
Abstract
Keywords
Introduction
Health care organizations are among the workplaces where bullying is a common phenomenon (Çamcı & Kutlu, 2011). Among health care professionals, nurses are more exposed to bullying than any other health care team member (Estryn-Behar et al., 2008; Quine, 1999, 2001; Rutherford & Rissel, 2004). In the literature, 20% to 44% of nurses are reported to have been subjected to bullying (Quine, 2001; Trepanier, Fernet, & Austin, 2013; Yıldırım, 2009).
The concept of bullying has been an international matter of concern for the past 20 years. When bullying was first identified, it was called as “mobbing” by Heinz Leymann (1996). He defined mobbing as psychological terror directed toward one individual by one or more persons in a systematic manner through hostile and unethical methods. In the nursing literature, generally mobbing is called bullying. Workplace bullying is defined as lateral or horizontal violence and currently attracts significant amount of international attention (Johnson, 2009).
Bullied victims’ mental health is significantly affected: Victims suffer serious psychiatric, psychosomatic, and psychosocial problems (Leymann, 1996). In a study by Yıldırım and Yıldırım (2007), those exposed to bullying were reported to suffer from stress, headaches, and fatigue. A study conducted with health care providers in New Zealand revealed that people who are exposed to bullying were under more strain and their well-being was adversely affected (Cooper-Thomas et al., 2013). In several studies of nurses exposed to bullying, they displayed severe symptoms of anxiety and depression (Quine, 2001; Sa & Fleming, 2008; Zapf, 1999). Employees exposed to bullying reportedly suffered mental fatigue and psychological distress and displayed more psychosomatic symptoms (Agervold & Mikkelsen, 2004; Mikkelsen & Einarsen, 2002).
Bullying has adverse effects not only on the health of employees but also on their work performance. Among bullied nurses, job satisfaction decreases, there is increased rates of sick leave and attrition, and there is decreased workplace productivity, satisfaction, and morale (Cleary, Hunt, & Horsfall, 2010; Quine, 2001). In a study conducted in Canada, nurses exposed to bullying had lower motivation and more intent to leave their jobs than did those who were not exposed to bullying (Trepanier et al., 2013).
In order to prevent and reduce bullying, it is important to know which nurses are at risk of these behaviors, who the perpetrators of bullying are, and how nurses react to bullying. In the literature, there are studies indicating that demographic variables pose a risk in terms of bullying. It is reported that young and inexperienced nurses are more exposed to bullying (Çevik Akyıl, Tan, Sarıtaş, & Altuntaş, 2012; Efe & Ayaz, 2010; Simons & Mawn, 2010; Yıldırım, 2009). On the other hand, some studies indicate that demographic variables do not pose any risk in terms of bullying (Mikkelsen & Einarsen, 2002; Yıldırım & Yıldırım, 2007).
It has been reported that perpetrators of bullying, a serious problem for nurses, are mostly other nurses. Several studies have reported that those who perpetrate bullying the most are head nurses, followed by physicians (Çevik Akyıl et al., 2012; Efe & Ayaz, 2010). In a study conducted in New Zealand, it was revealed that the majority of the nurses were exposed to bullying by senior and older nurses (Clendon & Walker, 2012).
The findings of several studies observed that although nurses’ mental health and work performance are adversely affected by the consequences of bullying, they prefer to remain silent and tend to share their discontent only with friends (Çevik Akyıl et al., 2012; Efe &Ayaz, 2010). Yıldırım and Yıldırım’s (2007) study indicates that nurses exposed to bullying try to avoid being bullied by working harder and more carefully.
Bullying in the workplace is a serious issue for nurses and needs immediate attention. Nurses are responsible for protecting and improving the health of society and of individuals, so they should be mentally healthy if they are to fulfill their duties and responsibilities as expected (Özgür, Gümüş, & Gürdağ, 2011). Organizations providing health care should make protecting the mental health of nurses a top priority. Studies on bullying have been increasing in recent years. However, the number of the studies on the rate Turkish nurses are exposed to bullying, how they react when they are exposed to bullying, who the perpetrators of bullying in the workplace are, and how the nurses’ mental health is affected by bullying is limited. The results of this study are expected to contribute to an understanding of the nature of bullying, its impact on nurses, and nurses’ reactions to bullying. In addition, these results can contribute to attempts to raise awareness of this issue, and to reduce and even prevent bullying in the workplace. The aim of this study is to determine variables affecting bullying, the rate of exposure of nurses to bullying, perpetrators of bullying, nurses’ reactions toward bullying, and the level of psychological distress of nurses exposed to bullying.
