
Abstract
Keywords
Each year, 3.4 billion people, half the world’s population, live at risk for malaria (World Health Organization [WHO], 2014c). Malaria invades and infects 287 million and, of the 1 million who die, 90% are children younger than 5 years in sub-Saharan Africa (WHO, 2014c). Malaria has a massive economic impact with an estimated $12 billion in lost productivity in Africa alone in 2011 (Nothing But Nets, 2012). This economic burden leads to the cycle of poverty (Centers for Disease Control and Prevention [CDC], 2012). Malaria remains in the top 10 causes of sickness and death in developing, low-income countries (WHO, 2014b). Eighty percent of all malaria cases occur in 17 African countries; one is Kenya, where 76% of the population lives at risk (U.S. Agency for International Development [USAID], 2013; President’s Malaria Initiative [PMI], 2014).
Background and Review of Literature
Malaria is a single-celled, parasitic tropical disease with a complicated cycle that involves a human host, a female Anopheles mosquito vector, and the environment (National Institute of Allergy and Infectious Diseases [NIAID], 2008; WHO, 2014b). Symptoms include a cold stage (chills, shivering), a hot stage (fever, headaches, nausea, vomiting), and a sweating stage (return to normal temperature, malaise) (CDC, 2012). Malaria can be uncomplicated or severe and is curable if diagnosed promptly and treated correctly.
Plasmodium falciparum, the leading species that causes severe infections and death, accounts for 85% of malaria in Kenya (PMI, 2014). Although malaria is preventable and curable, all of Maasailand, Kenya remains at risk (Kenya National Bureau of Statistics, 2011). Malaria care, in any culture, is multifaceted. Even those who use the best prevention measures can sometimes contract the disease. Thus, knowledge and use of prevention measures and appropriate care to minimize consequences for active disease are important for malaria care.
The global burden of malaria has regained a prominent research platform. The PMI (2014) and CDC (2014) support four interventions to prevent and treat malaria: insecticide-treated nets (ITN), indoor residual room spray with insecticides (IRS), intermittent preventive treatment for pregnant women (IPTp), and prompt treatment with artemisinin-based combination therapy (ACT). Research findings are unanimous that ITN use effectively decreases malaria incidence and malaria care education is needed for at-risk populations (CDC, 2014). WHO (2014a) recommends that all pregnant women and children younger than 5 years who live in risk areas sleep under ITN.
The Maasai people live in sub-Saharan Africa where malaria is endemic. Their pastoral, indigenous lifestyle places Maasai men, women, and children at risk daily. Although some prevention and treatment measures may be available, the Maasai community continues to uphold strong ties to traditional lifeways. The use of generic and professional malaria care within their culture is largely unknown. After an extensive literature review, only five related studies were found: one ethnographic study that examined malaria and included Tanzanian Maasai pastoralists (Malisa & Ndukai, 2009); one study that looked at Maasai attitudes toward health care, which included malaria care (Wanzala, Hassanali, Kibet, & Dossajee, 2005); and three ethnobotanical studies that focused on use of herbs for malaria care among Maasai (Bussmann et al., 2006; Kigondu et al., 2011; Koch, Tamez, Pezzuto, & Soejarto, 2005). No studies were found that explored Kenyan Maasai use of known professional prevention and treatment modalities, or why morbidity and mortality have not decreased in the region. Therefore, the beliefs and practices of malaria care within the Maasai culture are virtually unrecorded. This study focused on discovery of malaria care among Maasai who live in Kenya’s Kimana region.
Domain of Inquiry, Purpose, and Goal
The domain of inquiry (DOI) for this transcultural, ethnonursing study was culturally congruent malaria care (CCMC) among the Maasai people. This was an in-depth examination of ethnohistory and culture of the Maasai relevant to malaria care. Over the past 26 years, the researcher worked with, offered community health care to, and observed the consequences of malaria in Maasailand. Current global malaria care initiatives were not evident in the Maasai culture. The researcher speculated that a purposeful focus on the culture and malaria care of the Maasai could guide implications to benefit the health of this population.
The purpose of this qualitative study was to discover, describe, and systematically analyze the meanings, expressions, and practices related to malaria care among the Maasai who reside in the Kisongo Maasai villages in the Kimana region of Southern Kenya. The goal was to discover the emic (generic/traditional) and etic (professional nursing) care practices to make recommendations that promote CCMC for the Maasai. CCMC is defined as care that is safe, beneficial, and fits with people’s daily lives (McFarland & Wehbe-Alamah, 2015). This study used four primary research questions (Table 1).
