
Abstract
Background
Schools of nursing prepare their graduates to meet the needs of diverse patient populations by providing cultural diversity education in their curriculum, which is an integral component of undergraduate nursing education in the United States (American Association of Colleges of Nursing [AACN], 2016). Cultural diversity education in nursing involves educational sessions on cultural diversity, awareness, and sensitivity which provides students with opportunities to gain knowledge, skills, and understanding to improve the quality of patient care. Diversity education promotes patient-centered care through its recognition and elucidation of cultural difference among patients, including their varied preferences and perspectives, reflective of their specific values, spirituality, race, ethnicity, gender, and sexual orientation.
Colby and Ortman (2015) estimated that by 2044 over one half of all people within the United States will be composed of a minority group. Because of the increasing diversity within the United States, Wilson et al. (2012) comment that students in all health professions must focus on local, regional, national, and international health care problems. An emphasis on global health gives students the skills necessary to provide clinically competent, safe, and culturally appropriate care for all people (Wilson et al., 2012).
The AACN (2008) lists cultural diversity as an Essential of Baccalaureate Nursing Education and has developed a tool-kit to assist faculty by providing resources for content learning and teaching–learning activities to facilitate implementation of cultural competencies in baccalaureate nursing education. While schools of nursing seek to include diverse learning experiences that address the application of culturally sensitive care practices, increasing patient acuity and faculty shortages affect the ways cultural diversity is delivered in the nursing curriculum.
In most of the cultural diversity literature, there is an agreement that cultural diversity must be taught in nursing education. Throughout nursing literature there are different models, strategies, and methods of teaching cultural diversity, but there is little agreement over the best teaching approach (Paroz et al., 2016). Shen (2015) suggests there has been a lot of work done to create cultural diversity models and assessment instruments, but very few have undergone the rigorous psychometric testing and retesting to obtain high validity and reliability. Shen also states that more work needs to be done to measure patient outcomes which will evaluate the clinical cultural diversity education.
Davis and Davis (2010) suggest that before nurse educators teach cultural diversity, they must first educate themselves, formally, by taking a transcultural nursing course. Beard (2014) has suggested that faculty participate in workshops regarding cultural diversity. Songwathana (2013) believes that nurse educators should actually spend time with other cultures that are culturally different from their own. Once nurse educators have a solid background they can plan other learning opportunities for students. Carlson (2016) suggests that clinical faculty can look for learning opportunities with diverse populations for students, while others suggest placing students in communities and/or using simulation, role-playing, or storytelling. Online education approaches have included adding other activities such as blogging, recorded lectures, cultural immersion, and use of social media (Arbour, Kaspar, & Teall, 2015).
Culture is the shared beliefs, attitudes, values, and practices of a particular group of people. Such groups may distinguish themselves by socioeconomic class, race, ethnicity, color, religion, gender, sexual orientation, nationality, physical disability, or some other specific characteristic. The values and beliefs of the group guide and influence their behavior and social interactions, including the use of alcohol and other substances. Many culturally distinct groups use alcohol or other drugs with established codes of behavior that affect their approach to substance use (Abbott & Chase, 2008). The use of substances, including alcohol, illicit drugs, and prescription medications (such as benzodiazepines and narcotics), may be a learned behavior associated with the lifestyle of a certain culture. For many groups, culture may also play a protective role against the abuse of substances. It is crucial to note, therefore, that treatment for substance use disorders must be sensitive to cultural differences. For example, a study found that individuals of a specific ethnic group did not seek alcohol and drug treatment from a local program because it lacked staff of that certain cultural group (Abbott & Chase, 2008). Additionally, providers caring for patients with substance use disorders should refrain from making ethnocentric assumptions based on their cultural preferences. Thus, culturally competent care is vital to providing effective, quality care to patients with substance use disorders. Cultural diversity education can provide nurses with the necessary knowledge base and skill set to effectively work with and provide quality care cross-culturally.
Another aspect of cultural diversity education within nursing is the varied prevalence of alcohol, tobacco, and/or other drug use/misuse among patients of various cultural, ethnic, racial, and socioeconomic backgrounds. For example, Caucasians, persons reporting two or more races, and African Americans are more likely than other racial/ethnic groups to report current use of alcohol; moreover, the rate of current tobacco and illicit drug use is highest among persons of two or more races, American Indians, and Alaska Natives (Substance Abuse and Mental Health Services Administration [SAMHSA], 2011). Wilson et al. (2012) argue that nursing school curricula should focus on international health and should address social, economic, and political factors affecting health systems. Use of substances (e.g., alcohol, tobacco, illicit drugs, or misuse of prescription medications) is one such social factor.
