
Abstract
Keywords
Introduction
Colorectal cancer (CRC) is the third most commonly diagnosed form of cancer and the third leading cause of death in the United States (Ryerson et al., 2016). While CRC incidence and mortality have declined over the past two decades for the U.S. general population, some minority ethnic groups in the United States have shown patterns opposite to the national trends (Centers for Disease Control and Prevention, 2016). Specifically, Korean Americans (KAs) have experienced increased incidence of CRC and a persistence of CRC-related mortality over the same period (Giddings, Kwong, Parikh-Patel, Bates, & Snipes, 2012; Kohler et al., 2015). Among KAs, CRC is the second most commonly diagnosed cancer and the leading cause of death (Sabado, Jo, Kagawa-Singer, & Juhn, 2015).
According to the U.S. census data (U.S. Census Bureau, 2010), approximately 1.7 million of KAs live in the United States, constituting one of the fastest growing minority groups in the United States and the fifth largest group of Asian Americans. Georgia ranks eighth in the United States with respect to the size of its Korean American population (a total of 52,431 as of 2010), while the Atlanta metropolitan area ranks sixth among all metropolitan areas in numbers of Korean population (U.S. Census Bureau, 2010).
Despite the high incidence and death rates from CRC for KAs, their CRC screening rates (32.7%) remain significantly lower than those of non-Latino Whites (57.7%) and subgroups (46.8%) of Asian Americans, including Chinese (81.3%), Japanese (59.8%), and Vietnamese (47.8%), as well as the national target (i.e., 70.5%) specified by Healthy People 2020 (Jackson, Oman, Patel, & Vega, 2016; Tran et al., 2018; U.S. Department of Health and Human Services, 2010). The American Cancer Society (ACS) and the U.S. Preventive Services Task Force (USPSTF) both recommend early detection screening to reduce CRC incidence and deaths and removal of precancerous polyps (S.-Y. Lee & Lee, 2013). Although the guidelines for CRC screening vary and are complex, the commonly recommended guideline for CRC screening includes having a fecal occult blood test (FOBT) annually, a sigmoidoscopy every 5 years, or a colonoscopy every 10 years for those aged 50 to 75 years (ACS, 2017a; USPSTF, 2016a). Health care providers recommend these screening tests in primary care settings, discussing a patient’s lifestyle, personal or cultural beliefs, preferences for health care and the costs (USPSTF, 2016b). Although the Affordable Care Act allows for covering the costs of the CRC screening tests, these costs vary based on the type and plan of health insurance (private insurers, Medicare) and the procedure types (e.g., biopsy and polyp removal) so patients are also recommended to check with insurers in order to avoid unexpected costs prior to their decision to participate in a CRC screening test (ACS, 2018). However, a systematic review on CRC screening among KAs reported that only 25% to 50% of KAs had had a FOBT, sigmoidoscopy, or colonoscopy, and only 10% to 40% had had at least one of these tests within the past 5 or 10 years (Oh & Jacobsen, 2014).
Literature has shown that the primary factors affecting CRC screening uptake for KAs include higher socioeconomic status, greater acculturation, adequate knowledge of CRC and screening guidelines, more social support, and appropriate coverage of health insurance (H. Y. Lee & Im, 2013; Oh & Jacobsen, 2014; Ryu, Crespi, & Maxwell, 2014). While these findings are critical for the development of interventions for increasing CRC screening among KAs, the findings revealed some limitations because the studies overlooked the fact that behavior change, including screening adoption, is a process that occurs in decisional stages and past research aggregated data related to decisional stages of adoption of CRC screening behavior. Thus, little is known about how these factors are associated with the decisional stages of CRC screening adoption. A clearer understanding of these associations could offer useful information for developing stage-matched interventions that focus on increasing CRC screening among underserved minorities, by moving individuals along the decisional stages; this could, for example, specifically target KAs who are aware of risks (e.g., low 5-year relative survival rates diagnosed with an advanced stage of CRC and poor quality of life experienced after CRC treatment) from the disease and benefits from the screening, yet are unengaged with the screening (ACS, 2017b). Furthermore, studies have revealed how cultural factors may be linked to CRC adoption among KAs. A study found fear of finding CRC and burdening the family, fatalism, and stigma toward cancer to be cultural barriers to Chinese and KAs’ utilization of CRC screening (Jung et al., 2017). H. Y. Lee and Im (2013) reported that a sense of fatalism or helplessness plays a critical role in underutilization of CRC screening for KAs. However, there is a need for further studies that offer a better understanding of how these cultural factors influence decisional stages and processes pertaining to CRC screening adoption among KAs.
Theoretical Framework
The present study employed Weinstein’s precaution adoption process model (PAPM) as a theoretical framework, a stage-based theory of health behavior change (Weinstein, 1988). The PAPM describes the process of adoption of preventive behaviors such as cancer screening, and characterizes seven discrete stages by individuals’ awareness, intention, and past health behavior (i.e., engagement): Stage 1—unaware of screening, Stage 2—aware of but unengaged with screening, Stage 3—deciding screening, Stage 4—decided not to uptake screening, Stage 5—decided to uptake screening but not yet in action, Stage 6—completed screening, and Stage 7—maintaining screening (Costanza et al., 2005; Hester et al., 2015). Furthermore, the PAPM has been widely used to understand diverse health behaviors, including exercise, diet, smoking cessation, vaccination, and cancer screening (Costanza et al., 2005).