Primary Research Questions Used to Guide Study.
Ethnohistory
The Maasai are a proud African people group who live in the rural sub-Saharan environment of Kenya and Tanzania. These seminomadic people value their families and animal herds, traditional dress, handcrafted beaded jewelry, decorated ear piercings, life passage ceremonies, home design, stories, language, and traditional health care practices. Their language of Maa is oral and their history and traditions have been passed through the generations orally (Hodgson, 2011). Their worldview is a holistic, monotheistic perspective, which views community as integrated with and inseparable from the natural environment. Physical, mental, and spiritual realms are interconnected and death is a natural part of life; decisions are made for the good of the whole community. In many lifeways, the Maasai continue to live as they have for thousands of years: herding sheep, goats, and cattle; migrating with the rains that provide grass for grazing; searching daily for water and firewood; and continuing unique cultural traditions (Saitoti & Beckwith, 1980; Strang, 2014). One unwelcome lifeway is the inevitable suffering caused by malaria and the need for care. Professional malaria care and preventive measures remain unfamiliar and often unavailable in Maasailand. This study was essential to build on the known scholarly works, in the quest to offer Maasai CCMC. For this study, malaria care referred to any cultural, indigenous, folk, or professional meanings, expressions, or practices related to the treatment, recovery, prevention, and/or long-term consequences of malaria within individuals or the community as a whole (Strang, 2014).
Theoretical Framework and Method
The theory of Cultural Care Diversity and Universality [CCT] (McFarland & Wehbe-Alamah, 2015) was selected as this study’s theoretical framework because of its foundational premise that “people of different cultures can inform and are capable of guiding professionals to receive the kind of care they desire or need” (McFarland, 2010, p. 459). The CCT contends that specific care needs are an essential human need, essential to nursing, dependent on the patient’s unique cultural backgrounds, and can lead to participation in health management when culturally relevant care is offered (McFarland & Wehbe-Alamah, 2015; Ray, 2010). The CCT goal is that findings are used to establish a body of knowledge to guide transcultural nursing decisions and actions that promote culturally congruent, safe, responsible, and beneficial malaria care (Wehbe-Alamah & McFarland, 2015a).
The researcher aimed to respect Maasai culture and current care practices while discovering implications for beneficial health practices that would be receptively received. The CCT was used to guide discernment of largely unknown ideas about malaria care within their culture. The theoretical constructs of care and culture, which are foundational and essential toward discovery of care within any culture, encompass the multiple influencers on malaria care within the Maasai emic perspective. Of the 11 assumptive premises of the CCT, five were adapted for this study context (Table 2). It was intended that the ATLAS.ti qualitative computer software analysis program would be used to facilitate data management and analysis. However, because of limited access to electricity and internet service while on site in Africa, the researcher had to adjust this plan and make extensive use of a field note journal.
Five Assumptive Premises of the Culture Care Theory Adapted for This Research Study (McFarland & Wehbe-Alamah, 2015, pp. 8-9).
The ethnonursing research method was developed for use with the CCT and melds the unique relationship between culture and care (McFarland & Wehbe-Alamah, 2015; Wehbe-Alamah & McFarland, 2015a). As Maa is an oral language, only written in English characters in Holy Scripture, stories are the Maasai means of sharing values, beliefs and lifeways. Qualitative discovery through hearing the community’s malaria story was a culturally appropriate, effective approach to discover cultural truths about malaria care.
Institutional review board approval was received from the university and the Maasai Chief of the Kimana area. All participant volunteers gave verbal or written consent. Extensive forward, back, and monolingual translation assured linguistic accuracy and cultural understanding (Maneesriwongul & Dixon, 2004). Two interpreters were engaged for all interviews with informants who did not speak fluent English. The overwhelming local interest enabled 16 key informants (KIs) and 32 general informants (GIs) to share their stories, making this a macro ethnonursing study.
