
Abstract
Keywords
Cardiac disease is the leading cause of death in Lebanon, accounting for 22% to 26% of total deaths in the country (Jabbour, Giacaman, Khawaja, & Nuwayhid, 2012; Ministry of Public Health Lebanon, 2012; World Health Organization [WHO], 2011). Self-care programs are observed by the WHO as vital for the primary and secondary prevention of noncommunicable diseases including cardiovascular (WHO, 2011). Self-care is defined by Orem (1985) as a dynamic process or an action system evidenced when individuals engage in actions to take care for themselves. Riegel et al. (2009) defined self-care “as a naturalistic decision-making process that patients use in the choice of behaviors that maintain physiological stability (symptom monitoring and treatment adherence) and the response to symptoms when they occur” (p. 1141). Dickson et al. (2013) maintained that the cardiovascular literature relate self-care to compliance with the recommended treatment regimen such as assuming healthy lifestyle, adherence to prescribed medications, and weight control.
Several studies documented the positive effect of supporting and promoting self-care behavior and assuming lifestyle changes on cardiovascular outcomes (Condon & McCarthy, 2006; Worcester, Stojcevski, Murphy, & Goble, 2003; Zavertnik, 2014). Secondary prevention efforts against cardiac illnesses that are effective in the West focused on interventions that enhance self-care; however, perception and attitudes toward self-care may not be the same among different cultures (Evangelista & Shinnick, 2008). Cultural values are known to influence patients’ understanding of their illnesses and the related therapeutic interventions (Webster, Thompson, & Mayou, 2002); consequently, adopting intervention programs aiming at self-care without examining their cultural relevance and appropriateness may not be effective.
Limited research addressed cultural influences on patients’ self-care behaviors; studies that did rarely focused on cardiac patients. Thus, more research is needed to come up with culturally sensitive cardiac self-care interventions (Dickson et al., 2013). Kreuter, Lukwago, Bucholtz, Clark, and Sanders-Thompson (2003) maintained that factors such as beliefs, individualism, collectivism, familial roles, and spirituality might be associated with health-related behaviors recommending that health educators identify cultural factors within a particular population and integrate them in interventions aiming at changing behaviors. Voyer, Rail, Laberge, and Purnell (2005) found that perceptions about adherence to medical regimens differed considerably among cultural groups of women. The authors contended that nurses must incorporate such cultural differences when teaching their patients. In a study about power and self-care in women living in urban settlements in Pakistan, Lee (1999) indicated socioeconomic variables, ethnicity, and roles as predictors of power perception, enabling self-care agency, and self-care; it is worth noting that roles are determined by cultural values. In a study using focus group interviews to explore beliefs about health and diabetes in 35 men of different ethnicities in Sweden, the findings revealed that Arabs particularly depended on health care professionals, whereas Swedes were more likely to use independent self-care measures (Hjelm, Bard, Nyberg, & Apelqvist, 2005).
The “patient as the expert” approach is advocated by the WHO (2011). Patients’ perceptions of their illnesses and their roles in self-care need to be addressed to incorporate cultural values in their care. Zambroski (2003) and Clark (2003) claimed that most of the literature addressing self-management of cardiac illness has been framed from the viewpoint of health professionals rather than patients. Moreover, Kralik, Koch, Price, and Howard (2004), in a qualitative study of patients with arthritis, found that the health professionals’ views of self-management differed from those of the patients. Thus, to meet patients’ needs more effectively, their perspectives ought to be examined.
Kim and Flaskerud (2008) described the influence of culture as a basis for understanding and responding to disease; thus, the importance of considering cultural differences in sick role expectations. For example, cultural beliefs such as those relating sickness to God’s will and fate influence the sick role expectations of patients. Such cultural attitudes encourage interdependence and collective decision making in matters of illness response and adaptation to the sick role (Kim & Flaskerud, 2008). How the sick role would affect self-care behaviors is unclear and whether this concept exists among Lebanese cardiac patients is unknown. This area is worth exploring in the Lebanese, where families may encourage sick role behavior (Deyirmenjian, Karam, & Salameh, 2006; Meleis & Hattar-Pollara, 1995), thus affecting self-care practices. Such information can be used by nurses for designing culturally sensitive interventions with their cardiac patients to equip them and their families with relevant knowledge and skills needed for self-care.
