
Abstract
The Ayoreo population constitutes one of Bolivia’s most vulnerable ethnic groups in terms of HIV/AIDS. Being a woman, indigenous, and a sex worker signifies belonging to a high-risk group. The aim of this study is to explore the Ayoreo sex workers’ and health agents’ perceptions of HIV/AIDS prevention programs in order to identify variables that could influence their success or failure. This study used an ethnographic methodology that included participant observation and semistructured interviews. In the data collection, participant observation and semistructured interviews with sex workers and key informants were conducted. Three themes emerged from the inductive data analysis: health prevention efforts, cultural inadequacy of prevention programs, and the eventuality of interventions. We conclude that nursing can develop culturally-adequate HIV/AIDS prevention interventions and programs as well as promote health within these populations.
Introduction
Goal 6 of the Millennium Development Goals, established by the United Nations (UN), aims to combat HIV/AIDS, malaria, and other diseases. However, much remains to be done to achieve the new targets and commitments outlined in the 2011 UN Political Declaration on HIV/AIDS (UN, 2011) to secure a future free from HIV. Despite remarkable efforts being made to end the epidemic, the latest published data regarding new infections (2.5 million in 2011) show that figures are still high (Joint UN Program on HIV/AIDS [UNAIDS], 2012c).This report highlights the fact that HIV prevention and treatment programs have limited ability to reach vulnerable groups such as indigenous populations and sex workers. It is vital that structurally and culturally adapted preventive programs are developed both within specific populations in concentrated epidemics and across the whole population in generalized epidemics. Our study was carried out in the Ayoreo population in Bolivia, a discriminated and very vulnerable indigenous group (Roca, 2012). The objective was to explore the sex workers’ and health agents’ perception of HIV/AIDS prevention programs in order to identify variables that could have an influence on the success or failure of these activities.
Background
The UN highlights the necessity to tackle the particular vulnerability of women to HIV. This vulnerability is as much due to physiological factors as due to other factors: social, legal, economic, and gender inequality, including discrimination and violence (UN, 2011). Consequently, there have been joint efforts to focus on prevention through empowerment and the elimination of all types of discriminations, as promoting gender equality and the empowerment of women are fundamental for reducing their vulnerability to HIV (UN, 2011). This means reviewing political and legal frameworks, together with encouraging the commitment and participation of community, local, regional, national, and international leaders to eliminate obstacles preventing an efficient response to control and detain the HIV epidemic (UN, 2011, 2012). Sex workers require special attention, as they are in a vulnerable group where the probability of contracting HIV is 13.5 times higher (UNAIDS, 2012b). Information and education programs in the area of sex work and HIV prevention should focus not only on the risk, prevention, treatment, and care of HIV/AIDS but also on sexual health, rights, obligations, responsibilities, and opportunities for individual and collective action. These programs should also consider age, cultural adequacy, and the target population, which is the sex workers and to their clients (UNAIDS, 2012a). However, the programs to reach key populations (e.g., sex workers) receive only 4% of the amount invested in basic HIV prevention and treatment programs globally (UNAIDS, 2012c). The estimated HIV prevalence in Bolivia is 0.2%, a figure that rises to 0.56% among sex workers, who comprise the group with the second highest prevalence rate of HIV/AIDS in Bolivia (Bolivian Government, 2012). The Ayoreo population in the city of Santa Cruz live in conditions of social exclusion, poverty, and discrimination. Furthermore, the majority of women resort to sex work from adolescence. This situation has increased HIV/AIDS mortality rates and vulnerability in this minority population in recent years (Roca, 2012).
Although the traditional concept of prevention should be reviewed, primary prevention continues to be regarded as the promotion of health when faced with the development of the illness, secondary prevention as early detection, and tertiary prevention as something that halts or slows down the illness’s progression (Starfield, Hyde, Gérvas, & Heath, 2008).