Therefore, the purpose of this study was to examine factors associated with decisional stage of adoption for CRC screening among KAs using the PAPM. The research questions of the study were as follows:
Method
Study Design
A quantitative, descriptive, cross-sectional design was used. Participants were asked to complete a survey on sociodemographic information, health-related information (i.e., regular medical checkups and family cancer history), CRC screening history, a physician’s CRC screening recommendation, CRC screening knowledge, self-efficacy for CRC screening, decisional balance (i.e., attitudes and beliefs of CRC screening), and PAPM stage.
Sample
The sample included KAs aged 50 to 75 years who were recruited through advertisements via a local ethnic radio station, religious organizations, senior centers, and referrals. Interested participants were screened for eligibility based on the following criteria: a self-identified Korean or Korean American and a current resident in the Atlanta metropolitan area. Exclusion criteria were those younger than 50 years or older than 75 years because the ACS and the USPSTF both recommend beginning CRC screening at 50 years and continuing until age 75 (ACS, 2017a; USPSTF, 2016a). Individuals who reported having a history of any type of cancer were excluded.
Study Setting
The Atlanta metropolitan area in the state of Georgia was the setting. The researcher and three staff in the research team trained for data collection administered the survey to participants at locations, including senior centers, churches, and community centers, according to participants’ convenience and preference.
Data Collection
Data were collected between May 2015 and February 2016. To collect data, the research team developed a list of Korean American community organizations, including senior centers, churches/temples, and associations, and then contacted each organization via phone call and e-mail for data collection. With each organization’s permission and convenience for time and place, the research team administered self-report survey questionnaires, immediately after explaining the nature and purpose of the study and obtaining informed consent documents from participants who agreed with participation in the study. Selection of measures in the survey was guided by the existing literature and the PAPM. All of the instruments were translated into Korean using a back-translation method. Two bilingual faculty at an English literacy department at a university and a bilingual community health professional reviewed the translation. A pilot test of the survey questionnaire with six Korean American men and women was conducted. This study was approved by a university institutional review board.
Measures
Control Variables
Sociodemographic characteristics of the participants were assessed as control variables. These variables include a continuous variable (i.e., length of residence in the United States) and categorical variables (i.e., age, gender, health insurance, marital status, education, annual household income, self-rated economic status, and English proficiency).
Outcome Variable
The outcome variable of this study was the PAPM stage to investigate differences across the stages of CRC screening adoption. To determine the PAPM stage, the three criteria presented by Weinstein et al. (Bahmani, Baghianimoghadam, Enjezab, Mahmoodabad, & Askarshahi, 2016; Weinstein, Sandman, & Blalock, 2008) were used: (a) awareness of CRC screening, (b) engagement with CRC screening, and (c) intention on CRC screening. Figure 1 demonstrates the decision procedure of the PAPM stage in the participants.
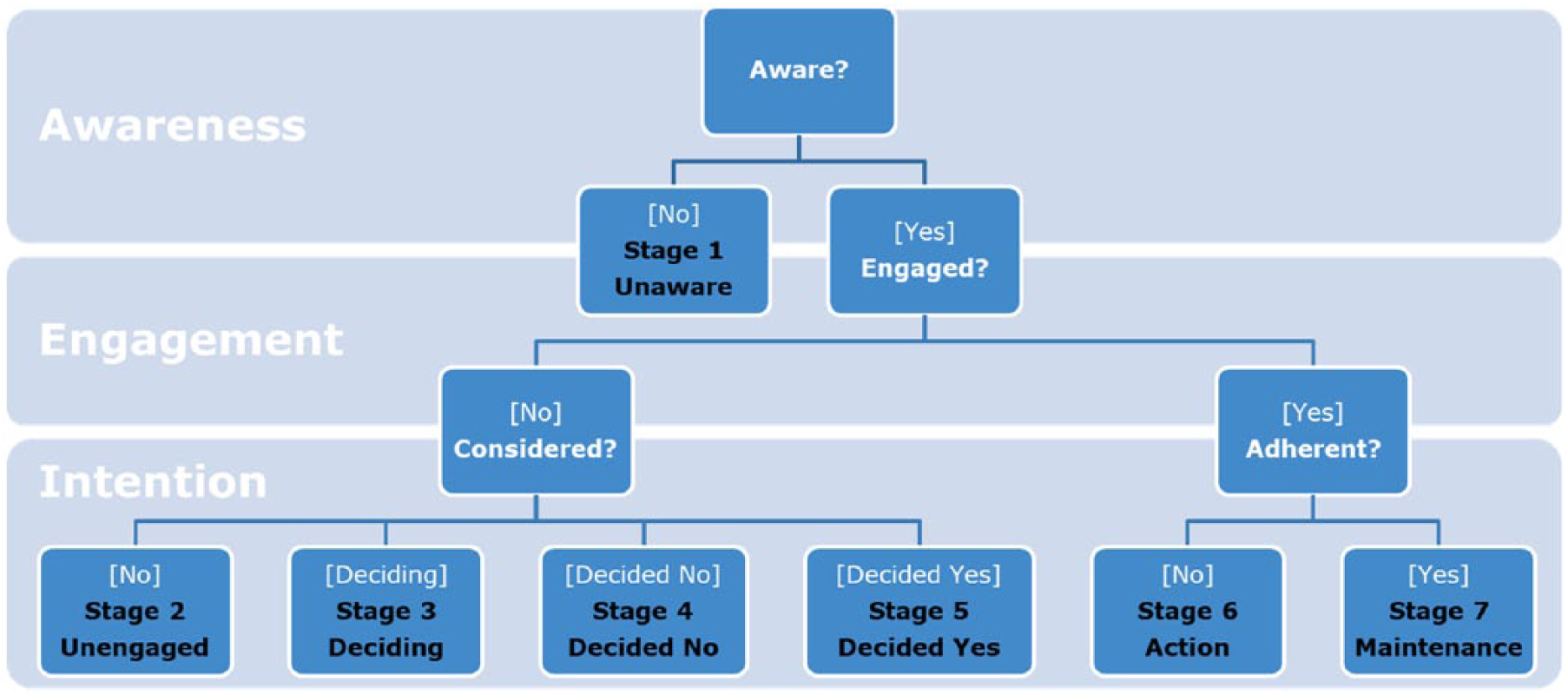
Precaution adoption process model (PAPM) decision tree.
