
Abstract
Recent reviews of vitamin D insufficiency among North Americans (Calvo & Whiting, 2003) and studies among Canadian mothers and infants (Li et al., 2011; Ward, 2005) have identified a need to understand knowledge and practice of vitamin D supplementation among the general population and, in particular, vulnerable populations. Vitamin D is best known for its essential role in bone formation and preventing rickets (Holick, 2008; Ward, 2005), but additional associations have been found between vitamin D deficiency and a variety of chronic diseases (Grant, 2006). Vitamin D is synthesized in the skin from exposure to ultraviolet radiation (UVR), but use of sunscreen to protect against skin damage and living at high latitude reduce UVR exposure (Holick, 2007). Although it has been found in Canada that during winter higher blood levels of vitamin D can be maintained through consumption of dietary supplements, among Canadians aged 6 to 79 years only 31% reported use of a vitamin D supplement (Whiting, Langlois, Vatanparast, & Greene-Finestone, 2011). Surveys of select groups of otherwise healthy adults and youth in Canada report a high prevalence of vitamin D insufficiency (Godzik et al., 2008; Mark et al., 2008; Vieth, Cole, Hawker, Trang, & Rubin, 2001; Whiting et al., 2011) as well as persistent rickets, particularly among children who reside in Canada’s north and among infants with darker skin who are breastfed without vitamin D supplements (Ward, Gaboury, Ladhani, & Zlotkin, 2007).
Canada has adopted the international recommendation that mothers exclusively breastfeed their children for the first 6 months of life (Health Canada, 2004a). Human breast milk contains relatively low amounts of vitamin D, and maternal deficiency in vitamin D is correlated with deficiency in their infants (Speck, 1994). Mothers in Canada who are exclusively breastfeeding are advised to supplement their infants with 400 international units (IU) of vitamin D daily until the infant’s diet includes 400 IU per day or the child reaches 1 year of age (Canadian Paediatric Society, 2007; Health Canada, 2004b).
Many immigrants confront a range of challenges and barriers to disease prevention and health promotion that affect their well-being on arrival in Canada and for several years thereafter (Wu, Penning, & Schimmele, 2005). Except for one report on vitamin D status of adult male and female East Indian Punjabi immigrants (Gibson, Bindra, Nizan, & Draper, 1987), remarkably little is known about the impact of resettlement in Canada on vitamin D status, despite evidence from other countries that immigrants and, in particular, immigrant women of child-bearing age and infants, may have high levels of deficiency (Madar, Stene, & Meyer, 2009; Wishart, Reeve, & Grant, 2007).
This pilot study is designed to narrow gaps in understanding of vitamin D deficiency among vulnerable populations in Canada. New Canadian mothers with infants are highlighted for five reasons. First, immigrant mothers are more likely to exclusively breastfeed their infants (Millar & Maclean, 2005). Second, they may be less likely to take vitamin D supplements or give them to their infants due to lack of information stemming from difficulties in cross-cultural communication (Zanchetta & Poureslami, 2006). Third, given the demographics of recent immigrants, where the top three regions of origin are Asia, the Middle East, and Africa (Citizenship and Immigration Canada, 2008), many immigrant mothers come from countries where there is sufficient UVR exposure to synthesize vitamin D year round. In many of these countries, however, there is also high reported prevalence of vitamin D insufficiency, possibly due to sun avoidance or clothing customs that prevent sufficient sun exposure for vitamin D synthesis (Dijkstra et al., 2007). Fourth, darker skin pigmentation can be a phenotypic characteristic of some peoples from Asia, the Middle East, and Africa that conditions a requirement for higher UVR exposure to synthesize sufficient vitamin D (Chen et al., 2007). Recent studies confirm that significantly higher proportions of Canadian adults and children of non-European descent have lower than recommended levels of serum 25(OH)D than those of European descent (Godzik et al., 2008; Langlois, Greene-Finestone, Little, Hidiroglou, & Whiting, 2010). Fifth, immigrants may consume less vitamin-D-rich or fortified foods due to higher levels of food insecurity (Rush, Ng, Irwin, Stitt, & Meizi, 2007) and the cost of supplements.
In this study, immigrants are distinguished from refugees. Immigrants are “independent” or “economic” immigrants and family class immigrants (those being reunited with their family members living in Canada). Refugees arrive in Canada fleeing persecution in their countries of origin. They may be refugees, who have been selected for resettlement in Canada either by the government (government-assisted refugees [GARs]) or by private sponsors. Refugees who come to Canada seeking asylum are called “in-Canada” refugees (Government of Canada, 2013). Immigrants can be classified as recent and long-term. Statistics Canada defines recent immigrants as those settled in Canada for less than 5 years (Statistics Canada, 2008). This study follows previous researchers, including Khandor and Koch (2011), who define recent immigrants as those who immigrated to Canada within the past 10 years. This allows health and behavior to be examined over a longer period of resettlement.