To address both cultural diversity and patient substance use in nursing education, a curriculum integration project has been initiated and sustained at a school of nursing affiliated with a large, academic, medical center (Burns et al., 2012). The project provided educational and skill-building activities to educate students to use screening, brief intervention, and referral to treatment (SBIRT) for alcohol and other drug use. This project, known as the Addiction Training for Nurses using SBIRT (ATN-SBIRT), was first introduced to students within their psychiatric–mental health nursing course during their junior year. The purpose of the project was to see if the students were able to apply their knowledge in a series of clinical rotations including medical–surgical, obstetric, and pediatric nursing (Mitchell et al., 2013). The medical–surgical course incorporated simulation as a method for students to practice and apply their knowledge and skills in culturally diverse scenarios. The ATN-SBIRT curriculum addressed a global health issue (substance use) and taught an evidence-based practice (SBIRT) while addressing culture as articulated in the Essentials of Baccalaureate Education for Professional Nursing (AACN, 2008).
As defined by SAMHSA, SBIRT is an evidence-based, public health model that is designed to provide universal screening, secondary prevention (or selective prevention/early intervention), brief interventions, and referral to treatment for individuals who have hazardous or harmful alcohol use within primary care and other health care settings. Teaching undergraduate nursing students SBIRT is timely and relevant. As of 2015, over 27 million people in the United States reported current use of illicit drugs or misuse of prescription drugs, and over 66 million people reported binge drinking in the past month (Center for Behavioral Health Statistics and Quality, 2016). Moreover, more than half (i.e., 66.6%.) of Americans aged 12 or older self-reported drinking alcohol, 25.5% reported using a tobacco product, and 9.4% reported using illicit drugs (SAMHSA, 2016). In 2015, an estimated 27.1 million Americans aged 12 or older were current (past month) illicit drug users as well (SAMHSA, 2016). Concerning substance use/misuse of this magnitude, SBIRT has been found to be an effective intervention, especially for addressing alcohol use. In 2003, SAMHSA instituted the largest screening and brief intervention service program of its kind across the United States, which has, since 2008, screened 690,000 individuals (Madras et al., 2009). According to Madras et al. (2009), 22.7% of participants screened positive for a spectrum of use (i.e., risky/problematic use, and use/misuse/substance disorders). In the study, among those who screened positive and received a brief intervention at baseline for heavy alcohol use, 38.6% reported lower use of alcohol at the 6-month follow-up (Madras et al., 2009). After the screening and brief intervention, Madras et al. (2009) observed improvements in general health, mental health, employment, housing, and criminal behavior.
Cultural Diversity
Culture has been defined as the way of life of a group of people that includes the sum of their beliefs, behavior patterns and practices, norms and attitudes, customs, and rituals (Luquis & Pérez, 2008). Culture is both complex and dynamic. Most people understand culture in its broadest sense and usually interpret culture as a something that characterizes distinct groups (e.g., Hispanic, African American, Asian American, etc.). Given the cultural diversity of the United States, nursing faculty often find it challenging to determine what aspect of culture to emphasize in order to maximize program success and build the cultural diversity of their students (Luquis & Pérez, 2008). Moreover, the approach to diverse health care delivery is shaped by one’s own cultural lens and can be subjective. In other words, culture is like looking through a one-way mirror: What we see is based on our own perspective (Lynch & Hanson, 1998). For this reason, educating students to become aware of what beliefs and practices shape their own cultural identity is important so they can then become culturally sensitive to the patients under their care.
Through cultural diversity education, health care providers can transcend cultural differences to enhance positive health outcomes among patients, rather than allow cultural misunderstanding to hinder health care delivery (Office of Minority Health, 2013). The AACN (2008) provides several rationales for incorporating cultural diversity into nursing education in order to address disparities in health and health care, promote justice and human rights among vulnerable patient populations, and respond to global infectious disease epidemics and chronic diseases. The strategies for increasing cultural competence may involve knowledge, creativity, and experience. Developing competencies by practicing with “real-life” patients may be an ethical issue because of the potential threat to the safety of the patient, as well as to the nursing student. Therefore, simulation can provide a safe, alternative approach to education. Most important, changes in health care delivery require that we develop new and creative methods for facilitating interprofessional, culturally based education. Through cultural competence, nurses can provide more equitable quality care to their patients that can, in turn, help reduce health disparities for minority populations.
