
Abstract
Sickle cell disease (SCD) is a chronic illness characterized by pain and progressive organ damage resulting from abnormal hemoglobin molecules that distort red blood cells into a sickle shape (Ballas, Gupta, & Adams-Graves, 2012; Olowoyeye & Okwundu, 2014). In the United States, SCD is the most common inherited blood disorder with at least 100,000 individuals affected (Centers for Disease Control and Prevention, 2019). SCD is most prevalent among individuals of African ancestry as the disease occurs in one of every 365 African American births (Centers for Disease Control and Prevention, 2019). Due to advances in disease management, mortality rates in childhood have decreased. Young adulthood has become a vulnerable time in which individuals with SCD have increases in medical complications, morbidity, and early mortality (Hamideh & Alvarez, 2013; Minniti & Vichinsky, 2017; Quinn, Rogers, McCavit, & Buchanan, 2010).
Young adults (YA), aged 18 to 25 years, typically experience a health care transition (Arnett, 2000; Berens, Jan, Szalda, & Hanna, 2017; Lanzkron et al., 2018). Health care transition is particularly challenging for YA living with SCD as they experience frequent pain episodes, high health care utilization, and high rehospitalizations often related to pain management (Debaun & Telfair, 2012; Jenerette, Brewer, Crandall, & Ataga, 2012; McPherson, Thaniel, & Minniti, 2009; Sobota, Neufeld, Sprinz, & Heeney, 2011; Treadwell et al., 2016).
For YA with SCD, medical challenges encountered during health care transition are further compounded by various sociological and economic challenges. As YA move from a typically nurturing pediatric health care environment, they experience the daunting task of learning how to balance daily responsibilities with self-management as they attempt to navigate the adult health care system (Matthie, Hamilton, Wells, & Jenerette, 2015; McClish et al., 2017). They often lack knowledge about the adult SCD care system, have limited decision-making experience, and have had a change in, or loss of, insurance (Asnani, Barton-Gooden, Grindley, & Knight-Madden, 2017).
To help address treatment gaps for YA with SCD, the Association of Pediatric Hematology/Oncology Nurses and the American Society of Pediatric Hematology Oncology recommended that pediatric patients with SCD receive early preparation for transitioning to the adult health care system (Bryant, Porter, & Sobota, 2015). Despite the recommendations of these groups and others, YA with SCD encounter multidimensional barriers to optimal transition. Despite the recommendations of these groups and others, EA with SCD encounter multidimensional barriers to transition (Smith et al., 2019). These barriers include SCD-related complications (Crosby, Quinn, & Kalinyak, 2015), concerns regarding leaving pediatric providers and adult provider knowledge of and ability to manage SCD care (Allemang et al., 2019; Berens et al., 2017; Porter, Graff, Lopez, & Hankins, 2014), access to a transition program and distance from home to an adult SCD center (Andemariam et al., 2014), low health literacy, and lack of knowledge regarding the transition process (Asnani et al., 2017; Stollon et al., 2015). Additional barriers include inadequate insurance coverage and reimbursement difficulties, policies regarding prescription pain medications (Bemrich-Stolz, Halanych, Howard, Hilliard, & Lebensburger, 2015; Mulchan, Valenzuela, Crosby, & Sang, 2016; Treadwell, Telfair, Gibson, Johnson, & Osunkwo, 2011), negative perceptions of SCD among some adult providers, and stigmatization as being drug seekers (Porter, Wesley, Zhao, Rupff, & Hankins, 2017; Sobota, Umeh, & Mack, 2015). All these issues can result in YA avoidance of necessary health care or lack of appropriate health care and contribute to poor health outcomes.
Currently, with young adulthood being a time of increased vulnerability to morbidity and mortality despite advances in medical care, there is an urgent need to identify barriers that are impeding the health of YAs living with SCD. Within a transcultural nursing approach, it is understood that the cultural contexts in which individuals live, influence their health-related values, attitudes, beliefs, and practices (Andrews & Boyle, 2019). A range of factors contribute to cultural contexts, including environmental, social, economic, religious, philosophical, moral, legal, political, educational, biological, lifestyle, and technological (Andrews & Boyle, 2019). The physical location of where one lives matters; for instance, urban living can affect health because of the physical and social environments and the availability of, and access to, health and social services (Galea & Vlahov, 2005). This study was conducted to explore how contextual factors influenced health care transition experiences for YA living with SCD. Consideration of contextual factors that affect YA during the critical health care transition period will allow for intervention development to address their complex needs (Braun & Clarke, 2008; Neergaard, Olesen, Andersen, & Sondergaard, 2009).
