
Abstract
Keywords
Introduction
The opportunity for nurses to affect Honduran community health is immense given the limited access to health services throughout the country. Nurses who understand the context of care can greatly enhance the effectiveness of their health promotion activities. Honduras is the second poorest country in Central America and more than half of its population is younger than 25 years (Central Intelligence Agency, 2016). Honduras has the world’s highest murder rate and suffers from a multitude of maladies. The top causes of years of life lost in 2013 were from ischemic heart disease, interpersonal violence, congenital anomalies, and preterm birth complications (Institute for Health Metrics and Evaluation, 2013). Dietary intake, high blood pressure, and high body mass index were the leading risk factors for disability adjusted life years in Honduras in 2013 (Institute for Health Metrics and Evaluation, 2013). An estimated 60% of the population lives below the poverty line and roughly 83% of the population lacks any form of health insurance (Central Intelligence Agency, 2016; Pan American Health Organization, 2007). Additionally, Honduras does not have enough trained health care workers to meet the population’s needs (Global Health Workforce Alliance and World Health Organization, 2013). Involving the community to identify health priorities and strategies for improvement have been effective approaches to building capacity for health promotion.
The limited availability of skilled nurses in many developing countries has spurred cross-cultural partnerships in academia between more developed and less developed nations (Atkins & Stone, 2006; Merson, 2014; Riner & Becklenberg, 2001). Nurses involved in international and community health experiences can be instrumental with task shifting from individual patient models to more holistic community or population-focused models of health care (International Council of Nurses, 2012, World Health Organization, 2012). However, even with personnel in place, communities’ priorities may not be clear. Community needs assessments which include assessment, dissemination, and implementation are an action-oriented approach to community engagement in health promotion activities (Crigger & Holcomb, 2007; Finifter, Jensen, Wilson, & Koenig, 2005).
The community where this study took place in was located in the outskirts of El Progreso, Honduras. Many families in Villa Soleada were left homeless in 1998 after the devastation of Hurricane Mitch. Prior to the construction of 44 houses in Villa Soleada, most families were living in temporary corrugated iron, wood, and tarp shacks with very limited resources without electricity, gathering water from a river, using pit latrines, and burning trash as their main source for waste removal. Health care was sought mostly at the public clinic or hospital in El Progreso for those who could access it, as transportation was not available for many families. As a result of health services scarcity, health promotion and education were severely limited. This community was chosen due to the deep-rooted partnership and investment in the development of Villa Soleada from Students Helping Honduras (SHH) and participating students. Grassroots efforts with events such as traditional dance, host family visits, shared meals, and soccer games fostered student and cross-cultural community teambuilding during service learning trips. As the partnership between SHH and Villa Soleada strengthened and basic needs were slowly being met, health needs could began to be identified. Mothers were chosen as participants due to their role as primary caretaker of children as well as their ability to answer questions regarding pregnancy and maternal health.
The health needs of Villa Soleada were unknown, thus, prior to designing a community health promotion program, a targeted needs assessment was designed. Therefore, the aims of this study were to understand mother’s perspectives of health priorities for families through a community health needs assessment, partner with a community and local organizations to plan and implement a sustainable community-based health promotion program, and provide U.S. nursing students an opportunity for a cultural immersion experience aimed to increase Honduran community engagement in a health promotion program to improve culturally congruent health care.
Theoretical Framework
Community needs assessments are used frequently for the purpose of obtaining baseline information before conducting an intervention (Finifter et al., 2005; Running, Martin, & Tolle, 2007). The transcultural nursing theory of Leininger (1985, 2002) and Leininger’s Sunrise Model are an important foundation for this study recognizing the need for cultural care competence and cultural humility when working in a different culture context. Leininger’s (2002) theory helps explain diverse and universal culturally based care factors influencing the health, well-being, illness, or death of individuals or groups. The purpose is to use research findings to provide culturally congruent, safe, and meaningful care to clients of diverse or similar cultures (Leininger, 2002).
The theoretical aspects of Leininger’s theory are important in this particular community needs assessment in Villa Soleada. The principal investigator had 4 years of experience working with this particular community; however, recognized differences in cultural and ethnic background was a factor, so an ethnonursing paradigm was critical to bringing awareness to cultural barriers (Leininger, 2002). Both emic—insider and local cultural views, as well as etic—outsider world views and especially professional views, were leveraged for this study (Leininger, 2000b; Murphy, 2006).
