
Abstract
Family caregivers are a vital asset to cancer survivors during cancer diagnosis, treatment, and symptom management. These informal caregivers, who typically provide at least half of the care needed, become involved in complex care activities (Fletcher, Miaskowski, Given, & Schumacher, 2012) for an average of 14 months (Yarbroff & Kim, 2009). However, providing care to a family member or loved one with cancer can simultaneously compromise the well-being of caregivers (Teixeira, Applebaum, Bhatia, & Brandao, 2018). Family caregivers experience levels of distress that are as severe, and sometimes even more severe, than the distress that is experienced by the patients themselves (Gropper et al., 2016; Hasson-Ohayon, Goldzweig, Braun, & Galinsky, 2010). Understanding distress in family caregivers is important as this distress predicts patients’ subsequent distress (Milbury, Badr, Fossella, Pisters, & Carmack, 2013; Segrin & Badger, 2014; Segrin, Badger, Dorros, Meek, & Lopez, 2007) and is concurrently associated with patients’ physical health outcomes (Kim et al., 2008). The specific aim of this study is to test for differences in psychological distress and social support among family caregivers as a function of their relationship with the cancer survivor.
Caregivers of cancer survivors are in a precarious position as they not only provide instrumental and emotional support to their ill family member but must manage their own anxiety and distress that accompanies a family member’s diagnosis with a life-threatening illness. Perhaps as a result, compromised physical health, psychiatric morbidity, fatigue, and sleep impairment (Bambauer et al., 2006; Butow et al., 2014; Kim, Carver, Shaffer, Gansler, & Cannady, 2015; Kotronoulas, Wengstrom, & Kearney, 2013) are often evident among family caregivers. During these times, social support has proven to be vital to family caregivers and appears to have health promoting effects on their quality of life (Butow et al., 2014). In contrast, unmet needs, particularly informational, are associated with depression and anxiety among caregivers of cancer patients (Oberoi et al., 2016).
Family caregiving may be particularly burdensome for Latina and Latino family members. This caregiving responsibility often occurs in a larger sociocultural context marked by economic and educational challenges, minority stress, immigration issues, and health disparities that define a fragile context for the well-being of Latina and Latino family caregivers (Badger, Sikorskii, & Segrin, 2019; Siefert, Williams, Dowd, Chappel-Aiken, & McCorkle, 2008). Sociocultural norms within Latin cultures, such as familism (placing needs of the family over the individual) and marianismo (female gender roles emphasizing self-sacrifice and moral strength) place a high premium on support from family members due to strong family allegiance and attachment (Lopez-Class et al., 2011; Mendez-Luck & Anthony, 2016). Latin family networks include extended family members (e.g., aunts, uncles, and cousins) and close friends and members of religious communities who function as fictive kin (Katiria Perez & Cruess, 2014), all of whom are expected to provide care when it is needed.
In the cancer caregiving literature, the focus has often been on spousal caregivers of adult cancer patients (Thana, Lehto, Sikorkskii, & Wyatt, 2019), or parental caregivers of pediatric cancer patients. However, marriage rates have dropped precipitously in the United States, resulting in a growing population of unmarried people (Lundberg, Pollak, & Stearns, 2016). By implication, many cancer survivors do not have a spouse and must look to other family members and friends for informal caregiving. Also, for a variety of reasons including a younger demographic and higher prevalence of thyroid cancer that tends to occur earlier in life (Miller et al., 2018), Latina and Latino cancer survivors tend to be younger than non-Hispanic Whites (Nahleh et al., 2018) and by virtue of that fact are perhaps more likely to have a parental caregiver.