Method
Research questions for this study include the following: What are the social and psychological factors associated with the perception of healthcare transition for YA living with SCD? What factors influence the experience of YA during healthcare transition? How have interactions with nurses and other health care providers influenced health care transition?
Research Design
A qualitative descriptive design was used. This design was used to obtain a description of the health care transition phenomena for YA living with SCD from their own perspectives.
Recruitment
After obtaining study approval from the institutional review board (IRB), participants were recruited from an SCD adult comprehensive center located in a Midwestern city in the United States. This city is highly segregated by race and ethnicity and high rates of poverty exist. A purposive, convenience sampling approach was used to recruit 10 to 20 YA. Eligibility criteria for participation were as follows: (1) diagnosis of SCD, (2) ability to understand English, (3) aged 19 to 25 years, and (4) completed health care transition. For this study, the age range of 19 to 25 years was selected because most teens have transitioned from pediatric to adult care by the age of 19 years. Twenty participants were recruited; however, the principal investigator (PI) experienced difficulty in contacting some participants to schedule an interview. Therefore, 13 YA participated in the study. The PI conducted individual 45-minute interviews in a private room at the clinic site, in a private room at a library, or at the participant’s home. The interview location of the interview was mutually decided by the participant and the PI. Interviews were completed once saturation was reached.
