which promote culturally congruent nursing care. We hope that this study will contribute to this end. Providing culturally congruent health care is a requisite of health care today (Douglas, 2002) and represents the standard for nursing in the 21st century (Spector, 1999).
Finally, it is necessary to promote new lines of research and further projects that will contribute toward knowledge and understanding immigrant caregivers’ situation. In particular, further research with other cultural and immigrant caregiver groups is recommended to explore the strategies they use for relieving the burden of care.
Footnotes
Acknowledgements
Thanks to the participants who generously shared their experiences with us and to the reviewers for their insightful comments.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article. The study was funded by the Health Research Found, Programme of Biomedical and Health Sciences Research Promotion, Ministry of Health and Consumer Affairs (PI 060005).