
Abstract
For the past two decades the Kingdom of Jordan has witnessed a shifting in the demographics of its population. More than two million immigrants and refugees fled from Iraq and Syria, especially women and children, to settle in Jordan due to violence, wars, and political changes in the region (UNICEF Annual Report, 2014). As a result, there are remarkable disparities among the population in Jordan in terms of socioeconomic status, geographical location (urban vs. rural), education, employments, and access to basic services (e.g., water, food, transportation) including health services (United Nations Development Program, 2015). Along with these changes, the burden of cancer is increasing among Jordanians (Ismail, Soubani, Nimri, & Al-Zeer, 2013; United Nations Development Program, 2015). In 2009, the crude incidence rate of cancer diseases among females in Ma’an city was 41/10,000, and the crude incidence rate for breast cancer was 17.3/1,000 (Al-Sayaideh, Nimri, Arqoub, Al-Zaghal, & Wafa, 2016). The mammography screening rate reported is 7.1% as compared with 13.5% in the Middle and 11.9% in the North regions (Al Nsour, Brown, Tarawneh, Haddadin, & Walks, 2012). Primary and secondary prevention strategies have been successful in saving lives (Eccles et al., 2013; Schopper & de Wolf, 2009). This ethnographic study was conducted to explore women’s values and beliefs related to breast cancer in Southern Jordan (Ma’an city).
Background
The Kingdom of Jordan is a Middle-Eastern country with an estimated population of around 9.5 million as of January 2016 (about 2.5 million are settlers from neighboring countries; Ghazal, 2016). Cancer is the second leading cause of death in Jordan (16.2%; Al-Sayaideh et al., 2016; Ismail et al., 2013). The incidence of breast cancer among adult Jordanian females has increased significantly from 21.4 to 40.9/100,000 during 1996 to 2009 (Ismail et al., 2013). At the regional level, Jordan ranks the fourth highest breast cancer prevalence after Lebanon, Bahrain, and Kuwait (Donnelly et al., 2013a).
Breast cancer affects Jordanian women at a younger age (median age between 49 and 52 years old) compared with American and European women (median age between 61 and 63 years; Arkoob, Al-Nsour, Al-Nermy, & Al-Hajawi, 2010; Donnelly et al., 2013a; Othman, Kiviniemi, Wu, & Lally, 2012). The average life expectancy for women in Jordan is about 74 years, but Jordanian woman with breast cancer are dying many years sooner than expected (Al-Kurfi & Al.Hadidi, 2014; Department of Statistics, Jordan, 2013; United Nations Department of Economic and Social Affairs, 2016). In this respect, breast cancer represents a significant threat to Jordanian families as many young women battle the disease while raising a family and playing an active role in the community.
Mortality is relatively higher because Jordanian women tend to be diagnosed at later stages of cancer. About 70% of breast cancer is diagnosed at Stages III and IV, when chances of survival are lower relative to women who are diagnosed earlier (Al Dasoqi, Zeilani, Abdalrahim, & Evans, 2013; Arkoob et al., 2010). Recent studies offer some insight as to why women of various cultural and ethnic backgrounds delay seeking breast health. The findings are summarized as follows: lack of knowledge, beliefs related to illness and health, personal responsibilities, incorrect interpretation of the symptoms, fear of abandonment by the woman’s partner, low income, fatalism, and failure to perceive negative consequences of the disease (Donnelly et al., 2013a; Kawar, 2013).
Considerable evidence shows that cultural, ethnic, and economic differences influence a woman’s perceptions and practices with respect to early detection and prevention of breast cancer (Donnelly et al., 2013a; Kawar, 2013; Salman, 2012). In the Middle Eastern Arab conservative cultures, many women are reluctant to share personal health information and tend not to seek professional health services until their conditions deteriorate and their personal support resources fail (Baron-Epel, Granot, Badarna, & Avrami, 2004). Furthermore, folk remedies, cultural beliefs about illness, lifestyle, disease, and death are passed on from generation to generation. They may use religious practices for recovery from disease prior to seeking medical advice. Among Arab Muslim women, modesty is valued, and it is embarrassing to talk about sensitive or private health issues related to sexuality, reproductive health, and marital relationships (Salman, 2012). Consequently, women may choose not to seek health care or participate in health screenings unless there are serious concerns or life-threatening conditions.