This study investigates the following questions: Are mothers who immigrated to Canada within the past 10 years less likely to know about and practice infant vitamin D supplementation than Canadian-born mothers? Do knowledge and practice of infant vitamin D supplementation differ between immigrant and refugee mothers?
The study is approached from a social perspective following Schubert, Gallegos, Foley, and Harrison (2010), which considers both structural barriers to infant vitamin D supplementation—lack of knowledge about the issue, financial inability to purchase supplements, food insecurity—as well as the agency of the mothers themselves—exposure to culturally acceptable nutrition education and ability to act on recommendations within their understanding of child care norms. This study qualitatively explores knowledge, barriers, intentions, and practice of vitamin D supplementation. It also accounts for some of the quantitative parameters such as the demographic characteristics of the mothers (age, years resident in Canada), infant feeding practice (formula, mixed, or exclusively breastfed), and whether or not mothers supplemented their infants with vitamin D (yes, no, or partially). Quantitative data are not used to test hypotheses but rather to aid in interpreting the qualitative results.
Method
Participants were recruited from three major urban centers of newcomer resettlement: one city in Western Canada and two cities in Central Canada. Following previous researchers working with refugees in Britain (Sellen, Tedstone, & Frize, 2002), service-based, purposive sampling was adopted. In the Central Canadian cities participants were recruited through early childhood centers that offer prenatal education classes and support for parents with children aged 0 to 6 years. In the Central Canadian cities two samples were recruited: one limited to mothers born outside of Canada who had immigrated to Canada within the past 10 years and the other to mothers born in Canada.
In the Western Canadian city the sample was recruited from a health clinic that exclusively serves GARs. The clinic provides primary care and public health workshops for refugees. GARs can be a difficult population to access due to their mobility within the host country and vulnerability and trust issues in working with researchers. Only GARs were included in the Western Canadian city sample because of the opportunity to include a large number of GAR participants at this location. GARs are quite distinct from other newcomers in that they often arrive from war-torn or fractured situations. Many have lived in refugee camps or other marginal living situations and thus generally experience slower sociocultural and economic integration into Canada; they have distinct needs regarding accessing both health care and health promotion messaging (Yu, Ouellet, & Warmington, 2007). Thus, focused attention on GARs is warranted to see whether they may have had different levels of knowledge or use of infant vitamin D supplementation compared to other types of immigrants or Canadian-born mothers. Though participants were recruited from each target stakeholder group studied—economic and family class immigrants, Canadian-born, and GARs—from each of the different cities, the services available in these major Canadian cities are comparable and thus do not compromise our ability to compare the groups.
Inclusion criteria for participants were the following: mothers with children 3 years of age or younger and some ability to speak English, except for GARs with whom interviews were conducted in Spanish and Arabic as well as English. Any information collected from immigrant mothers who arrived in Canada before 1999 were excluded from this analysis. This study protocol was given ethics clearance by three university institutional review boards. Focus group discussions (FGDs) were employed in order to interview a large number of participants in a short period of time and to generate discussion that could not have been generated during one-on-one interviews, in which some participants may not have been comfortable sharing information with a single interviewer. FGDs took place in private conference rooms from October 2009 to June 2010. Each volunteer provided written informed consent and completed a short quantitative sociodemographic questionnaire before participating. FGDs were facilitated using semistructured questions organized into the following themes: infant feeding practices both in country of origin and as practiced in Canada; basic knowledge of vitamin D and infant supplementation; experience with obtaining information and advice from health care providers and other sources such as family and friends; the actual use and practice of supplementation and any barriers or supports that accompanied it; and social support regarding infant care and infant feeding. Examples of questions pertaining to each of these sections include the following: Do you give any vitamins or supplements to your baby? Has anyone ever told you to take vitamins or supplements yourself or give them to your child? Who (Family member, friend, health care provider, etc.)? What have you been told to use for you and your baby (Probe for vitamin D)? What do you know about Vitamin D? Is it easy to give a baby a vitamin D supplement? Is it affordable?