Comparative analyses that examine caregiver well-being based on relation of the caregiver to the cancer survivor are rare and have thus far yielded mixed results. In one unique example, daughters caring for a mother with cancer reported higher depression and family strain compared with husbands caring for a spouse with cancer (Bernard & Guarnaccia, 2003). Some related evidence suggests that spousal caregivers are more likely to experience psychological distress compared with nonspousal caregivers (Gotze, Brahler, Gansera, Polze, & Kohler, 2014; Lee, Lin, Chien, Fang, & Wang, 2018), whereas other research shows that nonspousal caregivers (e.g., siblings, sons, and daughters) experience levels of psychological distress that are on par with those of spousal caregivers (Areia, Fonseca, Major, & Relvas, 2019; Segrin & Badger, 2010).
Providing care to a spouse/intimate partner or aging parent may be more normatively prescribed, whereas caring for a sibling or cousin may be driven more by the closeness of the relationship. Similarly, social network members and even health care providers may be more forthcoming with social support to spousal caregivers than to friends who function as fictive kin and are often overlooked and poorly understood in their role as caregivers to Latinas with breast cancer. At the same time, providing care to a spouse may be more emotionally and physically exhausting than providing care to a cousin, for example, due to the intensity of the relationship. Providing care to an adult child with cancer may also be emotionally taxing when the child’s mortality is perceived to be at risk. Such dynamics could have significant implications for caregivers’ well-being (Villalobos & Bridges, 2016). Latino families provide a useful context for the study of family caregiving by different relationship types due to their emphasis on family values that prescribe a strong commitment to care for family members in need, which reaches across generations and beyond to extended family and fictive kin (Juarez, Branin, & Rosales, 2014).
There is some evidence to suggest that low acculturation, which is the level of adoption of preferences and practices indicative of U.S. cultural customs, is a risk factor for compromised quality of life among Latino family caregivers in the United States (Meyer, Geller, He, Gonzalez, & Hinton, 2014). Caregivers with low acculturation are likely to have restricted access to information and support services due to linguistic barriers, for example. This could potentially make family caregivers with low acculturation particularly vulnerable to poor quality of life. Acculturation is also a phenomenon that may be differentially distributed over various relationships types with younger generations likely experiencing higher acculturation than older generations.
Purpose of the Study