Utilization of Simulation
Simulation has been used as an instructional method in a wide variety of venues and industries including health care, aviation, and education. This evidence-based learning strategy is becoming an increasingly popular teaching method in nursing education because highly complex work environments and higher patient acuity necessitate the provision of safe care. Moreover, the use of simulation in nursing education is an attempt to reproduce the essential features of a clinical situation. Simulation is a versatile pedagogical method, and it has been proven to improve teamwork, increase patient safety, and decrease patient errors without putting real patients at risk (Salas, Paige, & Rosen, 2013). Furthermore, simulation has advantages including that there is no risk to actual patients and students are able to practice and make mistakes in a safe environment. Simulation can be used to provide not only real-life learning experiences for students and other health care professionals but also provide the opportunity to practice newly learned concepts and skills; and, in this case, cultural and SBIRT assessment skills. As nursing students learn advanced communication and technical skills in a simulated environment, they are able to begin to bridge the gap from theory to practice. Simulation may also assist students and professionals to develop confidence in their abilities and improve their decision making. Simulation is now widely utilized by many schools of nursing in both the undergraduate and graduate nursing programs since approved by the National Council of State Boards of Nursing (Hayden, Smiley, Alexander, Kardong-Edgren, & Jeffries, 2014).
Tharp (2012) describes the concept of four dimensions of cultural competence for students and faculty. These dimensions are as follows: (a) be aware of and own your social identity and its impact on others; (b) know and apply social identity development theories; (c) recognize how multiple social identities and power interfere with society on an individual, community, and institutional level; and (d) carefully consider approaches to curriculum development and facilitation of diversity education (Tharp, 2012). Indeed, simulation provides this opportunity for students. Furthermore, Tharp (2012) contends that cultural competence and diversity education advance students’ development toward cultural competence. Simulation also provides the students with an opportunity to make strong connections to other social identities and constructions such as nationality, race, sex, gender, sexual orientation, religion, social class, and (dis)ability (Tharp, 2012). Cultural simulations offer a way to expose nursing students to care of patients of diverse backgrounds, while practicing in a safe environment (Bahreman & Swoboda, 2016).
Method
One strategy used within the ATN-SBIRT training program was to specifically teach an approach of cultural sensitivity. The students were taught a module on the Developmental Model of Intercultural Sensitivity (Bennett, 1993). The Bennett model defines intercultural competence across a continuum of experiences in which people experience culture from ethnocentrism (privileging one’s own culture in perceiving the world) to ethnorelativism (embracing many viable possibilities in perceiving the world; Bennett, 2004). Bennett (2004) also describes six experiences across the intercultural continuum. The six experiences are as follows: denial (i.e., denies any cultural differences); defense (i.e., defends cultural differences); minimization (i.e., minimizes cultural differences); acceptance (i.e., accepts cultural differences); adaptation (i.e., adapts to cultural differences); and integration (i.e., integrates cultural differences into one’s identity).
The ATN-SBIRT program also utilized simulation to ensure that all students encountered diverse patient situations that they may not have otherwise encountered during their clinical rotations. The simulations featured in ATN-SBIRT also allowed the faculty to combine patient culture and substance use issues in a format where students could deliver and later reflect on their choices and communication around these two specific areas. To contribute to a student’s readiness to practice in a multicultural environment on graduation, the University of Pittsburgh School of Nursing partnered with the Institute for Research, Education and Training in Addictions (IRETA) to develop and integrate a sustainable educational and skill-building program within the undergraduate nursing curriculum (Burns et al., 2012). The ATN-SBIRT training program includes an SBIRT seminar for junior-level nursing students in a psychiatric–mental health nursing course. Students were then expected to practice, utilize, and apply the newly learned skills in their medical–surgical and other clinical courses. The University of Pittsburgh School of Nursing faculty and the IRETA training staff specifically designed multiple, culturally diverse scenarios incorporating SBIRT concepts to ensure the scenarios adequately addressed age, gender, race, and culture. After the students received the SBIRT content, they reported to the simulation center in small groups during one of their clinical days.
According to The International Nursing Association for Clinical Simulation and Learning, “Standards of Best Practice: SimulationSM,” faculty utilizing simulation-based learning have an ethical obligation to review with students the rules of simulation, expectations, and behaviors that will be analyzed during the scenarios and the debriefing process (INACSL Standards Committee, 2016). Students were made to feel safe in their learning environments and realize that these scenarios and debriefing exercises are meant to be nonjudgmental and a tool for learning. Students were to maintain professional integrity regarding the simulation and show mutual respect for one and other. Additionally, students were also instructed to keep the scenarios confidential. The faculty and students were very familiar with the school’s rule of what happens in the sim lab stays in the sim lab.