Ma’an city is an Arab traditional city where culture and religious beliefs are well preserved and valued. Research related to exploring women’s beliefs, values, and experiences about breast health in remote cities will help health providers target women who are at risk and enable them to design culturally appropriate initiatives to save their lives. It may also help nurses and other health providers to examine the existing programs and evaluate their appropriateness to serve women in geographically remote regions. Last, culturally appropriate health awareness messages can be used in creating educational programs not only in Ma’an but also in other remote regions in Jordan to save women’s lives.
Purpose and Research Questions
The purpose of this study was to understand Jordanian women’s beliefs and values related to early detection of breast cancer and how these beliefs influence their decision to receive breast cancer screening. The research questions are as follows.
Method and Design
A focused ethnography method was used for this study to understand a cultural phenomenon from a personal perspective (Creswell, 2009). A focused ethnography allowed the researchers to understand the contextual cultural meaning and experiences of Jordanian women’s beliefs and values related to breast health. This study included field work, participant observation, individual and focus group interviews for data analysis, and overall confirmation.
Permission and institutional review board approval to conduct the study was obtained in the United States and Jordan. The protocol honored the privacy of the women. Participation was voluntary and the women were free to withdraw from the study at any time. The interviews were audio-taped.
Setting
Participants were recruited from the city of Ma’an governorate in southern Jordan. It is characterized by its rural, desert location, with an estimated population of 124,100 (about 1.9% of the total population) and a population density of 3.8 people per square kilometer compared with Amman city with a density of 333.6 per square kilometer (Department of Statistics, Jordan, 2013).
Informants
Purposive sampling and snowball method was used (Polit & Beck, 2012) to recruit informants for this study. Women were eligible to participate in the study if they were native Ma’an residents, between the age of 23 and 70 years, with no history of breast cancer, received health care from health providers, and were willing to discuss elements of personal health beliefs related to breast cancer within the larger cultural context. However, women with a history of breast cancer or mastectomy were excluded.
Instruments
A demographic data form in Arabic language was used for informants to self-report age, educational status, employment status, marital status, and number of children, if any. Additionally, a semistructured interview guide used open-ended questions to elicit data about the topic.
Data Collection
Recruitment for this study began after obtaining institutional review board approval. The principal investigator contacted women who indicated interest in participating in the study, explained the study, and determined eligibility. Once eligibility was established, the informant was invited to participate in the study. The initial meeting was scheduled at the convenience of the informant. Most informants requested to be interviewed at their own homes. Some interviews took place in neighbors’ homes and in a community center for women. Data were collected and analyzed over a 2-month period.
The semistructured interview guide was used for the first audio-taped interview with each study informant. A second interview was conducted with four informants and two focus groups to ensure the accuracy and trustworthiness of the data. Interviews ranged between 40 and 90 minutes and were completed in Arabic. All data were kept in a secure file cabinet with the primary investigator. These documents will be destroyed after 5 years after the completion of the study.
Data Analysis
Leininger’s Four Phases of qualitative data analysis was used to analyze the data (Leininger & McFarland, 2006). The phases included (a) collecting and documenting raw data; (b) identifying descriptors and categories according to the domains of inquiry and research questions (emic and etic data are coded for similarities and differences); (c) identifying patterns and contextual analysis, as well as discovering saturation of ideas and recurrent patterns; and (d) identifying themes, theoretical formulations, and recommendations.
The individual and focus group interviews were audio-taped and translated from Arabic to English, retranslated by another translator into Arabic to ensure conceptual equivalency, and then finally translated back to English for accuracy. Nvivo10 was used to assist with data management. The analysis of data involved the concurrent process of collecting, coding, categorizing, and interpreting data. This process was continued until saturation of data occurred.