The present study tests for differences in distress and social support among family caregivers of Latinas with breast cancer as a function of relationship type (e.g., spouse, sibling, and parent). Because of the diverse nature of family caregiver relationships in Latin cultures, we hypothesize that there will be differences in distress and social support as a function of the different caregiver–survivor relationship type. Participants were recruited for involvement in a larger intervention study for Latinas with breast cancer and their family caregivers. However, findings presented in this report are drawn exclusively from baseline assessments, before any interventions commenced, allowing for a snapshot of caregivers’ well-being as they presented for enrollment in the study.
Method
Participants
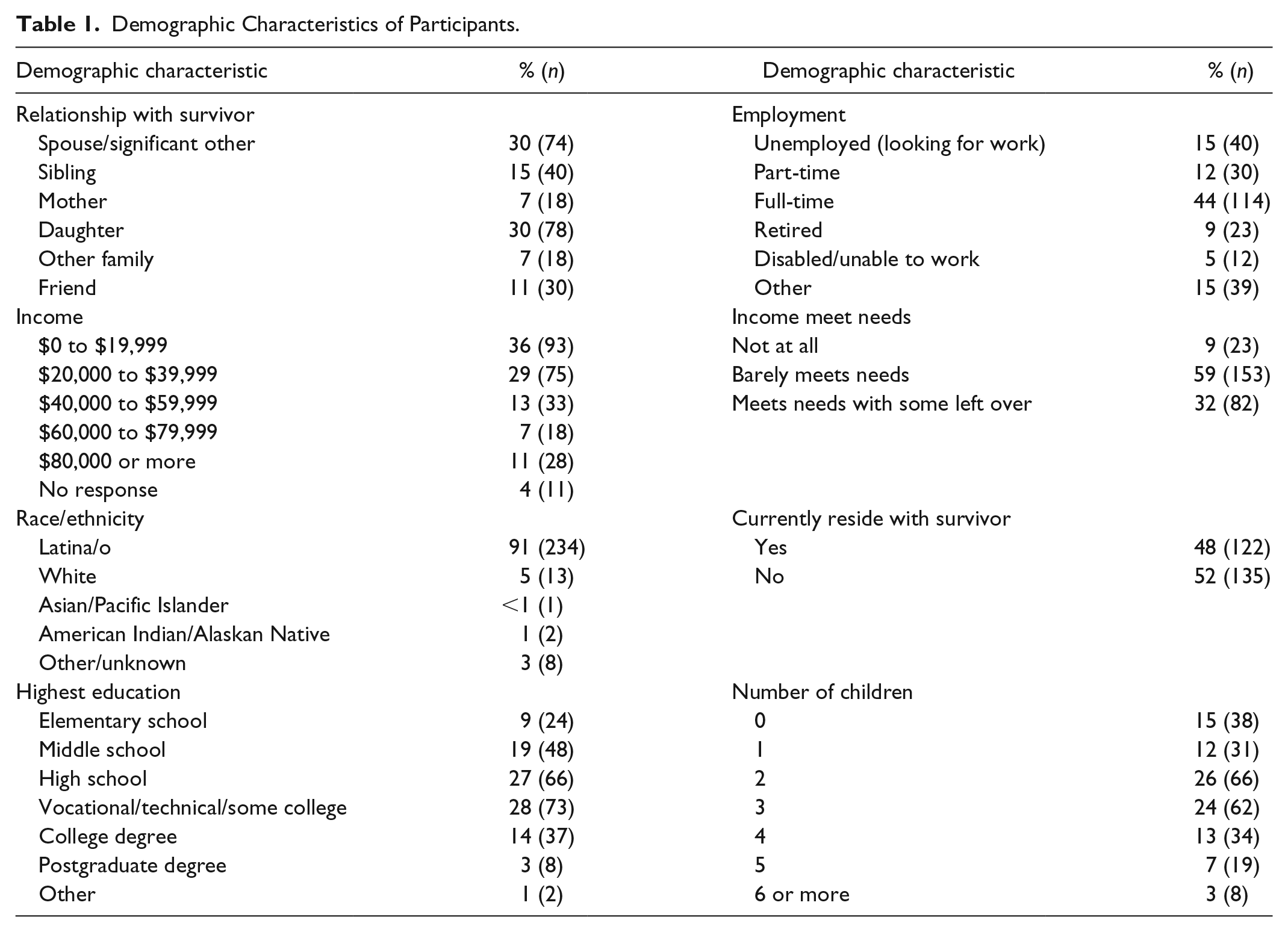
Participants in this study were 258 family caregivers of Latinas who were either in treatment or who had completed treatment for breast cancer within the past year. The sample of family caregivers was 32% male and 68% female with a mean age of 44.05 yeas (SD = 13.60, range: 21-82). The Latinas with breast cancer who they were caring for had a mean age of 50.55 years (SD = 10.38). The disease progression of Latinas with breast cancer was Stage 0 (1%), Stage 1 (17%), Stage 2 (32%), Stage 3 (26%), and Stage 4 (11%), for those who knew their stage. Their treatments (current or recently competed) included chemotherapy (81%), surgery (60%), radiation (27%), and hormone blocking (14%). Further demographic information for participants appears in Table 1.
Demographic Characteristics of Participants.
Procedure
The sample was a convenience sample of people who agreed to participate in a trial of supportive care interventions. Baseline data collected prior to delivery of any interventions were used in this secondary analysis. Family caregivers were recruited into this study by nomination from a Latina with breast cancer who was either actively in treatment or who had completed treatment within the past year. Both provided informed consent individually before participating in the study. Reasons provided by Latinas with breast cancer for selecting their particular family caregiver have been published elsewhere (Badger et al., 2017). Inclusion criteria for caregivers were aged 18 years or older, designated by the Latina with breast cancer, and having access to a telephone, as the dyads were participating in a larger study of telephone-delivered psychosocial interventions for Latinas with breast cancer and their family caregivers (Badger, Segrin, et al., 2019). Trained data collectors contacted family caregivers over the telephone and read the items on the instruments in either English or Spanish, according to the caregiver’s preference. Participants received gift cards to a national retail store to compensate them for their time to participate in the study. The study was approved by the University of Arizona Institutional Review Board (Protocol 1100000136).