KIs were experts on the DOI, Maasai, and a Kisongo Maasai village resident. Sixteen KIs—11 women and 5 men aged 18 to 100 years—participated in individual 1 to 2 hour initial interviews, plus one to three follow-up interviews. While five reported some formal education, none went beyond secondary school. GIs held general knowledge on malaria and provided additional data for understanding the DOI. Thirty-two GIs—16 males and 16 females aged 18 to 90 years—participated in individual and focus group interviews of 30 to 90 minutes: 18 were Maasai, 5 part-Maasai, and 9 non-Maasai. GIs were Maasai community members: community health workers, pharmacists, nurses or doctors from government and private facilities; pastors; or government and nongovernment malaria care partners. The researcher met the informants where they were able to take a pause in their day, in settings that were convenient, safe, and afforded private conversation. Most KIs chose to be interviewed in their home village, generally under the shade of a tree, with livestock and children quietly settled nearby (Figure 1).

Interview setting. Entering the environment of the Maasai elders for an interview.
Four research enablers facilitated documentation and confirmation of data and strengthened a rigorous study. The PI specifically chose an area of Maasailand only infrequently visited prior to this study to aid in suspending a priori judgments. The Sunrise Enabler, which depicts the integration of major CCT constructs (Figure 2; McFarland & Wehbe-Alamah, 2015), served as a cognitive map to guide comprehensive collection of malaria care data. It was also reviewed to guide the literature review, develop inquiry questions, and direct the analysis process, in a quest toward discovery of Maasai cultural influences and malaria care truths to guide CCMC. Three other enablers were resourced: (a) Observation-Participation-Reflection Enabler, to successfully enter and focus on the informants’ natural environment; (b) Stranger to Trusted Friend Enabler, to facilitate development of trusted relationships with the Maasai community that promoted sharing of truthful, credible data; and (c) Ethnodemographic Enabler, to guide formation of respectful inquiries into ethnodemographic topics such as gender, water and cooking fuel sources, toilet facility, mobile phone ownership, and ITN use (Wehbe-Alamah & McFarland, 2015b).
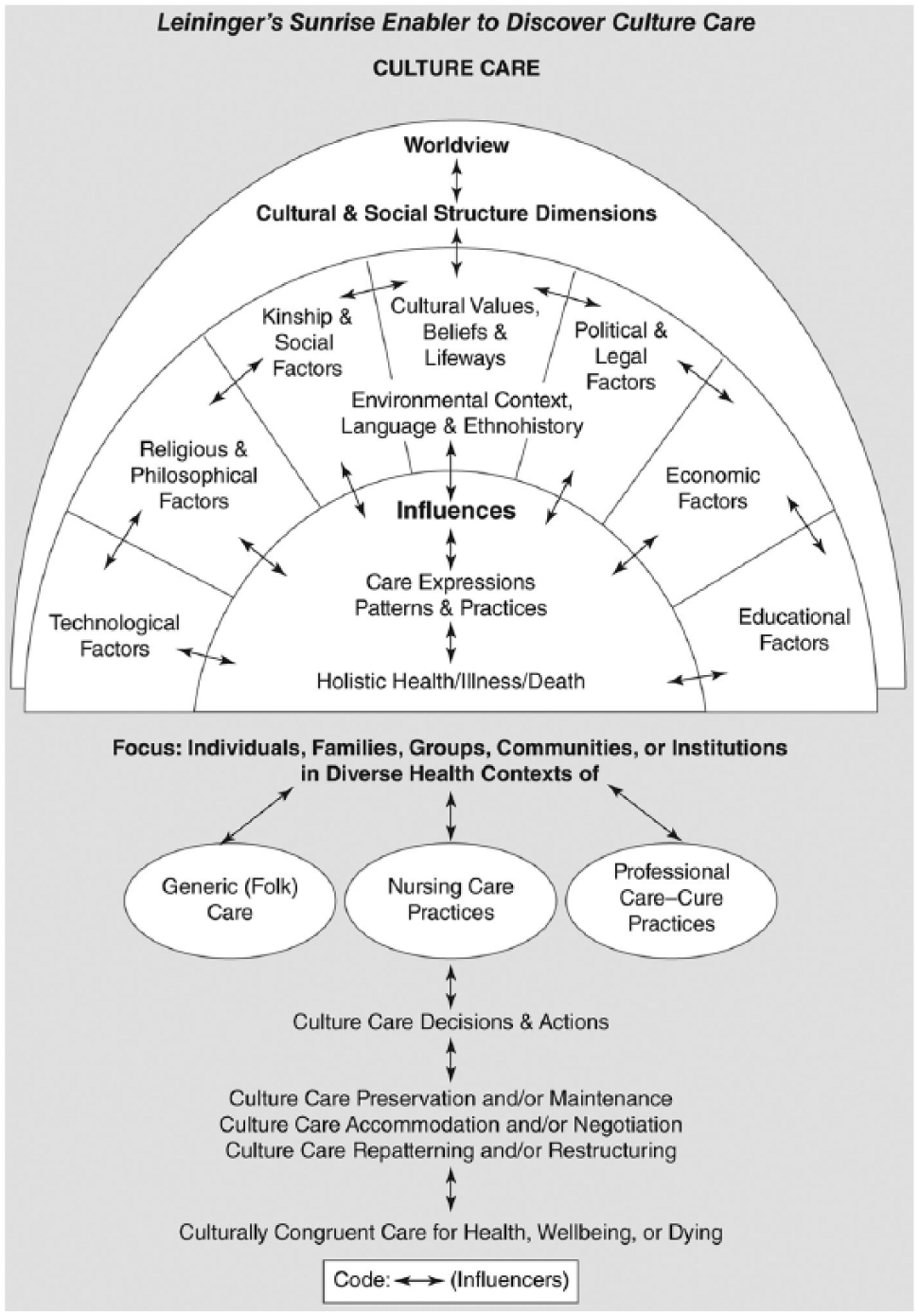
Leininger’s Sunrise Enabler to discover culture care (depicts the major theoretical concepts of the culture care theory).