Method
Study Design
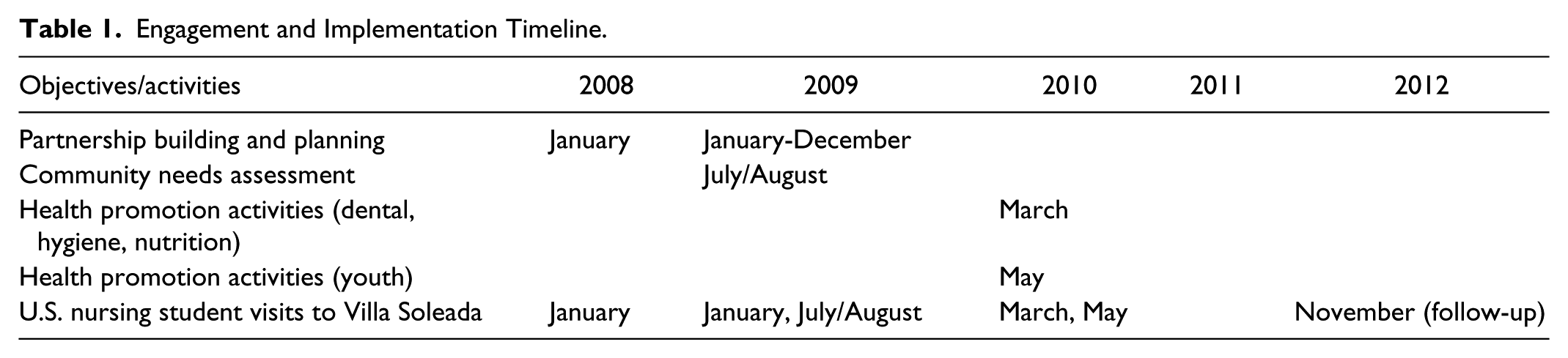
This participatory action research study was conducted as a partnership between a nongovernment organization in Honduras, local Hondurans, and students from a U.S. academic organization to assess the health needs of a community and to plan and implement a health promotion program (Crigger & Holcomb, 2007; Finifter et al., 2005). The study had three phases: planning, assessment, and health promotion. Planning took place between January 2008 and July 2009 during multiple short-term trips of nursing students visiting Honduras and through ongoing communication with partners in Honduras to establish rapport with the community. The needs assessment took place in July and August 2009 in Villa Soleada, Honduras. Finally, a health promotion program based on the results of the needs assessment and input from local partners took place in March and May 2010, during nursing student-led immersion trips. A community-centric approach, focused on community empowerment, was taken to provide culturally relevant health information appropriate to the needs and wants of the individuals in the study setting. Approval by the Boston College Institutional Review Board (principal investigator academic affiliation) was granted in July 2009 and approval was also provided by SHH and Villa Soleada community leadership.
Study Setting
Villa Soleada is a village of 44 families located in the outskirts of El Progreso near San Pedro Sula, Honduras. The closest clinic was 10 miles (30-minute bus ride) away, and the nearest hospital was 12 miles away. The village is a 20-minute walk to the tarmac road where the nearest bus stop is located.
The nonprofit SHH, located in El Progreso, is a partnership that began in 2007 with academic institutions in the United States and local Honduran families to build the community of Villa Soleada (SHH, 2015). SHH and the families, who were going to live in the newly constructed houses in Villa Soleada, united to invest in local capacity. A clear understanding of what the community identified as their health priorities was necessary to design and implement community-engaged health promotion.
Planning
Bachelors and masters nursing students from one U.S. institution were engaged with local leaders and SHH-based staff over the three phases of planning, community needs assessment, and health promotion implementation. Nine nursing student trips between January 2008 and November 2012 took place. Additionally, e-mails, Skype calls, and four visits from SHH-based staff to the United States facilitated the activities and the cultural immersion of students into Honduran health. Relationships between Villa Soleada, SHH, and students from SHH-affiliated academic institutions improved with each discussion and service-learning trip. Initial discussions of a community assessment began in January 2008 (Table 1). Discussions included the following: how to conduct a health needs assessment, what topics to address, the role of nurses, strategies for implementing a community-based health promotion program, and how to engage the community in each phase of the program. These discussions occurred during a 3-year period based on shared goal setting for Villa Soleada and students affiliated with SHH. Discussions were informal and organic, incorporating people in Villa Soleada to gauge interest in health promotion. The planning team led by a graduate nursing student and SHH-based staff expanded over time to include additional community partners and physicians at the El Progreso Hospital and local clinic. Partners were instrumental for improving cultural appropriateness of the study design and health topics, and later in supporting implementation.