Using high-fidelity simulation, students were informed that they should respond to the mannequin as if it were a real patient. One faculty member orchestrated the scenarios, while the other faculty member sat with a group of students in a classroom and watched the scenarios via live camera feed. At the end of each scenario, students were encouraged to discuss what went well during the simulation and what could have been done to improve the simulations. Both students and faculty participated in debriefing sessions. The debriefing sessions provided respectful, constructive feedback not only on the cultural component but also on how the student performed during the scenario. Bahreman and Swoboda (2016) believe that debriefing is a critical aspect of simulation because the process helps guide students through the simulation learning with reflection, and it allows them to apply theory to practice. The debriefing process states that simulation-based learning should always include a planned debriefing that helps students promote reflective thinking. As a result, students enhance their learning, build their confidence, and transfer the knowledge and skills they have learned (Decker et al., 2013).
As an addition to the high-fidelity simulation experience, the scenarios were expanded to include producing three videos to be used in future simulations. A standardized patient (SP) and a small group of students participated in making the videos that contained common culturally sensitive mistakes that health care providers make with patients. These multicultural medical–surgical/psychiatric nursing scenarios included the following: (a) a first-semester African American college student misusing prescription dextroamphetamine/amphetamine (Adderall) and cocaine, (b) a Middle Eastern woman accompanied by her husband, coming to the emergency department with abdominal pain, and (c) a postsurgical Hispanic female who had difficulty communicating with the nursing staff regarding her use of alcohol, pain medication, and fluid intake. Students were asked to view the videos and document what was done correctly and incorrectly. Each scenario was debriefed and an open discussion occurred regarding the cultural aspects presented in the video. These discussions included religious belief practices, nutritional preferences, communication styles, patient care issues, and handling of death.
Procedures
This project was exempt through the University of Pittsburgh School of Nursing Institutional Review Board. Students were informed that completion of surveys was voluntary, participation would not affect their course grade, and their responses were confidential. Students voluntarily signed consents for participating in the project.
Participants
The participants were 183 junior-level baccalaureate nursing students at the University of Pittsburgh School of Nursing. The students completed a cultural diversity survey, which also included demographic information, presimulation, and several weeks following the additional SBIRT training they received in their junior psychiatric–mental health course. The majority of the students were female (n = 157; 85.5%). Five participants reported being Hispanic (2.7%). Concerning race, 166 (90.7%) reported being Caucasian, 12 (6.6%) Asian, 3 (1.6%) African American, and 2 (1.1%) American Indian. The mean age of the students who participated in the simulation was 24.2 years (range 21 to 44 years). Complete data at presimulation and postsimulation were available for 119 students.
Instruments
In 2003, Schim, Doorenbos, Miller, and Benkert described initial testing of an instrument to measure cultural competence among health care providers. The Cultural Competence Assessment (CCA) was based on the cultural components of fact, knowledge, attitude, and behavior. At that time, expert panel reviews and field testing confirmed content and face validity (Schim et al., 2003). Internal reliability and validity with a group of 113 hospice health care providers demonstrated an internal consistency reliability of 0.92 (Schim et al., 2003).
The CCA includes demographic, employment, and training items. It consists of 44 items over two subscales: the Cultural Awareness and Sensitivity Subscale (CAS) and the Cultural Competence Behavior Subscale (CCB; Doorenbos, Schim, Benkert, & Borse, 2005). The CAS measures cultural awareness and sensitivity by using on a 5-point Likert-type scale with responses ranging from strongly agree, agree, strongly disagree, disagree, and no opinion. The CCB measures cultural competence behaviors that include five response categories from always, often, at times, never, and not sure. The combination of the CAS and the CCB scores generate the CCA score (Doorenbos et al., 2005). The higher the score, the higher the knowledge, the more positive the attitude, and the higher the cultural competence. In addition, items query experience with culturally diverse groups, including self-ratings of cultural competence. The tendency to provide socially desirable responses was assessed via items from the Marlowe–Crowne Social Desirability Scale (Reynolds, 1982) that are included in the CCA.
