
Abstract
Asian Americans (including Vietnamese Americans [VAs]) originate from over 50 different countries; however, the dominant literature tends to aggregate findings across subgroups (Gomez et al., 2013). Cervical cancer (CC) is disparately diagnosed in Vietnamese American women (VAW) and die at twice the rate (16.8/100,000 and 4.4/100,000, respectively) than White non-Hispanic women (8.1/100,000 and 2.4/100,000, respectively; Miller, Chu, Hankey, & Ries, 2008). The best way to detect CC early is to have regular screening with a Papanicolaou (Pap) test, which may be combined with a test for human papilloma virus. Early detection greatly improves the chances of successful treatment of CC; the survival rate is close to 100% for precancerous lesions, and 91% for women diagnosed with localized CC 5 years after diagnosis (American Cancer Society, 2015). Despite the importance of early detection, CC screening rates are persistently low among VAW. In prior studies, 69% to 81% of VAW reported being up-to-date with CC screening (Nguyen-Truong et al., 2012; Thompson et al., 2014). These rates are lower than the Healthy People 2020 goal to screen 93% of all women aged 21 to 65 years (HealthyPeople.gov, 2017a).
VAW face economic, language, health care access, and cultural barriers to preventive health care. Chawla, Breen, Liu, Lee, and Kagawa-Singer (2015) conducted a large cross-sectional survey study with Asian American women (n = 7,865). VAW who did not speak English or had limited English proficiency and/or had income levels lower than 200% below the federal poverty level reported infrequent medical visits to a health care provider (HCP) within the past 12 months. In addition, VAW were less likely to obtain regular CC screening than the women from many other Asian subgroups (Chawla et al., 2015). VAW who have a regular HCP and a HCP who had ever recommended a CC screening were more likely to be screened regularly than VAW women without a regular HCP, nor did they received a recommendation for a CC screening (Nguyen-Truong et al., 2012). Similarly, in Do’s (2015) cross-sectional survey study of 265 VAW, women reported the absence of a recommendation from a HCP as a major reason for why they did not seek CC screening. VA immigrants are less likely to seek information from HCPs about cancer than do White and African American populations (Nguyen et al., 2010). VAW may not view medical care as primary prevention. Rather, many rely on personal health regimens, including vaginal washing as a means of prevention (Gregg, Nguyen-Truong, Wang, & Kobus, 2011). HCPs should take a more active role in promoting VAW’s CC screening. Suboptimal CC screening rates and reports from VAW suggests that many HCPs are missing opportunities to counsel VAW about CC and the importance of being screened.
Little is known about what strategies are needed to strengthen health care practices within this population. One cross-sectional survey of Asian Americans’ perceptions of health care (n = 63) found that cultural sensitivity of clinicians significantly predicted trust in HCPs and of treatment adherence (Kang, Tucker, Wippold, Marsiske, & Wegener, 2016). Although the results are not conclusive about the influence of client–provider gender concordance on CC screening completion in VAW, the information available suggests that this is important. Do (2015) found the absence of available female HCPs was not identified by VAW as a major reason for not undergoing CC screening. In contrast, Thompson et al. (2014) and Lofters, Ng, and Lobb (2015) found that having a female HCP was positively associated with CC screening completion among VAW, whereas having a male physician had the opposite effect. Thompson et al. (2014) also examined the potential influence of HCPs’ licensure (physician vs. nurse practitioner, doctor of osteopathic, or physician assistant) and practice specialty (family vs. internal medicine) on VAW’s CC screening rates, and found not to have an effect. More information about how HCPs provide CC education and screening for VAW is needed to improve the capacity to provide culturally and linguistically appropriate care. Increasing the proportion of women who are counseled by their HCPs about Pap tests to screen for CC remains a national guideline (HealthyPeople.gov, 2017b).
Little information is available about how HCPs enact CC education with VAW whose culturally specific beliefs and practices must be carefully addressed in practice. The purpose of this study was to explore HCPs’ perceived barriers and facilitators to CC screening in VAW.
Method
Design
A qualitative descriptive method was used to guide the data collection and analysis procedurally, which was informed by the community-based participatory research (CBPR) design. Qualitative description entails the presentation of findings close to the data as provided by participants (Sandelowski, 2000, 2010). The VAW Health Project in the Portland, Oregon metropolitan area is a long-standing CBPR partnership between the Immigrant & Refugee Community Organization Asian Family Center and the Principal Investigator (PI; first author) who has successfully engaged in multiple studies addressing CC in VAW in the past 9 years. This pilot project grew organically from previous efforts in the VA community. Community member partners were involved in the study design and implementation, and details of involvement are described in the method.