Engagement and Implementation Timeline.
Needs Assessment
A community health needs assessment was planned for July and August 2009. The research lead and community partner used an iterative process to develop the assessment as a questionnaire based on empirical research and clinical experience in similar settings that would be culturally and contextually appropriate to Villa Soleada (Running et al., 2007). Mothers were identified as respondents as they are the family members most responsible for the home and family in Villa Soleada. Women were eligible to participate if they were between the ages of 18 and 65 years and had at least one child. In a community of 44 families, the team aimed to interview 30 women.
No recruitment materials were used due to the familiarity and positive presence of SHH and the study team in the community prior to interviews. Key informants or community “matriarchs” bestowed multiple blessings on the study team to encourage women to participate. Interviews were conducted in the setting most preferred by participants, either in the women’s house or in outdoor spaces.
A consent form was read to each woman in Spanish. Time was permitted to ask questions, reach a verbal understanding, and obtain written consent. The interviewer was fluent in Spanish and used the locally developed community needs assessment. One interviewer was used to conduct the interviews because of interrater reliability and resource constraints and the need for fluent bilingual language skills. This questionnaire was structured as a 32-item survey and included questions about sociodemographics, health priorities, and interest in health promotion and education opportunities. Each interview lasted 30 to 60 minutes and one interviewer completed all interviews. Data were manually entered into an Excel spreadsheet, rechecked for accuracy, and then examined for missing values where expected, outliers, and coding accuracy. Descriptive statistics were calculated in Excel using standard program data functions during the 2009-2010 academic year in preparation for a Spring 2010 health promotion program.
Health Promotion Program
A 1-day health promotion model was chosen to advance community engagement, support sustainability in a community with limited resources, and reflect the priorities identified by women who participated in the needs assessment. Health priorities identified during the interviews were reviewed in consideration of how education and training would be delivered that would be culturally sensitive, respectful of Honduran norms, and be appropriate for the community as determined by SHH leadership, local mothers of Villa Soleada, and local physicians at the Centro de Salud and Hospital in El Progreso (Crigger & Holcomb, 2007). Priorities identified were organized into three topic areas based on the appropriateness determined by the research team, SHH leadership, and local mothers. Consideration was given to recent community enhancements (the community newly had access to running water) and topics that could lead to actionable behavior change (e.g., handwashing and diet). Three U.S. nursing students facilitated the program in Spanish. Those more fluent provided more didactic information. Each topic was addressed in a 45- to 60-minute program for a total of three hours of health promotion activities in order to fully explore each topic, maintain interest, and be respectful of individuals’ time. Incentives for attendance included toothbrushes for all family members and toothpaste for participating mothers. Hand sanitizer, soap, and children’s vitamins were procured through solicited donations in the United States to incentivize participants to demonstrate skills learned. All community members were welcome to attend the program. The day prior, nurses and community volunteers went door-to-door to provide verbal reminders. The goal was to engage 15 to 20 mothers and 10 to 20 children in health promotion activities facilitated by nursing students. Assessment for success was planned to leverage qualitative verbal reports from participants due to low literacy.