FGDs were digitally recorded and transcribed verbatim. A content analysis was conducted (Graneheim & Lundman, 2004), coding responses according to themes described above and reporting themes for each subgroup (Canadian-born, immigrant, and GARs), and in some cases with frequency of response if warranted. Themes and subthemes were coded using NVivo 8 (QSR International) qualitative software. Participants’ responses on infant feeding of their youngest child (less than 3 years of age) and vitamin D supplementation practices (current or retrospective, in the case of children aged 1 to 3 years) were also aggregated quantitatively.
Results
The sample included 94 participants: 35 immigrant, 29 GARs, and 30 Canadian-born mothers. Focus group size ranged from 4 to 19, with an average of 10 participants. Table 1 shows frequencies of responses to the socio-demographic questionnaire.
Sociodemographic Profile of Study Participants (N = 94).
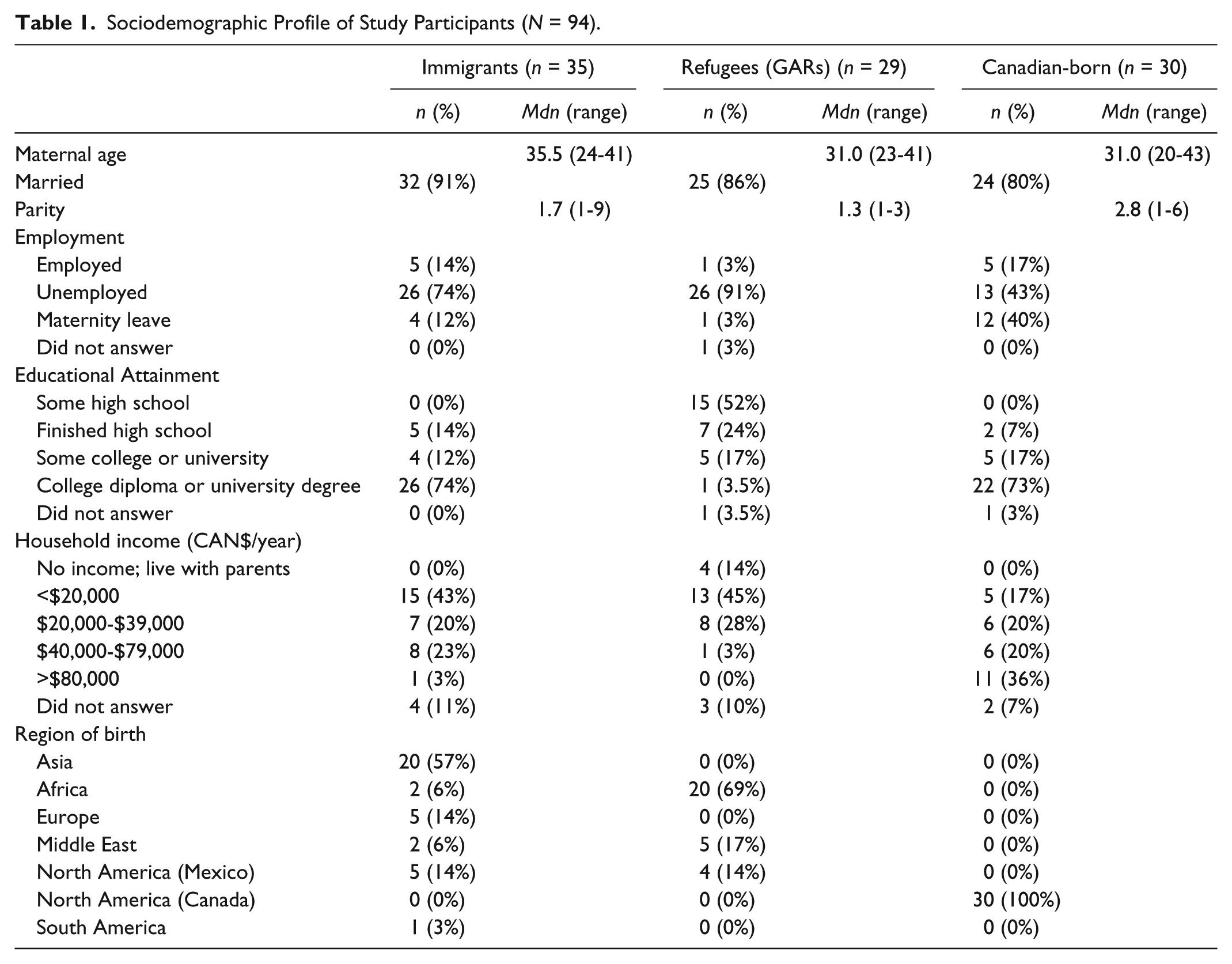
The proportion of unemployed mothers was markedly higher among the immigrant mothers in the two Central Canadian cities (74%) and higher yet among GARs in the Western Canadian city (91%) compared to Canadian-born mothers in the two Central Canadian cities (43%). While Canadian-born mothers and immigrants had similarly high levels of education, GARs were much less well educated. There was a wide range of countries of origin for immigrants in the two Central Canadian cities, but the majority of participants came from the top two regions of origin for Canadian immigrants: Asia and the Middle East (Table 1). Though participants were not classified by immigrant status in the Central Canadian cities, country of origin indicates that most of them likely arrived as economic and family class immigrants or refugee claimants but not as GARs (Citizenship and Immigration Canada, 2008). Nineteen (66%) of the 29 GAR participants interviewed in the Western Canadian city were from Sudan. Canadian-born mothers were not asked to identify ethnicity or ancestral countries of origin, but the majority could be inferred to be of Euro-Canadian ancestry based on surname and mothers’ discussion of their family backgrounds. There were a few exceptions but not enough to allow any comparative analysis among Canadian-born participants regarding the influence of ethnicity.