Sample
The study sample consisted of HCPs licensed to diagnose and prescribe, perform CC screenings, and whose service populations included VAW. The participants were from the Portland, Oregon metropolitan area, which has a large population of VAW, 14,976 (U.S. Census Bureau, 2009-2011). To purposively sample, referrals were requested from the CBPR partnership’s community advisory board and recruited participants from federally qualified health centers and clinics (private and nonprivate). Federally qualified centers serve “an underserved area or population, offer a sliding fee scale, provide comprehensive services, have an ongoing quality assurance program, and have a governing board of directors” (U.S. Department of Health and Human Services, n.d.). Snowball sampling was also used, which relied on direct referrals from the participants. The final sample size of 10 participants was influenced by the focused scope of the topic, the high quality of data obtained from each participant, and the study of Hennink, Kaiser, and Marconi (2017). Specifically, Hennink et al. (2017) found that saturation was typically reached by the ninth interview, with sufficient data to allow for identification of a broad range of thematic issues and of codebook stability.
Data Collection
Each participant was interviewed individually one time between December 2012 and November 2013. A semistructured, open-ended interview guide was used to conduct in-depth interviews (see Table 1). The PI was bicultural and bilingual in English and Vietnamese and co-conducted the interviews with two community investigators. Additional probes and follow-up questions for clarification and elaboration on responses were used. Each interview was digitally recorded and lasted about 60 minutes. The participants received a $50 grocery gift card for remuneration. Each interview was transcribed verbatim by a community investigator. The PI listened to each recorded interview and verified the accuracy of the transcriptions. The PI also referred back to the participants to ask clarifying questions.
Semistructured, Open-Ended Interview Guide.
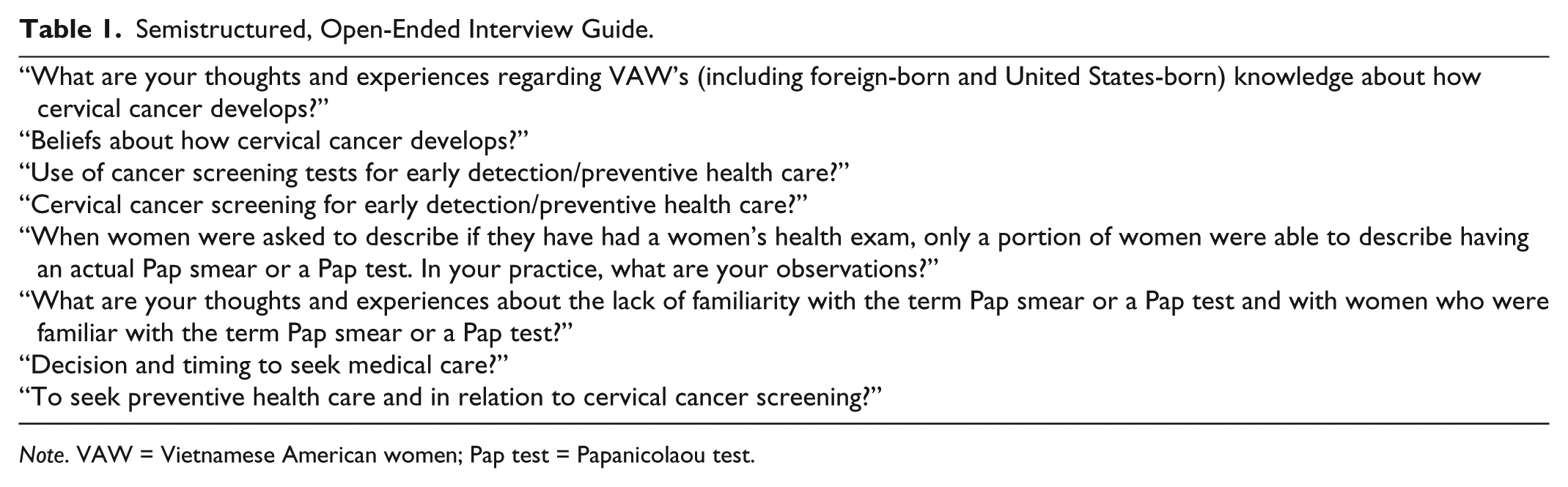
Note. VAW = Vietnamese American women; Pap test = Papanicolaou test.