Research Questions
Method
Design and Sample
This descriptive study was conducted in 2013 on a sample of nurses working in a university hospital in Izmir, Turkey. Nurses at this 1,000-bed university hospital work 12-hour shifts for 180 hours a month and provide care for an average of 15 to 20 patients per shift. There are 757 nurses working in the hospital. The sample size was calculated to be 262 using a sample calculation formula in universally known situations (Sümbüloğlu & Sümbüloğlu, 2005). To increase reliability, more participants were needed. For this reason, all the nurses (N = 757) were invited to participate in the study; 284 nurses completed and returned the questionnaires. The participation rate was 37.5%.
Instruments
Nurse Information Form
This questionnaire included factors such as age, educational status, total years of service, years of service, and position at their current institution, all of which can affect bullying. In addition, in the questionnaire, the nurses were asked about the identities of their perpetrators and how they react to bullying.
Workplace Bullying Behaviors Scale
To measure the nurses’ perception of bullying in the workplace, a 33-item tool developed by Yıldırım and Yıldırım (2007) was used. The nurses were asked to mark the frequency of bullying behaviors that they had been exposed to within the last 12 months and which had negative effects on their work performance. The tool had four subcategories. Psychological violence in the workplace was discussed under four main headings: “isolation from work,” “attack on professional status,” “attack on personality,” and “direct attack”. The items were evaluated on a 6-point Likert-type scale ranging from 0 (I have never been exposed to this) to 5 (I am constantly exposed to this). The total score received was divided by the total number of items (total score = 33); the score over one showed that the employee had been intentionally exposed to psychologically violent behaviors. The tool’s original internal consistency was 0.93. It was 0.95 in this study.
General Health Questionnaire
The 12-item version of the General Health Questionnaire (GHQ-12) was developed by David Goldberg in 1972 to assess nurses’ psychological distress levels. The GHQ-12 is a scale surveying psychological distress observed within the last few weeks. The items were evaluated on a 4-point Likert-type scale. Scoring was as follows (a) and (b), 0 points; (c) and (d), 1 point; and the total possible score ranged between 0 and 12 points. A Turkish validity and reliability study of the questionnaire was conducted in 1996 by Kılıç. The tool’s internal consistency was 0.78 in Kılıç’s study. It was 0.91 in this present study.
Data Collection
The research team distributed the questionnaires to the nurses in the sample from May to July 2013. Each questionnaire included a cover page explaining the purposes and procedures of the study. The questionnaires were collected by the research team on completion.
Data Analysis
Statistical Package for the Social Sciences (SPSS) for Windows version 16.0 (SPSS Inc., Chicago, IL) was used to conduct the data analysis. In order to assess the relationship between the nurses’ sociodemographic characteristics and their exposure to bullying behaviors, chi-square analysis was used. When the nurses’ psychological distress scores were compared with their exposure to bullying, the data were analyzed using the Mann–Whitney U test, because they did not conform to the normal distribution.
Ethical Considerations
Ethical approval to conduct the study was obtained from the Ethical Committee of the Dokuz Eylül University Institute of Health Sciences (decision numbered 154 and dated March 3, 2011). The relevant university ethics committee approved this research. All the questionnaires were answered anonymously. A description of the survey provided the purpose of the study and clearly stated that the data would only be used for scientific exploration. Contact information was provided along with the questionnaire. The nurses were asked to seal the completed questionnaires in individual envelopes provided by the research team.
Results
The relationship between the sociodemographic characteristics of the nurses and their exposure to bullying behaviors is given in Table 1. Of the nurses, 97.5% were female, and 65.4% were married. The majority of respondents had a bachelor’s degree in nursing (83.3%). Most of the participants worked in intensive care units (30.6%). Of the nurses, 31.7% had 0 to 5 years of professional experience, whereas 29.2% had 16 or more years. Their mean age was 34.14 ± 7.69 years. There was a significant difference between the nurses in terms of the relationship between their education levels and their exposure to bullying behaviors. The factor that led to this difference was the mean score of nurses with master’s degrees. According to this study, these nurses were exposed to more bullying than the others. In terms of other variables (age, total years of service, years of service, and position at their current institution), no statistically significant difference was determined (p > .05).