Infant Feeding and Vitamin D Supplementation
A majority of mothers in all groups reported exclusive breastfeeding for 4 to 6 months (Table 2). Of those infants who were currently or had been exclusively or partially breastfed almost all (25/30) immigrants and Canadian-born participants (21/26) answered “yes” to the question of whether they supplemented their infants daily with 400 IU of vitamin D. In contrast less than half (10/21) of the GAR participants from the Western Canadian city reported supplementing their exclusively breastfed infants (Table 3).
Reported Infant Feeding Practice for Youngest Child (N = 94).
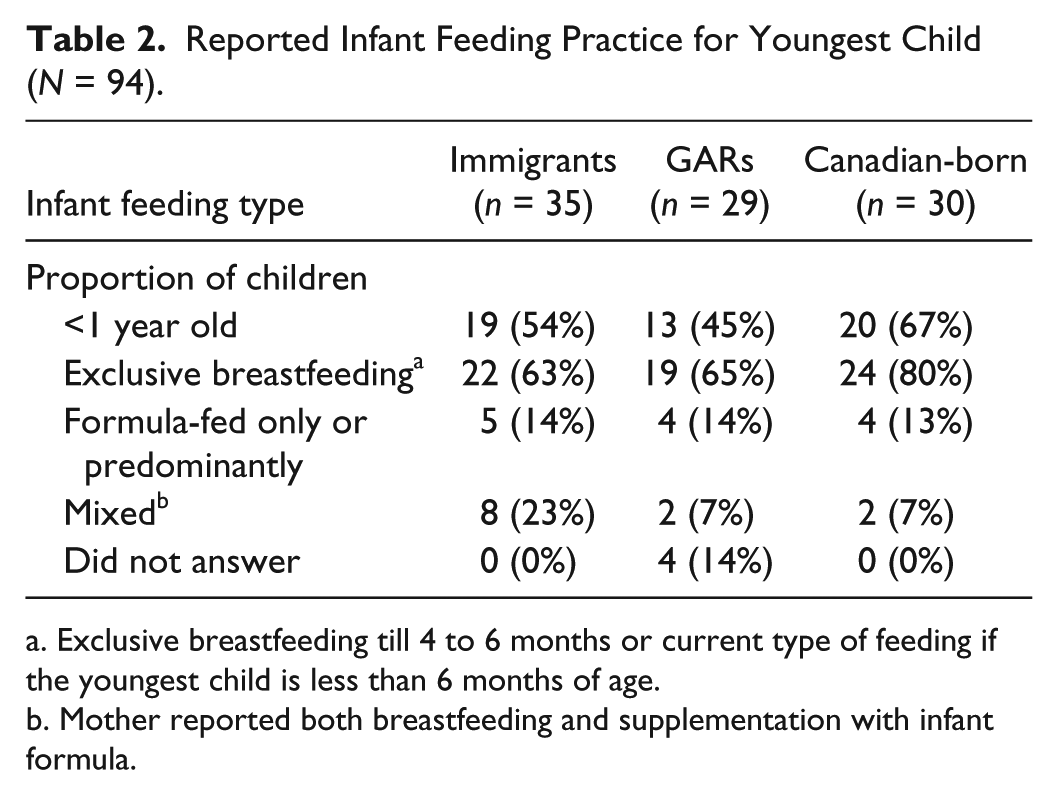
Exclusive breastfeeding till 4 to 6 months or current type of feeding if the youngest child is less than 6 months of age.
