
Abstract
Introduction
During the past two decades, the escalating prevalence of childhood obesity has become a global epidemic and public health issue (Karnik & Kanekar, 2012). In China, approximately 22% of children 2 to 6 years of age are now overweight or obese (Piernas et al., 2015). Data show that with children as with adults, unhealthy eating behaviors are associated with higher risks of obesity. These behaviors include eating in response to stimuli other than hunger and unhealthy eating style (such as eating in front of a TV; Marsh, Ni Mhurchu, & Maddison, 2013; Zong, Li, & Zhang, 2015). Data also show that physical activity and sedentary behavior can affect a child’s ability to maintain healthy weight (Cárdenas-Cárdenas et al., 2015; Schaefer et al., 2015). Preschoolers who spend less time in vigorous daily activity have higher body fat and are at greater risk for being overweight. Not surprisingly, in China and throughout the world, important predictors of overweight and/or obesity status in children are TV viewing time and amount of physical activity in preschool populations (Mendoza, McLeod, Chen, Nicklas, & Baranowski, 2014; Zong et al., 2015). Given this research evidence on diet and physical activity, interventions to reduce and prevent childhood obesity must focus on improving children’s healthy eating behaviors—and also on increasing children’s physical activity and reducing their sedentary activity.
Maternal Influence on Children’s Eating Behavior
Mothers can improve their children’s eating behavior and physical activity and sedentary activity by modeling their own adult behavior and by explaining in simple language the cognitive processes that determine how they, as parents, make healthy food and activity choices for their children. Maternal personal practices such as the use of healthy feeding practices (e.g., not pressuring children to eat, restriction of food, monitoring, and control of dietary intake), role modeling (e.g., physical activity and eating behaviors), and structuring of a healthy home environment as well as maternal self-efficacy in encouraging weight-related healthy behaviors have been shown to be associated with a child’s eating and physical activity behaviors (Schoeppe & Trost, 2015; van Ansem, van Lenthe, Schrijvers, Rodenburg, & van de Mheen, 2014). Parents’ feeding practices affect their children’s risk for obesity both directly (via demands or restrictions) and indirectly (via modeling or monitoring; Collins, Lacy, Campbell, & McNaughton, 2016; Kiefner-Burmeister, Hoffmann, Meers, Koball, & Musher-Eizenman, 2014).
Maternal Self-Efficacy
Maternal self-efficacy in making healthy food choices for a child may influence a child’s eating and activity behaviors. Self-efficacy is an important aspect of social cognitive theory introduced by Albert Bandura (1989). Self-efficacy is well studied and has been shown to relate to weight-related behaviors in children. For example, data suggest that parental self-efficacy is related to children’s eating and physical activity behaviors (Campbell, Hesketh, Silverii, & Abbott, 2010; Knowlden & Sharma, 2016; Koh et al., 2014). Given that in most families, the mother is the primary caregiver, the impact of her self-efficacy on her children’s health and weight-related health behaviors may be considerable. Although some investigators have examined the influence of maternal self-efficacy on children’s weight-related health behaviors (Knowlden & Sharma, 2015; Xu, Wen, Rissel, Flood, & Baur, 2013), to our knowledge, most of this research has been conducted in Western countries.
Early Childhood Eating and Activity Behavior
Early childhood is a critical period in the development of eating patterns and activity behaviors that may influence weight and health outcomes in later childhood and adulthood (Donin et al., 2014; Santos, Pegoraro, Sandrini, & Macuco, 2008). The few studies conducted in mainland China have identified multiple risk factors for overweight and obesity in preschool-age children: parental overweight, low maternal education level, food restriction, increased TV viewing, living in rural areas, and the introduction of solid food before a child is 4 months of age (Jiang et al., 2006; Zhang et al., 2009; Zheng et al., 2014; Zheng et al., 2015; Zhou et al., 2011). Thus, the purpose of the study was to examine the influence of maternal factors on children’s eating behaviors and physical activity, especially in Chinese preschool-age children. The research questions of this study include (a) What are the Chinese preschool-age children’s weight-related health behaviors (eating behaviors, physical activity, and home environment)? (b) What are the maternal feeding practices, maternal self-efficacy regarding encouragement of healthy eating, and physical activity? and (c) What are maternal factors that are associated with a child’s weight-related health behaviors in Chinese children in China?