Relationship Between Demographic Characteristics of the Nurses and Their Being Exposed Bullying (N = 284).
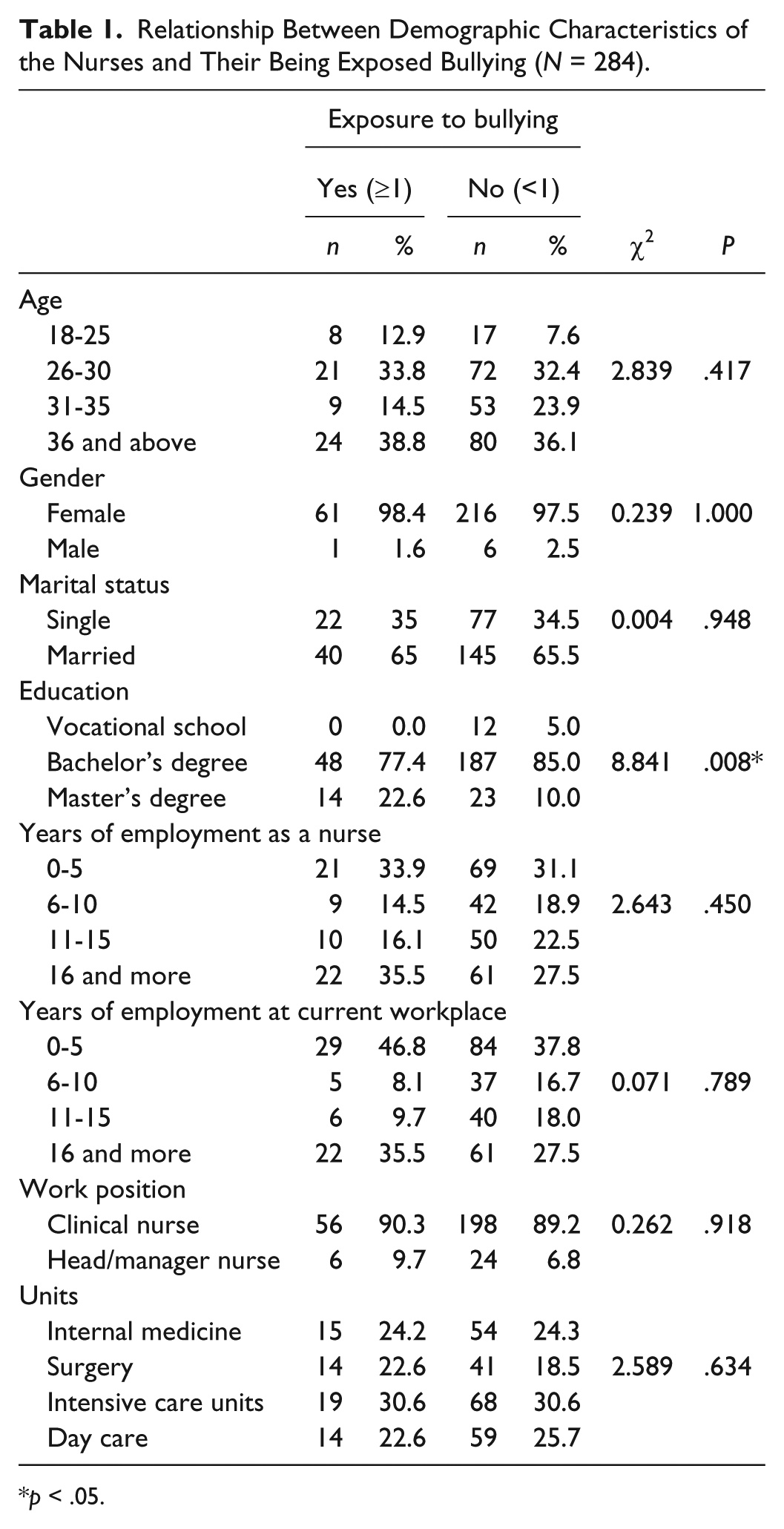
p < .05.