The Four Phases of Ethnonursing Analysis were used to guide a systematic analysis of study data (Wehbe-Alamah & McFarland, 2015b). In Phase 1 while cognizant of the etic perspective, the researcher remained focused on the DOI, context, and emic perspective, guided by an open-ended interview guide. Detailed field notes, audio recordings, and photographs contain observations, researcher participation events, and informant interviews. Phase 2 included coding and initial classification, and descriptors were studied for differences and similarities. During Phase 3, data were examined for saturation, recurrent patterns, meaning-in-context, credibility, and confirmation. Phase 4 included synthesis and interpretation toward confirmation of themes, which led to nursing decision and action recommendations. Findings tended toward universality of shared care meanings, expressions, and practices. Rather than linear, the analysis was a continual, fluid process that moved among the phases, with reconfirmations and an audit trail back to raw data.
Rigor of ethnonursing methodology is held to the high standards of qualitative research and occurred throughout the study: credibility, confirmability, meaning-in-context, recurrent patterning, saturation, and transferability (Strang, 2014). For example, to establish credibility, the researcher visited the area 2 years prior to this study to gain gatekeeper permission from Maasai elders and area chief. Confirmability was strengthened, as continual comparison of field notes was made and findings were reaffirmed during follow-up interviews with informants.
Major Research Findings
Analysis, synthesis, and interpretation of the data led to four major themes. All themes and care patterns tended toward universality and illustrated the informants’ worldview, cultural and social structure, environmental context, language, ethnohistory, and generic/traditional and professional care–cure practices.
Theme 1: Malaria Care Is a Response by the Entire Maasai Community to Promote Community Well-Being
Malaria care is a response by each member of the Maasai community to an expected illness in their environmental context. For the Maasai, each person’s well-being is a reflection of the whole community and vice versa. For example, when asked, “How are you?” the response was, “‘We’ are not well; my wife’s mother is sick.” Because of the harsh living environment in Maasailand, the well-being of self, family, village, and the community as a whole, is dependent on the investment of each member in daily tasks. This includes malaria care responsibilities of men, women, children, old ones, and even the sick. Three care patterns supported this theme.
Pattern 1: Recognizing Environment as Cause and Cure
While all informants related elements of the environment to the cause of malaria, diversity was noted in their responses: “rain,” “green grass,” “mosquitoes,” “God,” “cold weather,” “flowing or stagnant water,” and “sunset” or “evening.” Three Maasai informants reported: “The mosquito has malaria, especially when it rains;” “In the evening when the sun sets, all the mosquitoes come;” and “After drinking contaminated swamp water, we have malaria.” The environment as cure was reflected within the extensive use of herbs for malaria care (further described in Theme 3).