Data Collection
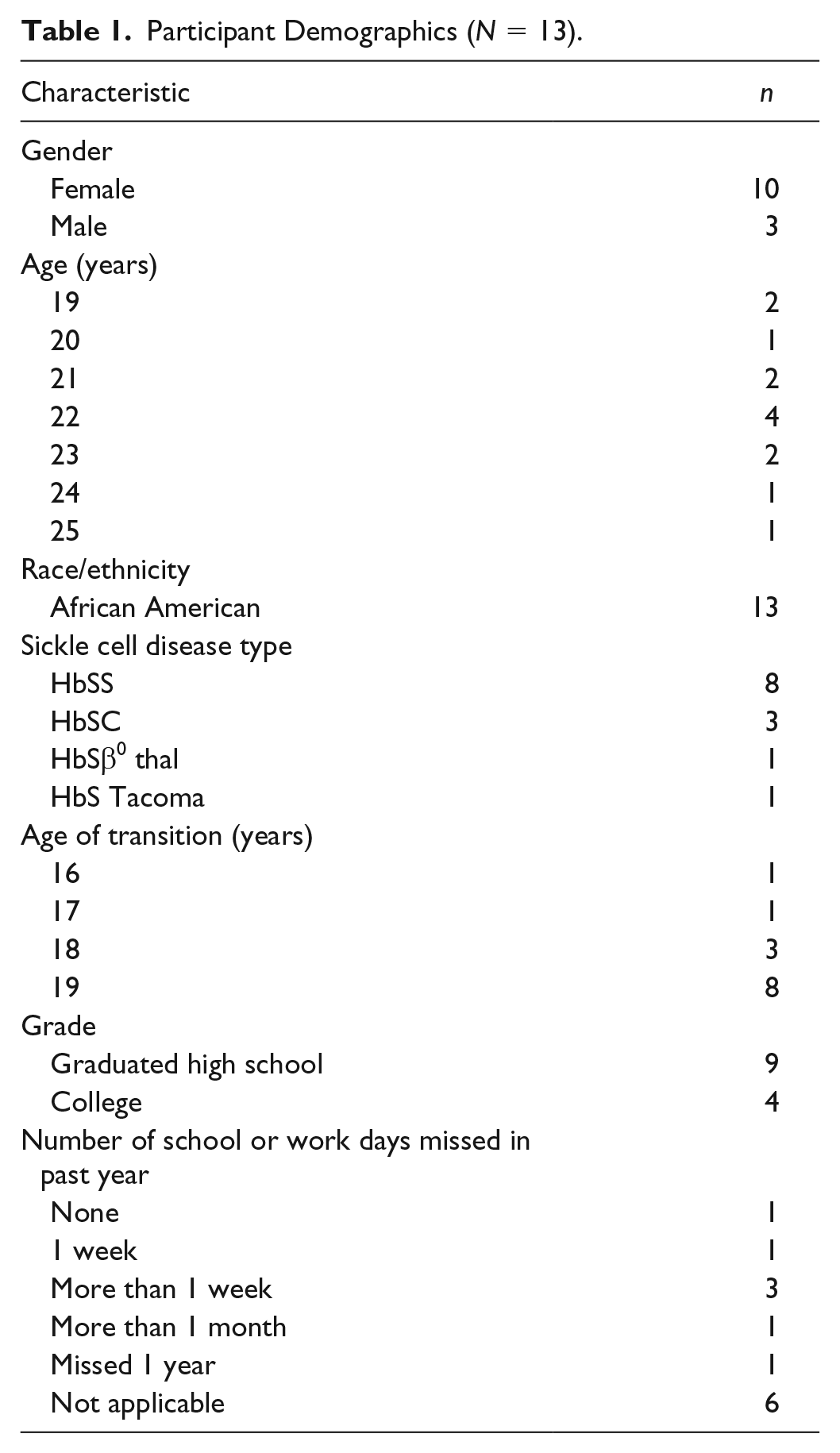
After obtaining written informed consent, data were collected via a demographic survey and semistructured interviews. The demographic survey was designed to request information regarding the participants’ age, gender, ethnicity, education, and questions related to SCD, such as vaso-occlusive crises, hospitalizations, and history of surgeries (see Tables 1 and 2). An interview guide, consisting of 16 open-ended questions accompanied by probes, was used to conduct in-depth semistructured interviews (see Table 3). Questions were designed to elicit information from participants regarding their experiences prior to and after transitioning from pediatric to adult health care. Additional information was related to social support (peers, family, and others), stigma, and well-being. The duration of the interviews was approximately 45 minutes. Most of the interviews (n = 10) were conducted in the participant’s home or in the community. On completion of the interview, participants received a US$30 gift card.
Participant Demographics (N = 13).
Participant Medical Information (N = 13).
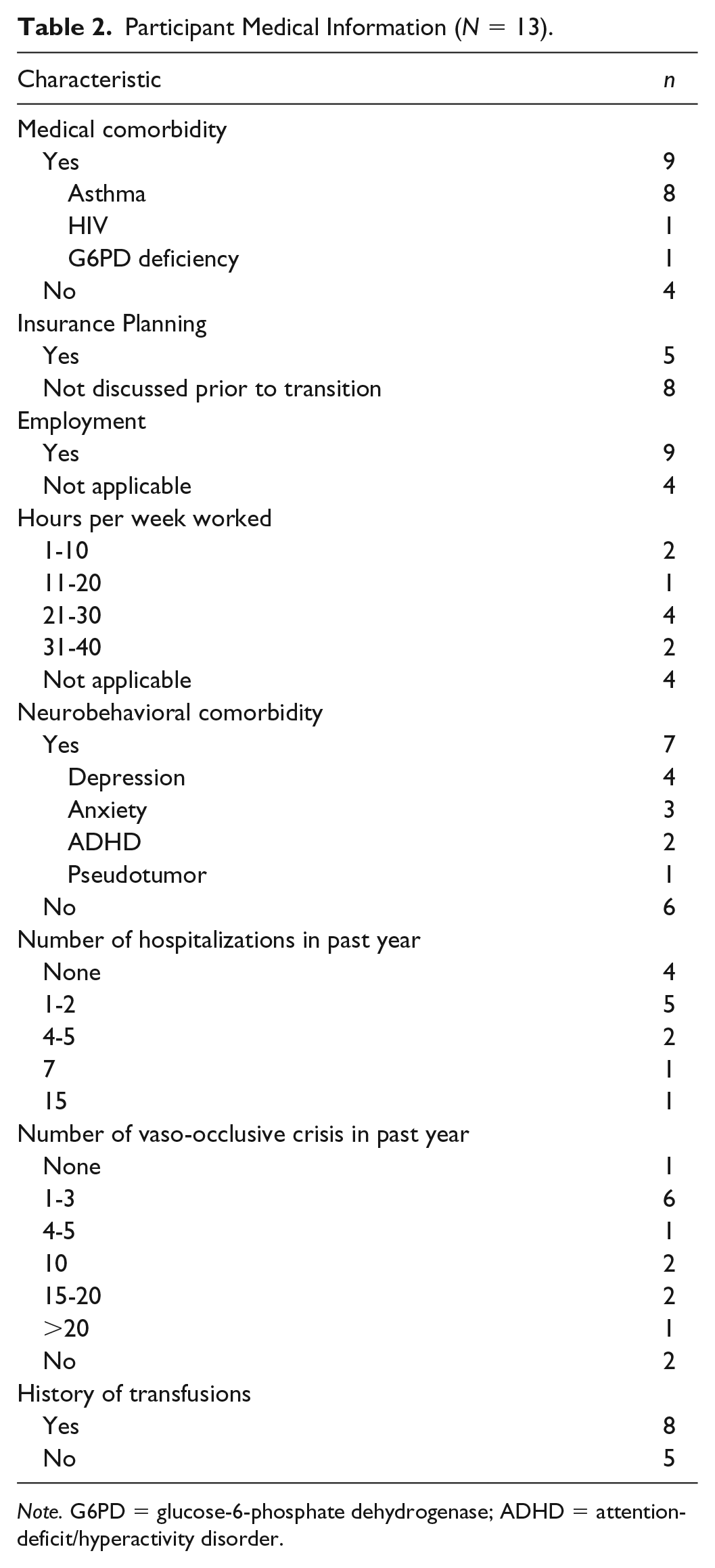
Note. G6PD = glucose-6-phosphate dehydrogenase; ADHD = attention-deficit/hyperactivity disorder.
Interview Guide.
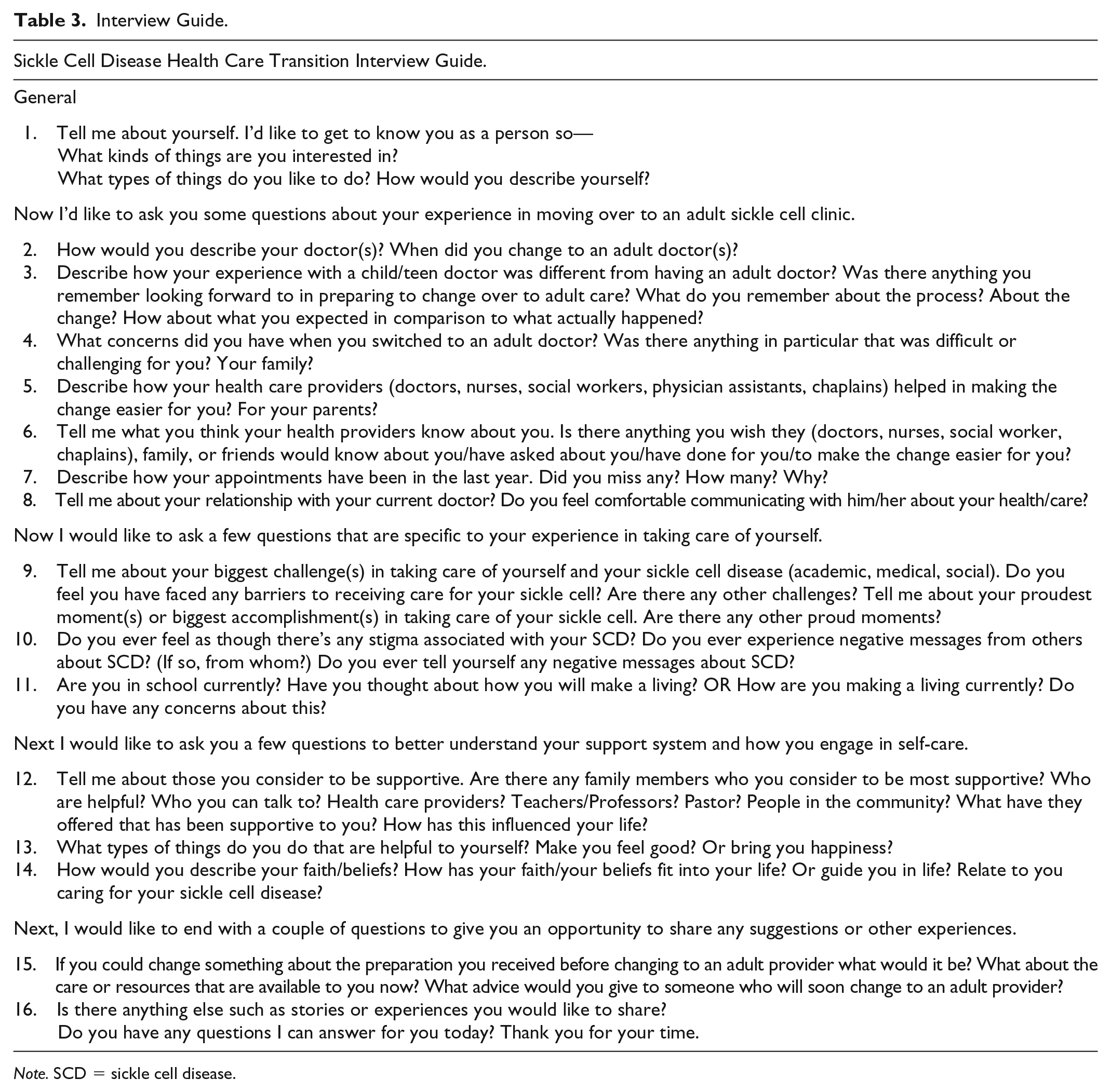