In Lebanon, family and relatives accompany patients during admission and hospitalization to alleviate the patients’ fears and worries and sometimes to answer questions on behalf of the patients (Adib & Mikkey, 2003). Deyirmenjian et al. (2006) reported that Lebanese patients assume passive-recipient roles. Family members assume the role of not only caregiving but also making decisions on behalf of the patient. Gebara and Tashijian (2006), describing end-of-life practices in Lebanon emphasized the involvement of family in patient care making the family a principal element in the communication protocol. The authors inferred that the Lebanese culture is family-oriented, whereby family members support each other in all aspects of life including health care and are required to preserve family values (Gebara & Tashijian, 2006).
Despite the prevalence of cardiovascular disease in Lebanon, no research has addressed cardiac self-care in the Lebanese cardiac population. A thorough understanding of patients’ perceptions of their cardiac illness and related self-care is critical to the development of secondary prevention programs tailored to their needs. Therefore, the purpose of this study was to explore perceptions of cardiac illness and self-care among Lebanese cardiac patients.
Method
Design and Sample
This study used a qualitative descriptive design to explore cardiac patients’ perceptions of their illness and the meaning they ascribe to self-care. Semistructured individual interviews with a sample of Lebanese cardiac patients were used. This design was selected to gain culturally relevant descriptions of cardiac illness and self-care from the perspective of participants (Denscombe, 2003, Sandelowski, 2000). Fifteen patients were recruited from the private cardiology clinics of a referral university medical center in Beirut the capital of Lebanon. Patients’ inclusion criteria included age over 30 years and diagnosed with coronary artery disease (CAD) for over a year. Purposive sampling was used to obtain cases deemed information-rich (Sandelowski, Barroso, & Voils, 2007). Participants varied by gender, socioeconomic status, educational level, religion (Christian, Muslim), and area of residence (urban, suburban, rural). With respect to religion, Christian patients in the sample belonged either to the Maronite/Catholic sect, the Eastern Orthodox sect, or the Protestant sect; Muslims were Sunni, Shiite, or Druze. This purposive variation allowed discovery of the unique perceptions of cardiac illness and self-care among Lebanese cardiac patients and provided sufficient information to achieve data saturation.
Procedure
After securing study approval by the Institutional Review Board of the university and its medical center, patients were recruited from the cardiology clinics. Those who agreed to participate in the study signed informed consent and were individually interviewed through semi-structured digitally audio-recorded interviews. Interviews lasted 40 to 60 minutes and were conducted in a location determined by the participants. Most were interviewed in their homes although two were interviewed in the researcher’s office. The primary investigator and first author conducted all the interviews in Arabic. Interview questions were open-ended, developed by the primary investigator (the first author), and evaluated for cultural congruence by three experts familiar with the culture. The questions were translated into Arabic and back translated into English by an independent person blinded to the original English form. Interview questions are provided in Table 1. Interviews and field notes were transcribed using the Arabic language. Then patterns were extracted and translated into English, then back translated into Arabic by a graduate nurse blinded to the original transcripts and fluent in both languages. All audio-recordings, transcriptions, and related documents were kept in a password protected personal computer.
Interview Questions.

Data Analysis
Qualitative descriptive analysis was used to summarize the data using data-driven codes, identifying patterns, categories, and themes (Creswell, 1998; Sandelowski, 2000) pertaining to cardiac illness and self-care perceptions. Trustworthiness was enhanced through immersion in the data prior to its analysis to assure the findings reflected the meanings expressed by the participants. Member checking was used to validate the findings and their interpretations. The co-authors participated in the analysis appraisal, construction, and explication of the themes.