Pattern 2: Understanding of and Familiarity With Malaria
This pattern was reflected in informant’s in-depth descriptions of malaria and their recognition of the need for an immediate care response. Most informants described that malaria comes when “there is rain, the air is cool, and the environment is green.” Participant responses showed understanding of and familiarity with symptom recognition, expected cycle of symptoms, malaria as a predominant and serious health issue, names for malaria, and types of mosquitoes and their relevance to illness severity and outcomes. “I learned about malaria for myself. I have that headache and I know.” One young informant stated, “Malaria is in the whole body, including the blood.” Enk-agang’ani, the Maa term for fever and mosquito, was used by all Maasai informants. “The mosquito is very poisonous. It bites you, blood comes out, and transmits to your blood. Then, you get malaria.” Most every informant used the same two specific words to describe malaria: olnairobi, the concept that malaria always starts out as cold; and irmotiook, meaning “changing a sufuria [a cooking pot]” and putting another on the fire. These concepts summarized that the sick ones are the same person, but inside they are different. They feel cold, then hot; they feel good, then suddenly bad. The symptoms of a child’s illness were also descriptive. One young mom quietly stated, “If a child cannot talk, they have malaria.” Another said malaria “begins with shaking and he becomes very hot. Their heart starts pumping. The child starts saying ‘um, um, um’ with the high fever.” One mom reported that “a person is very hot, you cannot be near because they will burn even you.”
Pattern 3: Responding as Community in Malaria Care
The community response included understanding the disease and being confident in knowing how to respond to the symptoms experienced personally or observed in others. “We have grown up with the symptoms. That is how we know” how to give malaria care. Women may be responsible to “care for the sick,” such as “serve herbs to the ill person,” “wash the patient,” “observe the sick person for signs of worsening illness or recovery,” and “make the recovery soup.” A herbalist, who may be a man or a woman, “has herbs for those who need them and cannot collect themselves.” Community members, especially elders and old women, have the “responsibility to educate the young about [traditional] malaria care.” Malaria care involves the knowledge of “knowing what to do first.” Informants addressed the reality that, even with care, death was a potential outcome. “Little children and old men with weak bodies usually die from malaria, but not the moran [strong young warriors].” An elderly, traditional Maasai herbalist expressively shared, “If you don’t get treatment for malaria you stay like this (she put her arms straight out, rolled her eyes back, wrinkled her mouth, and became very still) . . . and die.”
Theme 2: Enkai, as Creator, Is in Ultimate Control and Is Resourced in Malaria Care
The Maasai worldview revolves around daily life of family, community well-being, and the creation in which they live. Three universal care patterns from the data supported Theme 2.
Pattern 1: Enkai Is Enkai
Enkai [God] was cited by name by most KIs and GIs. One Maasai elder clarified, “Enkai is Enkai. God is God. It is the same God” recognized by traditional and Christian Maasai. Two GI pastors confirmed the “traditional Maasai monotheistic belief is in one God.” Many described God as being very near to them personally. “I have faith I am in God’s hands.”
Pattern 2: Enkai Is Creator and in Control of the World
Informants spoke of Enkai as trusted “creator of the rain, mosquitoes, and herbs” who “gives the Maasai life, children, and livestock.” A mom shared, “God is good, so we don’t blame God” for malaria. A grandmother said, “Only God can prevent malaria. We have nothing to prevent malaria.” A young moran thought deeply about his spiritual beliefs and spoke as a representative of his village, “God is the only one who can help our relatives, people, and families. Not the church, but God.”
Pattern 3: Enkai Is Resourced as an Act of Malaria Care
Enkai was trusted to provide malaria care: “I pray to God to chase away malaria.” A young traditional Maasai man and a young mom both shared, “I have faith that when somebody in my family gets sick, God can heal. God can heal me.” Historically, Maasai used a traditional, spiritual healer, the liabon. Informants is this study, however, reported that the liabon is no longer a trustworthy authority on malaria care. “We do not believe the liabon can heal. Only God can heal from malaria.” “We go to elders who know the herbs. We do not go to the liabon.”
Theme 3: Malaria Care Is a Planned Sequence of Traditional, Spiritual, and Professional Care/Cure Practices
Maasai have a malaria care plan: a sequence of practices for illness, recovery, and for prevention. The malaria care/cure practices involved traditional, spiritual, and/or professional care. Four care patterns supported this theme.