Data Analysis
The data collection occurred concurrently with the analysis. Pseudonyms were assigned to participants, and the data were managed using ATLAS.ti (version 7.0.76) qualitative software. Thematic analysis was used as described by Luckman (2016; Clarke & Braun, 2017) to identify broad (main) themes. The team members familiarized themselves with the data by reading and rereading the transcripts and engaging in peer debriefing (Lincoln & Guba, 1985). In an iterative process of thematic coding, the PI and the coinvestigator (third author) independently coded the first and second transcripts line-by-line using open coding. The PI and coinvestigator met to discuss discrepancies (e.g., variations in code names that represented the same meaning) and negotiated an agreed on codes to improve consistency.
The second author who served as an expert qualitative consultant, read the first and second coded transcripts and added additional codes. The PI, coinvestigator, and expert qualitative consultant met to debrief about the codes to discuss discrepancies, and agreed on the best codes to further improve consistency. Remaining transcripts were coded independently by the PI and coinvestigator and an expert qualitative consultant read selected coded transcripts and added additional codes. Next, the coding was reviewed and debriefed by the entire research team, until agreement on the coding was achieved. The codes for each interview were then compared across the transcripts. The team identified main themes and tested them as they moved between the codes and the entire data set. The team also discussed the analysis of the data with VAW community advisors with backgrounds in community health, public and health administration, and in science. They served as external auditors and enhanced rigor. A team approach helped provide different understandings of the findings while addressing reflexivity. Reflexivity denotes an awareness of one’s personal biases, and an examination of their potential influence on the research process (Rae & Green, 2016).
Research Ethics
The study protocol and materials were approved by a local institutional review board. An information sheet was used that did not require participants to sign their names to indicate consent for study enrollment. As a part of the informed consent process the PI provided the information sheet and explained the purpose of the study as well as the nature of participation. The PI also explained the lack of any known risks, discomforts, or personal benefits, and that participation was voluntary and confidential.
Results
Eight participants chose to be interviewed in-person (i.e., in an office or a public place with a private area) and two were interviewed by telephone. All initially chose to be interviewed in English, and two referred to Vietnamese terms and interpreted their meanings.
Participant Demographics and Background Characteristics
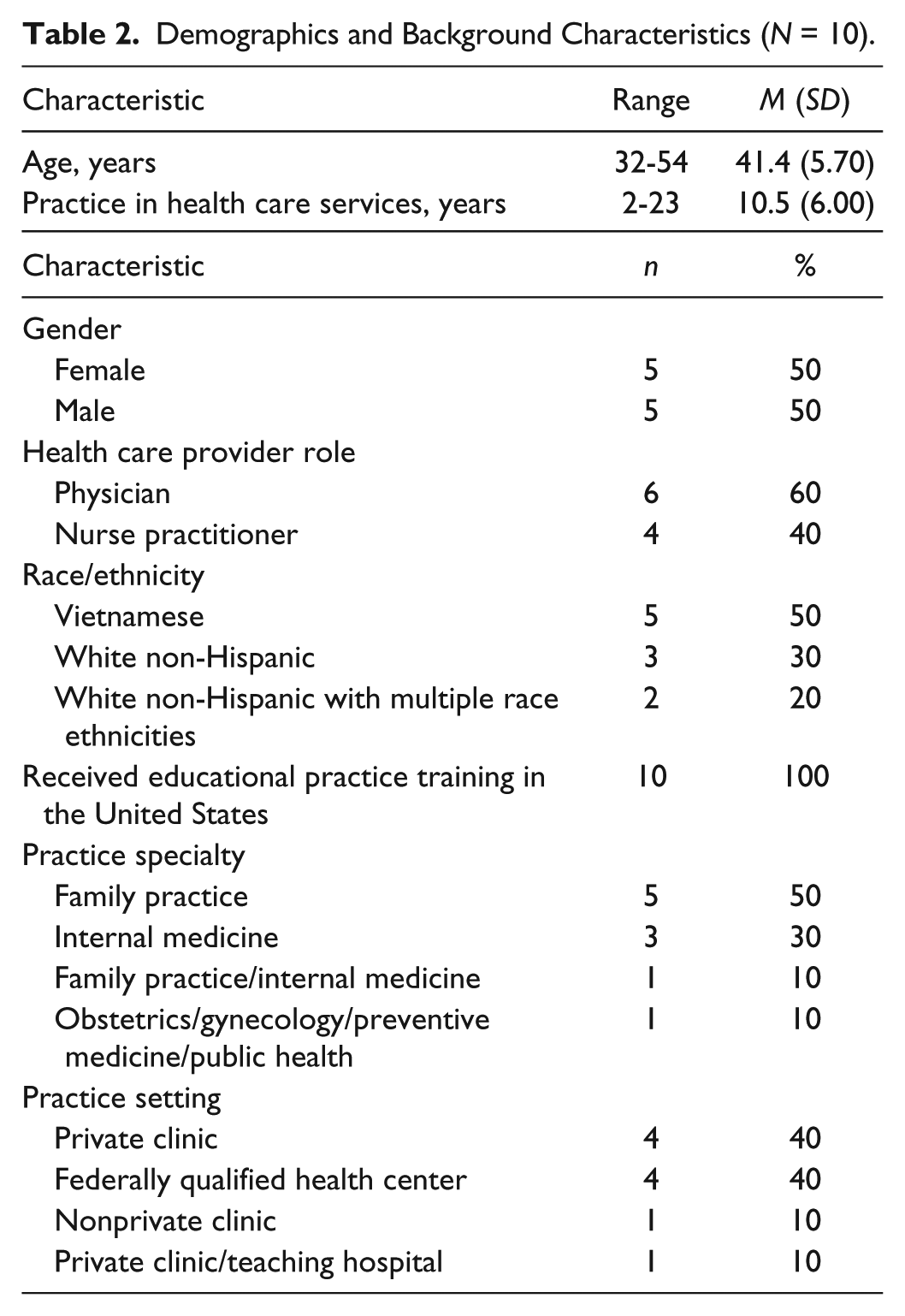
Of the 10 participants, 5 were bilingual in English and Vietnamese (see Table 2).
Demographics and Background Characteristics (N = 10).
Main Themes
The main themes were associated with barriers and facilitators to CC screening.
Barriers to CC Screening