Measures
Distress
Psychological distress was assessed with the PROMIS (Patient-Reported Outcomes Measurement Information System) depression, anxiety, and fatigue scales (Pilkonis et al., 2011; Teresi, Ocepek-Welikson, Kleinman, Ramirez, & Kim, 2016). Each scale was composed of eight items that assess frequency of experiencing different symptoms of the construct over the past 7 days (e.g., “I felt worthless,” “I felt nervous,” and “I have trouble starting things because I am tired”) on a 5-point scale ranging from never to always. PROMIS measures are scored on the T-metric, with a general U.S. population mean of 50 and standard deviation of 10. Higher T-scores indicate greater depression, anxiety, or fatigue. Reliability coefficients for the PROMIS measures were α = .92, .92, and .95 for depression, anxiety, and fatigue, respectively.
Social Support
Social support was measured with the PROMIS-informational support and emotional support subscales (Hahn et al., 2010; Hahn et al., 2014). The informational support (e.g., “I have someone to give me information if I need it”) and emotional support (e.g., “I have someone to confide in or talk to about myself or my problems”) scales each contain eight items to which participants respond on a 5-point scale ranging from never to always. The social support scales are also represented as T-scores with higher scores indicating more frequent availability of informational and emotional support. The reliability of these measures was α = .94 for informational support and α = .95 for emotional support.
Acculturation
The seven-item U.S. orientation subscale of the Acculturation Rating Scale for Mexican Americans–II (Cuellar, Arnold, & Maldonado, 1995) was administered to assess the extent to which participants embraced preferences and practices indicative of U.S. cultural customs (e.g., “I speak English,” and “My friends now are Anglo-American”). Response options ranged from not at all to almost always on a 5-point scale. Internal consistency reliability was α = .92.
Data Analysis
Distributions of the distress and social support outcomes were assessed, including examination of the variances which did not vary by relationship status between caregivers and patients. Hypotheses about differences in distress or social support as a function of relationship status between caregivers and patients were evaluated with a series of analyses of variance (ANOVAs). In addition to the p values, effect sizes expressed as η2 are reported. Conventions for interpretation of η2 specify .01, .06, and .14 as small, medium, and large effects, respectively (Cohen, 1977). Instances of statistically significant ANOVA models were followed by exploratory post hoc pairwise comparisons which identify specific differences among caregiver means. Because of the exploratory nature of these pairwise comparisons, and lack of a priori predictions about specific group differences, these tests were conducted in two phases. In the first phase, pairwise comparisons were made without controlling for the outcome-level error rate set at .05 using Tukey–Kramer tests. In the second phase, the Benjamini–Hochberg adjustment was used to control the false discovery rate at the level of each outcome (Benjamini & Hochberg, 1995; Thissen, Steinberg, & Kuang, 2002). Collectively the post hoc tests reveal which pairwise comparisons were significant at the .05 level and which of those remained significant when controlling the false discovery rate. With the size of this sample, an ANOVA model comparing means from six groups has power = .64 to detect a small effect of η2 = .01 (f = .10) and power = .93 to detect a medium sized effect of η2 = .06 (f = .15). Associations between acculturation, distress, and social support were assessed by Pearson correlations. Finally, several post hoc analysis of covariance (ANCOVA) models were conducted to test for differences in distress or social support while controlling for acculturation.