Pattern 1: Traditional Care/Cure Practices Are the First Care Act
Generic care was the predominate care/cure practice. The first malaria care act usually took the form of administering traditional herbs as care, “using elements within the environment,” to cause “purging of the malaria,” to “aid in recovery to regain strength and weight,” and to “prevent occurrence.” Fourteen of the 16 KIs, who represented all age groups and educational levels, stated that, “when we know a person has malaria, we use herbs.” Herbs in their environment were “available nearby,” “affordable,” and “they usually work.” Herbal care was described as a complex sequence of gathering, preparing, measuring, and administering the medicinal of herbs. Collection was usually by men because “men are stronger than women and the roots are hard to dig out of the ground.” Also, “we collect the herbs in forest far away where there are wild animals, because it is not safe for women to go.” Informants freely shared skills necessary for malaria care with the researcher, including names of herbs used, how to collect, dry and store the herbs, and how to mix the herbs using an olkipire (a special handmade stick). Herb potency was an important concept for herbal care safety. The “stronger/bitter herbs were for adults and moran,” and the “weaker herbs were for pregnant women and children” younger than 10 years. Frequently, herbs were used to purge the illness from the body through vomiting, diarrhea, and/or sweating. “In our community, we treat using roots of an herb.” “After drinking the herb, and after vomiting out watery, greenish liquid, you feel the body relax, and this is the sign the body is getting better.” A very old Maasai lady promoted, “If you drink herbs all the time, you will not get malaria.” One Maasai elder shared, “Herbs are given by Enkai to protect and heal in all illnesses, including for malaria care.”
Pattern 2: Spiritual Care/Cure Practices Are a Co-care Act
A very old KI “prays to God to heal me first, then I drink the medicine.” Mothers shared that, “when my child gets sick, I start with prayer.” Acts of prayer extended beyond the sick. Field notes recorded prayers for the researcher, “We will pray for you, that you will come back to help us in malaria care.”
Pattern 3: Professional Care/Cure Practices Are an Emerging Care Act
Professional care was referenced as a newer malaria care practice in Maasailand. Most informants shared that professional care was an appropriate resource, but not as the first act of care. Use of professional care was influenced by multiple factors that included the proximity of resources (accessibility), affordability, availability of quality professional care and medicines, and acceptability. KI and GI also attributed their use of professional care to ethnohistorical influences: “mistrust of outsiders;” “lack of knowledge about professional care;” “non-care acts experienced from professional care givers,” specifically related to respect of the Maasai in general and respect of their use of herbal medicines; and “unfamiliarity with care practices, such as use of tablets and injections.”
Pattern 4: The Maasai Environmental Context Influences Facilitators and Barriers to Malaria Care/Cure Practices
Facilitators and barriers to care included geographic environment and location, expectation to first use traditional care, knowledge of care options, financial means, and use of ITN. Of the 16 KIs, 4 were found to be currently using ITN, 7 had used ITN in the past, and 5 had never used ITN. However, no informant said that he or she would not sleep under a net, only that ITN were not available and/or affordable.
Theme 4: The Maasai Community Is Resolute in Responding to the Malaria Illness
KI were resolute that malaria is expected in their environmental context and their current care practices are good. The Maasai did not express worry or fear about becoming ill. Yet they were not content to live with the illness if there is a way to prevent it. Informants universally voiced the desire to hear and learn more. They were also resolute that care is their responsibility and there is limited help in Maasailand. Three patterns supported this theme.
Pattern 1: Maasai Do Not Live in Fear of the Malaria Illness
Malaria was described as just “part of life.” The Maasai live with it, accept it, know what to do, and do what needs to be done. One Maasai elder reflected, “There are mosquitoes. There is rain. There is malaria. God has provided herbs and the knowledge among Maasai of how to use the herbs to treat adults and children. No, we do not fear malaria.” One young mother stated matter-of-factly, “I do not worry about my child getting malaria. My child will get malaria.” Others said, “Only God can prevent malaria,” and “Malaria is too big of a problem for people or the government to control.”
Pattern 2: Maasai Are Curious to Learn More About Malaria Care
The Maasai’s resolve included the acts to consult, talk over, seek information, and ask for professional opinions. Every KI and GI was curious about how to best offer malaria care. One young moran offered a poignant disclaimer, “We are interested to learn more, because nobody loves to be sick.” A health care worker expressed that “many people think there is no malaria because they do not hear the mosquito passing. But they need to take precautions before they hear it moving.” Two health care provider informants said, “Education is critical. The Maasai have mobiles [phones].” This form of communication “could be a great asset to future malaria care in Maasailand.” An elderly man voiced openness to new malaria care ways, such as ITN use, “The hospital gives nets [to the women]. This may be a solution.”