Results
All 15 participants were native Lebanese, with a mean age of 62 years; 12 (80%) were married and 7 (46.6%) had intermediate school education or higher. About 9 (60%) lived in urban areas, and four (26.6%) resided in the suburbs, a distribution quite representative of the population in Lebanon. About half of the participants (7) were housewives. Occupation of the men ranged from semiskilled jobs to business. All participants were diagnosed with CAD for over 3 years with 11 (73.33%) diagnosed 5 to 7 years ago; some underwent open heart surgery and others angioplasty.
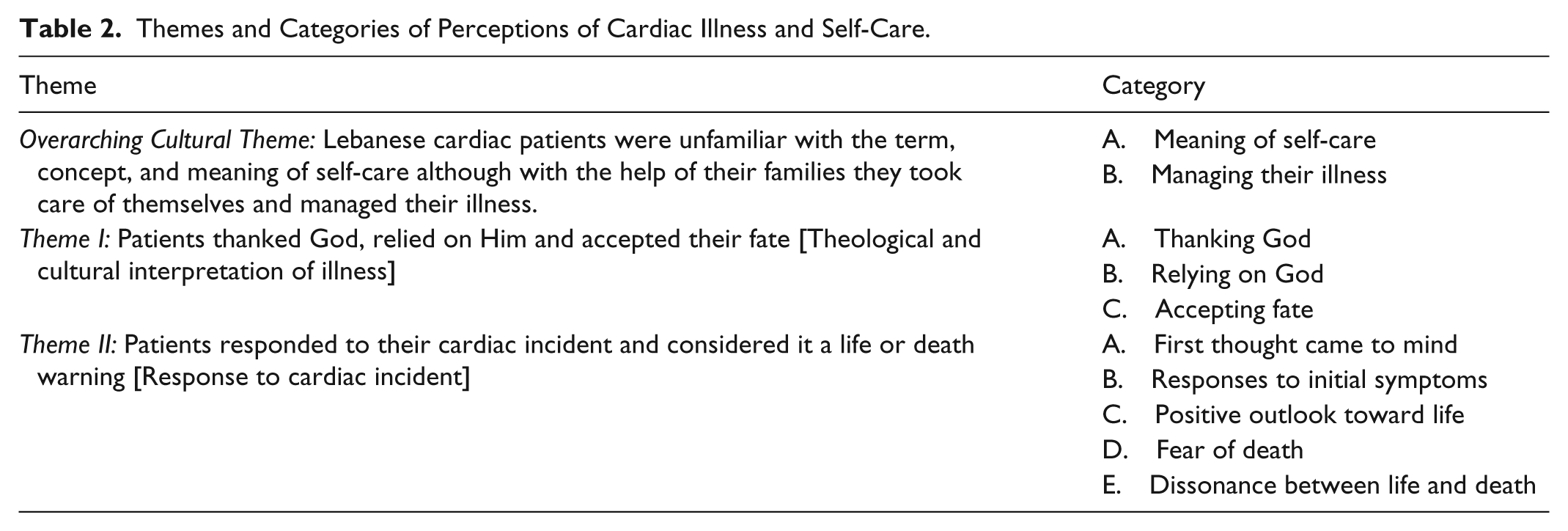
The analysis yielded one overarching and two additional themes (Table 2). The overarching theme was that Lebanese cardiac patients were unfamiliar with the term concept and meaning of self-care, although with the help of their families they took care of themselves and managed their illness. The additional themes were (a) patients thanked God, relied on Him, and accepted their fate; and (b) patients considered their cardiac incident a life or death warning. To protect participant privacy, names or pseudo-names are not used in the descriptions of the themes and quotes from the interviews. Arabic words are italicized and Arabic phrases are included for native speakers when direct translation could not convey the true meaning.
Themes and Categories of Perceptions of Cardiac Illness and Self-Care.