In order to examine the test–retest reliability of the CCA, Doorenbos and colleagues used a sample of 51 hospice health care providers who completed to instrument at two time points. It demonstrated satisfactory test–retest reliability (r = .85, p = .002), as well as the CCB (r = .87, p = .002) and CAS (r = .82, p = .002), which also demonstrated high correlations over the 4-month period (Doorenbos et al., 2005). Internal consistency reliability and construct validity in nonhospice settings were evaluated in a sample of 405 health care providers. In this sample, the overall internal consistency reliability for the CCA was .89 and Cronbach’s alpha for the CCB (.91) and CAS (.75) were reported, indicating acceptable reliability for the two subscales (Doorenbos et al., 2005). The CCA has been used multiple times with statistically significance in improvement of cultural competence after education. Reyes, Hadley, and Davenport (2013) utilized the CCA to perform a comparative analysis of cultural competence for beginning nursing students and then for graduating nursing students. The graduating nursing students perceptions of cultural competence were significantly higher (p = .002) than the perceptions of cultural competence for beginning nursing students. Most recently, Doorenbos, Morris, Haozous, Harris, and Flum (2016) found that participation in diversity training was the variable most significantly associated with CCA scores (p < .001).
Data Analysis
Students’ opinions of the simulation learning experience were examined through response frequencies. Next, CCA item response frequencies were recorded and examined to describe students’ self-ratings of cultural competence at presimulation and postsimulation. CCA subscale scores were inspected to assess normality and check for outliers. To determine whether students’ self-ratings were statistically different over time, paired t tests were run for each of the two CCA subscales using 119 students with complete data at presimulation and postsimulation. Statistical analyses were performed using SPSS (IBM SPSS Statistics, Version 22) software with a significance level of .05.
Results
Analyses of the CCA subscales showed an increase in the undergraduate nursing students’ perceptions of culture and their cultural competency (Figure 1). The students’ self-ratings of cultural awareness and sensitivity, t(118) = −7.07, p < .001, increased significantly from presimulation to postsimulation experience. Likewise, their cultural competence and behavior, t(118) = −5.87, p < .001, also increased significantly from presimulation to postsimulation.
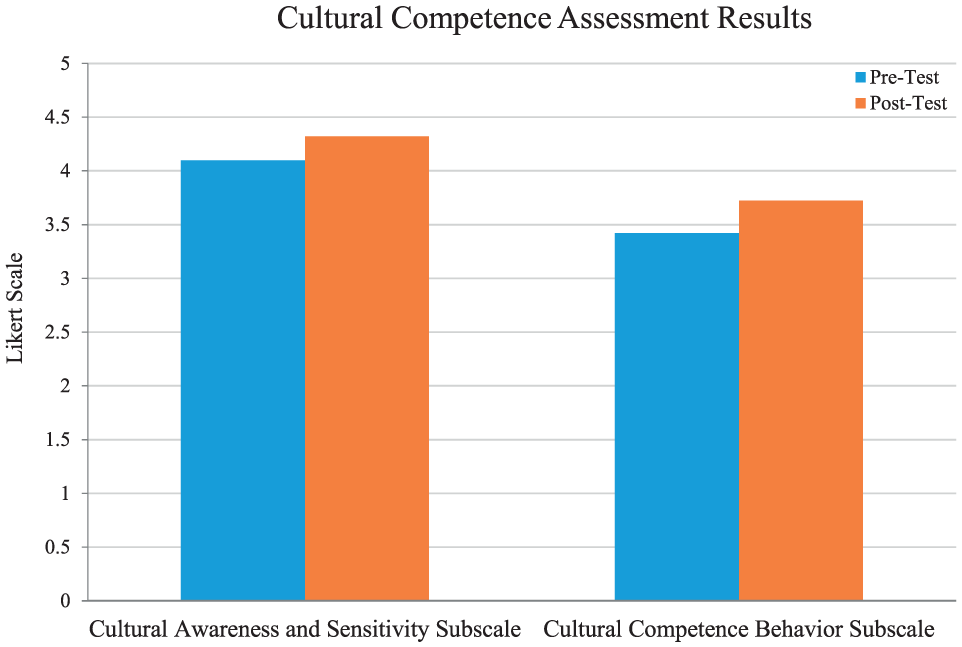
Cultural competence assessment results.
In general, prior to this specific simulation exercise, 47% of these undergraduate nursing students felt that simulation was an effective tool for learning and 14% felt that simulation was a very effective learning tool. After the present simulation experience, 72% of the students felt that the simulation was generally a very effective learning tool.