Results
Means and standard deviations of all major study variables appear in Table 2. The data file generated by this sample had 8% missing values and these were exclusively from the fatigue and acculturation variables. The pattern of these values was missing completely at random as determined by Little’s MCAR test, χ2 = 24.08, degrees of freedom = 20, p = .239. Therefore, for analyses involving the fatigue and acculturation variables, a multiple imputation procedure with fully conditional specification, using predictive mean matching, was used to generate 10 data files with imputed values. Pooled results based on the multiple imputations are presented for all analyses involving fatigue and acculturation.
Means and Standard Deviations for Major Study Variables.
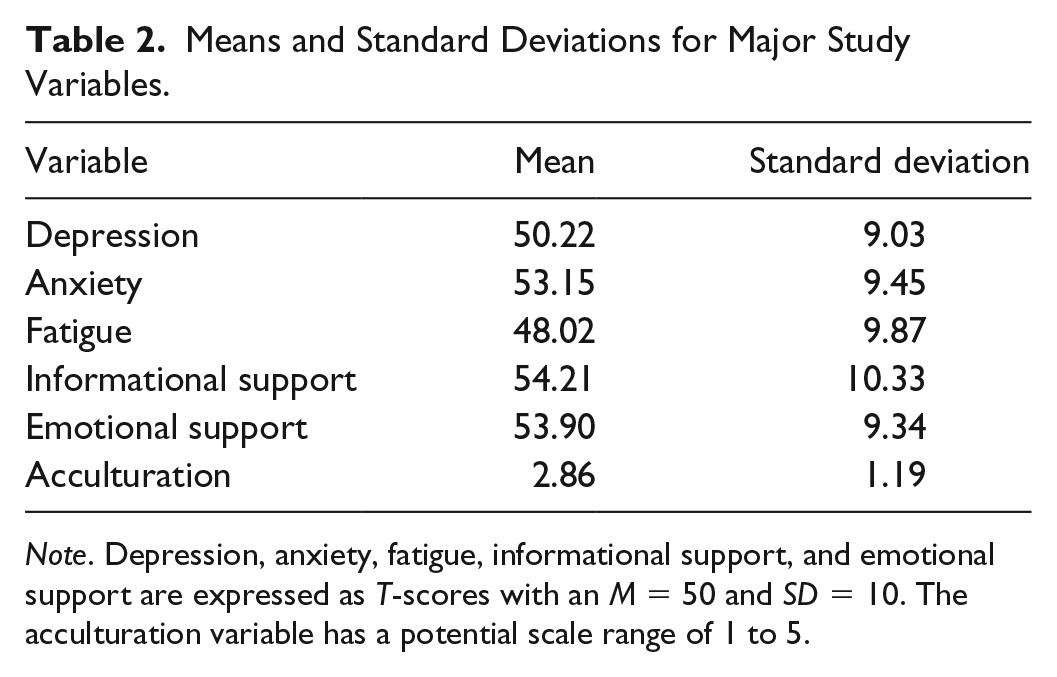
Note. Depression, anxiety, fatigue, informational support, and emotional support are expressed as T-scores with an M = 50 and SD = 10. The acculturation variable has a potential scale range of 1 to 5.
The first set of analyses tested for group differences in each of three indicators of distress: depression, anxiety, and fatigue. There were significant differences for depression, F(5, 251) = 3.57, p = .004, η2 = .07 and fatigue, F(4.19, 202.68) = 2.40, p = .049, η2 = .05. The differences in anxiety, F(5, 251) = 2.13, p = .062 did not reach statistical significance with η2 = .04. The second set of analyses tested for group differences in the two indicators of social support: informational and emotional. For these tests, there were statistically significant group differences in informational support, F(5, 251) = 2.78, p = .018, η2 = .05, but no significant differences in emotional support, F(5, 251) = 1.03, p = .403, η2 = .02. Results of pairwise comparisons of group means appear in Table 3. The results in Table 3 show that mothers differed significantly from at least three of the other groups on depression, anxiety, fatigue, information support, and acculturation.
Means (Standard Errors) and Pairwise Comparisons for Relationship Types.