Independent Variables
Independent variables for this study comprised regular annual medical checkups, family cancer history, a physician’s CRC screening recommendation, knowledge of CRC screening, self-efficacy for CRC screening, and decisional balance (i.e., attitudes and beliefs of CRC screening). A summary of the independent variables is presented in Table S1 (Supplementary table is available in online version of the article).
First, participants’ regular annual medical checkups were measured with a single item, “Do you receive regular medical checkups every year?” Family cancer history was measured with one item, “Has any of your family (parents, grandparents, siblings, or close relatives) ever had cancer of any kind?” A response to each question was “yes” (1) or “no” (0).
Second, a physician’s CRC screening recommendation was assessed using an item, “Has a doctor ever recommended you to have any of FOBT, sigmoidoscopy, and colonoscopy?” A “yes” response is denoted as 1 and “no” as 0. The selection of “no” indicates that a participant had never had any kind of CRC screening recommendation from a doctor.
Third, knowledge of CRC screening was assessed with two instruments: a 7-item CRC Knowledge Assessment Survey (KAS; Sanchez, Palacios, Thompson, Martinez, & O’Connell, 2013) and an 11-item CRC Familiarity Scale (Han, Huh, Kim, Kim, & Nguyen, 2014). The CRC KAS consisted of general CRC screening knowledge (four items, e.g., “Both men and women at age of 50 should begin colorectal cancer screening” and “To screen colorectal cancer or find polyps, one should take flexible colonoscopy every 10 years”) and CRC risk factor knowledge (three items, e.g., “Obesity raises the risk of colon cancer in both men and women” and “Colorectal cancer has been linked to the heavy use of alcohol”) with options of “true” and “false.” Additionally, the CRC Familiarity Scale asked about how familiar a participant is with the terms (e.g., abnormal, benign, colon, and polyp) used when patients undergo CRC screening. These terms in this scale were developed from printed materials such as flyers or brochures created by cancer-related institutes, on a 5-point Likert-type scale from 0 (not familiar) to 4 (very much familiar). A total CRC knowledge composite score was calculated as the mean value of both scales, with the higher score indicating the better CRC screening knowledge. The Cronbach’s α for this scale in this study was .866.
Fourth, self-efficacy for CRC screening was measured with 12 items adapted from Luszczynska and Schwarzer’s (2003) self-efficacy scale on a 7-point Likert-type scale from 1 (strongly disagree) to 7 (strongly agree). These 12 items consisted of a 4-item subscale about each of FOBT, sigmoidoscopy, and colonoscopy that asked certainty of overcoming expected difficulties. Example items included the following: “I am able to perform FOBT regularly even if I will have to make a detailed plan describing how to remember about FOBT” and “I am able to perform colonoscopy regularly even if I will have to overcome my different habit of nonexamination.” The Cronbach’s α for this scale in this study was .874.
Finally, decisional balance was measured using an adapted version of the 18-item decisional balance scale (Costanza et al., 2005). The 18 items consisted of 7 positive statements about CRC screening and 11 negative statements about each of CRC screening. A positive statement, for example, includes the following: “Having colorectal cancer screening gives me peace of mind about my health”; a negative statement example includes the following: “Screening causes me a lot of worry or anxiety about getting colorectal cancer.” A degree of agreement on a 5-point Likert-type scale from 1 (strongly agree) to 5 (strongly disagree) was computed. The Cronbach’s α for this scale in this study was .915.
Data Analysis
Descriptive statistics and univariate analysis were run to examine sociodemographic characteristics and CRC screening rates of the sample. Frequency analysis was used to assess the distribution of decisional stage of CRC screening adoption of the sample. To compare male and female samples, t test for continuous variables and chi-square test for categorical variables were used. Finally, multiple logistic regression analysis was used to assess associations of potential factors with PAPM stage of CRC screening adoption (Rakowski et al., 1997). For the purpose of data analysis, Stages 1 and 2 were combined into Stage 1/2 and Stages 6 and 7 into Stage 6/7 for bivariate analysis: Stages 1, 2, and 3 into Stage 1/2/3 (preadoption group) and Stages 5, 6, and 7 into Stage 5/6/7 (adoption group) for multiple logistic regression analysis. Stata/SE 14.1 was used for the analyses.