Theme 1: VAW’s Decision Making About CC Screening
The participants reported that the decision making about CC screening was made by VAW, and in particular immigrant women, without a good understanding of the CC symptoms and risk factors. The participants shared their efforts in attempting to communicate with their VAW clients. The participants reported that the clients’ lack of understanding of preventive health care and inaccurate beliefs about CC contributed to underutilization of screening. Many participants reported that the VAW viewed symptoms as a sign of disease requiring treatment, and no symptoms as an indication of good health. As described by Dr. Doan, “They [VAW] associate disease with symptoms and when you have symptoms you take medication or you get your body cut off [surgery] . . . ” As commented by Dr. Vong,
. . . [VAW] feel . . . whatever is broken is fixed right there . . . rather than do a lot of screenings. So, that’s why it’s hard to get them into the routine of doing screenings than [other] populations . . .
Similarly, Dr. Diep said, “ . . . the idea prevention is not very common. It’s more treatment. You have a medical problem, you treat it. If it doesn’t hurt, don’t touch it.” The participants described inaccurate beliefs held by some clients who viewed their relationships as monogamous, with perceived little or no risk for developing CC and no need for screening. Family Nurse Practitioner (FNP) Ahmed commented,
[some VAW] say . . . I don’t have cancer . . . I’ll say . . . CC is caused by a virus that is passed through sexual intercourse . . . when men have sex with women or men have sex with men . . . they . . . say . . . I’ve only had this [sex] with my partner or with my husband so I’m not worried about it . . . I don’t think they understand very well.
In addition, the participants reported that some clients believed a negative Pap test result means that there is no need for future testing. For example, Dr. Doan shared,
Unlike American [non-Vietnamese] patient, when you tell them [VAW] a Pap smear they know that’s a preventive thing. . . . Most people know [but] . . . for Vietnamese [immigrant] women, the term Pap smear, they never heard of. When you describe the test, they go oh, yeah, I had it done when I had a baby. . . . The American doctor did that. It was normal, never had it done again . . .
Theme 2: Sexual Health Divide
The following are the subthemes for this barrier: VAW’s fear of judgment (sexual health history “equals” prying/invading of privacy and a violation of confidentiality) and cultural beliefs about sexual behavior. Some participants described tension between the need to obtain a thorough sexual history and maintain client privacy while engaging in respectful communication. The male gender was perceived by some participants as a barrier to comfortable and candid conversations about VAW’s sexual histories. Nearly all the male participants mentioned the need to work with a female medical assistant, or to have hired a female registered nurse or nurse practitioner to help address the cultural barrier. For example, prior to their seeing or doing a CC screening with clients the medical assistant or registered nurse would obtain the VAW’s sexual health history.