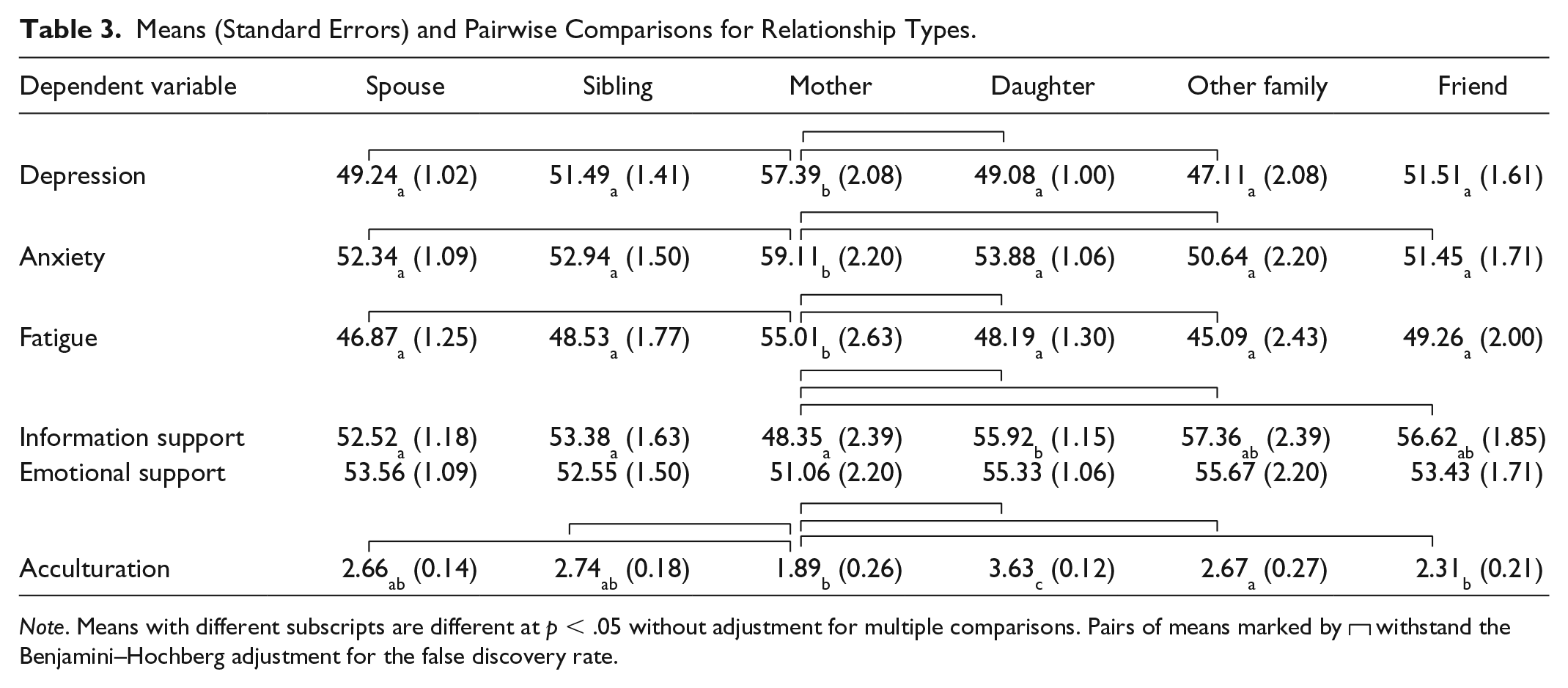
Note. Means with different subscripts are different at p < .05 without adjustment for multiple comparisons. Pairs of means marked by withstand the Benjamini–Hochberg adjustment for the false discovery rate.