Results
A total of 526 KAs met the study inclusion criteria and were enrolled to participate in this study. The final sample included 433 participants (82.3%) who completed the survey. Given the number of Korean American population in the state of Georgia and the level of significance set as a priori (p < .05), a sample size of ⩾500 was determined to address the study purpose.
Sample Characteristics
Table 1 shows the characteristics of the participants (N = 433). The majority were female (61.7%), married (84.0%), and insured (74.4%). The mean age was 58.8 (SD = 7.22), average length in the United States was 22.3 years (SD = 10.50), and 58.6% had completed college and above. About 41% had an annual household income below $40,000 and above three quarters (78.5%) self-rated economic status as moderate or above. Nearly half of the participants (47.8%) reported their English proficiency level as bad or very bad. There were significance gender differences in marital status (p < .01), education (p < .001), and English proficiency levels (p < .05).
Sample Sociodemographic Characteristics (N = 433).
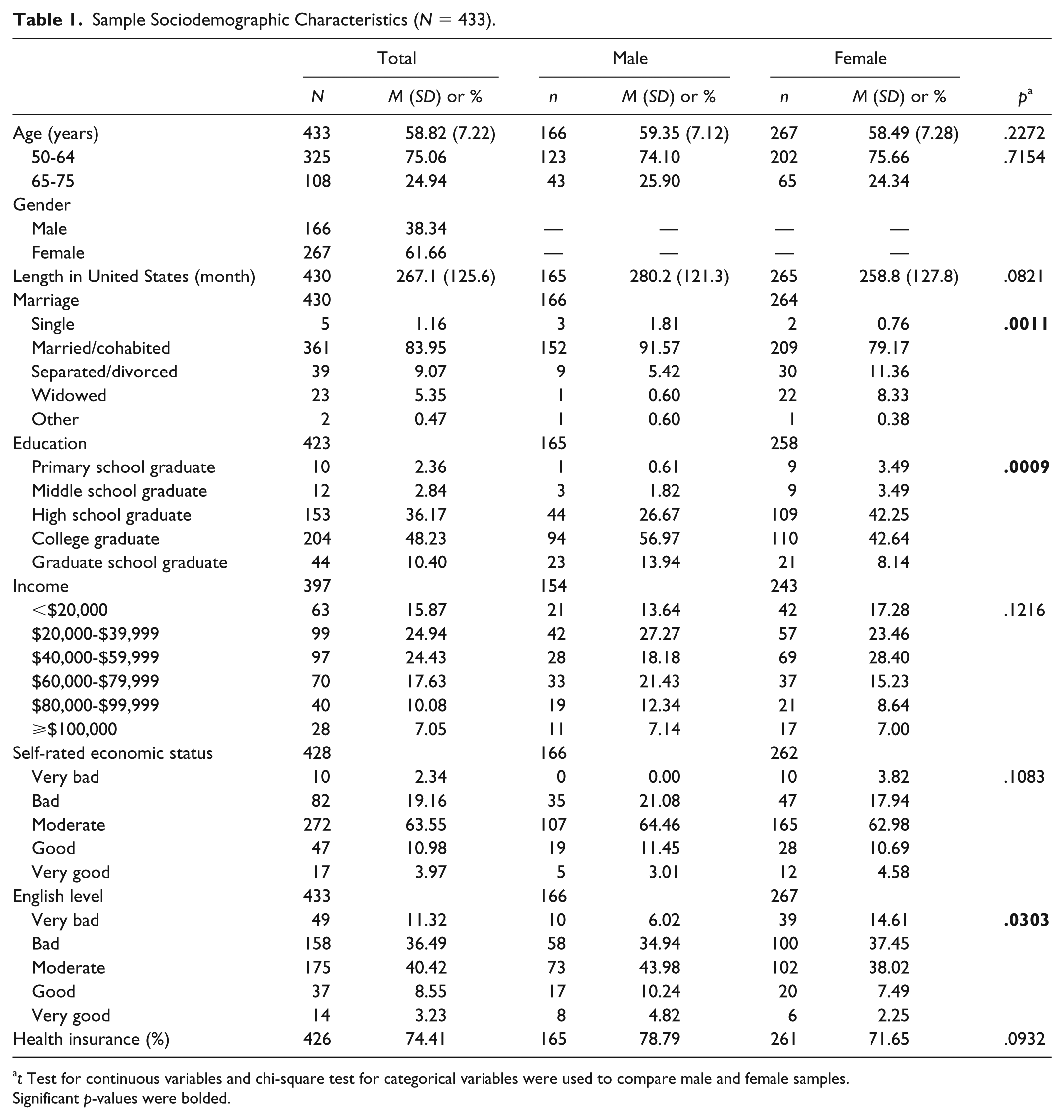
t Test for continuous variables and chi-square test for categorical variables were used to compare male and female samples.
Significant p-values were bolded.
Table 2 demonstrates distributions of PAPM stages for the participants. About 5% (n = 20) of the participants were in Stage 1 (unaware), 13.9% (n = 60) in Stage 2 (unengaged), 4.2% (n = 18) in Stage 3 (deciding), 12.9% (n = 56) in Stage 4 (decided no), 3.2% (n = 14) in Stage 5 (decided yes), 15.5% (n = 67) in Stage 6 (action), and 45.7% (n = 198) in Stage 7 (maintenance).