The cultural care diversity and universality theory is one of the most relevant nursing theories, the objective of which is to provide people culturally congruent and safe care, bearing in mind social structure, world perspective, and environmental context (Leininger & McFarland, 2006). In turn, this vision concurs with UNAIDS’ recommendations in terms of factors to take into consideration when dealing with prevention programs to tackle HIV/AIDS.
Method
We designed a qualitative study based on M. Leininger’s (2002) theory of cultural care diversity and universality: an ethnographic study that facilitates the knowledge regarding a cultural phenomenon in a specific context (Alexander, 2005). Ethno-nursing is a naturalistic research method focused on the way of understanding and experiencing the lives of its participants (Leininger, 2006). We developed a mini ethnography—a small-scale ethnography focused on a specific area of investigation, which can be adapted to the objective and the temporal limitations of the study (Wolf, 2012). Unlike traditional ethnography, which is focused on wider elements and populations, mini ethnography is focused on a specific research area. This use of method was important to learn about unknown aspects of a problem from an emic point of view (Flick, 2009).
Setting and Population
Having been awarded a grant from the Spanish Agency for International Development Cooperation, the main researcher traveled to the Santa Cruz department to carry out fieldwork. The Ayoreo are mainly located in rural communities and in three urban settlements in Bolivia. In the first stage of the study, key informants who complied with the following inclusion criteria were selected (Marshall & Rossman, 2011): to be working in HIV/AIDS prevention programs within the Ayoreo population, to have had contact with Ayoreo sex workers (cuajojodie, in the Zamuco language), and to be prepared to share their time and experiences with the researcher. The informants were chosen with help from Epua Kuñatai Foundation members, local partner of the nongovernmental organization (NGO) Nurses for the World in carrying out health education programs with the Ayoreo sex workers and the general population.
The main researcher took part in health education tasks in the Bolivian communities. In the second stage, contact was made with the sex workers in one Bolivian city. This neighborhood was chosen because the mediator had contact with sex workers who worked as prostitutes in that area. The girls, who do not have pimps, practice prostitution in wide, deserted streets. After contacting the clients, they go to small motels or to rooms in private houses. The sex workers had a good physical appearance, were clean, wore makeup, and were suitably dressed.