Findings
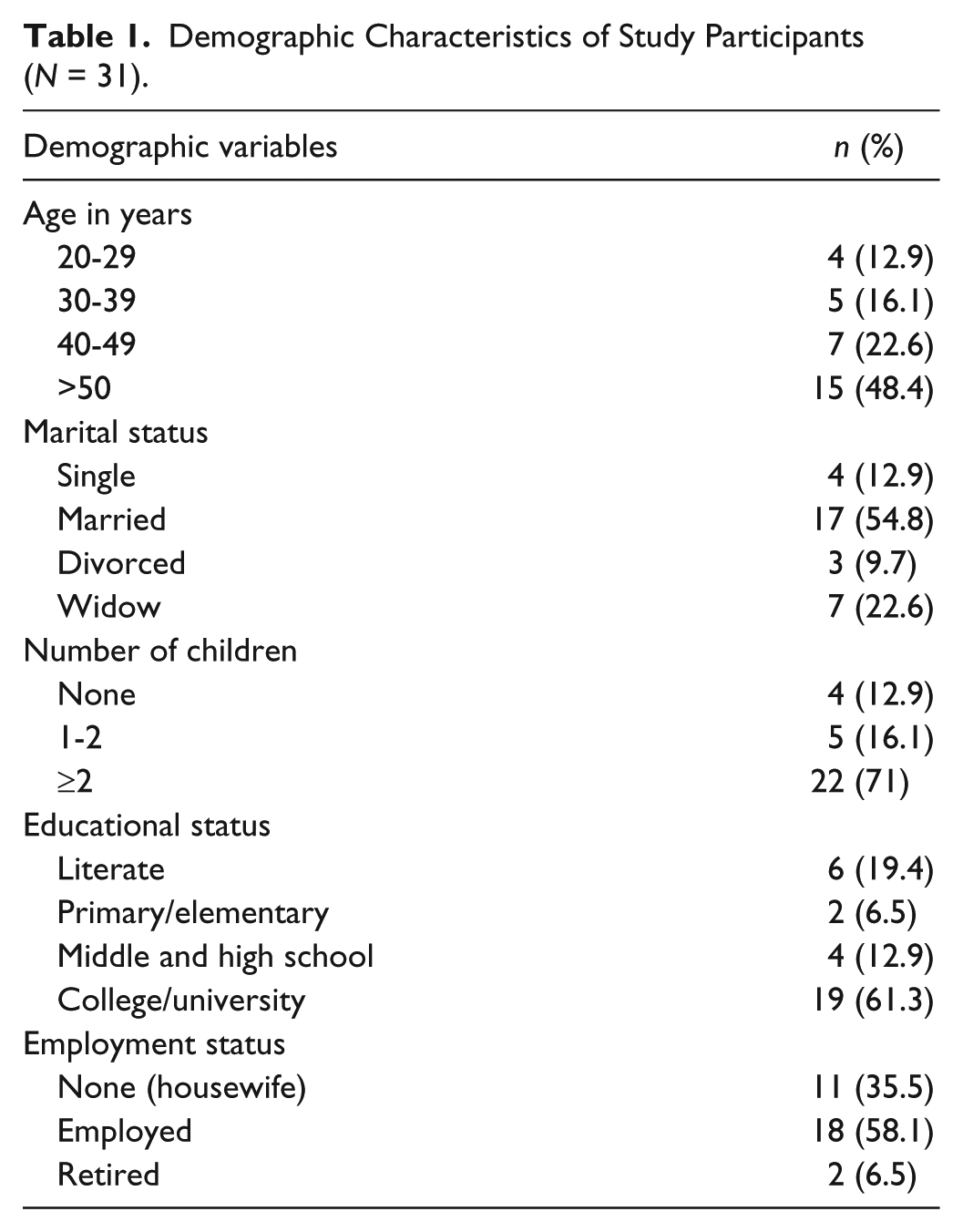
All participants self-identified as native Ma’an residents, Arab Muslims with no history of breast cancer. A total of 31 women participated in the study. Table 1 summarizes the demographic characteristics of all participants. In this study, the participants represented low- to average-income families. Individual interviews were conducted with 20 participants, and two focus groups were conducted with 11 participants. The second focus group was conducted to verify and confirm data and emerging themes.