Distribution of PAPM Stage of Adoption for CRC Screening (N = 433).
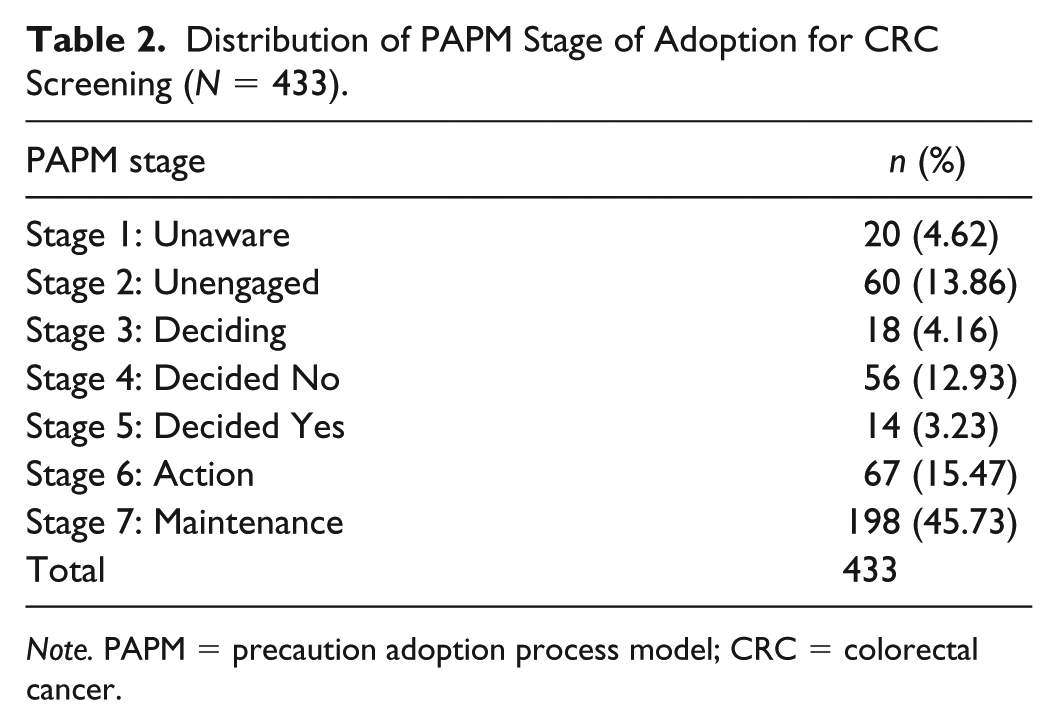
Note. PAPM = precaution adoption process model; CRC = colorectal cancer.
CRC Screening Rates (Research Question 1)
Table 3 shows the history of CRC screening completion and adherence to the screening guideline for the participants. While 61.2% reported to have ever had any screening test, only 46% were up-to-date with any of the tests. Moreover, about 8% completed FOBT in last year, 18.5% sigmoidoscopy within past 5 years, 43.4% colonoscopy within last 10 years—the percentages reported were not mutually exclusive.
CRC Screening Rates (N = 433).
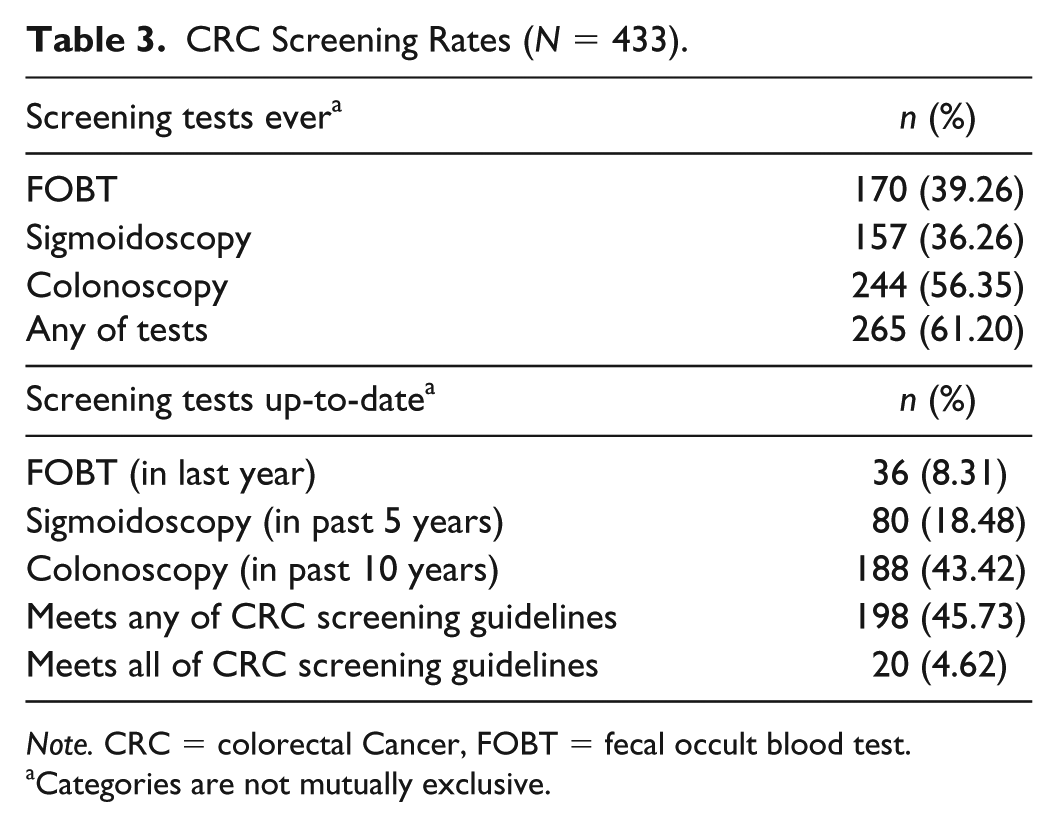
Note. CRC = colorectal Cancer, FOBT = fecal occult blood test.