Method
Study Design
This study used a cross-sectional study design. Mothers completed questionnaires regarding family eating and activity habits, child feeding practices, and maternal self-efficacy regarding their child’s health-related health behaviors.
Setting
Mother–child dyad participants were recruited from four preschools in urban and suburban Hunan Province in South Central China.
Sample
A mother–child dyad was eligible for study participation if (a) the mother and child identified as Chinese, (b) the child was 3 to 5 years of age and able to attend regular preschool activities, and (c) the mother was able to read and write in Mandarin Chinese. Preschool directors provided names of eligible participants. Potentially eligible participants were contacted by research assistants who are Chinese and were trained by the research team in recruitment and data collection methodology. Mothers of potentially eligible preschool children received an invitation letter describing the study and research consent forms. Interested mothers signed and returned the consent form within 2 weeks and children provided verbal assent for study participation. The response rate was about 50%. Participant mothers completed a set of questionnaires at home and their children had their weight and height measured at preschool sites. As an expression of appreciation for family members’ time, each family received a gift equivalent to US$5.00 after the family members returned their completed questionnaires. Human subject approval was obtained from the University of California San Francisco Committee on Human Research and the Central South University in China. Data were collected between October, 2015 and January, 2016.
Measurements
Mothers were asked to complete demographic questionnaires that inquired about parent and child demographics, maternal control practices, self-efficacy, and eating and physical and sedentary activity habits (Table 1). Children’s weight and height were measured. Weight data were analyzed separately and submitted for publication elsewhere (Chen, Guo, Esquivel, Chesla, & Tang, 2017). All questionnaires were previously translated into Mandarin Chinese and back translated to English. To ensure cultural and linguistic appropriateness, the questionnaires were then pilot tested with a small group of participants (eight mothers). All measures and study procedures employed had been previously used and tested in Chinese populations and had been found to have adequate psychometric properties.
Measurement Subscales.
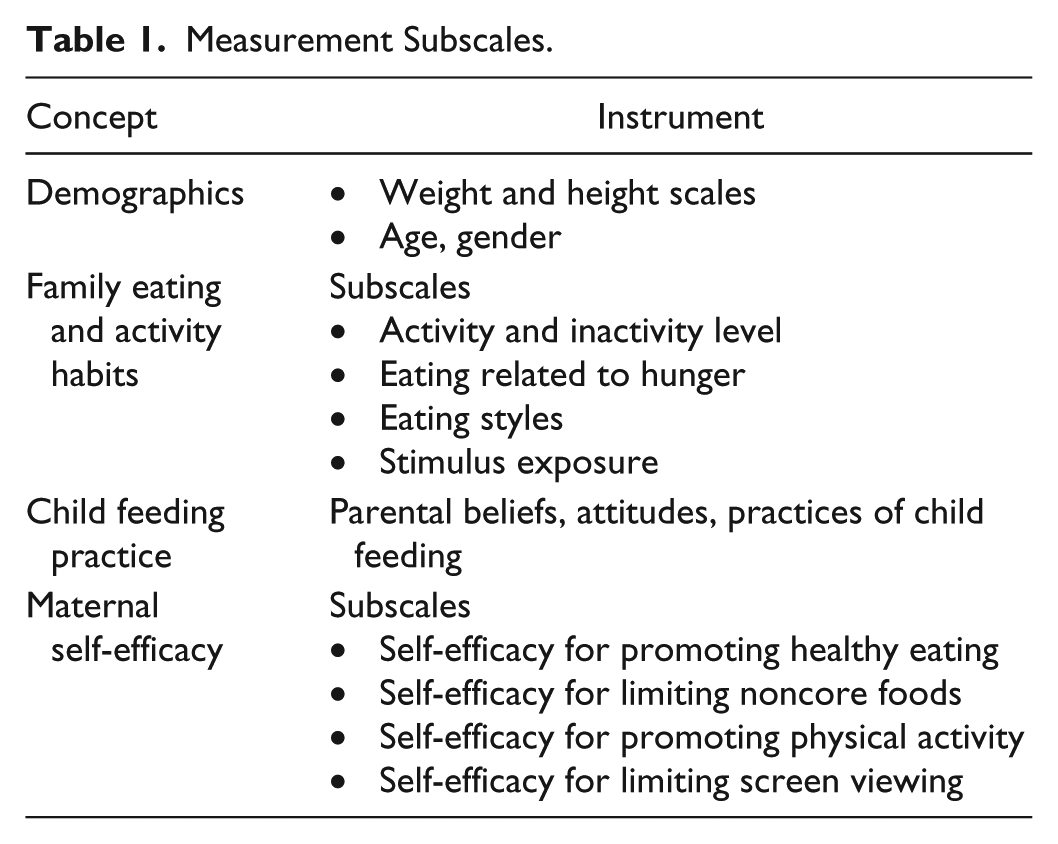
Family demographic survey
Mothers completed a demographic survey of the parent(s) and children. Data included ages of family members, child’s birth weight, parent(s)’ weight and height, parent(s)’ occupation(s), family income, and parent(s)’ educational level. Current weight and height of children were assessed by trained research assistants at the study sites.