Table 2 shows exposure to bullying behaviors, perpetrators of bullying behaviors, and nurses’ reactions to bullying behaviors. Of all the nurses participating in the study, 21.8% were determined to have been exposed to bullying. Most of the bullying behaviors were perpetrated by head nurses (33.5%) and physicians (26.8%) followed by their peers (17.7%) and senior nurses (17.1%). The nurses reacted to bullying behaviors mostly by remaining silent (42.3%), sharing it with friends and family (32.4%), and/or overlooking the perpetrator’s behavior (30.6%).
Exposure to Bullying, Perpetrators of Bullying, Nurses’ Reactions to Bullying.
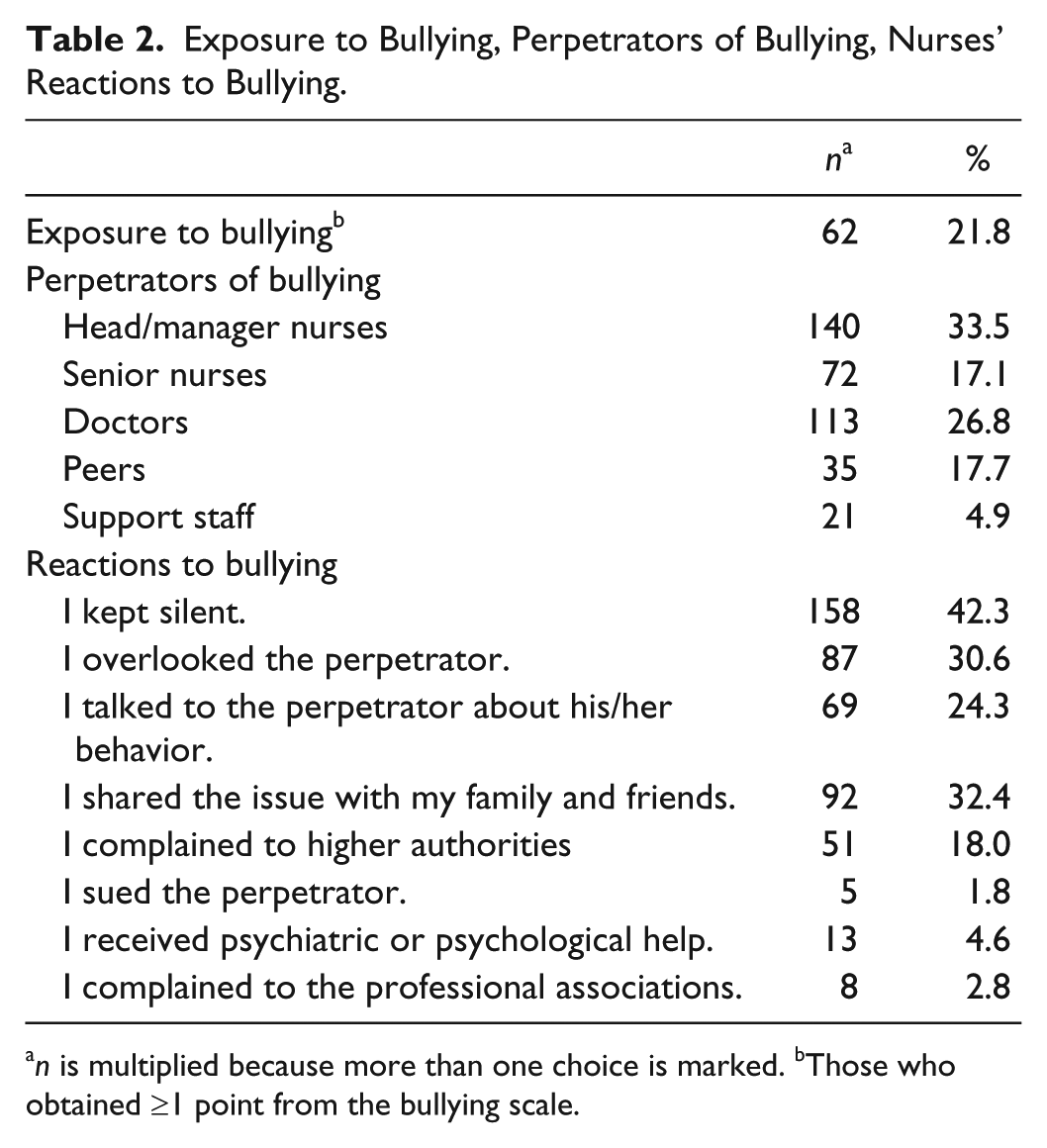
n is multiplied because more than one choice is marked. bThose who obtained ≥1 point from the bullying scale.