Categories are not mutually exclusive.
Factors Associated With PAPM Stage of CRC Screening Adoption (Research Question 2)
Logistic regression analyses were conducted to examine factors associated with PAPM stage of adoption of CRC screening. As mentioned earlier, for data analysis purposes, the PAPM stages were combined as the follows: Stage 1/2/3 (unaware/unengaged/deciding), Stage 4 (decided no), and Stage 5/6/7 (decided yes/adoption/maintenance). Table 4 shows the results.
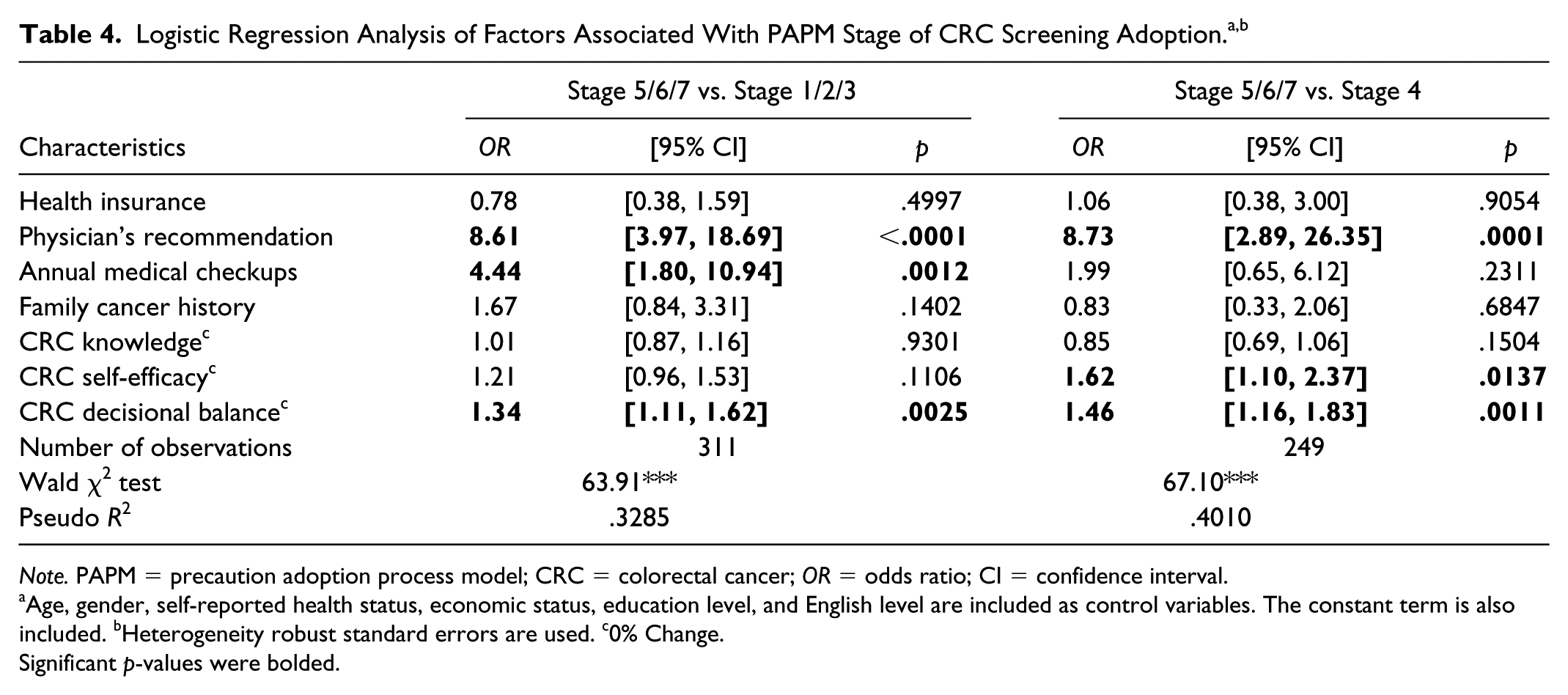
Note. PAPM = precaution adoption process model; CRC = colorectal cancer; OR = odds ratio; CI = confidence interval.
Age, gender, self-reported health status, economic status, education level, and English level are included as control variables. The constant term is also included. bHeterogeneity robust standard errors are used. c0% Change.
Significant p-values were bolded.