Results
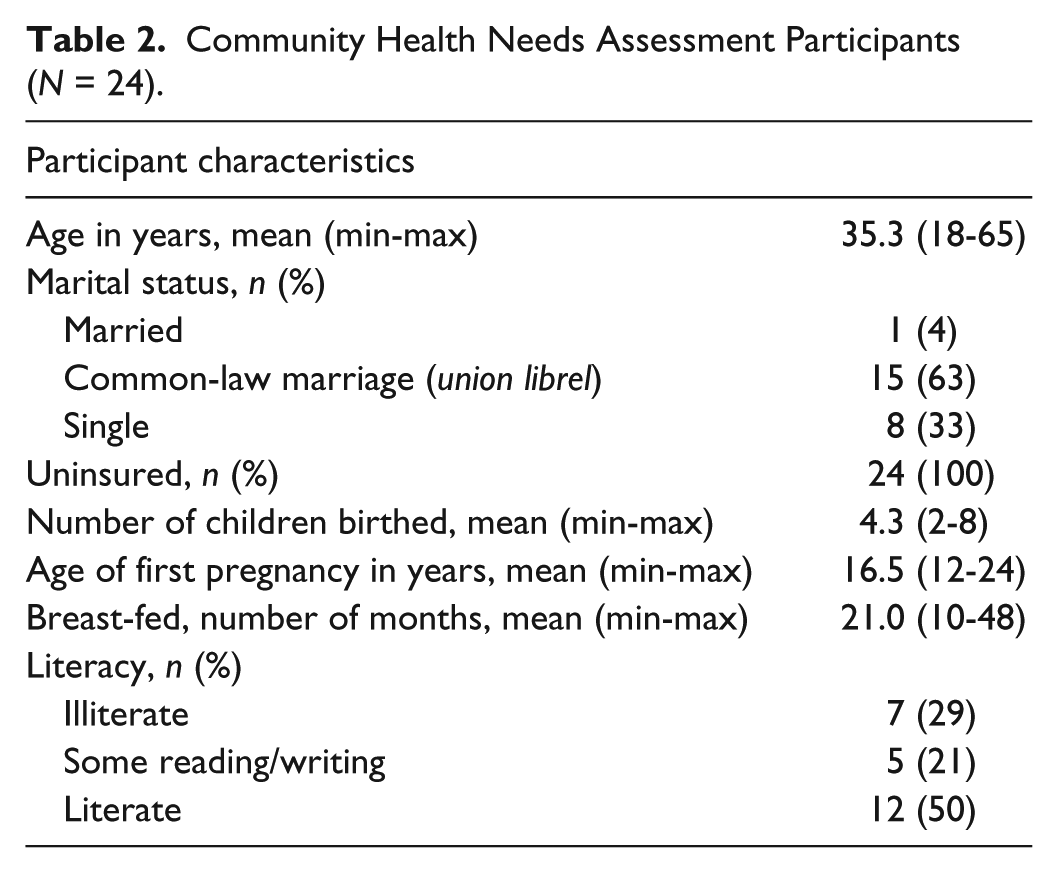
Of the 30 mothers who consented to participate, 24 were able to complete the interview (Table 2). Participants were on average 35.3 years old and 29.2% of the women interviewed were illiterate (could not write or recognize their name). Two thirds reported to have common law marriages, 33.3% were single, and one participant was legally married (4%). None of the families had any type of health insurance and participants were unsure how much they spent per year on health-related expenses. The women who participated cared for a number of family members and reported giving birth to two to eight children. The average age of first time pregnancy was 16.5 years (minimum of 12 to maximum of 24 years) and 40.0% of births occurred in the home. Women breast-fed between 9½ months and 48 months.
Community Health Needs Assessment Participants (N = 24).
Needs Assessment
Women were asked how they would rate their family’s health status and 62.5% reported normal/good (compared with very bad or bad) health. When asked, “What is your biggest health care concern/priority for your family and children,” seven reported gastrointestinal-related concerns (parasites, diarrhea, or nutrition), six reported access to care or quality of care, five reported malaria, three reported respiratory illness, one reported dental health, one reported influenza, and one reported child education. Water sources reported varied, but half of the women felt they had safe drinking water. Only five mothers (20.8%) reported toilets as their main sanitation/waste deposit and 12.5% had neither a toilet nor latrine and used the woods for sanitation. Seventy-nine percent reported to be living without electricity.
Interest in health education was high; however, only half of the participants were interested in becoming community health workers to lead health promotion activities in Villa Soleada (33.3% were indifferent and 16.7% were not interested in taking on that role). Almost all of the women said they would be interested in having health classes taught by nursing students from the United States (91.7%).
Health Promotion
To address the health priorities of the participants identified in the community needs assessment, three topics were collaboratively determined to be appropriate for health promotion: dental health, hand hygiene, and nutrition. Health promotion participants included 15 to 20 mothers between the ages of 17 and 50 years and 15 to 20 children. Visual aids (important for a largely illiterate group), demonstrations, and activities that promoted community participation were incorporated to promote engaged learning. Due to prior knowledge of low community literacy from the needs assessment, visual aids were developed at a third-grade reading level. Partnering with the community helped the study team develop culturally appropriate pictures, simple steps, and colorful posters while limiting reading materials such as pamphlets. Presentations were enhanced with diagrams and demonstrations. Nursing students further encouraged participation and learning with related resources such as soap and toothbrushes, which served as incentives. Keeping information simple and straightforward was helpful.