Family eating and activity habits
Mothers completed the Family Eating and Activity Habits Questionnaire (FEAHQ), which was used to assess the mother’s, father’s, child’s eating, and activity behaviors (Golan & Weizman, 1998). The 29-item questionnaire has four subscales: activity and inactivity level (computer and TV time), eating related to hunger, eating styles, and stimulus exposure. The activity and inactivity subscale (four items) measures activity frequency including activity outside of work or school for which the parent, spouse, and obese child is engaged. The eating habits and style subscale (12 items) measures (a) eating while standing in front of an open refrigerator or from the stove; (b) eating during TV viewing, doing homework, or reading; (c) eating following an experience of stress (anger, frustration, boredom); (d) eating between meals; (e) eating at night; (f) habits of asking for or taking a second helping; (g) eating pace; and (h) frequency of family meals. The internal hunger and satiety cues subscale (three items) measures family members’ responses to hunger and satiety cues and assesses eating initiator provocation. The stimulus exposure subscale (13 items) measures the presence and visibility of snacks, sweets, cakes, and ice cream in the home; boundaries of the child’s autonomy in buying or taking these types of foods; and parents’ presence during meals. Scores were calculated separately for each family member, with higher scores reflecting poorer eating habits and sedentary behaviors. The FEAHQ has an established validity and internal consistency and ranged from .78 to .88 (Golan & Weizman, 1998). In the present study, internal consistency ranged from .68 to .83.
Child feeding practices
The Child Feeding Questionnaire (CFQ) is a 31-item self-report measure that assesses parental beliefs, attitudes, and practices regarding child feeding. The CFQ queries respondents about four factors that influence parents’ beliefs regarding a child’s proneness to obesity: perceived parent weight, perceived weight of their child, parental concern about a child’s weight, and parental feeding responsibility. Three additional factors assess parental control attitudes and practices in child feeding: use of food restriction, pressuring children to eat more, and monitoring eating behavior. All scales assess the frequency of every feeding style on a 5-point Likert-type scale, with higher scores indicating a more frequent use of that specific style. The CFQ has adequate content validity and internal consistency and ranged from .70 to.90 (Boles et al., 2010; Corsini, Danthiir, Kettler, & Wilson, 2008). In this study, internal consistency ranged from .76 to .82.
Maternal self-efficacy
Mothers rated their level of confidence in influencing their child’s eating and sedentary behaviors using 12 items. Four subscales were included in this survey: (a) self-efficacy in promoting healthy eating (five items), which measures maternal confidence in the mother’s ability to promote healthy eating behavior in a child; (b) self-efficacy in limiting noncore foods (four items), which measures maternal confidence in refusing a child’s requests for unhealthy foods; (c) self-efficacy in promoting physical activity to displace viewing of TV, DVD, or videos (two items), which measures mothers’ perceived ability to promote physical activity when their child wishes to be sedentary; and (d) self-efficacy in limiting viewing (one item), which measures maternal ability to limit a child’s TV viewing time (Campbell et al., 2010). All items relating to maternal self-efficacy were scored on a 5-point Likert-type scale ranging from 1 (not at all confident) to 5 (extremely confident). Adequate validity and reliability have been reported in the literature (Campbell et al., 2010). In the present study, internal consistency ranged from .72 to .85.