Mother reported both breastfeeding and supplementation with infant formula.
Reported Infant Vitamin D Supplementation Practice for Exclusively Breastfed or Mixed-Fed a Infants (Youngest Child; N = 77).
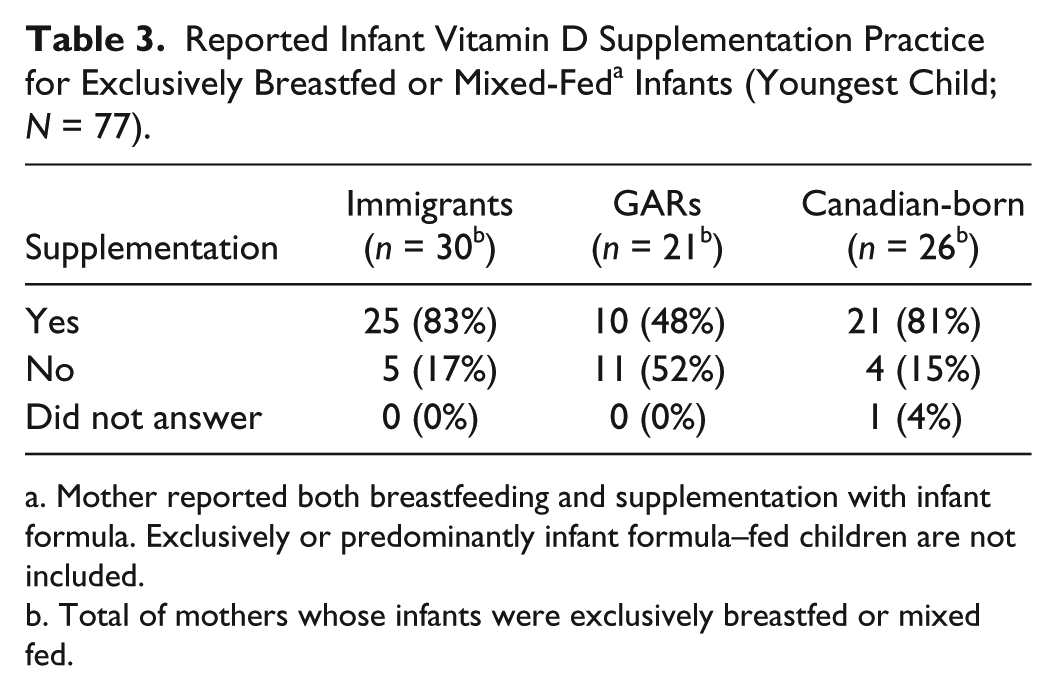
Mother reported both breastfeeding and supplementation with infant formula. Exclusively or predominantly infant formula–fed children are not included.
Total of mothers whose infants were exclusively breastfed or mixed fed.
Many Sudanese GAR mothers explained that they do not supplement children with vitamins before the age of 3 years and that giving young children vitamins is considered to be a sign of poor health. One woman phrased it this way: Back home we usually don’t take vitamins. If someone use vitamin or any medicine that means he’s very sick. That is the mentality for the people who come from there. You give them vitamins, that means they’re very sick, not like normal people who can support themselves and prevent themselves from the sickness. (Sudanese refugee)
While reported vitamin D supplementation was high for immigrant and Canadian-born mothers, there was much discussion about the challenges of infant supplementation. A few (4/25) immigrants and some (7/21) Canadian-born mothers who answered “yes” to the question about daily supplementation reported that they supplemented intermittently, started late (after 1 month), or stopped early (before 6 months postpartum). Discussion of supplementation practice revealed challenges such as forgetting to supplement—sometimes for days or weeks at a time—or difficulty getting an infant to swallow the whole 1-mL dose (with a dropper), as some spat the syrup back out. Others reported that using the dropper was easy and that their babies enjoyed the sweet taste. For those who used an alternative type of infant supplement (one drop as opposed to a 1-mL dose), the main concern was with dispensing the appropriate dose. Some mothers had difficulty discerning if the child had actually ingested the drop and were afraid of the potential ill effects of double dosing. See Table 4 for select quotes regarding the use of infant vitamin D supplementation.
Select Quotes a From Focus Group Interviews That Represent Findings From Each Topic in the Interview: Vitamin D Infant Supplement Use, Knowledge, and Sources of Information.