The Overarching Theme
Lebanese cardiac patients were unfamiliar with the term concept and meaning of self-care, although with the help of their families they took care of themselves and managed their illness. At first query, most participants had no recognition of the term self-care (in Arabic Inaya Bilnafes “ألعناية بالنفس”). They reported unfamiliarity with the term, confusing it with psychological well-being because of the close enunciation of the terms self and psyche in Arabic. When asked what such a term might mean, responses varied. Several participants responded: “Does it mean (care for self) psychologically?” Others questioned, “Do you mean we need psychological care?” As the term was clarified, several participants commented that a person is his/her own “doctor” meaning one who provides remedy with wisdom. Some explained that one should have strong will, depending on his mind—not “heart” to be that doctor.
When asked how they take care of themselves, a number of participants used a different expression for self-care than that translated by the research team. The term used could be translated into mind manage self (in Arabic “yedeer belo a halo”“يدير بالو عحالو”). Several participants thought managing their illness meant taking medications, paying attention to oneself, taking care of one’s life, not exerting effort or getting exhausted, and following dietary regimen and doctor’s instructions. One participant insisted that self-care is restricted to the sick. Other practices less frequently reported related to observing physical activity and rest, using protective measures, and setting self-care goals. Avoiding Za’al
In describing their self-care practices, some participants said “I depend on myself.” However, some expressed having support from family members such as helping in administering their medications, accompanying them to the doctor’s clinic, and relying on their wives for preparing the prescribed meals. Most participants said decisions about major procedures such as open heart surgery or angioplasty were made in consultation with the family; they reported that involving family members in their care and related decisions is expected.
To conclude the overarching theme, although self-care as a concept is not clear in the culture, Lebanese patients performed self-care practices with family involvement. The following themes further clarify perceptions of cardiac illness and its implications.
Theme I
Patients thanked God, relied on Him, and accepted their fate. Participants interpreted their cardiac illness through a theological lens. They thanked God for being saved, relied on Him for their lives, and accepted their fate as written by God. Muslims and Christians expressed these ideas unanimously. Several participants repeatedly thanked God during their interviews; several added phrases of faith assertion and praises such as “we believe in Him,” “praise to God,” and “thank God.”
The relationship of God and fate to cardiac illness is represented by this statement made by a 67-year-old Muslim woman diagnosed with CAD for 5 years: “If it isn’t what you want, then want what it is. In spite of yourself you have to accept circumstances because you cannot get away from what God has written.”
Participants thanked God for having their surgery and considered that the procedure helped them resume their ordinary lives. A 68-year-old Muslim female diagnosed with CAD for 20 years said, “They did the operation in my chest and thank God I can carry on, work at home. Thank God I became better.” Another 67-year-old Christian female diagnosed 10 years ago with CAD expressed her gratitude to God and Saint Elie for her surgery that made her feel better. Similarly, a 73-year-old Christian male participant diagnosed with CAD for 7 years expressed gratitude to God stating: “No doubt having a heart problem in a human being’s life, the human being has to accept and thank God for it.”
Participants expressed their reliance on God and trust in Him for their lives, their health, and cure, for giving them the courage to go on with their lives, and guiding their way. A 63-year-old Muslim female participant diagnosed with CAD 7 years ago conveyed her belief in God and dependence on Him to take care of her matters [troubles and concerns]. She maintained: I gave up, there is no way, gave my matters to God. We believe that we will die like all beings . . . that is why a human being has to be realistic and will have his return [reward] by patience.
Some participants considered their illness to be fate predetermined by God. Participants believed that each human being has a share [kismet] in life that God decides. While praising Allah (God), patients expressed their belief that this is their destiny; to them God heals whomever He wants to heal: “Thank God as we believe in God we believe that this is written for us . . . Fate you have to succumb for the circumstances” one said. Participants believed their length of life is predetermined by God, and if it is their fate to die then they will. A 51-year-old Muslim participant diagnosed with CAD 5 years ago compared two individual situations saying “one will not die until his age is over, another, walking, drops alone, [and] falls on the floor, just like that, he’s not sick, nothing is wrong with him, his life is over.”
