
Abstract
Introduction
Health care providers working in critical care units are susceptible to more stress than any other health professionals (American Association of Critical-Care Nurses, 2008). Workers in such environments are emotionally influenced by caring for dying patients (Todaro-Franceschi, 2013), ethical decision making (Teixeira, Ribeiro, Fonseca, & Carvalho, 2013), patients’ persistent suffering (Todaro-Franceschi, 2012), medical futility, miscommunication (Curtis, Sprung, & Azoulay, 2014), and the needs of patients’ relatives (Epp, 2012). Also, the critical care unit work environment is a highly specialized section that requires high medical knowledge and skills (Van Mol, Kompanje, Benoit, Bakker, & Nijkamp, 2014). Hence, stress is a common phenomenon for nurses working in critical care units and often results in physical and psychological suffering of nurses (Maiden, Georges, & Connelly, 2011).
Although the stressful nature of critical care work is common across settings, little is known about how professionals from various cultures may respond to this stress and how their reactions may affect delivery of patient care or workers’ well-being. Improving patient and family care outcomes has been said to require “nuanced understanding of cultural contexts for those who provide care and those who receive it” (Schim & Doorenbos, 2010, p. 1). Because beliefs, customs, and practices related to health care may differ across societies and cultural groups, responses to high-stress nursing environments should be examined within a framework of cultural congruence (Schim & Doorenbos, 2010). The meaning nurses give to patient suffering and one’s self-care practices to ameliorate stress may differ depending on religious and cultural values (Günüşen, Wilson, & Aksoy, 2018). To reduce health disparities, investigations that consider the social environment and context of care are needed to uncover cultural differences that could, ultimately, influence patient care (World Health Organization, 2005).
In recent years, the concept of professional quality of life (ProQOL) has been proposed to show the level of occupational stress and has been particularly relevant in examining providers of health care. ProQOL is a general construct that is defined as “the quality of one’s feeling in relation to his/her job as a helper.” It has both positive and negative aspects. The negative aspect is called compassion fatigue (CF) that includes both burnout (BO) and secondary traumatic stress (STS; Stamm, 2010). CF has also been called the cost of care (Figley, 1995) and has been described as a negative effect of working with suffering and traumatic patients in health care professionals (Bride, Radey, & Figley, 2007). CF is a cumulative and progressive result of prolonged, continuous, and high-frequency contact with patients and also exposure to stressful environments (Smart et al., 2014). CF can be distinguished from BO in that CF is more specific and includes behavioral responses of health care providers who are involved with suffering patients (Gilmore, 2012) and can lead to physical and psychological distress (Sheppard, 2015). BO as a component of CF can significantly affect the health outcomes of patients and has a strong negative relationship with the staff morale (Leiter & Maslach, 2009). The other component of CF is STS, which is an extreme response to traumatized patients or traumatic stressful events (Stamm, 2010). The negative effects of STS include fear, sleep disturbances, intrusive images, and avoiding reminders of traumatic experiences (Stamm, 2010).
The positive aspect of ProQOL is called compassion satisfaction (CS). CS is the opposite of CF (Coetzee & Klopper, 2010). In fact, despite high level of CF, studies have shown that health care providers have positive feelings in addition to negative ones while caring for patients (Dunn, 2009; Stamm, 2010). Caring, compassion, and empathy for patients are believed to affect the personal and professional aspects of care providers’ lives. Ideally, there should be a balance between CF and CS within and outside the workplace, and the two constructs have been found to be inversely related (Smart et al., 2014). Low professional quality of life can lead to a poor attitude toward the profession, delay or absence from work (Poghosyan, Clarke, Finlayson, & Aiken, 2010), loss of self-worth, reduced productivity, and staff turnover (Boyle, 2011; Haber, 2013). Alternatively, high ProQOL can lead to an increase in the number of patients who are satisfied (McHugh, Kutney-Lee, Cimiotti, Sloane, & Aiken, 2011).