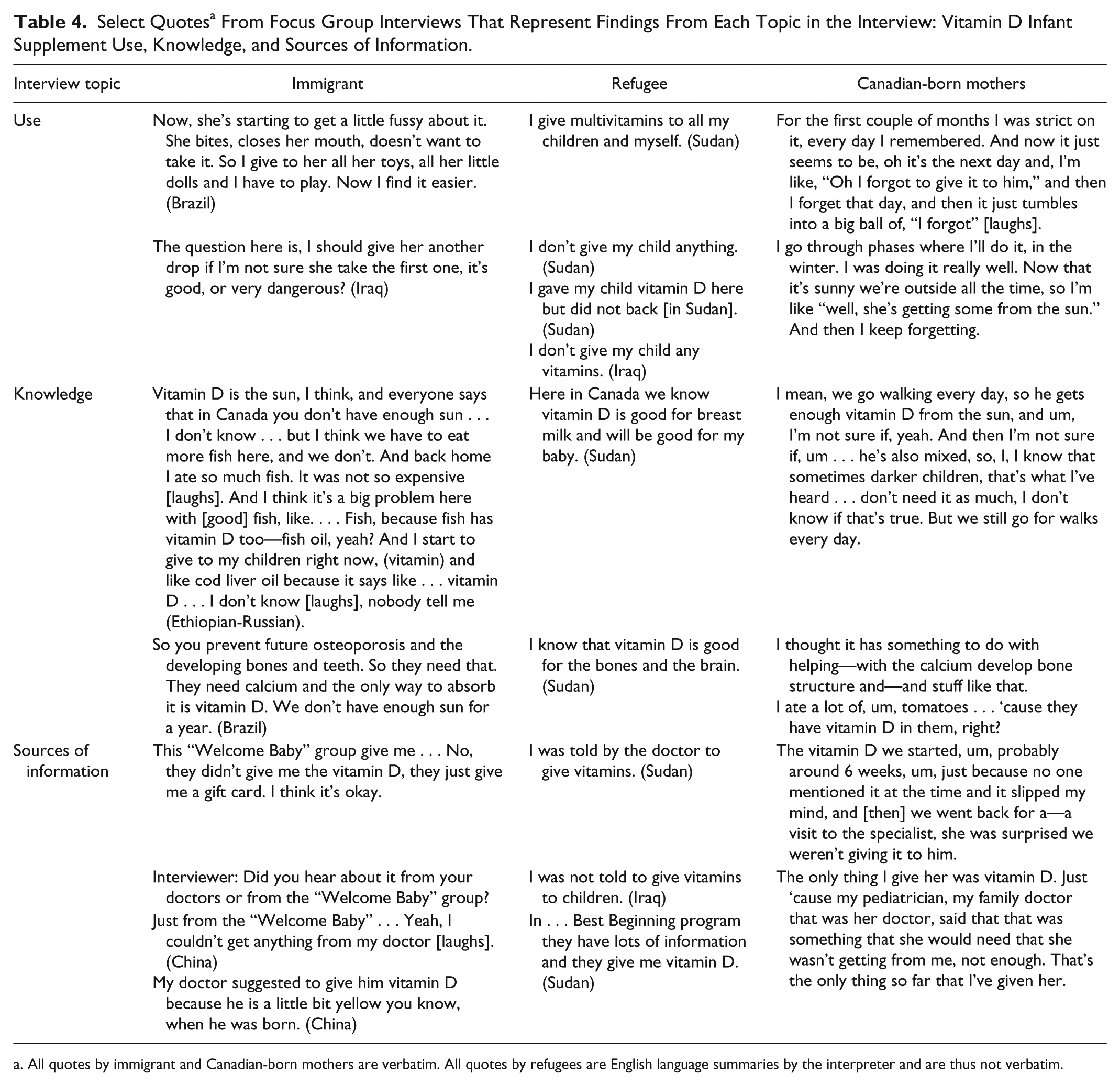
All quotes by immigrant and Canadian-born mothers are verbatim. All quotes by refugees are English language summaries by the interpreter and are thus not verbatim.
Knowledge
Although most mothers in the Central Canadian cities had heard of vitamin D as the “sunshine” vitamin, some of the specifics of consumption and synthesis were less well understood. Many knew that sun exposure is the best source of vitamin D, but they did not mention that at northern latitudes sun exposure during the winter was insufficient to produce vitamin D. Some immigrant mothers mistakenly believed that their babies could synthesize vitamin D from indoor sunlight exposure through window glass.