Evaluation
Because literacy was low, program evaluation leveraged informal qualitative communication rather than written evaluations of knowledge gained. The health promotion program was received very well in the village. Verbal reports from participants about material learned were positive. For example, one spirited participant was a 17-year-old mother of a 2-year-old daughter who was also 9 months pregnant. She was very interested in learning about tooth decay and bottle-feeding during the dental presentation. She was unaware that children older than 12 months should discontinue bottle use; and after the presentation she said, Ya no le voy a dar la pacha . . . ni hoy en la noche! [I will not give her a bottle anymore . . . not even tonight!] She was intent on learning the dental health information correctly and was appreciative afterward for the information learned. She asked additional questions after the presentation, showing her enthusiasm. The nurses also wrote about their positive experiences in reflections such as, “the mothers and children were very eager to learn and listened to what we had to say with respect and participation” and “I really felt as if the community was taking what I said to heart and [the health promotion] was the time that I felt I was most giving back to Honduras.” Overall, previous exposure to the community and trusting relationships aided in fostering respect and attention.
This model of transcultural nurse-led health promotion continued in Villa Soleada. Two months after the initial health promotion program, SHH asked for the development of additional health promotion activities and a tailored premedical student trip to foster continued Honduran partnerships related to health education. The study-lead led this endeavor and with 10 premedical students from multiple U.S.-based universities, developed education materials on sexually transmitted infections (STIs), contraception, alcohol, tobacco, and drug use for the youth in Villa Soleada. Due to the low average age of first pregnancy in the community (16.5 years), it became apparent that many teens were sexually active. Not only did this put them at risk for pregnancy but also STIs. Therefore, adolescent health topics were presented in May 2010. These were positively received by the youth. We focused on the biomedical aspects of STIs, contraception, alcohol, tobacco, and drug use, and did not lead discussions around the moral, religious, or legal aspects of adolescent health and behavior such as relationship power dynamics, domestic/sexual violence, or drug use, as we were community “outsiders.” Prior to conducting these health promotions, the materials and activities were reviewed by Honduran and American SHH staff embedded within the Villa Soleada community. Planning and implementation included structured cultural exchanges with the Centro de Salud, El Progreso Hospital, and local health care providers. SHH continues to partner U.S.-based students with Villa Soleada community leadership for ongoing service learning experiences.
Discussion
Health promotion in Villa Soleada was an effective strategy to engage mothers and children in activities aimed to prevent acute and chronic diseases, particularly waterborne and diarrheal diseases that are endemic to Honduras and chronic conditions such as hypertension and heart disease. Partnerships between community leaders, a locally established nongovernmental organization (SHH), and academic institutions in the United States led to a successful transcultural partnership. A community health needs assessment with mother’s perspectives of health priorities for their families identified gastrointestinal-related illnesses as their primary health concern. Collaborative planning led to implementation of a sustainable and contextually appropriate and acceptable nurse-led community-based health promotion program on dental health, hand hygiene, and nutrition for families. Furthermore, a second health promotion was developed after the success of the first for youth, focused on STIs, contraception, alcohol, tobacco, and drug use. Nursing students gained a rich cultural immersion experience and gained important new knowledge and skills in community-based research collaboration and conducting needs assessments and health promotion program development. Overall, this approach to providing health education and promotion proved to be acceptable and sustainable.
The Villa Soleada—SHH partnership involving students from developed countries was a worthwhile effort for stimulating and supporting health promotion activities. Although the time investment to achieve the study objectives was significant, a solid foundation for continued collaboration on health promotion was established. This included relationships that led to committed partners, an engaged community, and firsthand knowledge of the community’s needs and barriers to address them. This approach is transferrable to myriad regions with limited health care resources. Not only was this community engagement enriching for members of Villa Soleada but also for the nursing students as they learned to work within a global context and empower local leaders to shape planning and implementation to ensure cultural appropriateness, two important aspects of participatory action research and transcultural nursing theory (Auemaneekul, 2010; Leininger, 2000b). Access to transcultural nursing experiences enhances students’ perspectives and can increase their personal and professional development (Atkins & Stone, 2006; Riner & Becklenberg, 2001). Transcultural experiences can help strengthen students’ critical thinking skills and for some students, confirms their desire to practice in low resource settings.