Data Collection
Data collection was carried out in November and December 2011. The study was formed of a total of 12 participants: 8 key informants and 4 Ayoreo female sex workers (Table 1). The interviews were conducted in Spanish, the official language in Bolivia. The number of key informants interviewed was determined by saturation of data; when no new themes were emerging, collection was stopped. Interviews with Ayoreo sex workers were interrupted by the murder of one of the sex workers. This prompted a warning from the authorities for cojñone (outsiders) to leave the area.
Demographic and Professional Characteristics of Study Sample (N = 12).
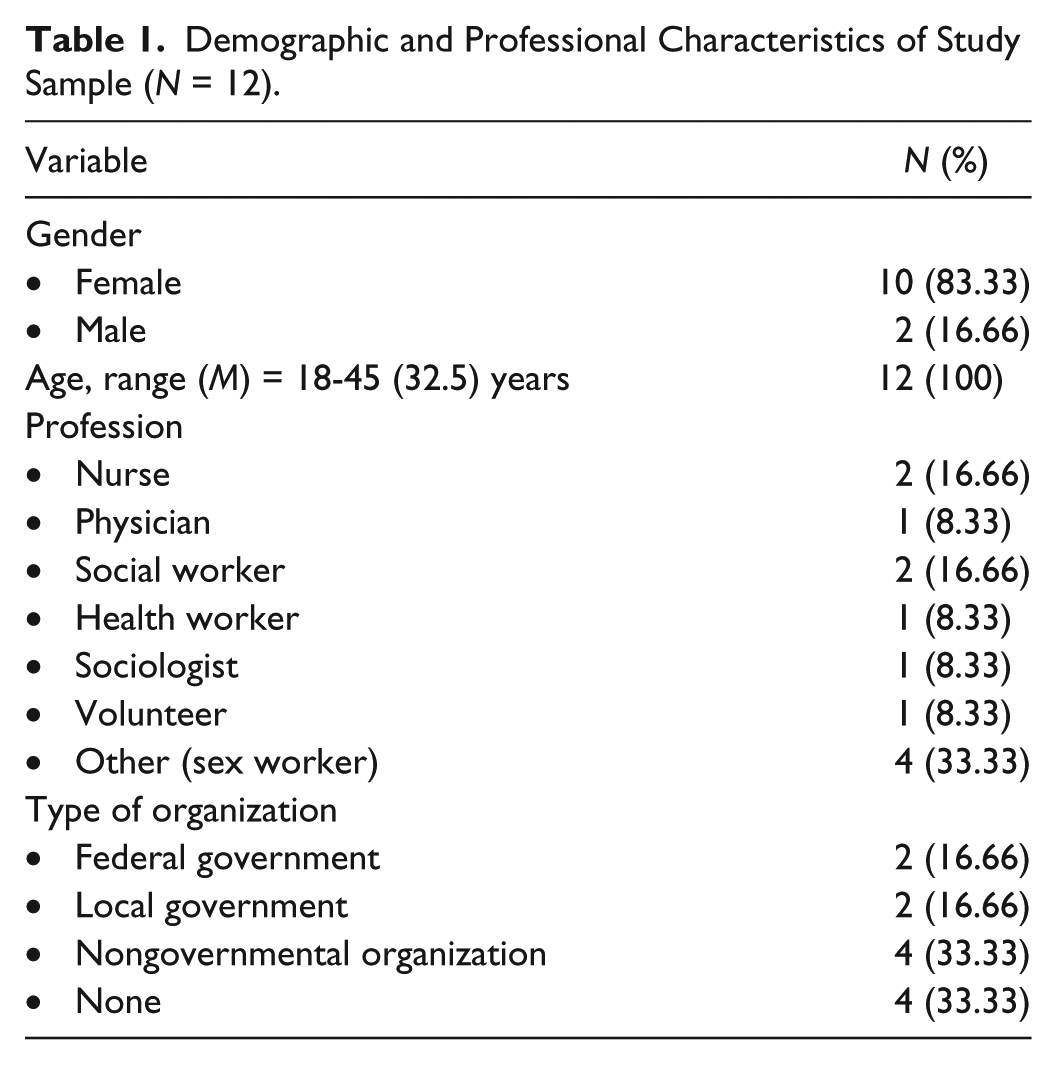
Observation took place for 6 hours a day in centers where the key informants carry out epidemiological surveillance and health education programs as well as in streets where sex workers engage in prostitution. Interviews with key informants were carried out in work offices or clinics and lasted 45 to 60 minutes; interviews with sex workers were 15 to 30 minutes long.
Data Analysis
Data analysis was based on Leininger’s (2006) four stages of ethno-nursing for qualitative data. In the first stage, the main researcher compiled the data collected in the recorded interviews and fieldwork. Afterward, the data were transcribed and listened to again in order to ensure their integrity together with contextual meaning. During the second stage, the transcripts were reread and codes were assigned to specific sections that described the meaning of the interview data. Furthermore, field notes were examined, searching for similarities, differences, and meanings. In the third stage, the researchers studied the data, grouping codes into conceptual categories, taking into consideration nonverbal behaviors and contextual elements that could influence meaning. In the fourth stage, inductive work was carried out, which allowed for major conceptual categories or themes to be extracted (Hammersley & Atkinson, 2007). Atlas.ti 7 software was used throughout all stages of the study.
Rigor
Methodological rigor was verified in the stages of fieldwork, observation, interviews, and data analysis. Auditability was guaranteed by creating paper records of the recordings. All research team members worked together to check reliability of coding and to evaluate the evidence throughout data collection (Guba & Lincoln, 2005).
Comparability and confirmability were established by confirming derived themes with several of the participants.