Note. SCD = sickle cell disease.
Data Analysis
Participants’ interviews were digitally audio-recorded and transcribed verbatim by a professional transcriptionist. Accuracy of the transcription was checked against the original digital recording by the PI or research assistant. The interview for the first participant was coded, and a template was created that consisted of eight codes. Another researcher independently coded the same transcript using the coding template. Interrater reliability for coding by the two researchers was approximately 90%. A final coding scheme was used to code the remaining transcripts. The code summaries were used to perform a thematic analysis to look within and across codes for relationships and patterns to evaluate for themes.
Results
Thirteen participants ranged in age from 19 to 25 years (M = 21.5 years, SD = 1.73). Ten were male and three were female. All participants reported their ethnicity as African American. Four participants attended college, three participants worked 20 hours per week or fewer, six participants worked 21 to 40 hours per week, and four participants did not work. The hemoglobinopathy type for eight participants was hemoglobin SS (HbSS), three had hemoglobin SC (HbSC), one had hemoglobin S beta-zero thalassemia (HbSβ0 thal), and one had hemoglobin S Tacoma (HbS Tacoma). The age range that participants transitioned from pediatric to adult care was 16 to 19 years. The usual age for participants to transition was 19 years. Some transitioned prior to 19 years, but the participants did not always know the reasons.
All participants completed one semistructured interview. Eight major themes emerged from the data analysis: (1) need for accessible support (peer support and community support); (2) early assistance with goal setting; (3) incongruence among expectations, preparation, and experiences; (4) spiritual distress; (5) stigma (general and internal); (6) need for greater collaboration; (7) appreciation for caring providers; and (8) isolation.
Need for Accessible Support
Participants described their need for support as they coped with health care transition. The first subtheme was desire for consistent peer support. For the second subtheme, YA verbalized the importance of community-based support.
Desire for Consistent Peer Support
While most of the YA shared that family provided a strong sense of support, some indicated that they did not have a best friend or close friend with whom they could talk with or share their concerns. YA expressed the need to feel supported by their peers. Many felt that if they had more support early on, then it could have made a difference in their lives today. A 21-year-old female shared how difficult it was to build relationships with peers during childhood and adolescence because of her peers’ lack of awareness about SCD.
Oh, will I catch that [SCD]? We can’t be friends anymore. I don’t know what that is. Is it contractible, how do you get it? And I’m like I’m born with it, and I had to explain everything, so I just stopped making friends.