Statistical Analysis
Quantitative variables were presented as means with standard deviations, frequencies, and percentages. Independent t tests for all variables were used to examine gender differences. Multivariate regression was used to identify factors associated with children’s health behaviors including physical activity, TV and computer viewing time, eating behaviors, and stimulus home environment. Factors included in the model were child’s age and gender, maternal health behaviors (physical activity and eating behaviors), maternal self-efficacy (all subscales), and maternal feeding practices (all subscales). SPSS 23.0 software was used to conduct the analysis. A p value less than .05 was considered significant. With an anticipated effect size of .15, 15 predictors, power of .80 and probability level of .05, a total sample of 139 is required.
Results
Participants
A total of 222 mother–child dyads (i.e., 222 mothers and their children) participated in this study; their mean ages were 31.04 years (SD ± 4.28) and 3.68 years (SD ± 0.75), respectively. Approximately 52% of the children were boys. More than half (54%) of the mothers had completed college or graduate education and 29% had completed high school education. Approximately 95% of mother are Han and about 53% of mothers worked outside of their home. The mothers’ mean body mass index was 19.87 (SD ± 3.9); the children’s mean body mass index was 15.76 (SD ± 1.77).
What Are the Health Behaviors of Children?
Eating Behaviors
The average scores for child and maternal eating behavior—such as eating styles and eating related to hunger—are listed in Table 2. The health behaviors of mothers of girls did not differ from those of mothers of boys, except in relation to hunger and maternal eating style (p = .008). In comparison with male children, female children self-reported a higher frequency of engagement in unhealthy eating behaviors related to hunger tendency (p = .03). In comparison with mothers of male children, mothers of female children were more likely to report that their style of eating was unhealthy (p = .008).