Demographic Characteristics of Study Participants (N = 31).
The findings of this study are presented according to the process of data analysis identified by Leininger and McFarland (2006). The first phase of analysis included a review of all the raw data. In the second phase, the data were analyzed and coded line-by-line for identification of descriptors and categories according to the domains of inquiry and research questions. Emic and etic data were coded for similarities and differences. There were 19 categories identified in this second phase of the data analysis.
During the third phase of data analysis, the researchers identified patterns, contextual analysis, and saturation of ideas and recurrent patterns. The following seven patterns were identified as recurring patterns in the data according to Leininger and McFarland (2006): (a) Fear of breast cancer, (b) Discovering breast cancer late, (c) Little to no knowledge of breast cancer, (d) Being embarrassed to discuss breast cancer screening, (e) Willingness to do what one is told, (f) Reliance on family regarding health issues, and (g) Health care professionals not focusing on breast health.
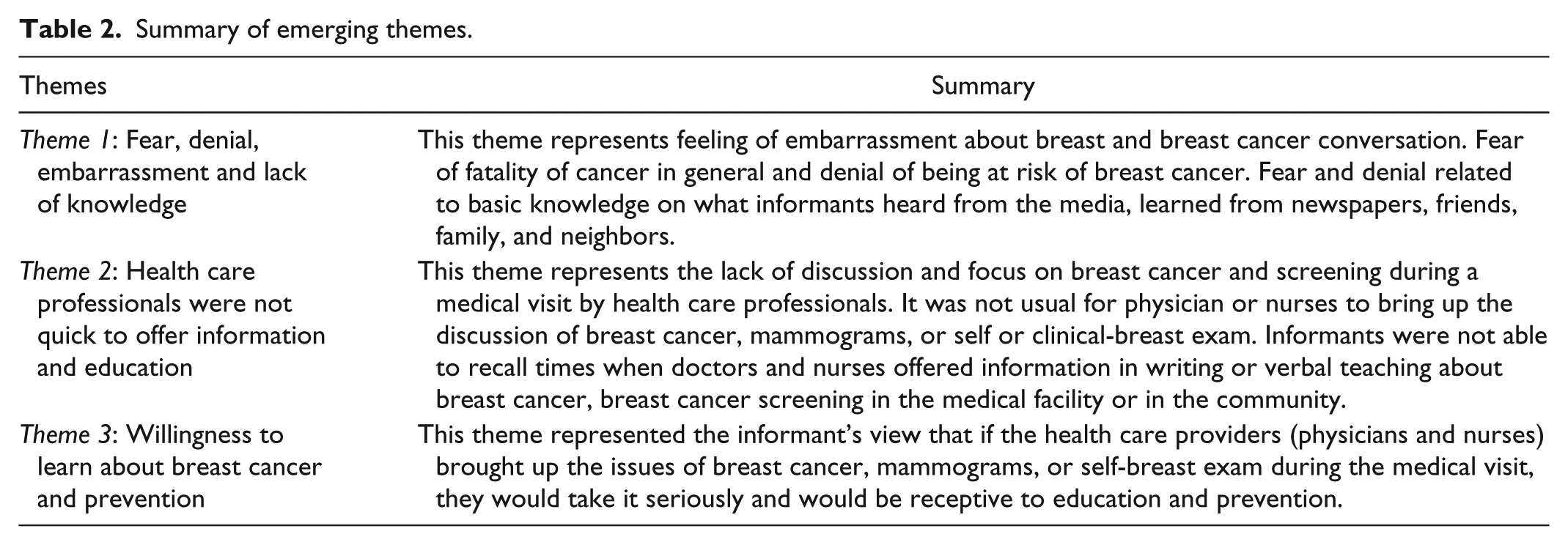
In the fourth and final phase of data analysis, the categories and patterns were analyzed for the identification of themes and theoretical formulations. The following three major themes emerged from the data. Table 2 includes a summary of these themes.