Although CF is believed to be improved through workplace social support, very few studies can be found that examine how different religious or cultural groups can specifically support workers based on values and beliefs regarding suffering and death (Günüşen et al., 2018). Cultural awareness that includes knowledge and recognition of facts that may influence patient care is an important aspect of providing culturally congruent care (Schim, Doorenbos, Benkert, & Miller, 2007). The findings of several studies indicate that the degree of BO in critical care nurses is higher than that of those who work in other wards (Hunsaker, Chen, Maughan, & Heaston, 2015; Rushton, Batcheller, Schroeder, & Donohue, 2015). While evidence from studies in North America show that the concept of professional quality of life is an important phenomenon (Beck, 2011; Boyle, 2011; Coetzee & Klopper, 2010; Hooper, Craig, Janvrin, Wetsel, & Reimels, 2010; Potter et al., 2010), to date, most of the studies on ProQOL have been conducted in the United States (Drury, Craigie, Francis, Aoun, & Hegney, 2014). The status of ProQOL among nurses working in critical care environments in Iran or other Middle Eastern countries is not well-investigated.
One of the most important and effective individual beliefs in providing nursing care is the nurses’ cultural and religious beliefs (Ghafourifard, Zamanzade, Valizadeh, & Rahmani, 2017; K. Kim, Han, & Kim, 2015). Considering that Iran is a country dominated by Islam and Islamic Iranian culture is dominant, many Iranian behaviors and practices are based on religious teachings. A few prior studies suggest that religious orders in Iran can influence health-related social activities, such as blood donation (Charsetad, 2016) and delivery of compassionate care (Zamanzadeh et al., 2017). Two small qualitative studies of Iranian nurses suggested that Islamic teachings influence the delivery of compassionate acts (Zamanzadeh et al., 2017), and organizational support is needed to remove barriers to compassionate care (Valizadeh et al., 2016). As of yet, little research is available to measure whether Islamic religious beliefs can protect against the negative aspects of delivering care, such as CF. Results of studies that are generally conducted in Western countries may not reflect other countries. Therefore, the aim of this study was to assess the prevalence of BO, STS, and CS among Iranian nurses working in critical care units. It also sought to determine the relationship between these concepts in order to provide validation for the ProQOL measurement among Iranian nurses. By evaluating and comparing with other published studies, we can learn whether unique findings exist for the cultural group of Iranian critical care nurses and if the ProQOL tool performs similarly.
Material and Method
Design and Setting
This is a descriptive, correlational, survey study. The study was conducted in eight educational hospitals affiliated with University of Medical Sciences in Province, East Azarbayjan a north-western province of Iran.
Participants
Study participants were recruited from critical care units within the participating hospitals. The study population includes nurses who met the following criteria: providing bedside care in critical care units, working at least 1 year in the selected units, and having at least a bachelor’s degree in nursing. The study sample size (n = 397) was calculated using G Power program 3_1 (Franz Faul, Universität Kiel, Germany) at the significance level of .05. The stratified nonrandom sampling method was used in which the population divided into subgroups (hospitals) and a predetermined portion of sample drawn from each subgroup. Considering 10% expected sample attrition and/or missing data, 440 nurses were invited to participate in the study and 400 nurses accepted the invitation to join.
Instruments
The instrument for data collection consisted of two parts. The first part was a demographic questionnaire, which includes some personal and professional characteristics of nurses such as age, gender, type of ward, and their professional experiences. The second part was ProQOL, which consisted of 30 items to assess nurses’ quality of life in three dimensions: BO, STS, and CS. Nurses responded to each item of this questionnaire based on a 5-point Likert-type scale ranging from 1 (not at all) to 5 (most of the time), with 6 items that are scored in reverse. The Persian version of the ProQOL was used, which has had its psychometric properties studied among 464 Iranian physicians, midwives, and nurses resulting in an intraclass reliability value of r = .96 and internal reliability (Cronbach’s alpha) of r = .73 (Ghorji, Keshavarz, Ebadi, & Nasiri, 2018). We then tested the questionnaire for reliability within our targeted population of Iranian nurses in a pilot study including 20 nurses. Cronbach’s alpha coefficient value for CS, BO, and STS dimensions were .80, .72, and .76, respectively, in this pilot study. In the final study sample, Cronbach’s alpha coefficient values for CS, BO, and STS dimensions were .83, .78, and .79, respectively, demonstrating acceptable internal reliability.