Descriptive Data.
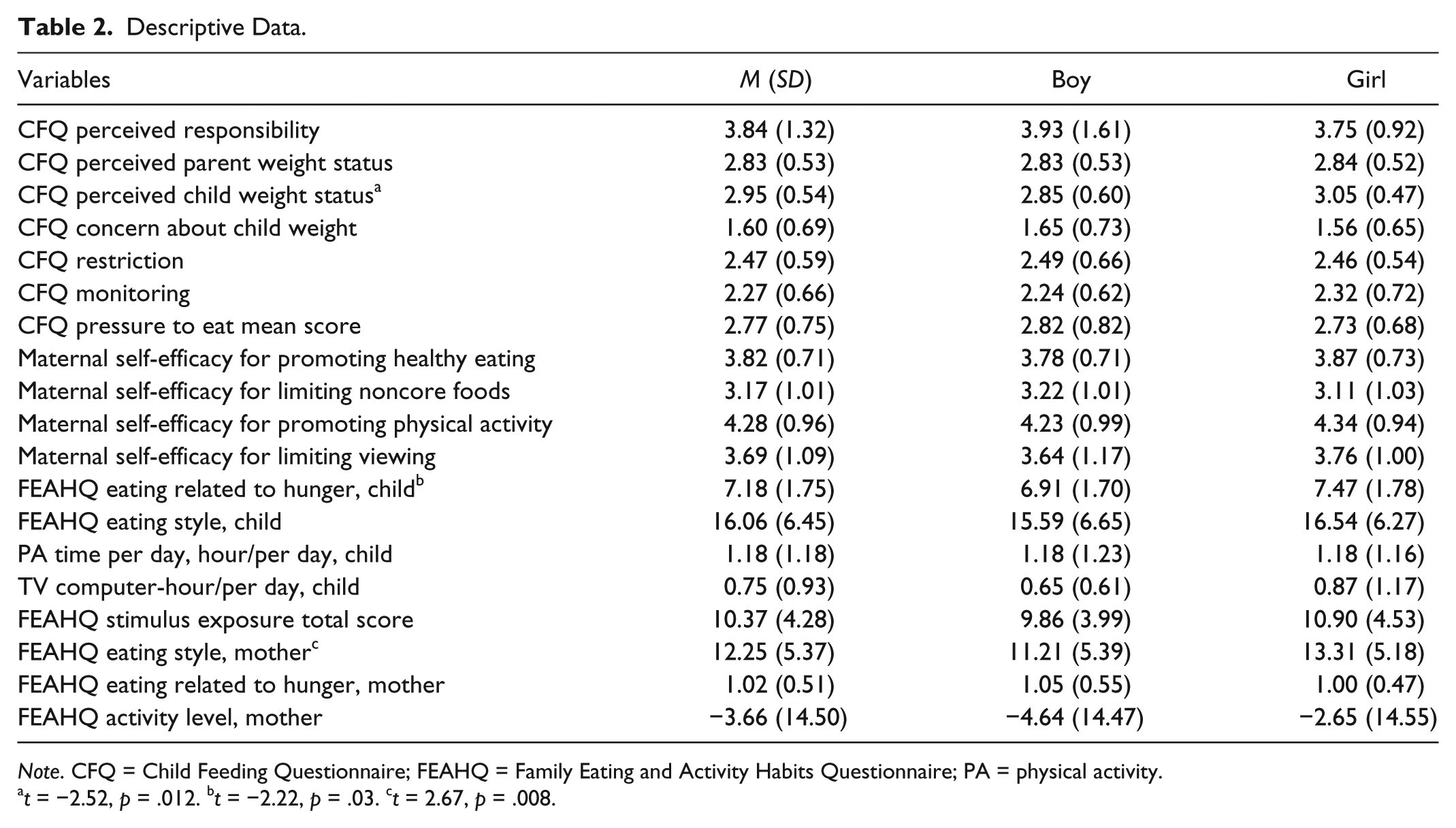
Note. CFQ = Child Feeding Questionnaire; FEAHQ = Family Eating and Activity Habits Questionnaire; PA = physical activity.
t = −2.52, p = .012. bt = −2.22, p = .03. ct = 2.67, p = .008.
Physical Activity and Sedentary Activity
The average time children spent daily in physical activity and in sedentary activity (e.g., watching TV, playing computer or video games) was 1.18 hours (SD ± 1.18) and 0.75 hour (SD ± 0.93), respectively. Approximately 44% of the children engaged in daily physical activity lasting more than 1 hour; 92% of children viewed TV or computer games less than 2 hours per day.
What Are the Maternal Feeding Practices, Maternal Self-Efficacy Regarding Encouragement of Healthy Eating and Physical Activity?
Most of the mothers in our study were relatively unconcerned about their child’s weight. Mothers were neutral with regard to parental control attitudes and practices in their child’s meals and feeding behaviors—such as use of restriction, pressuring children to eat more, and monitoring eating behavior and food intake (Table 2). Mothers reported having a moderate level of confidence in their ability to promote healthy eating and a high level of confidence in their ability to promote physical activity to displace screen viewing (TV, DVD, video; M = 4.28, SD ± 0.96). The maternal feeding practices and self-efficacy of mothers of girls did not differ from those of mothers of boys, except in relation to perceived weight status: In comparison with mothers of boys, mothers of girls were more likely to perceive that their female children were heavy (p = .012).
What Are Maternal Factors Associated With a Child’s Health Behavior?