Summary of emerging themes.
Theme 1: Fear, Denial, Embarrassment, and Lack of Knowledge
Impressions and explication of Theme 1 include the following: The majority of women in the study reported feeling embarrassment about breast cancer conversation with their family members as well as health providers, especially if they were males. About six (19%) women expressed the embarrassment feelings directly and were reluctant of seeking primary and secondary prevention measures if they perceived there was no problem. For example, one participant stated, “My experience was good, I go to the doctor to be reassured about my health . . . I don’t feel comfortable talking about my breast health if there is nothing wrong with me.” Another participant stated, “I am very shy person, I know it is not right.”
When women were asked if they knew a close friend or a family member who had been diagnosed with breast cancer, the response from 75% of the participants was they knew friends, neighbors, or relatives who had been diagnosed with breast cancer. This prompted fear and denial of being at risk for breast cancer. A participant shared her fears, stating, “I am afraid of this disease. I don’t know much about it, but I know when I had my breast abscess, the doctor told me that it was a benign tumor. . . . Cancer comes suddenly with no reason.” About eight participants (26%) also expressed their fear of fatality of cancer in general. One of the participants shared a story about a friend who died with breast and lung cancer, stating, “She did not notice or know the signs [of cancer], and she died with the cancer . . . she did not know that she had lung cancer.” Another one stated, “Yes, I hear about it often. I heard about my father’s cousin, they removed her breasts . . . they discovered it very late.”
The participants were asked about how much they knew about breast cancer and why it happens. While only two participants (6.5%) did not know anything about it, others expressed basic knowledge about the disease. Their knowledge was based on what they heard from the media, learned from newspapers, friends, family, and neighbors.
When they were asked about what causes breast cancer, and why it has risen recently, their answers were limited to factors related to the nature of the food grown in radioactive soil, smoke in the air, canned food, hormone instability, aging, and unknown reasons. For example, a participant said,
I think it happens because they used chemicals in the food, or radiation. Also, there is a rumor about using the leftover of metals after the Gulf war . . . they used it in building and maybe it has radiation that is why we got more cancer in Jordan.
The participants’ beliefs and attitudes toward what causes cancer were consistent. They blamed food preservatives and products as the primary factor for the sudden increase in cancer diseases. A participant stated, “Almighty Allah knows why cancer is happening, but the change in food, life style, lack of knowledge; ignorance, and environment may contribute to the breast cancer. The food now is not healthy. It has hormones.” However, about 70% suggested that screening or checkups are good if women are doubtful about their risk of getting the disease.
Many participants endorsed the use of folk medicine and prescribed herbs as the initial step to take care of health issues. A participant stated,
I don’t feel comfortable discussing breast health with him [physician]. But, I had a breast abscess in 1990, and I went twice to clean it up. I went to the hospital many times, but the abscess and drainage continued from my breast. I tried another prescription I learned from a journal that included boiling onion and garlic then drinking the juice. After a couple of times the drainage was dry and I had no abscess. I also prescribed this to another friend who had also infection, and she was recovered.
Another woman stated, “Oftentimes I use folk remedy and herbs to take care of my health issues. If that doesn’t help, I seek professional help.”
Theme 2: Health Care Professionals Were Not Quick To Offer Information and Education
Impressions and explications of Theme 2 include the following discussion: Women in the study shared their perceptions about their providers and their lack of focus on breast cancer screening during a medical visit. A participant stated, “No, they [providers] never told me anything except when I had my problem in 2005, and 2007. I never knew about mammograms.” In addition, it was rare in many cases for doctors or nurses to perform a clinical breast exam during a routine visit or medical exam. Women reported scheduling their medical visit to see the doctor with a particular medical issue, and that issue would be the focus of the visit. Another participant stated, “They [health providers] will not examine your breast, they will just ask you about your complaints and if you have pain. They focus on what you complain of.” Many women believed that if the doctor or nurse did not discuss or examine their breasts during the medical visit, then everything must be fine.