Procedures
Before data collection, the study proposal was approved by the regional ethics committee of University of Medical Sciences (5d.24196). Next, researchers were referred to the predetermined hospitals from May 2016 to January 2017. Nurses who met the criteria for the study were identified, and all eligible nurses were invited to participate. After informing nurses about the study purposes, willing nurses were asked to fill the questionnaire and sign a written informed consent. Participants also were assured that their contribution to the study was fully voluntary and they could be excluded whenever they wished. The data were analyzed using SPSS version 16 after the reverse scoring of selected items. After the reverse scoring of selected items, participants were classified into three groups based on past publications. In the CS dimensions, average score is 37. About 25% of the people score higher than 42, and about 25% of the people score below 33. The average score on the BO scale is 22. About 25% of the people score above 27, and about 25% of the people score below 18. The average score on STS is 13. About 25% of the people score below 8, and about 25% of the people score above 17 (Stamm, 2005).
Demographic data and ProQOL were analyzed using descriptive statistics including frequencies, percentage, means, and standard deviations. To investigate the possible associations between ProQOL dimensions, Pearson correlation coefficient analyses were used. Independent t test were used to compare differences in mean scores of BO, STS, and CS between males and females. Analysis of variance (ANOVA) was used to compare mean differences of BO, STS, and CS scores according to age, marriage status, educational degree, unit, type of shift, work experience, and work experience in the current unit.
Results
A total of 440 questionnaires were distributed among nurses, of which 400 questionnaires were completed and returned (response rate of 91%). Table 1 shows participants’ descriptive characteristics. Most participants were married females between the ages of 30 and 39 years with baccalaureate degrees in nursing. The majority had rotational shifts and worked in the intensive care unit (ICU) with 6 to 10 years’ experience in nursing and 1 to 5 years’ experience in the current unit. The mean (SD) of nurses’ age was 33.64 years (7.12), and the mean (SD) of participants’ work experience in nursing and their work experience in the current unit were 9.72 (5.79) and 6.36 (5.26) years, respectively.
Descriptive Characteristics of the Study Sample (n = 400).
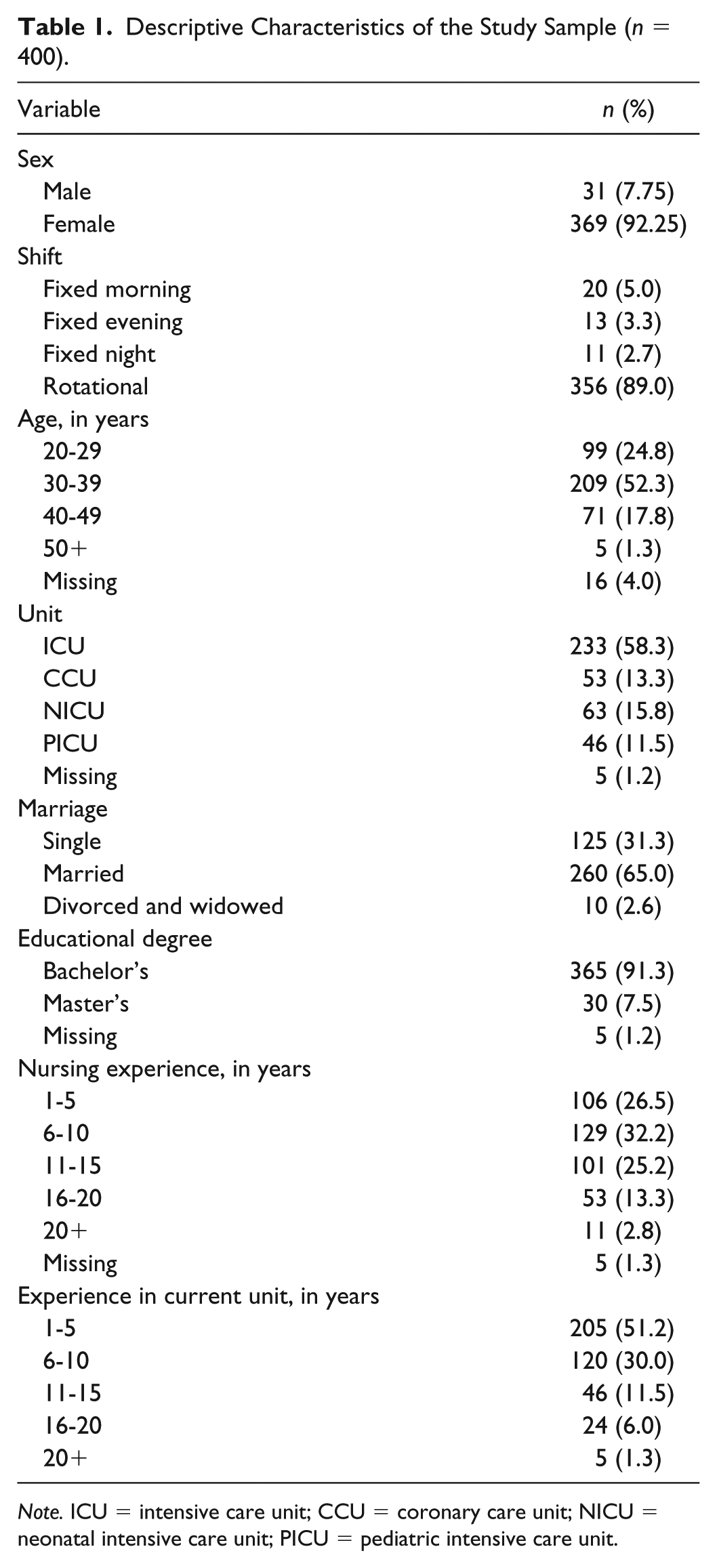
Note. ICU = intensive care unit; CCU = coronary care unit; NICU = neonatal intensive care unit; PICU = pediatric intensive care unit.
ProQOL Results