Both male and female participants described cultural barriers to obtaining a sexual health history as a divide that occurred when clients feared being viewed negatively by HCPs. This was particularly so when VAW’s were asked to provide information about their number of sexual partners. The clients often emphasized and reassured participants that they only had one lifetime partner. The participants described being cautious in their communication when taking a sexual history, to avoid implying that women had had multiple sexual partners. As Dr. Ngo described,
. . . to bring up sexual history or sexual discussions in practice was really an issue, very hard for me as an Asian American [male] provider . . . my younger [VAW] patients were much easier for me to discuss things with. It’s the older ones that was a lot harder . . . I can’t really get a good . . . [sexual] history because they’re not going to disclose more. . . .Community and society is so small. . . . If [VAW] tell me [have] two [partners], they’re afraid I’m going to . . . rat [tell] to everybody. . . . It’s already an uncomfortable situation when I gotta put them . . . to get the [Pap] test. So, I utilize a lot of testing [discretion] . . . to convince them of [Pap] testing . . . not too much . . . prying [in]to their sexual history.
FNP Makawee said,
My [VAW] patients certainly wanted to reassure me that her husband and her were a couple . . . it definitely felt like I [female HCP] was prying a little bit, and I was backpedaling [not making assumptions] to try to make . . . the situation comfortable . . . I don’t schedule . . . more than 40 minutes for [a] gynecological exam . . . but it’s not enough time to do a whole bunch of education . . .
The human papilloma virus is responsible for most CCs (Centers for Disease Control and Prevention, 2017). A few participants reported being aware that some of their clients, in particular immigrant VAW believe that an infection of the genitalia represents “very bad”/immoral behavior, is associated with being punished, and is a taboo topic. Hence, the participants perceived that their clients do not want to find out if there is a problem. Dr. Doan said,
Taboo like an STD [sexually transmitted disease] . . . a relationship within a marriage or not . . . they [VAW] think it’s a bad thing. Immoral! . . . Another fear. . . . You got to have done very bad thing in your life . . . don’t want to talk about it. . . . They don’t want to find out . . . a problem involved the genital . . . I am punished.
Theme 3: Language Discordance, Relying on Interpreters
Half of the participants described being completely dependent on Vietnamese interpreters, and some expressed concerns about the quality of the interpretation and its effect on the quality of care. As described by Dr. Johnson,
. . . the difficult part always is, how good is the interpreter. . . . Some of them I feel are excellent, some of them I feel like they’re not . . .I’ll tell them something and they’ll go like, oh yeah . . . and I’m like, no please explain this to the patient. [interpreter said] Oh she knows that . . . There’s some interpreters that I’m more comfortable with than others . . . that’s frustrating . . . increasingly difficult to get an onsite [Vietnamese] interpreter . . . I’ve been lucky . . . a few times . . . it’s just not consistent.
Theme 4: Breaking Suspicion
Most participants described the need for a culturally and linguistically appropriate educational community outreach to VAW in Vietnamese language by trusted people in the Vietnamese community to help promote CC screening. They emphasized how VA community involvement would help promote CC screening and help ameliorate trust issues that impede the effectiveness of clinical practice. FNP Ahmed shared,
I have a lot of [VAW] patients that have come in feeling very suspicious about the medical system, and I have to break past that barrier first before I can even talk to them about their health care because they don’t trust that I know what I am doing . . . An open forum . . . led by [a] health care provider or community worker or somebody that was trusted in the [Vietnamese] community and they talk about the need for CC screening . . . why it’s important . . . where women can talk to each other very openly . . . to let women know this is a normalize . . . thing to do . . . people that speak their language that can answer their questions really honestly . . .
Facilitators to CC Screening
Theme 1: VAW’s Exposure to Health Sources About CC Screening
Prolonged exposure to information about CC and CC screening facilitated screening. Some participants described a difference between the younger U.S.-born VAW and the older, immigrant VAW, and the importance of viewing the needs of these groups differently. Dr. Vong said,
Many [immigrant VAW] are older . . . [than] the young [U.S.-born VAW] population . . . 30 . . . 50 . . . born, raised in America . . . [immigrant VAW from] Vietnam, they don’t have . . . much exposure to the screenings before they came here [America] . . . shall have more hesitance . . . to do screening . . . In term of CC . . . the people that born and raised here . . . they get used to that idea and get taught like in school . . . heard more…more open to do . . . [CC] screenings.