Ethical Issues
The ethical research committee at the researcher’s university granted approval to carry out this study. Both sex workers and key informants were informed of the nature and purpose of the study, prior to obtaining consent. Data privacy and confidentiality were maintained at all times. Participation was voluntary, with the right to refuse and/or withdraw from the study at any time.
Findings
Here, we show the three themes that emerged from the analysis of information given by the informants (Figure 1), together with the authors’ interpretation and textual quotes from the informants. Participants have not been identified in order to ensure their anonymity.
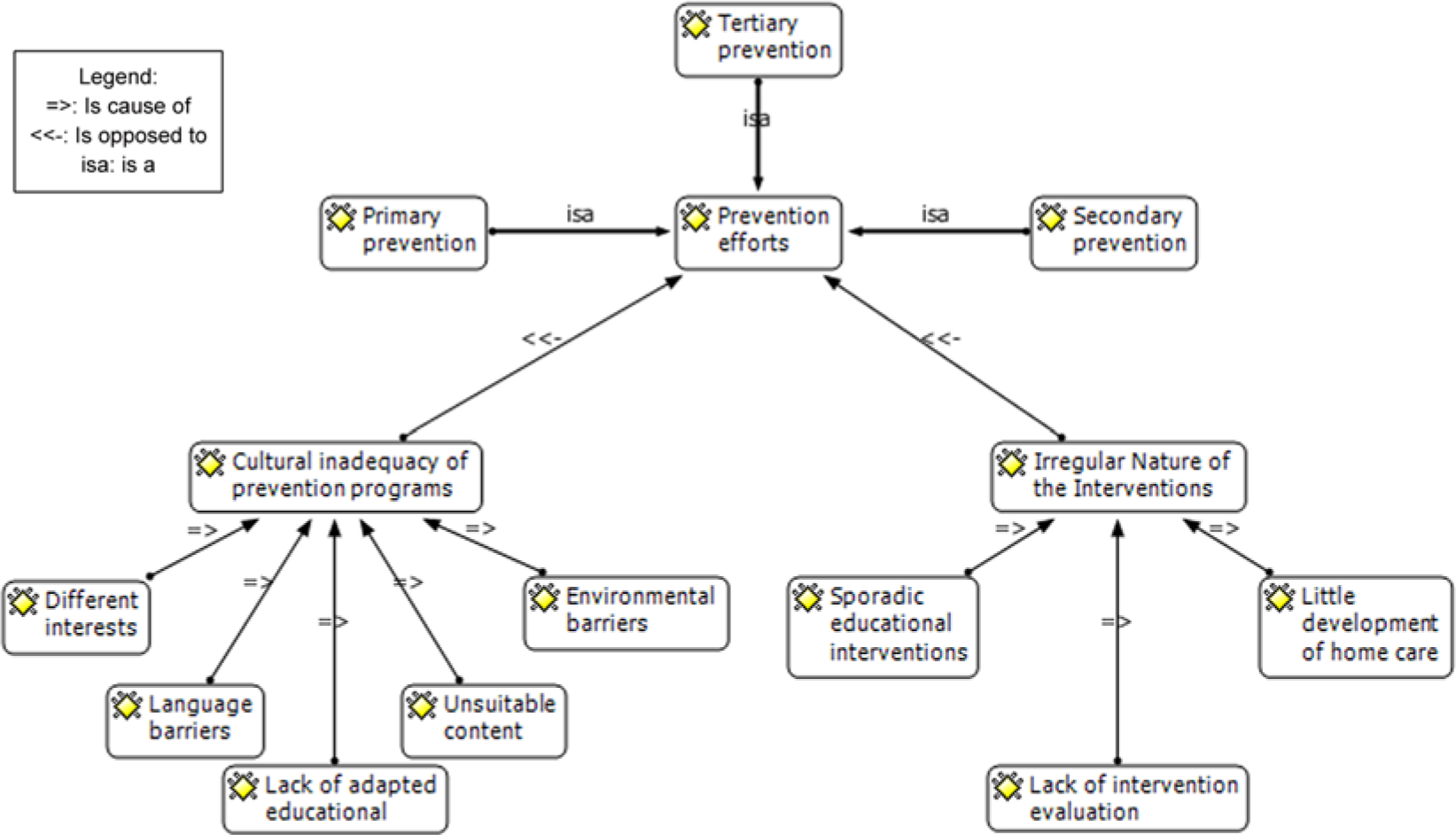
Conceptual map of interrelated emergent themes and subthemes.