Table 2 summarizes ProQOL scores of participants. The mean (SD) of CS, BO, and STS scores were 36.27 (7.45), 26.68 (5.67), and 26.90 (5.66), respectively. The most favorable category of possible ratings for CS was identified in 18.8% of the subjects, while 37% had the lowest category of possible ratings. Also, 42% and 96% of the subjects had BO and STS scores higher than the average level, respectively, indicating unfavorable levels of CF.
Compassion Satisfaction, Burnout, and Secondary Traumatic Stress in Iranian Critical Care Nurses (n = 400).
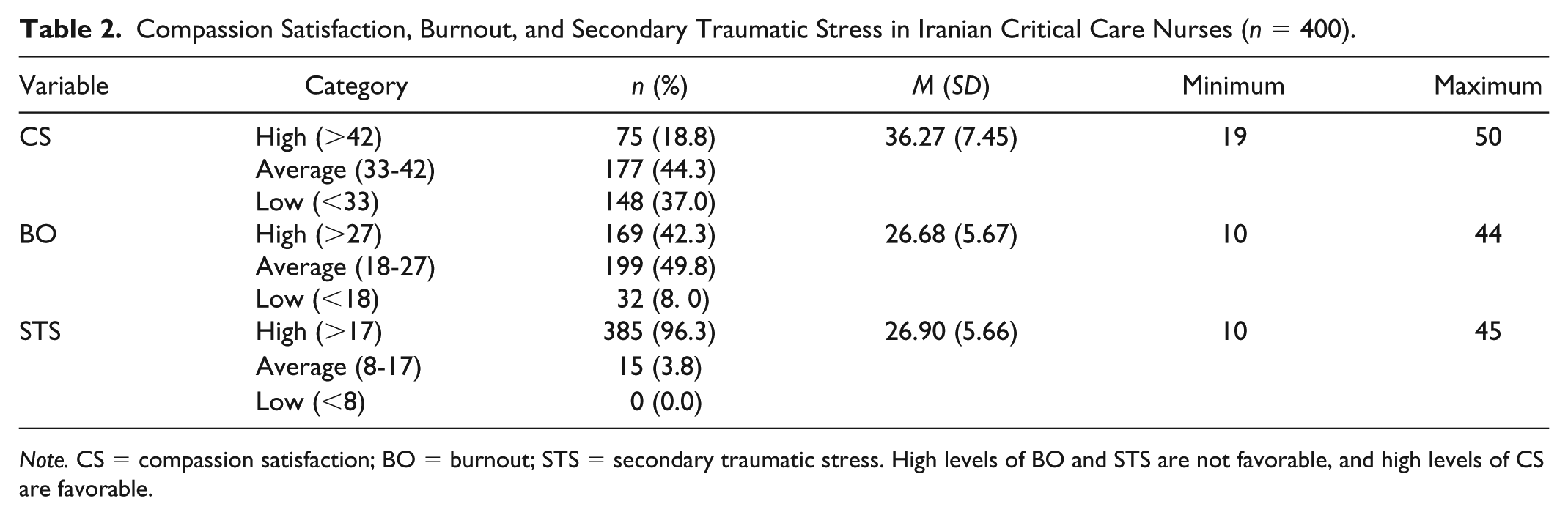
Note. CS = compassion satisfaction; BO = burnout; STS = secondary traumatic stress. High levels of BO and STS are not favorable, and high levels of CS are favorable.
Pearson correlation coefficient analyses revealed a significant positive association between BO and STS among nurses who worked in critical care units (r = .380, p < .001). In addition, a significant negative association was found between CS and BO (r = −.571, p < .001) and CS and STS (r = −.032, p < .001).
As shown in Table 3, the ANOVA test found a significant difference in CS scores according to the nurse’s age subgroup (p = .02) and nursing experience (p = .045). The post hoc Tukey’s test showed a significant difference between the mean of nurses’ CS scores in 30 to 39 and 40 to 49 years of age subgroups, with more favorable CS score in the 40 to 49 years subgroup. There was also a significant difference between the mean of CS scores among nurses with more than 20 years and those who had 6 to 10 years of work experiences, with most favorable scores in the nurses with more than 20 years of experience