Pattern 3: Maasai Do Not Depend on Political or Nongovernment Organization (NGO) Support for Malaria Care
Most informants stated that they currently receive no outside help from political or nongovernment organizations (NGO’s) for malaria care. A GI health worker commented, Previously, there has been no advocacy from [within] the Maasai communities. They did not know their rights of health care. Their transport is walking or maybe using donkeys. By the time they reach a health care facility, they may be wasted, anemic, or dead. Then, the facility they got to cannot accurately diagnose the illness. Today, there are NGOs interested in these isolated and hard-to-reach areas and advocacy is beginning for the Maasai people.
Discussion
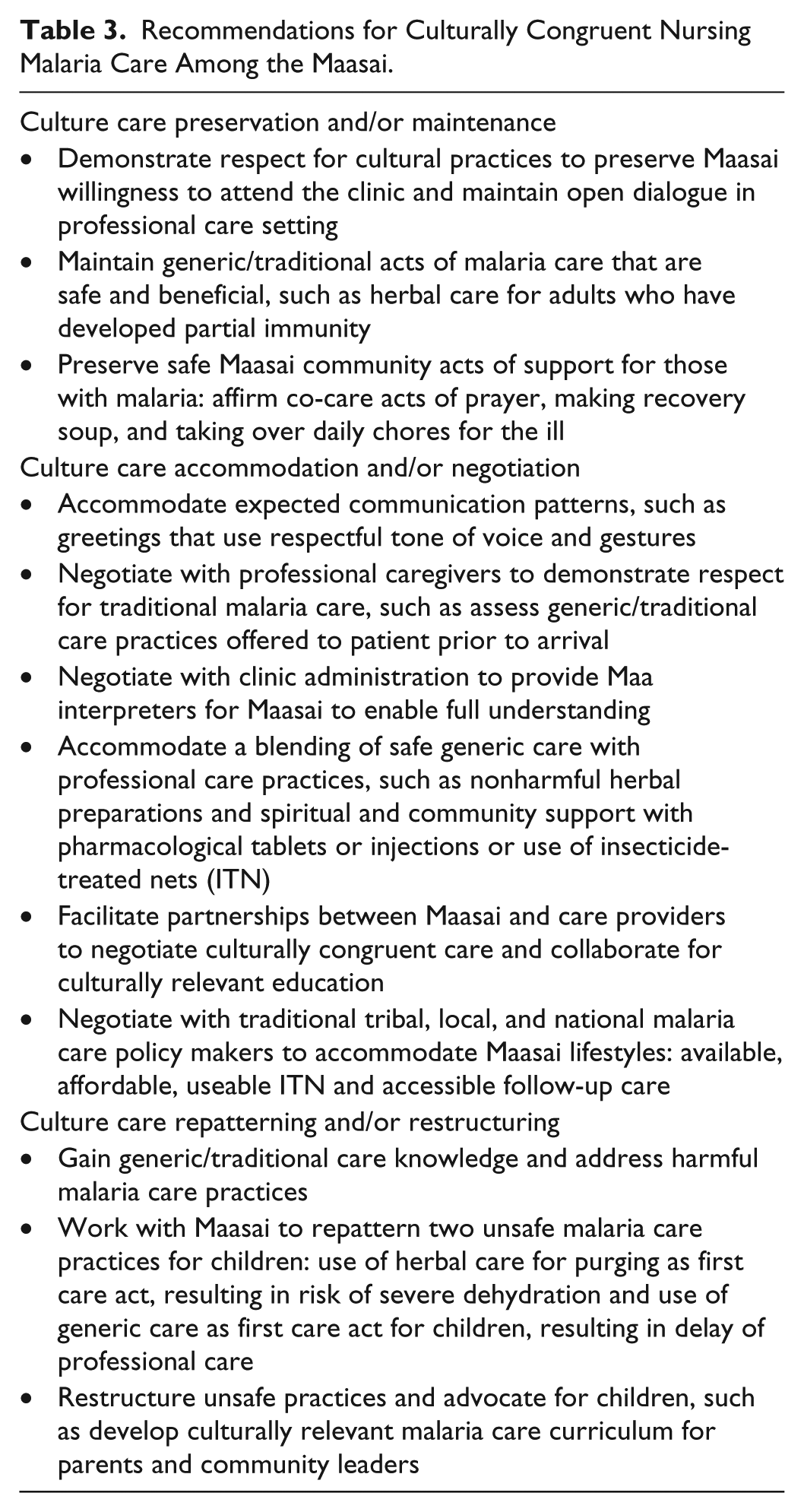
Universal and diverse themes and care patterns discovered among the Maasai are unique to their culture. The CCT predicts three modes that will assist, support, facilitate, or enable nursing care (McFarland & Wehbe-Alamah, 2015). Research data were used to recommend nursing decisions and actions for CCMC that is holistic, promotes community well-being, and is safe, beneficial, and fits with people’s daily lives (Table 3).