Most mothers connected vitamin D with good bone health. Mothers who were feeding their children infant formula correctly reported that they should not supplement, as infant formula is fortified with vitamin D. There was some confusion about which foods are good sources of vitamin D. For example, one Canadian-born mother said that she ate a lot of tomatoes when she was pregnant, as she believed tomatoes to be “a great source of vitamin D.” Many mothers correctly identified fortified milk as a source of vitamin D. They also mentioned other dairy products such as cheese as an additional source but erroneously since in Canada most dairy products, including cheese, are not made with vitamin D fortified milks (Calvo, Whiting, & Barton, 2004).
In comparison to the immigrants, GAR participants were most likely to say they did not know anything about vitamin D. New Canadians in both the Central and Western cities mentioned that they thought vitamin D was helpful in alleviating infant jaundice, “removing the yellow from the skin,” perhaps conflating this with light therapy used to treat infant jaundice. In all samples, both new Canadian and Canadian-born, some mothers were unsure of the age at which they should discontinue supplement use and whether older children needed vitamin D supplements. See Table 4 for select quotes regarding knowledge about vitamin D.
Sources of Information
Both new and Canadian-born participant mothers identified public health nurses and dietitians delivering education through prenatal programs as the most influential and frequently cited sources of vitamin D knowledge. This was indirectly corroborated by our observation that those who had not attended prenatal classes began supplementing later (one at 6 weeks, another at 9 months) or not at all. Many participants reported that the provision of samples or vouchers was helpful in encouraging supplementation. GAR mothers cited a variety of sources including doctors, nurses, and public health programs. The refugee health clinic gave GAR mothers free infant vitamin D supplements. New Canadians reported female relatives, particularly mothers and mothers-in-law, as the most important source of information about infant feeding but never mentioned them as sources of specific information on infant vitamin D supplementation.
There was a range of experience in terms of whether or not mothers were advised to supplement their exclusively breastfed infants with vitamin D. In five different focus groups, in all three cities, mothers reported that physicians’, midwives’, and maternity nurses’ advice about vitamin D supplementation was inconsistent. Three mothers stated independently (i.e., in separate focus groups and without prompting from the interviewer) that during their stay at the hospital after the birth of their child no one recommended them to supplement their exclusively breastfed infants. Similarly, four mothers independently stated that supplementation was not recommended at postnatal visits with their family physician and in one case a nurse. In the case of another mother, she heard nothing from the hospital or physician about vitamin D supplementation. Another mother stated that the nurse in the hospital where her child was born told her that there is no need for extra vitamins, since “the baby has normal weight and is eating well.”
Several mothers mentioned that they received different messages from various health care providers. The mixed messaging is evident in the following statement of one Canadian-born mother, who noted that although her previous doctor recommended vitamin D supplementation for her exclusively breastfed infant, her current doctor said she didn’t need any vitamin D supplements. She concluded by saying, “ . . . and the confusion within the medical society . . . confused me, and anytime I’m confused I just take a step back. So, we didn’t do any supplements.”
At the other end of the spectrum one mother stated that she was told to supplement her exclusively breastfed infant both in hospital and later by her health care provider: Yeah, we take vitamin D as well, or it’s tri-vi-sol which is three vitamins: D, A and C, I think. And that was something that the charge nurse actually told us when I was in the NICU. She actually gave me my letter of discharge and said go see your pediatrician immediately and they’ll probably tell you to go on vitamin D, you might as well buy it today. And the pediatrician said the exact same thing so. . . . I’m good at it; we do it every day without fail. And I still take the maternal vitamins as well. So I’m hoping that some of that gets through too. (Canadian-born participant)
When asked by the interviewer if mothers had any questions, two mothers independently asked about whether they should supplement their children more than 1 year of age with vitamin D. One woman explained that she had heard different recommendations: When my son was up to one year, they say until one year you give then you stop, then or when it’s summer. In the summer, there’s vitamin D. But now, there was one workshop and they were talking about it, and the nurse from public health, she said that the recent studies say until they’re at least eight or ten years old they have to take it every day. (Mexican immigrant)
See Table 4 for select quotes about sources of information for infant vitamin D supplementation.
Discussion and Conclusions
Non-refugee immigrant and Canadian-born mothers are mostly positive and proactive about supplementing their infants due, at least partly, to public health education delivered through prenatal classes. Excluding GARs there was little difference in reported vitamin D supplementation practices, knowledge, or beliefs between immigrant and Canadian-born mothers.