This theme represents the theological interpretation of heart disease that participants used to help them cope with their illness; their perception of cardiac illness is inseparable from their belief and faith. The strong reliance on God is embedded in the Lebanese culture and transcends religious affiliation, as these participants represented diverse backgrounds. Their gratitude to God and reliance on Him for their health was a common cultural pattern consistent with Lebanese culture and language.
Theme II
Patients considered their cardiac incident a life or death warning; they considered their heart problem a warning to change their outlook toward their health. Their views of their cardiac illness varied between a positive outlook toward life and fear of death. Some participants responded to their cardiac illness with a positive outlook toward life. Participants regarded what happened to them as a warning to wake up and start a new life by taking care of themselves. A 47-year-old Muslim participant diagnosed with CAD 7 years ago described his new outlook toward life in this way: This feeling made me sense the value of life, value age which is not for waste, not a game. . . . I used to go to work, do my job but (was) not satisfied with it, not that it is laziness or something, but I did not feel the joy of work. After this thing [cardiac incident] I feel myself I am here, I exist, I am producing, I am able to help. It gave me new motive that today is a new day, today I will give, today is better than the day before, you feel the value of life, after this incident the work is still the same, but the thinking about the work is different. You feel pleasure, you are still carrying on but better, knowing where is the wrong in you and fixing it.
Fear of death was the first feeling experienced when the symptoms started. Some participants described their feelings of fear when they were told that they had cardiac disease. A 51-year-old Muslim male participant diagnosed with CAD 5 years ago claimed that dying was the first thought he had, “I was gone and then came back . . . I was afraid, afraid that I have the heart [disease] . . . First thing came to my mind is the idea of death.”
Participants expressed the significance of the heart as a source of life and death. A 73-year-old Christian participant expressed living in dissonance between life and death at times due to his experience. He said, I look at the mirror and laugh and say: is it possible that this desiring self inside me is wearing this shattered body? The body is not able to satisfy the needs of the desiring self which is still in me yearning for the love of life.
To these patients, cardiac incidents engendered fear of death. Being saved from a cardiac incident, on the other hand, brought new hopes and generated a new outlook toward life.
Discussion
The findings of this research provide in-depth insight into the Lebanese cardiac patients’ perceptions of their illness and its related self-care. The participants were unfamiliar with the concept and meaning of self-care. They did not recognize the term self-care and considered it psychological care because of the similar words used for “self” and “psyche” in the Arabic language. Although self-care behaviors existed among these Lebanese cardiac patients, the concept itself did not exist. Furthermore, the meaning given to self-care is different from the definition used by health care professionals, showing a discrepancy in perceptions of patients versus health care providers. Results of this study suggest that the term mind manage self is a more meaningful expression than self-care for Lebanese cardiac patients.
The unfamiliarity and confusion with the term self-care may not only relate to language interpretation. Perhaps the cultural meaning of the term self reflects an “individual” as opposed to a “collective being” perspective, where self exists as a member of the family. The meaning given to “self” and how it relates to individual/personal care versus collective care provided by patient and family needs further exploration. This notion also has implications for health care providers who follow the Western model of health care that assumes self-care is performed independently by individuals, rather than by families.
Nakkash et al. (2003) have identified Za’al as a barrier to healthy lifestyle in their study that tested the “feasibility of a community-based prevention program in reducing the prevalence of cardiovascular risk factors” (p. 725). Similarly, in this study, participants identified avoiding za’al as a facilitator to or a self-care behavior. Participants thanked God continuously as they were describing their heart disease. It is common knowledge among the Lebanese that thanking God during any kind of social conversation such as birth, success, wedding, buying a car, and even death, is a norm and a common Lebanese pattern irrespective of religious sect. This pattern is intensified during stressful situations and is usually accompanied by prayers. Participants of all faiths in this study thanked God for facilitating their surgery or angioplasty, saving their lives, and for being able to carry on with their lives. Relying on God is based in the patients’ beliefs that whatever they are going through is “meant to be,” destined, and “written” by God. They believe each human being has his/her share of life’s good and bad. These findings concur with those of a study of Hindu cardiac patients in the United Kingdom (Webster et al., 2002).