Some participants described that their clients use media as a source of health information including Vietnamese language media. This points to a need to be aware of other sources of health information influencing clients, and to verify the accuracy of such information. Dr. Bui commented, “ . . . [some VAW] read it [CC screening] in the newspaper, they hear that on the radio, on television Vietnamese language media . . . and they come in, they see the doctors [and] that get reinforced again.”
Theme 2: Sustainable Trust in the Client and HCP Relationship
Building a sustainable, trusting relationship over time while being sensitive to VAW’s cultural beliefs as information is delivered facilitated screening. Most participants described the importance of being sensitive when talking with clients about CC screening. The assumption that VAW may be fearful seemed to help guide participants’ sensitive communication. Dr. Diep said,
[VAW] . . . fear of die in pain . . . in suffer . . . we do say not in a threatened way, but it’s a reality . . . certain cancer would say . . . it metastasized, you have to 2 years to live, but you have to go through chemo, you have surgery, radiation . . . take a while for them to digest . . . accept information and they will be fine.
Most participants talked about the importance of getting to know their clients to motivate VAW to return for ongoing health care, including CC screening. FNP Ahmed shared,
In the realm of trust . . . I mention . . . there’s an exam that we can do to check for CC, . . . I definitely don’t make . . . that a requirement at my first visit . . . I want to get to know them . . . I want them to feel that they can build a relationship with me . . . I’m asking . . . about their family . . . children . . . support, and how long they have been here, and I say now you can come back in 2 weeks or 3 weeks and we can see you again . . . I try to let them know that I’m not just gonna poke and prod them the first time they come in . . . that’s helpful . . . very often they’ll come back . . . calm . . . they know me already . . .
A few participants talked about working with VAW as partners. Dr. Diep described,
[As] their partner inform them something in their best interest, but not [as] their parent to tell them what to do . . . get a better relationship that way . . . have to hear from their side why something doesn’t happen . . . work with them because guideline is there to help. . . . We work together to make you healthier, you don’t have to pay to come to see me if you don’t want to make a difference . . . it works very well . . . they know that you care, you don’t take it personally . . . don’t make a judgment . . . they can comeback . . .
Theme 3: Motivated Health Care Practices
Sharing the same Vietnamese cultural background and language, scheduling CC screening during clinic visits, and addressing financial barriers facilitated CC screening. All participants practiced in health care settings that went to great lengths to improve clients’ access to CC screenings. Those participants who identified as bicultural and bilingual in Vietnamese and English described their background as the main reason why VAW sought them out as HCPs. As described by Dr. Bui,
Why is it that so many [VAW] patients come to me? I think one of it is the [Vietnamese] culture, and language . . . I come from the same culture that they come from, and I speak their language . . . Other than . . . we [also] are very convenient for them location-wise . . . Because the language barrier, we help schedule it for them . . .
FNP Brooks commented,
[referring to follow-up on positive Pap test screening outside of the federally qualified health center] The [Vietnamese] in-house interpreter can make phone calls for us, then see [VAW] patients but when it come . . . to help and register, they really don’t have the capacity . . . if they’re generous enough, they have the time . . . help call and figure out documents needed and try to explain . . .
The participants talked about financial barriers to Pap testing (e.g., lack of health insurance). Dr. Ngo shared,
They [VAW] lost their insurance and I would say…I can either work with you and give you cheaper rates . . . I work with the labs to give me cash pricing . . . patients would do the exam . . . pay is much cheaper than . . . if I had to bill it through insurance . . . if they can’t do that, I would . . . send them to Planned Parenthood.
Most participants described doing manual reviews of their clients’ electronic health records to identify cancer screening needs, including Pap testing. FNP Smith said,
. . . trying to make time for screening . . . in this environment, it’s hard . . . try to find ways to incorporate it into what you do . . . scrubbing [reviewing electronic health records] and the huddling [discussion between HCP and medical assistant] . . . we try to fit things in. . . . Either having my medical assistant talk to the patient about it. If they’re insured, go ahead and scheduling them their well woman exam . . .
See Table 3 for a summary of the main themes.
Summary of Main Themes.