Specifically in relationship to teaching cultural competency in this project, 61% of the undergraduate nursing students reported that they valued the simulation experience for teaching cultural diversity and 73% thought the simulation scenarios were an effective learning tool. Although we do not have exact numbers, qualitative notes identify that some of the remaining 39% of the students reported that they were embarrassed and afraid to make mistakes in front of their peers and professors. Additionally, students commented that participating in simulation caused them anxiety, which is a common theme in simulation (Willhaus, Averette, Gates, Jackson, & Windnagel, 2014). However, in the postsurvey, 91% of the students felt that they were more comfortable and able to apply culturally competent knowledge that they learned during the simulation scenarios and the corresponding debriefings. Moreover, students communicated an increase in not only their awareness and understanding of culture when working with patients but also their ease in applying SBIRT techniques to address alcohol and other drug use while treating patients with cultural backgrounds different from their own.
Discussion and Limitations
This project demonstrates that using simulation to promote cultural diversity among undergraduate nursing students has many advantages. There are no risks to actual patients, students are able to practice and make mistakes in a safe environment, and part of the simulation includes learning from the mistakes. As undergraduate nursing students learn advanced communication and technical skills in the simulated environment, they are able to bridge the gap from theory to practice. Even though there is a lack of robust research that supports the best debriefing methods, debriefing after a scenario is where much of the learning takes place.
Cultural diversity education can be embedded in teaching the broader evidence-based practice of SBIRT to undergraduate nursing students through simulation. The culturally diverse simulation scenarios promoted cultural engagement rather than cultural stigmatization, while students learned how to screen and intervene with patients who use substances. Other schools of nursing could benefit from a curriculum that combines the concepts of cultural diversity, SBIRT, and simulation. Simulation provides an opportunity for faculty to address a cultural competency within a safe environment (Tharp, 2012).
Limitations and Lessons Learned
A limitation to this project was using SPs for the first time, while the faculty were not familiar with the specific training needs and expectations of using SPs. The SP population at the University of Pittsburgh prefers to be given detailed scripts in advance because it helps them better assume the patient role, including verbal and nonverbal communication, clothing, emotions, and the expected learning outcomes. By receiving the simulation scripts in advance, the SP can ask questions about the scenarios and their roles prior to simulation. The SPs are taught to follow scripted scenarios and “stay in character.” At the end of the scenario, the SP provides verbal feedback to each student regarding the scenario, while the faculty conduct a debriefing to discuss observations of the student’s clinical performance. Szauter (2014) agrees that when adding SPs to a simulation scenario, it requires careful preparation and planning to ensure that the SP enhanced rather than derailed a scenario.
This project included high-fidelity simulation and the production of videos in a simulation lab utilizing SPs and a small group of students. These videos were produced to be used again with all junior-level psychiatric–mental health and medical–surgical nursing students. The videotaped simulation scenarios did not feature scripted dialogue, but rather general themes related to culture and SBIRT. Because the videos were not scripted, some components of the cultures and SBIRT implementation were not always portrayed as the faculty would have preferred. However, feedback during the debriefing process opened the door to rich discussions on the importance of health care professionals being culturally competent. The videos were a tool to help develop an environment in which the nursing students could practice both SBIRT and cultural diversity skills. After watching the videos and debriefing with students, faculty have an avenue to discuss common themes, open lines of communication, and provide constructive feedback through critiquing, correcting, and evaluating the students.
Conclusions
Simulation allows nursing students to address health disparities that may have a cultural dimension, such substance use/misuse (Tharp, 2012). In this project, 91% of undergraduate nursing student participants reported they were able to apply what they had learned through debriefing of the simulation exercises and the simulation videos. Junior-level nursing students significantly increased their cultural awareness and sensitivity toward patients who use alcohol or other drugs. Furthermore, post simulation, they were able to demonstrate more culturally competent behaviors while interacting with patients who are using substances. This project provides an example of creative learning through simulation to address two patient health issues: health care provider’s cultural competence and patient’s alcohol or other drug use. Future studies could examine student differences at baseline, their experiences with culturally diverse groups, and students’ report of change in experiences in the actual clinical arena, from presimulation to postsimulation. This educational training and skill building model could also be expanded from undergraduate nursing classrooms to utilization within clinical practice settings with practicing nurses in orientation or residency programs.
Footnotes
Authors’ Note
The information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by the Division of Nursing, BHPr, HRSA, DHHS, or the U.S. Government.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported in part by funds from the Division of Nursing (DN), Bureau of Health Professions (BHPr), Health Resources and Services Administration (HRSA), Department of Health and Human Services (DHHS) under Grant Number D11HP14629, “Addiction Training for nurses using Screening, Brief Intervention and Referral to Treatment” (ATN-SBIRT).