In Table 3, the nurses’ psychological distress scores are compared in terms of their exposure to bullying. It was determined that the psychological distress level of the nurses who were exposed to bullying was significantly higher than that of the nurses who were not exposed to bullying (p < .05).
Comparison of Nurses’ Psychological Distress Scores in Terms of Their Exposure to Bullying.
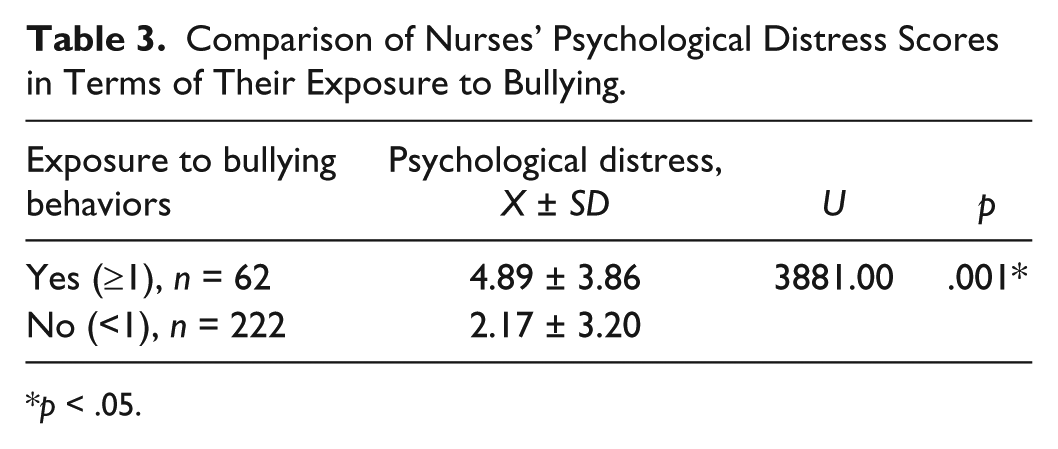
p < .05.
Discussion and Conclusions
Exposure to Bullying Behaviors in Terms of Demographic Variables
Comparison of exposure to bullying and demographic variables in this study revealed that the nurses with a higher level of education were exposed to more bullying; however, in terms of other variables, the difference was not statistically significant. In the literature, there are varying results regarding the relationship between exposure to bullying and demographic variables. Although some studies indicate that demographic variables have no effect on exposure to bullying (Mikkelsen & Einarsen, 2002; Yıldırım & Yıldırım, 2007), other studies indicate that being young and inexperienced poses a higher risk of being exposed to bullying (Çevik Akyıl et al., 2012; Efe & Ayaz, 2010; Yıldırım, 2009). In this study, the nurses with higher education were exposed to more bullying. According to Björkqvist (2001), the most important factor leading to bullying behaviors in the workplace is competition. In the university hospital where the study was conducted, the factor playing the most important role in promotion was a nurse’s education level. Therefore, nurses having higher education can be considered as more frequent targets of bullying.
Rate at Which Nurses Are Exposed to Bullying Behavior
In this study, 21.8% of the nurses were exposed to bullying behaviors. In the literature, the rate varies from one study to another. In one study (Quine, 2001), 44% of health care workers were exposed to bullying, whereas in another study (Yıldırım, 2009), 21% of the nurses were exposed to bullying. In Quine’s (1999) study, 38% of health care workers encountered bullying behaviors at least once within the last 12 months, and the perpetrators were mostly managers. In a study of nurses in Canada, 20.4% of nurses stated that they encountered negative behaviors in the workplace in the last 6 months (Trepanier et al., 2013). The results of this and other studies in the literature indicate that worldwide, nurses are at serious risk of being exposed to bullying behavior. These results confirm that bullying in the workplace is the foremost issue facing nurses.