Stage 5/6/7 (Decided Yes/Adoption/Maintenance) Versus Stage 1/2/3 (Unaware/Unengaged/Deciding)
Factors that distinguish those who had decided to adopt CRC screening from those who had never decided were investigated. The analysis revealed that higher scores of decisional balance (odds ratio [OR] = 1.34; 95% confidence interval [CI: 1.11, 1.62]), having a physician’s recommendation (OR = 8.61; 95% CI [3.97, 18.69]), and having regular annual medical checkups (OR = 4.44; 95% CI [1.80, 10.94]) were significantly associated with higher PAPM stage (Stage 5/6/7) compared with lower stage (Stage 1/2/3), controlling for other variables.
Stage 5/6/7 (Decided Yes/Adoption/Maintenance) Versus Stage 4 (Decided No)
Factors that distinguish those who had decided to adopt CRC screening from those who decided not to adopt CRC screening were examined. The analysis revealed that those in Stage 5/6/7 were likely to have greater perceived self-efficacy for CRC screening (OR = 1.62; 95% CI [1.10, 2.37]), higher scores of decisional balance (OR = 1.46; 95% CI [1.16, 1.83]), and a physician’s recommendation (OR = 8.73; 95% CI [2.89, 26.35]) compared with those in Stage 4.
Discussion
The present study examined factors associated with decisional stage of adoption for CRC screening among KAs using the PAPM. This study highlighted a range of factors that may increase CRC screening among KAs, such as a physician’s recommendation, regular annual medical checkups, greater perceived CRC self-efficacy, and higher scores of decisional balance (attitudes and beliefs about CRC screening). The findings of this study provide useful information for community health care providers that may be used to improve patient-centered screening services and develop culturally tailored interventions designed to promote CRC screening among KAs.
First, the study found that less than half (45.7%) of the participants adhered to the recommended CRC screening guideline (Research Question 1). The adherence rate reported in this study is lower than that of a population-based study (52%) and slightly higher than those of other previous studies for KAs (Oh & Jacobsen, 2014). More specifically, this rate is still lower compared with those among overall Asian Americans (58%), non-Hispanic White Americans (66%), and the Healthy People 2020 goal (70.5%; Jackson et al., 2016; Oh & Jacobsen, 2014). According to existing literature, the low rates of adherence to CRC screening for KAs can be, in part, because of poor acculturation—nearly half (47.8%) of the study participants rated their English proficiency level as “bad” or “very bad,” while their average length of residence in the United States was more than 20 years (Diaz et al., 2013; Sentell, Braun, Davis, & Davis, 2013). Particularly, as sigmoidoscopy and colonoscopy composite complex procedures of tests (e.g., patients’ taking bowel preparation medication prior to the procedure), keen cooperation between health care providers and patients who lack English proficiency is warranted for successful completion of screening (Hayat, Lee, Lopez, Vargo, & Rizk, 2016). Therefore, for patients with limited English proficiency, it is important for health care providers to actively involve a medical interpreter or phone-based interpretation assistance in their screening services in order to enable transparent health care provider–patient communication to occur during the entire screening process (Peterson et al., 2016).
Next, in both hypothesized models, the study found a physician’s recommendation and decisional balance to be factors that distinguish the higher decisional stage (Stage 5/6/7) of CRC screening adoption from the lower stages (Stage 1/2/3 and Stage 4; Research Question 2). As expected, a physician’s recommendation was the strongest factor in both models, which are consistent with findings of previous studies that a physician’s recommendation is significantly linked to CRC screening for KAs and other Asian populations (Jung et al., 2017; S. Lee, Chen, Jung, Baezconde-Garbanati, & Juon, 2014; Oh, Jun, Zhao, Kreps, & Lee, 2015). This finding suggests that physicians and other health care providers should continue to recommend that their patients who have not yet decided to or have decided not to uptake CRC screening get screened. Specifically, the finding sheds light on potential roles of nurses or nurse practitioners in recommending CRC screening for KA patients at health care settings.
Future research should test the effects of practitioner recommendations on the adoption of CRC screening among KAs to extend relevant knowledge in the field. Furthermore, as the literature regarding cancer screening using PAPM analysis revealed, our models also found that positive decisional balance is significantly associated with higher PAPM stage in comparison with a lower one (Tuokko et al., 2016). This finding implies that although patients are recommended to undergo CRC screening by their health care provider, the recommendation may not necessarily lead to progress in decisional stage of CRC screening adoption because of negative attitudes and beliefs pertaining to CRC screening, namely, decisional balance. Prior research also indicated that compared with those having ever had CRC screening, KAs having never had CRC screening tend to report greater culturally embedded beliefs and attitudes of CRC screening (e.g., having no symptoms, a sense of fatalism/helplessness regarding CRC, fear of finding CRC and pain/embarrassment regarding CRC screening, stigma toward CRC, and concerns about burdening the family) which impede KAs from seeking CRC screening (Jung et al., 2017; S. Lee, Jung, Ng, & Sim, 2015; Maxwell, Crespi, Antonio, & Lu, 2010). Therefore, when these attitudes and beliefs are deeply interwoven with patients’ own culture, health care providers should be well versed with cultural barriers to screening and consider tailoring recommendations in a manner that improves attitudes and beliefs about CRC screening (Alden, Friend, Schapira, & Stiggelbout, 2014; Donnelly & Hwang, 2015).