Many U.S. universities offer short- and long-term cultural immersion trips for prelicensure and graduate nursing and medical students with varying degrees of clinical, educational, and community engagement. Some of these experiences consist of semester-long courses on community health with a short global immersion trip to implement health promotion within a community with ongoing relationships. Other experiences are supported as part of faculty research. North America has over 250 institutions with global health education offerings (Merson, 2014). Although criticism exists for short-term immersion trips largely due to concerns for sustainability, health promotion programs are a sustainable investment in communities to empower and educate (McCall & Iltis, 2014; Sullivan, 2013). The student–community engagement model is replicable while easy to customize for differing contexts. In this study, the students prepared, planned, implemented, and reflected on their community engagement. Flexibility during the planning, service-learning trip, and health promotion, was vital to the success of the engagement.
Success also arose unexpectedly from the evolution of additional partnerships over the three years described. Initially, few Honduran partners were involved beyond SHH staff and Villa Soleada residents. Local physicians from the hospital and clinic were increasingly interested in the work as the community needs assessment was developed and the health promotion program was implemented. Local clinicians were generous with their time, offering shadowing experiences in the hospital for students, and providing context into the Honduran health care system from a provider perspective. Gaining enthusiasm from early adopters, such as community leaders, was also crucial to conducting the interviews and implementing the health promotion.
Limitations
Several limitations of this research are important to address as key areas for improvement in future research. The needs assessment was not piloted prior to conducting interviews for data collection. This could have led to some revisions to better meet the level of literacy among participating mothers. Also, additional community partners could have been identified if the team had more broadly assessed the region prior to implementation. Laying a foundation and learning from local partners is critical for endorsement, community participation, and sustainability. Community partners emerged later in the process than was necessary.
Although the team had the vision for a participatory action research framework at the outset, fully employing all principles of community-based participatory research (CBPR) could have led to engagement of mothers, for example, in the design of the needs assessment and involvement of all parties involved in dissemination efforts (Wallerstein & Duran, 2003). Several key CBPR principles were, however, met. These included recognizing the community as a unit of identity, building on community strengths and resources, fostering colearning and capacity building between partners, integrating and balancing knowledge generation with interventions and actions, focusing on locally relevant health concerns and on determinants of health, and engaging in a cyclical iterative process of development, and investing in long-term processes in which partners are committed to sustainability (Israel, Schulz, Parker, & Becker, 1998; Wallerstein & Duran, 2003). Although the study was technical (i.e., based on health and nursing knowledge) and based on the researcher’s prespecified theoretical transcultural nursing framework (Auemaneekul, 2010; Leininger, 2002), the questions and purpose of conducting the community needs assessment was developed in response to the community and partner organization’s outreach and desire to develop a health promotion activity in the community.
Implications and Recommendations
Future efforts in this specific community should be targeted to teens due to the young age of first time pregnancy (16.5 years) in Villa Soleada compared with the national average 20.4 years (Central Intelligence Agency, 2016). Considering the need for nursing science in low- or middle-income settings, there is a tremendous opportunity to fully apply transcultural nursing theory and CBPR (Israel et al., 1998; Leininger, 2000a). This would allow for enhanced relationship building between nurses and community members from different cultural backgrounds as well as enhance community participation and community ownership and empowerment in research in their local setting. Flexibility for organic developments and shifts in priorities from any of the community members, organizational partners, or research team members outside of the local community should be considered and accepted throughout the research process.
Conclusion
Community informed health promotion is one strategy in which to distribute health knowledge to prevent diseases and empower communities with health-related knowledge. In Villa Soleada, improving health with targeted education and a health promotion program was a foundational cornerstone for building a healthier community. Partnering with local, sustainable organizations, and resources already in place is vital for community acceptance. Collaborative investment in community-identified priorities encourages active participation. In Villa Soleada, this investment led to successful transcultural engagement for nurses and community members.
Footnotes
Acknowledgements
Leila Bucchino, RN, collected data and interviews, and completed translations of the questionnaire. Joyce Pulcini, PhD, RN, PNP-BC, FAAN, FAANP, helped with the design of the community needs assessment. We would like to thank the staff of Students Helping Honduras, the nurses who presented the teaching topics, and especially the mothers and families of Villa Soleada who participated in this endeavor.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.