Theme 1: Health Prevention Efforts
The participants reported various interventions that can be related to different levels of prevention. Primary health prevention is defined as an etiological prevention of the illness. Within the context analyzed and with the Ayoreo sex workers, such prevention is limited to intermittent interventions within the community, in the same place where sex workers engage in prostitution, as pointed out by one of the informants, a sociologist: Primary prevention is occasionally carried out in the place of work, right? That means on a corner or a place on the street that they have access to. (Informant 5)
In these interventions, the aim is to give information about the disease, how it is transmitted, and prevention methods, while avoiding stigmatizing people who have AIDS, talking about living together in the community. This was confirmed by a social worker: What’s been done with them is giving basic information about what HIV is, how it’s transmitted, what the difference is between HIV and AIDS and what would be risky situations. They are told about how to prevent it, how it’s transmitted and how to live with another person in the community who has HIV. (Informant 7)
However, reports from the sex workers imply that there are other “more important” questions for them: Do you use the condoms?—Some men don’t want to [. . .] once a guy told me, “I’ll pay you 200 on the side [. . .] if you give me a blow job without a condom.” What happened? [Laughs, looks at the ground] Did he give you the 200 in the end? Yes. (Informant 4)
Secondary health prevention relates to early detection or screening programs. For Ayoreo women, this is limited to the rapid detection test that has been offered to sex workers since 2007. However, taking the test does not guarantee the sex workers participation in the following stages or levels of prevention or care: We go to communities to do the rapid test to catch HIV in women. That’s what we do, but they don’t carry on coming . . . There’s no continuity . . . (Informant 11)
We have serious difficulties in communication with Ayoreo sex workers, as our conversation about the rapid test with the sex workers demonstrates: Has anyone ever come to talk to you about HIV?—Yes.—Who? –People.—People on the street?—Yes.—What about doctors, nurses? Have they come to your community to talk about HIV? -They talk, yes. (Informant 1)
The sex workers acknowledge the existence of the head office of a mobile unit in charge of carrying out the rapid detection test, but they are not always attended: Aha! The van went there to do the test but we weren’t around . . . (Informant 3)
The participant observation field notes (FN) confirm the existence of prevention efforts which combine educational interventions (primary prevention) and early detection (secondary prevention). However, the results have also been shown to be very limited: The doctor went from one to the other, asking them about the use of a condom and if they remembered talking about HIV the last time they came. Neither Informant 1 nor Informant 2 knew how to answer the questions, “What is HIV, how is it transmitted and how can it make you ill?” (FN)
Tertiary prevention is focused on achieving adherence to treatments, on learning to live with HIV, and on overcoming the tendency to stigmatize people who are HIV-positive. A medical informant confirms this: We come to try to help a person with HIV so that they don’t reach the stage of AIDS too quickly, so that they adhere to treatment, that they know a little more about HIV, that they learn to live along side it, both personally and within the community. (Informant 9)
On this prevention level, there are also serious problems. Even though antiretroviral treatment is ensured with the help of international organizations, attempts to secure adherence to treatment are often done in vain. As one health care worker stated, Of 10 cases identified in the community, only 2 attend the program. (Informant 6)
Theme 2: Cultural Inadequacy of Prevention Programs
We have identified a series of obstacles affecting the success of the prevention programs. The first of which is the language barrier. The Ayoreo people are a population that have recently left the jungle and have established themselves in Western society. The level of schooling is minimal, and there are high levels of illiteracy. This contributes to the Ayoreo people’s poor grasp of the Spanish language, influenced by the scarce interest shown toward educational interventions. This was confirmed by a nurse: It might be that one person has a good understanding of Spanish . . . for example, from a group of 20 Ayoreo women, one [has a good understanding] and the other 19 women are confused. (Informant 8)
These language barriers are confirmed by field notes, which show that during the interview, they already do not remember what was said to them an hour before, when they attended the consultation, during which the basic information was reiterated: The doctor repeated the basic information about HIV and insisted on the use of a condom and they agreed. The interviews for this study were carried out after, and despite receiving the information less than an hour before, they still didn’t reply. (FN)
Together with this obstacle, the participants stated that the prevention programs are not culturally adapted, starting with the lack of adapted educational material: You can have great material translated into Ayoreo, [but] after, you’re going to have to ask yourself, “Right, how many are literate and can read educational material fluently?” Audio and audiovisual material is better, where they’re going to see it, listen to it and it’s going to reach the population. (Informant 9)