Finally, in the same models, this study found that regular annual medical checkups were associated with Stage 5/6/7 compared with Stage 1/2/3, while self-efficacy for CRC screening was associated with Stage 5/6/7 compared with Stage 4. The findings suggest that regular annual medical checkups can be instrumental in making the decision to participate in screening. This may be because patients adhering to regular annual medical checkups have opportunities for receiving recommendations for CRC screening, which may, in turn, improve their attitudes and beliefs regarding screening. Therefore, it is essential for health care providers to ensure their patients are informed of CRC screening during annual medical checkups. The findings also suggest developing a community-based intervention in collaboration with health care providers for educating patients and distributing stool-based test kits, especially for patients who have not made a decision to undergo CRC screening (Sarfaty et al., 2013; Wolf et al., 2015). On the other hand, for individuals who have decided against CRC screening uptake (Stage 4), the findings suggest health care providers should consider patients’ levels of self-efficacy. As mentioned earlier, partly because patients with low self-efficacy for CRC screening may perceive increased complexity in taking the screening tests, despite continuous a physician’s recommendation, it is highly likely for these patients to have difficulties in overcoming multiple barriers to receiving screening.
Researchers have noted culture- and gender-related barriers to the uptake of CRC among KAs. The cultural related barriers include low knowledge and awareness of CRC, reluctance to discuss CRC with a health care provider, relatively poor health/medical literacy, high anxiety or fear about CRC and CRC screening, absence of health insurance or a health care provider, limited English proficiency, fatalism, and stigmas toward cancer (Jung et al., 2017; Le et al, 2014; H. Y. Lee & Im, 2013). Also, Korean American women tend to feel more comfortable with female physicians and technicians (Le et al., 2014). These culture- and gender-related factors prevent access to CRC screening tests and the early detection of CRC, and that can result in a late-stage CRC diagnoses for KAs. Previous research shows that KAs are diagnosed with the highest rate of Stage III cancer among other Asian subgroups (Yi et al., 2013). Therefore, it is crucial to address culture- and gender-related barriers to allow for the early detection of CRC. Moreover, health care providers, especially those working in clinics serving underserved communities, could play a key role in identifying whether patients are reluctant to or refuse screening. Such determinations can help health care providers navigate barriers to CRC screening among KAs.
Limitations
The findings of the present study have several limitations. As this study employed convenience sampling to recruit study participants from Korean American communities in a metropolitan area of the U.S. Southeastern region, the findings of this study cannot be generalized to all KAs. Next, although the findings of this study showed important associations among study variables, the findings derived from cross-sectional survey data cannot explain causal-effect relationships between PAPM stages and the variables. Due to the low number of participants in certain decisional stages, several PAPM stages were combined for the analyses. A more evenly distributed number of participants in each stage might reveal different distinguishing characteristics between the stages. Finally, this study excluded participants self-reporting a history of any kind of cancer but included those with a history of colitis and/or polyps. Exclusion of participants with a history of colitis and/or polyps from the present study might affect the decisional processes of the older KAs.
Implications for Future Studies
To our knowledge, this study is the first to adopt the PAPM to examine decisional stage associated with CRC screening adoption among KAs. The findings provide key considerations for nursing practices and interventions to facilitate CRC screening among KAs. In the primary care setting, nurses can assess patients’ decisional stages of CRC screening. Particularly for patients who are in low decisional stage groups, nurses can develop culturally tailored and language-concordant interventions that focus on improving knowledge and self-efficacy regarding CRC screening. For patients with limited English proficiency, it is also important for nurses to provide adequate information and resources about CRC (e.g., incidence rate, risk factors, and symptoms) and CRC screening (e.g., procedure, cost, detection rate, and side effects), free from medical jargon. In community settings, nurses in collaboration with partners (e.g., nonprofit organizations and ethnic churches) could reach out to individuals exhibiting risk factors for CRC through community events. Novel prescreening activities in public contexts may serve to eliminate barriers to accessing screening services among KAs and increasing their knowledge and self-efficacy of CRC screening. Finally, increasing public awareness of the importance of CRC screening, within the cultural context of health, would be a substantial secondary prevention intervention to change the public view of CRC screening.
Supplemental Material
Table_S1-10.9 – Supplemental material for Analyzing Factors Associated With Decisional Stage of Adoption for Colorectal Cancer Screening Among Older Korean Americans Using Precaution Adoption Process Model
Supplemental material, Table_S1-10.9 for Analyzing Factors Associated With Decisional Stage of Adoption for Colorectal Cancer Screening Among Older Korean Americans Using Precaution Adoption Process Model by Seok Won Jin, Jongwook Lee and Sohye Lee in Journal of Transcultural Nursing
Footnotes
Acknowledgements
Special thanks to Professor Ruth A. Lindquist, PhD, RN, FAAN, School of Nursing, University of Minnesota, Minneapolis for her careful reviewing of our article and her many insightful comments and suggestions.
Authors’ Note
The contents are solely the responsibility of the authors and do not necessarily represent the official views of NIMHD or NIH.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The first author was supported by the National Institute on Minority Health and Health Disparities (NIMHD) Grant Number U54MD008173, a component of the National Institutes of Health (NIH).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.