As previously mentioned, the women felt embarrassed about getting breast cancer screening, breast self-examination, or even talking about breast health, and would not bring these issue up with their physician or nurse during a medical visit. At the same time, neither the physician nor the nurse initiates the discussion of breast cancer, mammograms, or self- or clinical-breast exam. However, women in the study reported that they trusted and felt cared for by the health care professionals about other health care issues. They reported that physicians are very busy in the hospitals and do not have time to spend to discuss breast health.
About (65%) of informants in the study did not recall times when doctors and nurses would offer information either in writing or verbally about breast health or breast cancer screening, either in the medical facility or in the community. A few participants felt that women should also ask about the information they need, stating, for example, “They [providers] may not give you information, but you need to ask them about it. So you should be willing or ready to ask them for that.”
As far as practicing breast care, about eight women in the study (26%) stated that they know how to perform a self-breast exam, but they have not actually done it on a regular or consistent basis. Other women in the study did not know how to perform a self-breast exam, but they attempted to ask their health care providers about it.
Theme 3: Willingness to Learn About Breast Cancer and Prevention
Although the participants expressed fear, embarrassment, and denial about discussing breast health, they felt that if the physician or a nurse asked them about breast cancer, screening, or self-breast exams, they would discuss it. Twenty-four women (77%) expressed interest in learning about health and wellness in general and breast health in particular. They also said that during the visit with health care providers if information about breast cancer was provided, they would consider it seriously. One participant stated, “I attended many workshops about this subject when I was in college. Sometimes the ministry of health distributes flyers about breast cancer, and family planning (in Arabic, this program is called Tanthem Al Osrah).” Essentially, women expressed a common sentiment, “If you tell me I will listen, and if you teach me, I will learn.” This suggests they would be receptive if the health care providers brought up the issue with them during the medical visit.
Discussion
The present study provides an in-depth understanding of Jordanian rural women’s values and beliefs that influence their behavior related to breast health. It highlights the attitudes of Ma’an women toward breast health and mammogram screening. All the participants were Jordanians, Ma’an residents, and Arab traditional women, who take pride in their cultural and Islamic traditions. The study participants were very cooperative, open, and expressed their thoughts without hesitancy. The findings about women’s reservations toward breast exposure to providers suggested that they valued their own cultural and religious beliefs more than their own physical health. Despite their perceptions of fear, denial, and fatality about breast cancer, their strong defense mechanism is their deep beliefs in their destiny and the protection of the Almighty Allah (means God in Arabic) against cancer and other diseases. In this study, these cultural values and beliefs are consistent findings among Muslim women (Donnelly et al., 2013b; Kawar, 2013; Salman, 2012; Vu, Azmat, Radejko, & Padela, 2016).
The findings of this study are consistent with previous studies that have focused on Jordanian women. Kawar (2012) examined cultural conflicts related to cancer screening documenting that modesty, values, and beliefs influence decisions about screening. That study also found that women’s spouses may discourage or do not approve of seeking information about breast cancer. In contrast, the participants in the present study expressed the support of their husbands in seeking health care such as taking them to Amman city for better health facilities. For those who had no spouses, their sons and daughters took them for their medical visits. The researchers believe that the reason could be related to the geographic location of the city and the limited access to health care services in Ma’an.
Although age was not a focus of the interviews, it was noticed that older women (60 years and older) were more traditional in their beliefs and less interested in seeking knowledge or attention about breast health. This behavior may be explained by the feeling that after a woman has met society’s expectations related to marriage, having children, and reaching the menopausal age, breast health should not be important. This attitude was common among women regardless of their education and employment status, which may represent a barrier to early detection and prevention of breast cancer as women age.