A suitable adaptation of the contents is also missing. The informants complain that the majority of the material does not address the needs of the people it is aimed at. What interests the population is not anatomical or physiological ideas but more practical questions: It doesn’t help me for an Ayoreo person to know the physiology of his or her body, the sexual organs, that the penis is called a penis, that the vagina is called a vagina. Ok, I agree, but for me now, what’s most important is that they know how to take care of one’s health and where they can go to care after their health. It’s important for them to know what to do if they are going to be sexually abused and what to do to avoid getting sexually abused (Informant 6)
The lack of following of the activities and the inadequacy of contents produces mutual frustration, suggesting that the interests of the female Ayoreo population and those of the health agents are quite different. One sociologist stated, People who attend feel frustrated because they don’t understand, or they don’t like it, or because they want money or food. People who are giving they talk feel frustrated because they want everyone to pay attention, to be still and quiet. (Informant 5)
This idea is confirmed by a sex worker, who states that what she likes most about the health education interventions are the infusions that are normally offered at all of the meetings in Bolivia.
Has anyone come to talk to you about HIV?—Yes—What do you like most?—That they brought [herbs] to make mate [traditional South American infusion]—Did you like what they talked to you about?—I didn’t understand a lot of it. (Informant 2)
Observation field notes verify the lack of interest of those attending the Health education talks: In the health education talks, I’ve often seen the Ayoreo people get distracted, and I’ve seen a lack of attention towards what the speaker was saying. On several occasions, they have even had to stop talking because no one was listening. (FN)
When other means have been tried, such as audiovisual projections, the researcher witnessed environmental barriers, which were added to those already mentioned: The NGO Vivo en Positivo (Live Positive) is projecting a 20-minute video about the how HIV is transmitted. The video can hardly be heard because of the tremendous noise from the cars; the windows are open because of the heat. (FN)
Theme 3: Irregular Nature of the Interventions
Health education is not a service offered by the health system in a systematic way, but rather one that is occasional, to comply with some quality control criterion or other. As such, interventions are carried out sporadically to comply with indicators but without the desirable continuity. As one health care worker stated, Nurses do [the health education], but normally they carry them out to cover indicators . . . Whilst these actions aren’t continuous and in the Ayoreo language, it’ll just be a pretty presentation where they’ll get some kind of free gift, rather than dealing with a process of empowerment and ways of real prevention. (Informant 6)
It does not seem like the NGOs have managed to overcome these difficulties either, falling into the same problems of discontinuity and inadequacy with their interventions: They’ve done various interventions . . . “Enfermeras para el Mundo” (Nurses for the World), people from “18 de marzo” (March 18), from “SEXSALUD” . . . but all of these have been one-off occurrences and have not been culturally adapted. (Informant 5)
In an environment with significant limitations related to accessibility (little tradition of going to the physician, economic cost) home care could contribute to the establishing and continuing of prevention programs. However, this care method has been scarcely developed, depending more on the voluntarism of the nurse than on the health organization: [The nurses] always say that they don’t do many patient home follow-up visits because they don’t have the time, because they have to watch the supplies and other things. Nurses concentrate on care, on the clinical side. (Informant 12)
In relation to this topic, the lack of evaluation of the interventions also emerged. No planning is complete without the evaluation stage, which provides the necessary outputs to measure the efficacy of the interventions. As one health care worker stated, When you see that the use of a condom isn’t happening and you ask, “But have they gone to the hospital?” “Yes they have” “Have they gone to the organizations?” “Yes” “And did they give you them?” “Yes” “Ah! And did you use them?” “No”. This tells you that the process wasn’t a success and they could do a thousand more presentations the same, and they’re going to fail in the same way, simply because there isn’t a postevent evaluation to see what effects and impacts the processes are having. (Informant 6)
Discussion
The objective of this study was to explore the perceptions that female Ayoreo sex workers and health agents have regarding HIV/AIDS prevention programs in order to identify variables that could have an influence on their levels of success or failure. Employing an ethno-nursing approach, based on M. Leininger’s theory (Leininger & McFarland, 2006) has allowed us to gain understanding from an emic point of view, without which our prevention efforts could have been in vain.