Taken together, these findings suggest that current public health education on vitamin D supplementation delivered by nurses, dieticians, and other health educators is similarly effective for Canadian- and non-Canadian-born parents. The positive response to infant vitamin D supplementation among immigrant and Canadian-born mothers may be explained by the fact that participants were recruited through early childhood centers, where they received public health education promoting infant vitamin D supplementation, and indeed that was their mostly frequently cited source of information. The lack of difference by parental origin concords with results of a recent quantitative survey in a Montreal maternity hospital, which found 98% and 88% vitamin D supplementation reported by women who were exclusive breastfeeding or mixed feeding, respectively, with no difference in supplementation practice between mothers born in or outside North America (Gallo, Jean-Philippe, Rodd, & Weiler, 2010). Information regarding supplementation of infants by health care providers, however, was inconsistent; this may in part be a reflection of current low levels of nutrition education in medical schools, as indicated by a U.S. study (Adams, Kohlmeier, & Zeisel, 2010) and the ongoing debates concerning vitamin D intake requirements (Gillie, 2011).
This study was designed to investigate some of the heterogeneity among newcomers. GARs stood out as unique, due to the more difficult circumstances they emigrated from and their more disadvantaged position in Canada relative to other newcomers. Many GAR mothers, and a high proportion of the Sudanese GAR participants, reported that they did not supplement their exclusively breastfed infants, even though supplements were provided free of charge to them. This contrasted with immigrant and Canadian-born reports and may have potential negative health implications if they and their infants are also likely to be vitamin D deficient. A vitamin D serum study among 1,217 refugee women and children attending the refugee clinic in the Western Canadian city found that 88% of women and 82% of children had low levels of vitamin D (<75 nmol/L), and 21% of women and 10% of children were deficient (<25 nmol/L; Aucoin, Weaver, Jones, & Thomas, 2011). Low infant supplementation practice among GARs in this study was concentrated among Sudanese mothers, who explicitly cited perceived social stigma about “vitamins” to explain why they did not supplement. Nevertheless, there may be other reasons such as lower levels of education and family income, as well as other competing and higher placed health priorities.
Focus group discussions revealed potential divergence in the likelihood of reporting or actually practicing supplementation. A number of mothers stated that they would forget for days or weeks at a stretch or had difficulty getting their infant to actually ingest the supplement. Mothers also reported difficulties with supplementation in the Montreal hospital study mentioned above (Gallo et al., 2010). Parental difficulties with supplementation suggest need for more “hands-on” instruction.
Maternal knowledge of food sources of vitamin D and synthesis from UVR was low for many mothers, despite knowledge of the importance of vitamin D infant supplementation, again similar to findings in the Montreal study (Gallo et al., 2010). Some mothers wanted information about supplementing children more than 1 year of age. Currently there are no vitamin D supplementation guidelines for this age group because previous dietary reference intake guidelines for vitamin D of 200 IU/day among all Canadian children more than 1 year of age led to a recommendation that they should not be supplemented with vitamin D (Roth, 2009). New guidelines may be needed, because the new dietary reference intake of 600 IU/day (Ross, Taylor, Yaktine, & Del Valle, 2010) likely cannot be achieved by diet alone (Vatanparast, Calvo, Green, & Whiting, 2010).
Limitations
These qualitative results about individual care-giver experiences must be interpreted with careful attention to limitations of sample size, recruitment bias, and potential reporting bias. The small, purposive sample was comprised of participants from the user groups accessing particular services at each participating organization. The practices of those who do not access such services may differ. Some focus group participants may have chosen not to participate as much, voice dissenting opinions, or honestly report their supplementation practices in front of others. There may have been inaccuracy in recall of infant feeding and supplementation practices; this was more likely for mothers whose youngest child was between 1 and 3 years of age at the time of interview (approximately half the sample). Unlike many studies of immigrants this study does not focus on one particular country of origin/region or ethnicity. Therefore, beyond the substantial number of Sudanese participants in the GAR sample, it is impossible to comment on how the context or cultural practices of a particular ethnic group would influence infant vitamin D supplement practice or knowledge.
Implications for Practice and Research
Canadian parents, whether native born or newcomers, would benefit from more detailed information about dietary sources of vitamin D and synthesis from sun exposure. They also require more clear and consistent messaging regarding infant supplementation and guidelines for vitamin D supplementation of older children from the various categories of health professionals working both in clinical facilities and in community-based public health outreach programs. Targeted and culturally competent knowledge translation and practical aid may be required to effectively deliver coordinated health messaging about vitamin D to GARs, a more vulnerable segment of the New Canadian population. More prevalence data and targeted research on supports and barriers for infant vitamin D supplementation among refugees would inform outreach program design.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for this research was provided by the Social Science and Humanities Research Council of Canada (SSHRC), Research Development Initiatives, Grant No. 820-2007-1052 and the Canada Research Chair Program.