Differences Between ProQOL Subscales Scores and Participants’ Demographic Characteristics (n = 400).
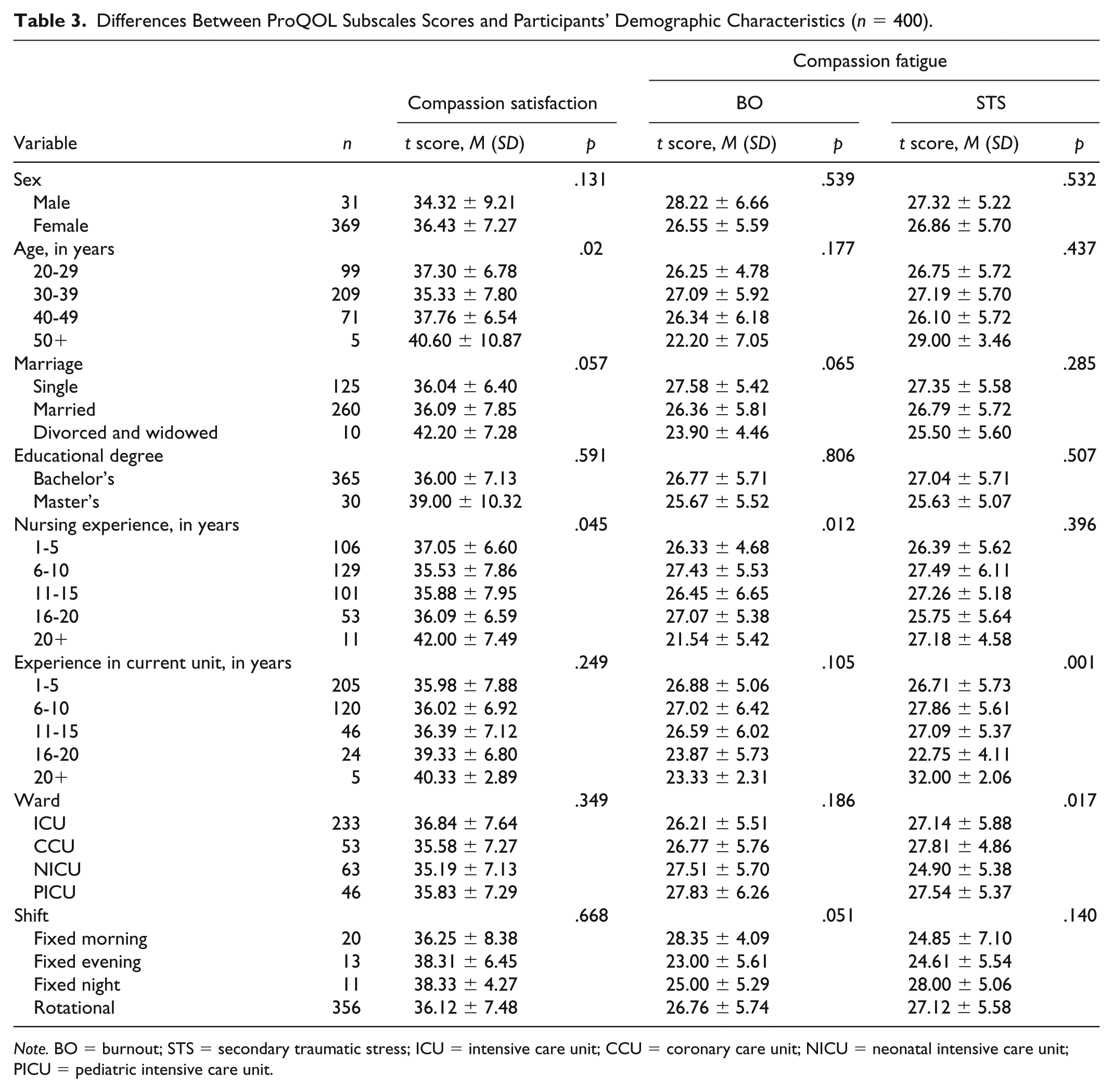
Note. BO = burnout; STS = secondary traumatic stress; ICU = intensive care unit; CCU = coronary care unit; NICU = neonatal intensive care unit; PICU = pediatric intensive care unit.
Using the ANOVA test, there was a significant difference in BO scores according to nursing experience (p = .012). The post hoc Tukey’s test showed a significant difference between the mean of BO scores among nurses with more than 20 years and among those who had 6 to 10 years of work experiences, with most favorable scores in the nurses with more than 20 years of experience.
Using the ANOVA test, there was also significant difference between nurses’ STS scores according to their work experience in the current unit (p = .001) and type of unit (p = .017). The post hoc Tukey’s test showed a significant difference between the mean of STS scores in nurses with 16 to 20 years and those who had 1 to 5, 6 to 10, and 11 to 15 years of work experiences, with most favorable scores in the nurses with 16 to 20 years of experience. There was also a significant difference between the mean of STS scores among neonatal intensive care unit (NICU) nurses and among CCU and ICU nurses, with most favorable scores in the NICU nurses group (Table 3).