Acculturation was significantly associated with relationship status, F(4.97, 238.21) = 13.31, p < .001 (see Table 3 for means). Acculturation was also significantly correlated with depression, r(256) = −.16, p = .015 and with informational support, r(256) = .22, p = .001. It is clear from Table 3 that mothers had the lowest level of acculturation and information support, and the highest levels of distress of any of the caregiver groups. Therefore, a series of post hoc ANCOVAs controlling for acculturation was conducted based on those ANOVAs that previously revealed statistically significant differences by group. Controlling for acculturation, the previously significant differences among caregiver groups were still statistically significant for depression, F(4.95, 250.67) = 2.70, p = .022, η2 = .05 but not fatigue, F(4.21, 200.77) = 2.21, p = .065, η2 = .04. The previous nonsignificant (p = .062) effect for anxiety, remained the same when controlling for acculturation, F(4.99, 250.10) = 2.16, p = .059, η2 = .04. Finally, the previously significant group differences for information support were no longer statistically significant when controlling for acculturation, F(4.96, 248.90) = 2.05, p = .072, η2 = .04.
Discussion
In the present study, differences in family caregivers’ distress and available social support were examined as a function of relationship status between the caregiver and the Latina with breast cancer. The results revealed a clear and consistent pattern whereby mothers had the highest distress and the lowest available social support, although these differences were not always statistically significant. Caregivers who were mothers also had the lowest level of acculturation. Post hoc ANCOVAs indicated that at least some of the association between motherhood and greater distress and lower support could be attributed to lower acculturation, especially when considering informational support. It may be that mothers were unable to access the information they needed to care for the Latinas with breast cancer due to multiple barriers (e.g., linguistic, education, and financial).
Family members who provide informal care for cancer survivors face significant risk of psychiatric morbidity (Bambauer et al., 2006; Kim & Given, 2008). Latin sociocultural values are likely to compel a diverse range of family members into this role. Indeed, the family caregiver participants in this study included spouses, daughters, mothers, siblings, and a range of other family and fictive kin. Even among those Latinas with breast cancer who were married, close to 60% nominated some other family member as their primary caregiver. The results of this study show that most of the different caregivers had levels of depression and fatigue that were at or below population norms (i.e., M = 50). However, the means for anxiety were higher than population norms for all caregiver groups. More prominently, mothers appeared to be at particular risk for psychological distress compared with other family caregivers. Just as mothers caring for pediatric cancer patients experience significant distress (Sulkers et al., 2015), providing care to an adult child with cancer is also psychologically taxing. In both cases, having a young or even middle-aged child with a life-threatening illness may be especially stressful, and certainly counter normative to a parent.
This study identified what may be a somewhat unique complicating factor for family caregivers of Latinas with breast cancer. The mothers in this study had lower acculturation than any of the other type of family caregiver. Low acculturation is a risk factor for compromised quality of life in Latino and Latina family caregivers (Meyer et al., 2014). People with low acculturation have less access to resources, particularly informational (Becerra, Androff, Messing, Castillo, & Cimino, 2015), due to linguistic barriers and may also have less access to educational and financial resources (Buscemi, Williams, Tappen, & Blais, 2012). Part of the reason why mothers may have experienced more distress and lower informational support is because of their lower acculturation level. Mothers represent an older generation who are more likely to have been born and raised in another country and who are still struggling to acclimate to life in a new country. These are taxing background circumstances for a family member who is taking on the task of providing care to an adult daughter with breast cancer.
It is perhaps understandable that the family caregivers with the lowest informational support (mothers) had the highest anxiety and depression. Informational support can decrease the risk of experiencing anxiety and depression in the context of cancer care (Faller, Strahl, Richard, Niehues, & Meng, 2017). In some cases, caregivers may experience elevated distress even though the cancer survivor with early stage disease has a positive prognosis, but the caregiver does not fully comprehend this due to unmet information needs. In other cases, unmet informational support may deprive family caregivers of other health care system and community services that may be available to them and the cancer survivor, again allowing distress and exhaustion to go unchecked (Wang, Molassiotis, Chung, & Tan, 2018). Anxiety and depression often exacerbate fatigue (Bonhof et al., 2019), which was also noticeably higher in mothers compared with other caregiver types. These and other possibilities highlight the importance of providing culturally and linguistically competent informational resources to family caregivers who may not be as acculturated as younger family members.