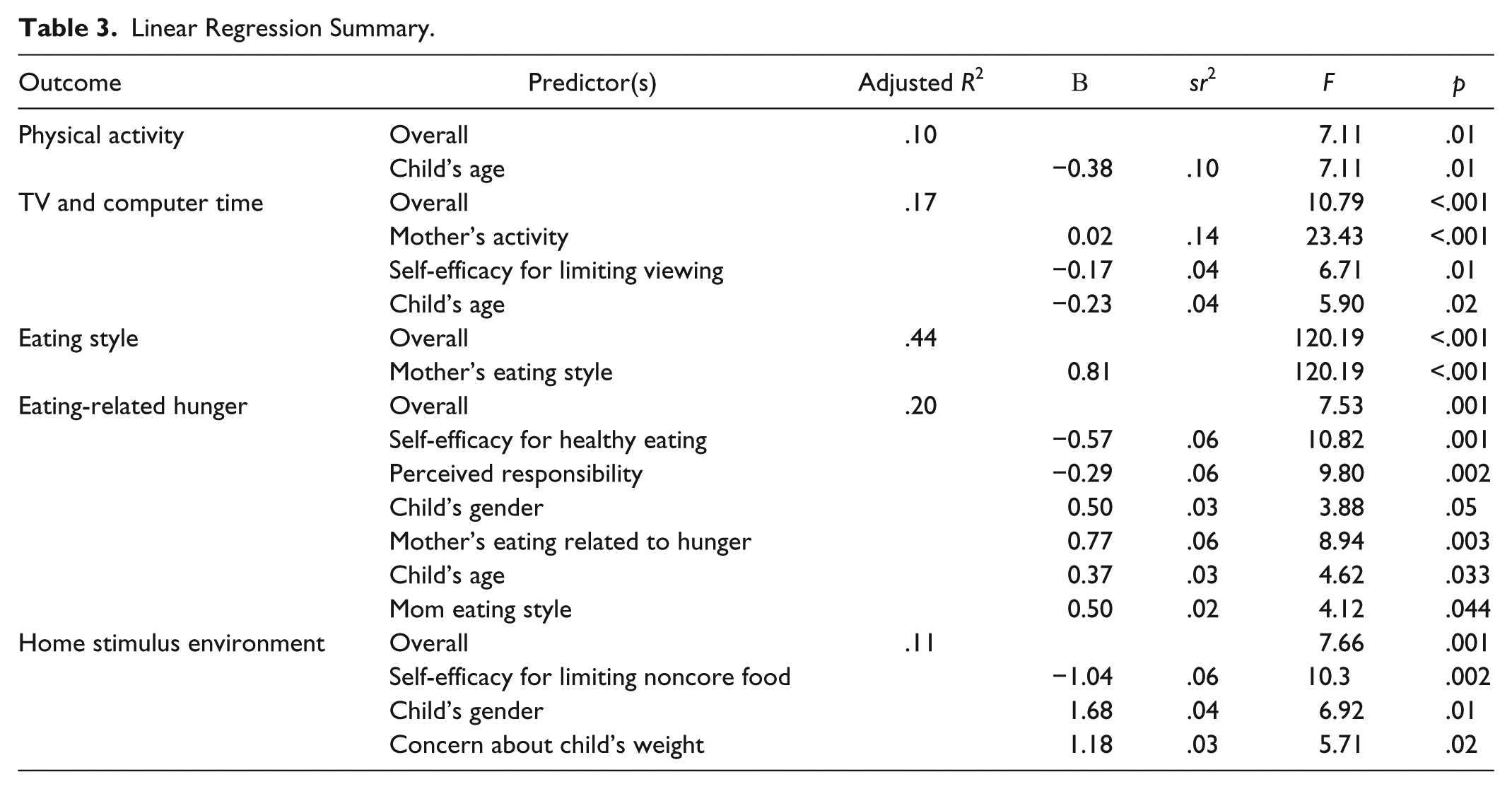
Multivariate linear regression was conducted with regard to five factors pertaining to the children: eating style, eating in relation to hunger behavior, TV and screen viewing time, physical activity factors, and home environment for healthy behavior (see Table 3). In the model, five types of factors were significant. First, a child’s eating style was associated with her or his mother’s eating style (adjusted R2 = .44, F = 120.19, p < .001). Second, low maternal self-efficacy regarding healthy eating, low perceived maternal feeding responsibility, a child’s female gender, an unhealthy maternal eating style in relation to hunger and eating, and an older child’s age were associated with children’s unhealthy eating behavior (adjusted R2 = .20, F = 7.53, p = .001). Third, higher levels of children’s physical activity were associated with younger age (sr2 = .10, p = .01). Fourth, higher maternal physical activity level, maternal self-efficacy for limiting screen viewing, and, for children, younger age were related to less time that children spent viewing TV and computers (adjusted R2 = .17, F = 10.79, p < .001). Fifth, factors related to an unhealthy home environment included lower maternal self-efficacy for limiting noncore food, female child gender, and a mother’s concern about her child’s weight (adjusted R2 = .11, F = 7.66, p = .001).