Specific HIV prevention programs are being called for in South American countries (Bautista et al., 2008), but our results suggest that even though HIV prevention efforts are being made in the Ayoreo population, they are sporadic interventions that lack cultural adaptation and, as such, have little success.
In this regard, our findings agree with those of Roca (2012), who points out that there are no specific HIV/AIDS prevention programs for Ayoreo sex workers, nor are there any for the community as a whole. Similar problems (lack of funding, few programs) have been described in other geographic locations such as Papua New Guinea (Clark, Chapman, & Francis, 2011).
Previous studies on the beliefs and attitudes of Ayoreo sex workers in relation to HIV/AIDS point out the social and family acceptance of sex work and the opposition to wearing a condom. All of this, together with the lack of knowledge or concern about the disease and how it is transmitted, contributes to maintaining risk behaviors (López-Entrambasaguas, Granero-Molina, & Fernández-Sola, 2013; Roca, 2012). The sex workers interviewed did not show any knowledge about HIV and maintained that no one had told them about it, although they pointed out that health professionals had visited their community. Participant observation in the Ayoreo communities produced similar perceptions: They had heard talk about HIV but they did not respond to questions about what it is, nor were they clear about how it is transmitted.
Education has been identified as one of the fundamental defenses against the spreading of HIV (Gardner, 2013; Hurtado, Alastrue, Pavlou, Tasa, & Pérez-Hoyos, 2012) and against the stigmatization of people with AIDS (Badahdah, 2010). In our study, this defense proved to be weak, as there were many barriers or obstacles, among which language barriers stood out, which were probably related to the low levels of literacy. We also found socioeconomic barriers, most probably related to the fact that we are dealing with a marginalized population, dominated by oppression and poverty. This agrees with other studies that state that literacy, psychosocial barriers, and socioeconomic barriers are obstacles in HIV/AIDS prevention programs (Huedo-Medina et al., 2010; Mackenzie et al., 2011).
As well as helping maintain risk behaviors, these elements also encourage stigmatization, which in turn feeds the problem, as shown by a recent study in which women refused to take the test for fear of rejection (Gardner, 2013).
We were witness to the attendees’ lack of interest and attention at the HIV/AIDS information talks. This made us question if this was due to language barriers, the cojñone’s disinterest, or the maladjustment of the health promotion strategies. In any case, it seems to be clear that it is vital to look for other ways of approaching the issue and of creating trust so that safe and responsible sex education is more successful. In relation to this, Puig and Montalvo (2011) report that in their study of Bolivian indigenous people, they asked for information about STIs/HIV by means of illustrated or audiovisual mediums, in their language. Furthermore, the Pan American Health Organization (2010) highlights the need to develop sexual and reproductive health programs that are adapted to different cultures, which take the different stages of life into consideration and incorporate aspects regarding the prevention of gender-based violence. In this respect, various authors have highlighted the need to focus HIV/AIDS prevention programs on adolescents (Castillo-Arcos & Benavides-Torres, 2012; Sawyer et al., 2012), as strategies centered on this stage of life offer important chances to improve health, both in adolescence and in the later stages of life. This is particularly important in the topic studied, as it is known that Ayoreo sex workers are active from adolescence (López-Entrambasaguas et al., 2013; Roca, 2012).