Discussion
This is the first known study to measure Iranian critical care nurses using the ProQOL instrument. The findings indicate high levels of CF with the majority of respondents scoring in the average or higher level of BO and STS. This high burden of CF is an important finding among critical care nurses because it can negatively affect the health of both professionals and their patients (Bride et al., 2007; Kashani, Eliasson, Chrosniak, & Vernalis, 2010; Shanafelt, Bradley, Wipf, & Back, 2002). Therefore, it is important to recognize that culturally appropriate supports may be needed to deal with caregivers’ stress even when societies have strong religious underpinnings (Günüşen et al., 2017). Consistent with our findings, a high level of STS was found in nurses working with chronically ill children in Turkey where a high proportion of Muslim nurses practice (Günüşen et al., 2017). Comparatively, Maytum, Heiman, and Garwick (2004) found a moderate to high level of STS and BO among American nurses who work with children with chronic conditions where less than 1% identify as Muslim (Günüşen et al., 2017). One review study found that the prevalence of high risk for CF among nurses working in critical care units ranged from 7.3% to 40% around the world, suggesting a wide range of values that could be dependent on workplace characteristics or culture (Van Mol, Kompanje, Bakker, & Nijkamp, 2014).
Our study results showed that the mean score of BO (26), one of the dimensions of CF, was higher (more favorable) than that of some other published studies of nurses and health care professionals (Circenis & Millere, 2011; Galiana, Arena, Oliver, Sansó, & Benito, 2017). For example, the results of a similar study that was carried out among palliative care professionals using ProQOL questionnaire showed that the BO in both Spanish and Brazilian race was 15.62 and 15.05, respectively (Galiana et al., 2017). In the Circenis and Millere (2011) study, which was done using the ProQOL questionnaire on acute care nurses from all hospital units in Latvia, 54% have higher scores. Comparatively, in a study by Alexander (2006) of U.S. emergency nurses after a natural disaster, the BO score was 13.9, nearly twice as poor as our nurses’ scores. Further study is needed to determine if the differences between the results are due to individual, organizational, or cultural differences between the countries or work units.
According to our findings, 42% of the participants had high levels of BO. The results of another study showed that 58% of U.S. surgical intensive care unit trauma nurses reported moderate BO (Mason et al., 2014). It has been highlighted in previous studies that BO among nurses in critical care units is common due to stressful work environment (Embriaco, Papazian, Kentish-Barnes, Pochard, & Azoulay, 2007). In a review study by Van Mol et al. (2014), the prevalence of BO among nurses working in critical care units was reported to span from 1.2% to 49%. Our findings do fit within this range; yet it is notable that wide variations exist between studies.
Regarding STS as the second dimension of CF, our study findings showed that the mean score of STS in critical care nurses was 26.90 indicating a moderate or high level of STS for most of our respondents. The findings of a similar study in Spain showed that the mean of STS in both Spanish and Brazilian races were about half that score at 12.24 and 14.24, respectively (Galiana et al., 2017), where lower scores are more favorable. In two similar studies of Latvian acute care nurses and U.S. critical care nurses using the ProQOL questionnaire, the mean score of nurses’ STS was about 19 (Circenis & Millere, 2011; Smart et al., 2014), which also shows more favorable scores than our findings. Also, in a review study of predominantly North American and European countries, the prevalence of high-risk STS in critical care nurses ranged from 21% to 44% (Van Mol et al., 2014). The highest level of STS was reported by Jang, Kim, and Kim (2016) in Korea, who found that more than 79% of oncology nurses had moderate to high levels of STS (Jang et al., 2016). Compare this with our sample where 96% had higher than average levels of STS. STS is a negative, trauma-related emotion and happens due to encountering the suffering of another traumatized person (Stamm, 2002). The incongruities in scores may be related to specific unit differences in the frequency or severity of traumatic event, cultural factors in nursing care, or personal or organizational factors in how traumatic events are handled. The setting for nurses in our study involved contact with many suffering patients and few psychological support systems for workers. Iranian nurses have previously reported poor job security, inappropriate work conditions, and low wages, which are all factors that could contribute to increase in STS (Sokhanvar, Kakemam, Chegini, & Sarbakhsh, 2018).