Linear Regression Summary.
Discussion
This study is novel in that it focused on the influence of maternal behavior on children’s health behavior using mother–child dyads in a non-Western cultural group. This study found that maternal health-related behavior and attitudes regarding feeding practices and self-efficacy were associated with children’s health-related behaviors, including eating behaviors and activity, both physical and sedentary. The influence of maternal behaviors and attitudes were domain specific.
Mothers’ Influence on Children’s Eating Behaviors
We found that mothers’ eating behaviors were associated with their children’s eating behaviors. Also, with mothers who self-reported their own unhealthy eating habits, eating styles, and eating not motivated by hunger, their children reported similar eating behaviors. Previous studies have also suggested that maternal eating directly affects a child’s eating behaviors—because children tend to imitate their mother’s behavior (Kiefner-Burmeister et al., 2014; Schoeppe & Trost, 2015). Moreover, mothers who indicated that they felt low self-efficacy regarding healthy eating and who did not assume responsibility for their child’s feeding contributed to their child’s elevated risk of being motivated to eat by factors other than hunger and satiety cues. Mothers who do not feel competent in providing a healthy eating environment and who are not responsible for their child’s feeding may not actively engage in developing healthy eating habits for their children; these maternal perceptions increase both the mothers’ and children’s risk for unhealthy eating. Given that mothers also greatly influence young children’s socialization regarding dietary and physical activity norms, designers of interventions for improving children’s eating behaviors must consider the children’s mother’s own eating behaviors. Such interventions must effectively encourage mothers to take responsibility for and improve competency in structuring a healthy eating environment for their children.
An increased presence and visibility of snacks, sweets, cakes, and ice cream in the home and lack of boundary setting regarding the child’s autonomy in buying or taking these unhealthy foods increase a child’s risk for unhealthy eating behavior and obesity. Results of our study in China found that, for Chinese children and their mothers, a lower level of maternal self-efficacy in limiting noncore food at home and concern about the child’s weight increased the home environment’s obesogenicity. Research has suggested that greater availability of noncore foods at home was associated with children’s greater consumption of unhealthy foods (Ostbye et al., 2013; Veldhuis, van Grieken, Renders, Hirasing, & Raat, 2014; Wang et al., 2013). Given that in many households, mothers are responsible for food shopping and meal preparation, educating mothers about limiting unhealthy foods at home is important. Perhaps households in which noncore foods are more available are also more likely to have children who consume these foods and who are thereby at elevated risk for overweight and obesity. In addition, the mothers of these children might be more likely to be concerned about their children’s weight.
We also found that mothers of female children self-reported a higher frequency of engagement in unhealthy eating behaviors related to hunger tendency as well as perceived female’s children weight more than male children. It is not clear whether these perceptions are related to body image of female children. Future studies need to examine whether these perceptions differ by gender and reasons for different perceptions.
Mothers’ Influence on Children’s Physical Activity
In addition to influencing their children’s eating behaviors, mothers also influence their children’s activity—both physical and sedentary. We found that a high level of maternal sedentary activity (conversely, a low level of physical activity) and a low level of maternal self-efficacy for limiting TV viewing were related to a greater amount of child’s sedentary time (e.g., TV and computer time).
Previous research has emphasized that children’s physical activity and sedentary behavior can affect their ability to maintain a healthy weight and health (Cárdenas-Cárdenas et al., 2015; Senso et al., 2015). Our study found that the majority of preschool-age children (92%) in China spent less than 2 hours per day in sedentary activity, but fewer than half of the children (44%) reported engaging in activity for more than 60 minutes per day. Results also revealed that for children, older age is related to more time spent in both physical activity and sedentary activity. Also, the more inactive the mother was and the less competent she felt in limiting a child’s TV and computer viewing at home, the more time the child spent watching TV and using a computer. Our study’s results are consistent with those of previous studies that have suggested that mothers play a critical role in influencing children’s sedentary activity behavior (Hnatiuk, Salmon, Campbell, Ridgers, & Hesketh, 2015; Jago, Sebire, Edwards, & Thompson, 2013; Jago, Wood, Zahra, Thompson, & Sebire, 2015).