Despite the fact that participants expressed their appreciation and trust in their health providers (especially physicians), neither women nor providers took advantage of the opportunity of a clinical visit to discuss breast health cancer prevention. The majority (about 65%) of women in the study did not recall times when doctors and nurses would offer information either in writing or verbally about breast cancer and breast cancer screening, either in the medical facility or in the community. The women indicated that they would consent to the screening if they were told about it. Results suggest that if health providers would be willing to educate them about breast health, women would be receptive.
Comparing Jordanian women’s findings to other Arab Muslim Middle Eastern women in other countries, it appears that Arab women’s beliefs and attitude about breast cancer may not be different. Donnelly et al. (2013b) found that modesty and embarrassment, fear of cancer, preference for female providers, and lack of provider recommendations were significant barriers among women from Qatar. Their study results were consistent with Kawar’s study (2013) on Palestinian and Jordanian women living in the United States.
Many participants heard about an increase in prevalence of breast cancer in Jordan, but they did not understand the cause. They believed that cancer is a fatal disease, with a very limited understanding based on information obtained from family, friends, community, and media. Women identified two facilities in the city, which lacked mammogram screening maintenance and were dysfunctional. As a result, all mammogram referrals can only be done in Amman city (approximately 215 km away). They claimed that there is a shortage of trained staff who are prepared to provide health education and screening. These above noted challenges may partially explain women’s delay to see a provider when a health issue arises.
Implication
The main findings of the study include the value of women’s cultural beliefs, lack of awareness about breast health, barriers to accessing health services, shortage of suitably qualified nurses, and lack of the nursing role in prevention and health education. Health care providers including nurses may capitalize on women’s willingness to learn and follow health provider advice. Female nurses from the community can serve as advocates for women, identify community resources, educate women on breast health, serve as a health agent or a liaison between community members and policy makers, and prepare effective programs to reduce the burden of the disease. Since cancer probability increased with age, a special focus on the woman as she ages is recommended. Authorities and health policy makers can increase the number of mammogram screening units and consider a mobile facility for serving rural communities.
Conclusion
Our findings address very important personal and systemic barriers, which may explain the high incidence of morbidity and mortality of breast cancer among Jordanian women at a younger age. From the nursing perspective, these findings are very important, as they stress the importance of the integration of gender-concordant care as a basic component of cultural competent care for Middle Eastern women. In clinical practice, the availability of female providers, including nurses, may encourage women to engage in patient-centered interactions and ask questions, express concerns or fears, and disclose false beliefs about breast cancer. Education is paramount to changing women’s behavior and attitudes. Successful educational strategies are those that aim at changing behavior without jeopardizing the existing cultural values and beliefs. If modesty, shyness, and breast exposure influence women’s decisions, then effective education strategies should not only focus on breast health but also on the differences between religious and cultural modesty. It is well known among Muslims that the Islamic principles encourage self-care, and women are allowed to expose parts of their bodies for health reasons. To overcome cultural barriers, women with previous experience of breast cancer screening should be encouraged to talk about their experiences to others who have not had the screening.
The systemic challenges were demonstrated by the disparities noted between the infrastructures and resourcing in rural and urban areas of Jordan. The role of the Ministry of Health (MOH) should not only focus on providing health resources but also establishing health education programs to target rural women via media, radio, television, newspapers, schools, religious places, and shopping centers to motivate them. The MOH and Al-Hussien Bin Talal University can work effectively to train nurses regarding breast assessment and mammography screening through workshops, presentations, and education programs. The MOH can support and mobilize additional resources for health promotion programs targeting the public in rural Jordan with respect to breast assessment and cancer screening.
Footnotes
Acknowledgements
This study was a collaborative international research effort between Schools of Nursing at Duquesne University and Al-Hussein Bin Talal University in Ma’an governorate. The research was made possible by Duquesne University School of Nursing Faculty Development Grant and the support and collaboration of the School of Nursing at Al-Hussein Bin Talal University. The researchers are very grateful to the key informants who helped us in recruiting the participants. Our special and sincere thanks also go to all the women participants who welcomed us into their homes and allowed us to collect the data.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Duquesne University School of Nursing Faculty Development Grant.