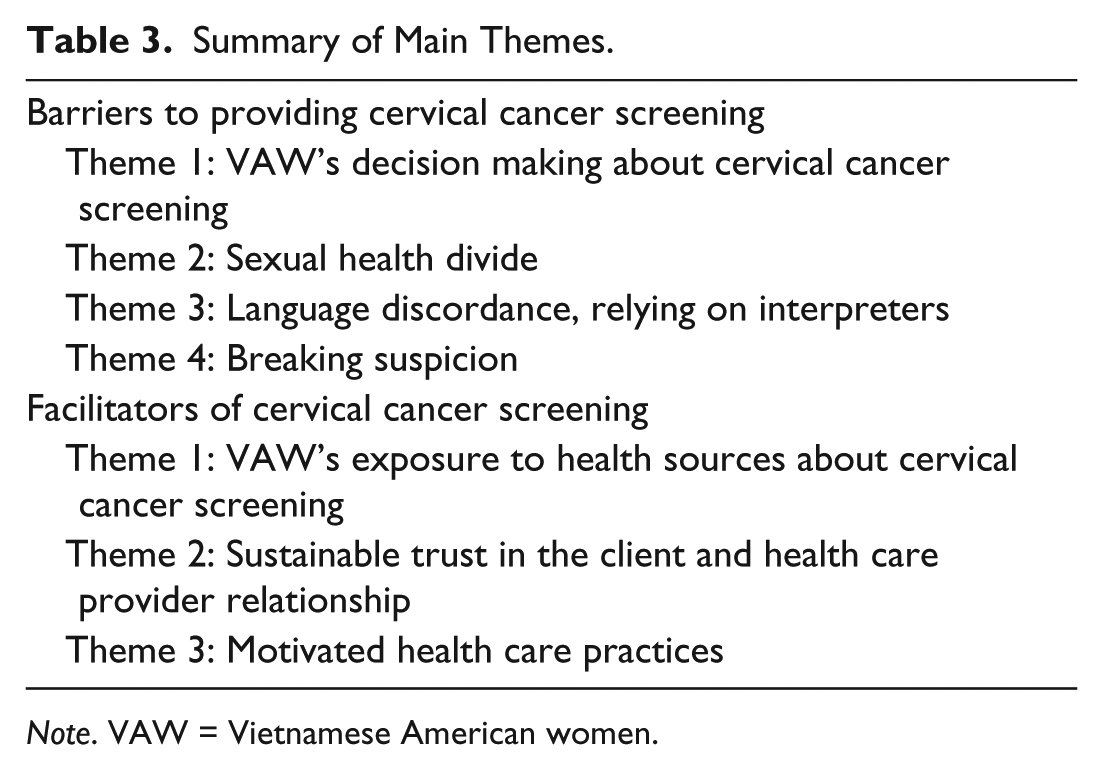
Note. VAW = Vietnamese American women.
Discussion
Suboptimal CC screening rates and VAW’s reports in previous research suggests many HCPs are missing opportunities to counsel VAW about CC and the importance of being screened (Chawla et al., 2015; Do, 2015; Nguyen-Truong et al., 2012; Thompson et al., 2014). The current study findings point to the need for HCPs to provide tailored, culturally, and linguistically appropriate information when counseling VAW about CC screening, rather than using a generic approach with this population. Furthermore, the study findings on barriers and facilitators to CC screening to VAW provide concrete information that HCPs can use to improve care access and quality with this population. When providing VAW with CC education, it is critical to address the culturally specific beliefs and practices identified in this study. Finally, the findings provide a basis for the design of future CC research with VAW.
The literature is clear in that HCP recommendations for CC screening is an important factor (Do, 2015; Lofters et al., 2015; Nguyen-Truong et al., 2012; Thompson et al., 2014). The participants perceived that VAW clients appeared to lack understanding of the CC symptoms and risk factors, suggesting this influenced the decision making to not undergo a CC screening. The findings suggest that the decision making may not have been a shared exchange between some HCPs with their VAW clients about the need for CC screening. Participants perceived that some of their clients made their own decision that lacked a good understanding. The findings contrast with the literature, where Mead et al. (2013) found that the clients showed respect for the HCPs’ status as an authority figure by deferring the decision making to them. Mead et al. (2013) asserted that shared decision making leads to mutual health care decision making. This underscores the critical need for HCPs when counseling VAW clients about CC screening, to be proactive in facilitating a shared exchange that considers both preferences.