A mother can be a role model for her child—for example, the mother’s ability to set limits on TV viewing and computer use are critical determinants in her child’s levels of physical activity and sedentary activity. We found that the more competent a mother felt in setting time limits for her child’s TV viewing and computer use, the less likely the child was to watch TV and play computer games. However, a meta-analysis found that parental modeling may have limited effect or even no effect in children’s physical activity level (Pugliese & Tinsley, 2007). Alternatively, parents who encourage and support their children may improve their children’s activity levels (Pugliese & Tinsley, 2007). This meta-analysis also noted that extant data were insufficient for determining whether mothers and fathers differed on measures of influence. The authors of the meta-analysis speculated that mothers and fathers do differ in measures of influence and that specific differences have simply not yet been identified. Our study provides quantitative evidence on the impact of mothers’ self-efficacy and maternal activity level on children’s activity level. In light of the evidence that children’s lower levels of physical activity are associated with higher obesity risk, interventions tailored to increase children’s engagement in physical activity (and/or to reduce their engagement in sedentary activity) may include increasing their mothers’ engagement in physical activity—and strengthening maternal self-efficacy with regard to setting limits for TV viewing.
Notably, as children get older, they spend more time in both physical activity and sedentary activity. This change in activity pattern may be related to children’s developmental stage. As children develop better motor skills and expand their social circle, they are more likely to engage in activity—both physical activity and TV viewing, which involve others, including peers (Barbosa, Coledam, Stabelini Neto, Elias, & Oliveira, 2016; Edwards et al., 2015). Although in the present study, the majority of preschool-age Chinese children spent less than 2 hours per day in sedentary activity, fewer than half of them met the recommended physical activity level. A healthy lifestyle, including regular physical activity in childhood, contributes to the prevention of obesity and other chronic diseases (Cárdenas-Cárdenas et al., 2015; Larouche, Saunders, Faulkner, Colley, & Tremblay, 2014); a healthy lifestyle also stimulates cognitive performance and improves psychological health (Carson et al., 2015; Carson et al., 2016). Because health behaviors are established early in life, and early childhood is an important period for physical activity promotion and the establishment of physical activity habits, intervention to promote active lifestyle for the whole family is critical.
Strengths, Limitations, and Future Research
Our study has several limitations. First, because we used a cross-sectional study design with convenience sampling, causation relationships cannot be established. Second, given that our study’s measurement of health behaviors used self-reporting, our findings may have been biased by self-report bias. Third, our recruitment of study participants from four preschools in China constrains the generalizability of our findings and conclusions. Moreover, we did not investigate other important factors such as genetic and father’s and grandparents’ influences in Chinese children’s health and health behaviors. Future research may need to include these important factors. Finally, some weak reliability was found in FEAHQ and CFQ that could have affected the results. However, despite these limitations, several strengths augment the study’s validity: the use of standardized measures, the use of multiple study sites, and our study participants’ socioeconomic diversity. We provided mothers with ample time to complete the surveys, and we provided research staff with ample time to assess the children’s height and weight. Given our study’s findings, future studies may consider larger sample sizes, use additional measures of health behaviors that are more objective, and use a longitudinal design to assess factors related to change of health-related behaviors in children and their mothers. Future research should also investigate the relationship between maternal concerns regarding a child’s weight and a child’s eating and weight status.
Implications for Practice
Because children’s health is critical to the health of the nation and to global development, understanding the factors related to children’s health-related behaviors is an important first step toward development of tailored, culturally sensitive interventions for promoting a healthy lifestyle and preventing obesity. Efforts to improve children’s health behaviors must involve their mothers—specifically, by promoting the mothers’ engagement in a healthy lifestyle and by strengthening their self-efficacy with regard to provision of a healthy home environment for their children.
Footnotes
Acknowledgements
The authors wish to thank all the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Bureau of Education and Cultural Affair, Fulbright U.S. Research Program and University of California, School of Nursing Global Health Nursing Research Grant.