Traditionally, the family caregiving literature has been heavily focused on the role of spouses as caregivers. This is likely due to the fact that cancer is often a disease of advanced age and spouses are ordinarily the first line of support in times of need. However, the results of this investigation raise questions about whether spouses represent a unique population, at least in terms of their psychological distress and available social support in the context of caring for a family member with cancer. Aside from their differences from mothers, who stood out as a unique group in this sample, spouses’ levels of depression, anxiety, and fatigue were on par with those of daughters, siblings, and even more extended family such as those in the “other family” or “friends” category. That, coupled with the fact that 70% of the family caregivers nominated by Latinas with breast cancer were nonspouses, perhaps argues for expanding the focus of family caregiver research to include a wider range of caregivers, especially when working with Latinas and Latinos.
Limitations
There are a number of limitations of this study that must be considered when interpreting its findings. First, the sample of mothers in this study was very small and these findings would need to be replicated on a larger sample of mothers to have confidence in their at-risk status as family caregivers. Second, caregiver demographics, often by definition, are not randomly distributed across family caregiver types. For example, all of the spousal family caregivers in this study were men, but there were very few men in any of the other family caregiver relationship categories, sometimes by definition (e.g., mother and daughter). Consequently, it is difficult to make inferences about distress and available support for male caregivers other than those who are spouses. Third, the cross-sectional nature of these data make it impossible to determine if caregiver distress levels represent a response to the cancer diagnosis and treatment of the person with breast cancer, or if they represent coincidental features of the psychological landscape of people who are otherwise living under challenging conditions. Fourth, data were collected exclusively via self-report from a survey. Reporting biases could potentially influence participants’ responses, especially in the case of caregivers who want to appear strong or Latina participants who value marianismo and may be reluctant to fully report on their level of distress. Finally, Latinas with breast cancer in this study were required to identify a caregiver who could also participate with them in the larger study. This could have placed restrictions on the inclusion of certain caregivers, thus limiting the generalizability of these findings.
Implications for Nursing Practice
These findings have implications for nursing practice with caregivers caring for Latina/o cancer survivors. Although there are norms and values that define any cultural group, individual variations exist requiring that nurses assess these norms and values to avoid stereotyping (Badger, Sikorskii, et al., 2019). Nurses can develop a relationship (becoming a trusted person) with cancer survivors’ designated caregivers to capitalize on the key strengths of their relationship and facilitate gaps in learning for caregivers to promote their own and the survivors’ well-being. For example, where there is a great deal of trust and respect in the cancer survivor–caregiver relationship, nurses may be able to work through the caregiver to effect adherence to treatment protocols, recommended lifestyle changes, and so on, in the cancer survivor. Assessing each cancer survivor and caregiver dyad will allow nurses to be better able to understand the family dynamics, include key decision makers within the Hispanic family, and provide quality care (Caplan & Whittemore, 2013). Psychosocial support interventions that recognize the uniqueness of the Latin family and address access barriers for individual families (e.g., linguistic, financial, and alternatives to face-to-face psychosocial care delivery) will likely be the most successful in providing the informational and emotional support needed to facilitate well-being. This may be especially important with mothers providing care for their adult child with cancer.
In conclusion, the results of this study suggest that mothers caring for an adult child with cancer may be particularly vulnerable to psychological distress, fatigue, and unmet informational support needs. Owing to their older age compared with other family caregivers (e.g., daughters), mothers of Latinas with breast cancer appear to have lower acculturation, and this explains some of the variation in their distress and lower informational support. Latinas with breast cancer appear to receive informal care from a diverse range of family and fictive kin who are essentially comparable in their experience of distress and available social support, with the exception of mothers who may represent a population worthy of special attention in both clinical and research contexts.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by funding provided by the American Cancer Society (RSG-12-120-01-CPPB) to Terry Badger.