Recommendations for Culturally Congruent Nursing Malaria Care Among the Maasai.
Following is a discussion of implications for nursing practice, policy, future research, and theory contributions. Respect of Maasai lifeways and traditional care practices are of primary importance in their acceptance of malaria care from health care professionals (HCP). Ethnonursing studies have shown repeatedly that respect is the most valued and frequently identified care construct (McFarland & Zehnder, 2006; Mixer, 2011; Morris, 2012; Schumacher, 2010; Wehbe-Alamah, 2015). Care ethics demand that respect be offered to care recipients and caregivers (Mixer et al., 2013). Most research participants, including the HCP, requested education methods and content that convey respect and affirm safe, generic care practices. Education should be relevant to and cocreated with the Maasai. Informants voiced preferences for active learning measures, such as hands-on practice with hanging an ITN and use of drama. Use of mobile phones for appointment reminders and suggested care protocols may be an effective way to communicate between HCP and Maasai in remote villages. Confirmed as the first care act in this study, African researchers found that the first-line treatment for 60% of children with a high malaria fever is traditional herbal care (Johnson, 2008). Herbal care has been used for thousands of years because it is trusted, available, and affordable (Graz, Kitua, & Malebo, 2011). CCMC that educates Maasai about safe and unsafe herbal practices, particularly for children, is needed.
The provision of malaria care in Maasailand has multiple health policy implications. To alleviate barriers to CCMC, HCP can negotiate with traditional Maasai elders and on behalf of the Maasai with global partners, such as CDC, WHO, and PMI. Malaria care needs identified by informants included gaining adequate knowledge; cultural acceptance for use of professional care; infrastructure for adequate access care facilities; and affordable and available supplies to prevent, test, and treat malaria, such as ITN, rapid diagnostic tests, and quality pharmaceuticals.
The research findings also contributed to building nursing theory. Each of the five CCT assumptive premises used in this study was upheld (Strang, 2014; Table 2). Care constructs are dominant care meanings and/or action modes discovered using the CCT and this study further supported their discovery (McFarland & Wehbe-Alamah, 2015). Seven care constructs represent the core meanings, expressions, and practices of malaria care among the Maasai informants and facilitate the nurse’s understanding. Four were congruent with previous transcultural nursing findings: respect for/about lifeways, acceptance, purging, and interest in/about (McFarland & Wehbe-Alamah, 2015). Three new care constructs were revealed. Herbs as care was at the forefront of each KI description as the first care act and the responsibility of the entire community. Community as care meant all members provided physical and spiritual care and completed their daily tasks toward the well-being of the whole community. Praying to/for was universally voiced by the Maasai informants, as they reported praying to Enkai to heal the sick, for herbs and/or medicines to heal the patient, and for the researcher to be successful in her work and return to assist the Maasai in malaria care.
This study can be used as the basis for future research. First, this study could be repeated in other Maasai regions and the results compared with those of this study. Second, the CCT concepts could be used to create, administer, and examine the effectiveness of malaria education seminars or other specific prevention measures. Since many Maasai possess mobile phones or access to radios, research could examine the use of technology for malaria education and behavior change communication. Moreover, other researchers and practitioners may transfer these findings to other vulnerable populations who suffer from the malaria. Finally, the Maasai participants in this study invited the researcher to return to implement CCMC education, influence malaria care policy, and conduct future research among them.
Conclusion
This was the first qualitative study with the Kenyan Maasai focused only on malaria, and the first use of the CCT and ethnonursing method for study of malaria care and in the Maasai culture. The theory and method enabled a rigorous, culturally sensitive study. Study findings filled a gap in the literature and revealed meanings, expressions, and practices of malaria care among the Maasai in the Kimana region of Kenya, as well as their desire to become knowledgeable to improve their health. Maasai leaders and national and global malaria care partners can use these findings to implement CCMC education, policy, and health care practice to improve malaria care health behaviors and outcomes in the Maasai community.
Footnotes
Acknowledgements
The authors gratefully acknowledge the Maasai people, who welcomed and trusted the researcher’s presence in their culture and agreed to participate in the study to share their malaria care stories.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.