Perpetrators of Bullying Behavior
In this study, most of the bullying behaviors were perpetrated by head nurses (33.5%) followed by physicians (26.8%), their peers (17.7%), and senior nurses (17.1%). The findings of this study are similar to those in the literature. In several studies, head nurses are reported to perpetrate bullying behaviors the most (Çevik Akyıl et al., 2012; Yıldırım & Yıldırım, 2007). According to Efe and Ayaz’s (2010) findings, nurses are subjected to bullying behaviors perpetrated by head nurses (25.2%) and physicians (19.4%). In Trepanier et al.’s (2013) study, the perpetrators were head nurses (37.3%), colleagues (27.1%), and physicians (16.9%). The results of these studies suggest that nurses are mostly exposed to bullying behaviors perpetrated by other nurses. Lateral and horizontal violence is a phenomenon on the agenda in the nursing literature. There are many different definitions of bullying but it can be broadly defined as nurse-on-nurse aggression, resulting in destructive behaviors of nurses against each other. It is stated that taking measures aimed at reducing violence in the workplace is of great importance (AbuAlRub & Al-Asmar, 2014). Therefore, if health care institutions are to improve nursing environment, patient care, and nurse retention, they should take necessary precautions (Embree & White, 2010).
Nurses’ Reactions to Bullying Behaviors
In this study, the nurses reacted to bullying behaviors mostly by keeping silent (42.3%), sharing the issue with friends and family (32.4%), and/or overlooking the perpetrator (30.6%). It is also reported in the literature that nurses react to bullying behaviors mostly either by keeping silent or by sharing the issue with friends (Çevik Akyıl et al., 2012; Efe & Ayaz, 2010). In a study by Yıldırım and Yıldırım (2007), nurses exposed to bullying tried to avoid it by working diligently. These results suggest that nurses try to deal with bullying using passive ways of defense. Therefore, for nurses to deal with bullying behaviors effectively, they should be supported by their organizations. To achieve this, these organizations should take precautions such as providing nurses with training on how to deal with bullying and having a no-tolerance policy toward the perpetrators of bullying or any other kind of psychological or physical violence.
Effects of Bullying Behaviors on Psychological Distress
In this study, nurses who were exposed to bullying behaviors had higher psychological distress levels than did the nurses who were not exposed. In the literature, it has been demonstrated that nurses exposed to bullying have significantly more symptoms of anxiety and depression (Quine, 2001, Sa & Fleming, 2008; Zapf, 1999). Compared with other job stressors, bullying is the leading cause of anxiety and depression (Hauge, Skogstad, & Einarsen, 2010). Nurses have the right to work in a healthy working environment. Nurses’ mental health status affects not only other nurses but also institutions and patients, because institutions cannot retain nurses, and patients cannot receive sufficient care. For the benefit of all, the mental health of nurses needs to be taken into account.
Limitations
This study has several limitations. One major limitation was the self-reported design, which holds the possibility of recall bias. A second limitation was nonresponse bias, which may have resulted in an underestimation of nurse exposure to bullying behaviors. Another related limitation was the cross-sectional design, which cannot determine causality. Thus, follow-up research is needed. The small size of the sample was another limitation, and finally, the participants of the sample were all from one single hospital. Therefore, the study results cannot be generalized.
Implications for Practice
Managers and policy makers of health care institutions should always keep in mind nurses’ high risk of exposure to bullying behaviors and that measures should be taken to support nurses. As long as nurses keep silent when they are exposed to bullying behaviors, this issue will not receive the attention it deserves but will remain in the background. Therefore, it would be beneficial to inform nurses about their rights, to create a positive atmosphere in health care institutions for nurses so that they can express themselves comfortably and to establish social support groups to help nurses exposed to bullying behavior.
Summary
In conclusion, it was determined that 21.8% of nurses encountered bullying behaviors in the workplace and that those with higher education were at a greater risk of being exposed to bullying behavior. The nurses were mostly exposed to bullying behaviors perpetrated by head nurses and physicians; unfortunately, the victims kept silent in most cases. In addition, nurses who were exposed to bullying behaviors had higher psychological distress levels than did the nurses who were not exposed to.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.