The faith of these patients could be a source of coping with their disease, a resource to manage their needs and face the stress of their illness. Faith was shown to be effective in modifying psychosocial stress associated with cardiovascular disease in a review of the impact of stress on cardiovascular health (Das & O’Keefe, 2006). It is noteworthy to mention that participants in this study referred to fate or destiny when describing their lifestyles, a factor that might affect behavior modification efforts. Faith, as a potential resource, could be promoted effectively by health care providers as a coping mechanism. However, the concept of faith and its effect on the perception of cardiac illness needs further investigation.
Most patients did not interpret their initial symptoms as heart problems, but rather thought that they were caused by various conditions such as the flu or indigestion, and so the actions they took when they had the symptoms varied. The symptom interpretation and actions taken concur with the findings by Henriksson, Lindahl, and Larsson (2007); Kristofferzon, Lofmark, and Carlsson (2007); and Noureddine et al. (2006). Patients at the first incident delayed initiating treatment promptly, similar to the findings of two studies of Lebanese cardiac patients (Noureddine et al., 2006; Sawaya et al., 2000). These findings suggest the need for awareness campaigns among the general population regarding symptoms of heart disease.
Participants interpreted their cardiac incident as a wakeup call or warning to start taking care of their health. Some reported a change in their outlook toward life and, as a consequence, took responsibility for changing their lifeways. This finding concurs with Bergman and Bertero (2001), who reported that the disease gave their subjects a new perspective on life. Similarly, “life style warning sign” emerged as a major theme in a study of myocardial infarction patients (Condon & McCarthy, 2006). Conversely, and as found by others (Condon & McCarthy, 2006), some participants in the current study associated cardiac illness with death, a perception they held even prior to getting sick themselves.
Several participants demonstrated dissonance between life and death, oscillating between their acceptance of destined death because of a heart incident and hope for living longer. They expressed their yearning for life yet at the same time felt their bodies were weakening and unable to fully satisfy their desiring selves. The yearning that motivated self-care was also reported by Kristofferzon et al. (2007), whose participants tried “to increase their zest for life” thus making lifestyle changes. Being given another chance for living, patients seemed to embrace their future with a sense of faith and hope based on self-determination that they are “going to make it this time.”
Implications for Research, Practice, and Education
Results of this investigation have implications for nursing research, practice, and education. Further research is needed on the following: (a) the extent to which faith affects self-care practices and the stress experience in this population; (b) factors affecting patients’ responses to cardiac symptoms; and (c) the influence of the family on cardiac self-care. Perceptions and roles of Lebanese health care providers is another area worth studying.
Nursing practice implications include utilization of these findings in planning self-care interventions for cardiac patients. Nurses ought to be careful in using the term self-care with Lebanese cardiac patients, since it is not a common concept in the Lebanese culture and cardiac patients may interpret it differently. In situations where the nurses are obliged to address self-care in patient teaching, they need to make sure patients understand what is meant by it.
Implications for nursing education include the need to disseminate research findings pertaining to cardiac self-care and to train students to use these findings effectively in practice. Nursing faculty ought to guide their students to integrate research findings when planning culturally appropriate care for cardiac patients especially in patient teaching.
Conclusion
In this study the perception of cardiac illness and the meaning of self-care in Lebanese cardiac patients are explored. One limitation is the translation of patterns from Arabic to English, resulting in some loss of meaning in translation. However, back translation by a nurse fluent in both languages and blinded to the study and initial translation promoted the credibility of findings. Moreover, the nature of the study necessitated patients’ dependence on their memory to describe their responses to cardiac illness. Nevertheless, the credibility of the study findings was enhanced by the participants’ rich verbatim quotes and member checking.
In conclusion, this research clarified the concept of self-care as mind managing illness and provided patient perceptions of cardiac illness. Health care providers need to integrate patients’ perceptions in any cardiac self-care intervention to achieve better health care outcomes.
Footnotes
Acknowledgements
We acknowledge Dr. Samar Noureddine for her valuable revision of the article and Ms. Sarah Abboud for the back translation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.