Health education and home care are hardly developed in the communities studied. According to our informants, some nurses carry out the work sporadically, but this is done to comply with indicators rather than for the needs of the population. From this, we can deduce that the health system has a potential for development if it is decided to take full advantage of the resources at its disposal. This has also been suggested by the Pan American Health Organization (2001), which points out that nurses, regardless of any curative care they carry out in hospitals or districts, should perform tasks related to health education, encourage healthy behaviors, and organize preventative health activities.
Furthermore, cultural aspects related to the care and research of AIDS/HIV must be considered (UN, 2011), just as we have done in this study. In this way, and from a health research perspective, social justice is aided, focusing efforts on more disadvantaged populations (Rogers& Kelly, 2012). Cultural care should help nurses maintain an unprejudiced view of the “other” (Plaza &Veiga, 2012), thus avoiding the authoritarian and punitive role that health professionals often adopt when faced with unhealthy behaviors (UNAIDS, 2012a). Similarly, sharing cultural practices and beliefs could have a positive influence on risk behaviors in the population in question (Lara, Brito, & Rezende, 2012).
Along these lines, NGO professionals have been characterized by their holistic approach, by their cultural and professional competences, and by the activities they offer being adapted to the needs of those they are aimed at. Preventative activities of NGOs that work with HIV/AIDS are based on a model of participative health education, adapted to the needs of the population, based on their empowerment (Berenguera et al., 2011). Our results show a contrast with this image, as participants stated that NGO interventions lack the same cultural suitability as the other health professionals.
Limitations
The limitations of this study are related to the small sample size of sex workers. A violent act against a sex worker in the community made it advisable for the main researcher to leave the area. Interviews with new sex workers could produce different results and improve understanding of the phenomenon from their point of view. However, the key informants displayed good knowledge of the community studied, having worked with it for many years.
Another limitation of this study is that it was carried out as part of a wider cooperative research program that examines factors such as sexual-reproductive culture in the Ayoreo community and the sex workers’ beliefs and attitudes regarding HIV/AIDS. An overview could have provided the study with greater richness and contrast, but this would have been detrimental to the depth with which each topic was dealt.
Conclusion and Implications
In this study, we have identified factors that limit the success of HIV/AIDS prevention programs for Ayoreo sex workers. Among these, the cultural inadequacy of existing interventions, language and environmental barriers, unsuitable content, and a lack of continuity, monitoring, and evaluation of the interventions stand out.
Nurses represent 65% of human resources in Bolivia’s health system structure (Pan American Health Organization, 2011) and have demonstrated their abilities and desire to be involved in improving health care (Fernández-Sola et al., 2011). For this reason, they could actively participate in the design of culturally adapted programs aimed at preventing illnesses and promoting health (Carvalho, Galvão, & Silva, 2010; East, Jackson, O’Brien, & Peters, 2011). The results of this study suggest that theory-driven interventions, for example, interventions driven by the transcultural care theory, could enhance the success of HIV prevention among the Ayoreo population.
Footnotes
Acknowledgements
The authors would like to express their gratitude to the young Ayoreo women who participated in the study, to the informants who took part in the interviews and who made it possible for the main researcher to access the area, and finally to the NGO Enfermeraspara el Mundo (Nurses for the World). This article was accepted under the editorship of Marty Douglas, PhD, RN, FAAN.
Declaration of Conflicting Interests
The author(s) declared that they have no potential conflicts of interests with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by Department of Nursing Science, Physiotherapy and Medicine, University of Almería and NGO Enfermeras para el Mundo (Nursing of World).