In contrast to CF, there is CS that is defined as the intense satisfaction with the provision of care (Hooper et al., 2010). Studies about CS are very limited, despite that compassionate care is a way by which to improve patients’ outcomes and satisfaction. Our study findings showed that the mean score of CS in nurses working in critical care units was 36.27, with 37% of respondents scoring in the least favorable category. About half of our participants scored in the moderate range. Similar to our findings, the studies by Circenis and Millere (2011), Galiana et al. (2017), and Smart et al. (2014), using the ProQOL questionnaire, the CS reported were 37, 41.05, and 38.2, respectively. Mason et al. (2014) reported that 73% of U.S. surgical intensive care nurses had moderate levels of CS. In our study, we also found that CS had a significant negative correlation with BO and STS. Consistent with our findings, Smart et al. (2014) and Slocum-Gori, Hemsworth, Chan, Carson, and Kazanjian (2013) discovered a negative correlation between CS with BO and STS. We also found a significant positive correlation between BO and STS, which is congruent to the findings of other studies and shows that the ProQOL instrument performed as expected in our sample (Slocum-Gori et al., 2013; Smart et al., 2014).
In the current study, as in others, the ProQOL domains were found to be significantly different depending on demographic variables. For example, the CS scores were significantly different among varied age-groups and work experiences. Similarly, J. Kim and Lee (2016) found that CS had a significant relationship with age and work experience. Our study findings showed that nurses with more than 20 years of work experience had higher level of CS and lower BO than other nurses. This can be due to more adaptation of experienced nurses with the ward rules or that those who do not derive satisfaction from their work do not stay in the setting, along with perhaps they receive more support from other nurses with time in the job (Gilmore, 2012; Maslach & Leiter, 2008).
According to our findings, the STS level of nurses who were working in NICU was less than that of nurses working in CCU and ICU, which may be due to the stressful and sensitive environment of CCU and ICU. There was no similar study that assesses CCU and ICU nurses’ STS and compares it with nurses in other wards. More studies are needed to know whether our results are due to organizational deficits or individual traits of nurses working in various intensive care units. Also, nurses who had 16 to 20 years of work experience in the current ward had less STS than other nurses who had less experience. Kolthoff and Hickman (2017) reported that novice nurses had a higher level of STS than those with more work experience, which is consistent with our findings. Longitudinal studies are required to examine the causal relationship between these factors and ProQOL dimensions.
This study has limitations that should be taken into consideration including that it only included nurses working in the critical care units of the selected units and the perspectives of nurses working in other hospitals, as well as nurse managers, were not considered. Also, the psychological status of the participants during the study was not known and could have affected their responses. Future research replicating such studies in other settings and taking into account the views of nurses working in other wards are required. Evaluating how nurses from different work settings, cultures, and religious groups respond to self-care interventions could be important for tailoring effective programs in the future.
Conclusion
Assessing nurses’ professional quality of life is necessary before any interventions can be implemented to improve the work environment (Smart et al., 2014). Our study findings support the expected relationships between the three constructs of ProQOL and show that both dimensions of CF (BO and STS) are higher than many of those reported in Western countries. CF has diverse symptoms and can progress over time (Stamm, 2010). It also could have many negative consequences for workers, organizations (Sheppard, 2015), and patients (Hooper et al., 2010). Therefore, culturally appropriate strategies are needed to prevent and reduce CF complications.
Considering the desirable effects of CS for both professionals and patients (Lloyd & Carson, 2011; van der Cingel, 2011) and its negative relationship with CF, improving CS seems like one strategy to reduce CF in nurses. To enhance the ProQOL of nurses, especially those who are working in critical care units, preventive programs at the personal and organizational levels are crucial. In-service training programs such as stress and crisis management as well as the establishment of peer social support networks are essential. Additionally, in order to deal with CF, personal interventions are required to enhance nurses’ adaptation skills and their ability to maintain professional distances (Slatten, Carson, & Carson, 2011).
Footnotes
Acknowledgements
This article is part of the master thesis in nursing submitted to Nursing and Midwifery Department of Tabriz University of Medical Sciences and was supported by the Research Deputy of Tabriz University of Medical Sciences (Grant Number 5d.24197). The authors thank all the study participants.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Research Deputy of Tabriz University of Medical Sciences (Grant Number 5d.24196).