The study findings also suggest that the participants encountered cultural barriers in providing CC education and screening for VAW, which includes obtaining a sexual health history as a divide. A perceived stigma and fear by participants appeared to be present, in particular with VA male HCPs about their clients’ worries about loss of confidentiality. Furthermore, the findings suggest an underlying concern about facing resistance from clients when male VA HCPs talked to their clients about performing CC screening. The findings add significant cultural context to Thompson et al.’s (2014) and Lofters et al.’s (2015) findings on gender discordance and suggest that this may be a culturally based barrier. Based on these findings, both female and male participants considered the sensitive nature of CC screening when communicating with their VAW clients. However, education required a significant amount of time, which was not always available in the context of a busy clinic schedule.
Trust was found to be both a barrier and facilitator in participants who provided CC screening in VAW. Some participants perceived that their VAW clients were suspicious of the medical system and the time needed to overcome that suspicion. The current authors found the importance of culturally sensitive communication and trust building in the client and HCP relationship should be built in stages, starting from the first visit and to be sustained over time. The current study findings are consistent with those of Kang et al.’s (2016) survey study of perceptions in health care, who found that when Asian American clients’ level of perceived culturally sensitivity of a provider increased, their level of trust in providers and treatment adherence increased as well (Kang et al., 2016).
The participants stretched their capacity to promote team-based care in order to boost CC screening in VAW. The participants or staff members may have been driven by individual commitment or passion to help VAW to overcome barriers to CC screening. The current study findings suggest that HCPs need to partner with trusted Vietnamese bilingual community members for building trust with the Vietnamese community, which in turn will increase the willingness of women to see a HCP for CC screening. Advances in population health rely on critical partnerships between health care delivery organizations and community/public health entities (Goldberg, Feng, & Kuzel, 2016).
Half of the participants did not speak Vietnamese and depended on a pool of interpreters or worked with a Vietnamese in-house interpreter to communicate with their clients. The study findings suggest that the quality of interpretation affected their care of VAW clients in a negative or positive way. A qualitative study about client–provider communication in CC-related care with Spanish-speaking women sheds light on this concern. Simon et al. (2013) found that although jargon is omitted when health information is communicated in Spanish, a loss in the translation may occur because interpretations differ due to cultural differences in meanings and the quality of mastery of technical vocabulary in a nonnative language (Simon et al., 2013). The current study findings suggest that HCPs, VAW clients, and interpreters should discuss goals and potential barriers and facilitators in language interpretation as interpreters are members of the interprofessional team. This may help address concerns about quality interpretation with Vietnamese-speaking VAW.
Implications
This CBPR qualitative descriptive pilot study was conducted with HCPs who provide care to VAW in a northwest region of Oregon. Further research is needed to build on this pilot study, such as focus groups consisting of VAW to capture group perceptions of meaning, cervical health and illness, to inform the development of an intervention. In addition to the critical role that HCPs play to improve regular CC screening, the current authors found that it would be helpful for HCPs to develop a culturally and linguistically appropriate and relevant educational intervention that addresses these barriers and facilitators. HCPs perceived a lack of understanding, cultural barriers, language, and trust issues in VAW as reasons why women were not being screened or would delay screening. This affected some HCPs ability to provide culturally congruent health care as they experienced barriers in engaging and counseling VAW about CC screening.
Footnotes
Acknowledgements
The authors thank Tuyen Tran, MPA-HA, at Providence Cancer Center, and Nga-My Vuong, Chi Bui, BA, and Stephanie Lam, BS, from the Vietnamese Women’s Health Project III Community Advisory Board for debriefing on the findings. The authors thank Dr. Lillian M. Nail, PhD, RN, FAAN, Rawlinson Distinguished Professor and Senior Scientist, at Oregon Health & Science University School of Nursing, who was an investigator advisor and provided research mentoring. The authors also thank John Van Son for editing assistance and the anonymous peer reviewers for their assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Connie Kim Yen Nguyen-Truong, PhD, RN, PCCN, received grant funding from the National Institute of Nursing Research (T32 #5T32NR007061), Beta Psi Chapter of Sigma Theta Tau International and Washington State University Vancouver New Faculty Research Start-Up, which supported the research. Chiao-Yun Hsiao, BS, Tuong Vy Le, MS, BS, Joannie Tang, BS, Margret Vu, AD, and Anthony My Truong, BS, RPh, had an independent contract under the National Institute of Nursing Research grant and received an appreciation gift card under the Beta Psi Chapter of Sigma Theta Tau International grant.