Community Support
Most of the participants were aware of the monthly support group meetings hosted by one hospital but faced challenges that prevented them from attending the meetings. Most shared that they had not participated in the past because of the inconvenience of traveling to the meeting location, a schedule conflict, forgetting about the meeting time, or just not feeling like attending. They verbalized that they wanted the support, but their challenges appeared to be a competing force for them attending. A 20-year-old commenting on the existing support group and meeting said, “It’s hard getting to support group meetings. I work during the day and my body is just too tired at the end of the day to add another thing. I could really use the help now.”
Early Assistance With Goal Setting
YA verbalized how they wanted to set goals that were realistic and that were not always related to their SCD. A 22-year-old female described how she prefers to be asked about her plans for the future and for nurses and other health care providers to initiate the discussion: I guess my biggest thing is that I want to know, I want someone to talk to me about what happens long term without . . . I don’t know. It feels as if we’re just expected to live as long as we can with the pain meds and just die off, if that makes sense.
YA expressed that their personal goals related to college, career, and family planning should be assessed by their nurses and other health care providers prior to, and after, their health care transition and periodically throughout their care. This was believed to enhance the patient–provider relationship and goal congruency as well as enhance their overall quality of life. YA expressed how they believed that potential options were not always presented, because maybe nurses and other health care providers felt it may add stress to their lives or lead to complications. They commented on how they wanted the potential for positive or negative outcomes for their choices to be shared, and that in the end, they want to exercise their decision regarding their care and their future.
Incongruence Among Expectations, Preparation, and Experiences
YA shared that what they expected during the health care transition process was not what they experienced. In some instances, this was a result of YA having their personal ideas and views about what would happen in a different health care environment. YA admitted that they may not have had a realistic view of what the actual health care transition process would be like. Some held the belief that they would have greater independence and that they were ready for this next stage. Some of the YA shared that they may not have been optimally prepared by their parents or nurses and other health care providers for what was to come. They expressed that the preparation period appeared to be brief when compared with the significantly increased level of responsibility that is required as an adult who has moved over to adult care. Some felt that information came too late. They received information for self-management skills at age 18 to 19 years during transition, although they felt that they had been ready for this information at younger ages. Many of the YA felt that everyone comes from different circumstances and that the approach would likely need to be customized for each person with some standards in place. A 19-year-old female shared her encounter with transitioning to adult care: I guess when I first came back to the clinic, when I was 18 and they were like no you can’t be here anymore, because you’re older now you’ve got to go over to . . . They just sent me away, they could have talked to me and explained this is the day you’re leaving. They could have explained.
A 23-year-old described his experience after moving over to adult care and not feeling as if he was aware of or prepared for the changes: “Yeah. It was a lot of different things. The medications, the doctors. They had me on like five different medications when I first got there.”
Spiritual Distress
Participants described experiences when they felt their faith was challenged or their relationship with a Higher Power changed after specific life events. A 23-year-old male shared that at one point he attended church almost weekly but he felt that there was no longer anything for him at this particular church, stating, “I used to have somebody, but I’m no longer at their church.” A 22-year-old female shared some of her life experiences in living with SCD as well as her personal experiences with loss, and how all of the experiences combined have had an impact on her spiritual life: “I feel like I have a love/hate relationship with God to the point where when she [grandmother], died, it stopped me from going to church. I go to church when I feel like it.”
Stigma
YA described their experiences with stigma. Subthemes include general perceived stigma as experienced within the community and with internal stigma imposed on themselves.
General Stigma
While some YA were aware of general stigma, they may have experienced, others were not able to articulate the meaning of stigma. When stigma was defined and described by the PI, most YA were able to identify at least one instance when they experienced general stigma. Examples of stigma that participants experienced included the perceptions of SCD among others in general, attitudes observed of staff in the emergency room, being treated differently than others waiting to be seen in the emergency room, having the label of being a person with a disability by those in the community, and the perception of individuals with SCD among their peers across the life span. A 22-year-old female reflected on her school experiences: Yeah. I feel like some people think sickle cell is a disease that you can contract with each other. I feel like when I was in school people used to talk about me because I’ve had an IEP [Individualized Education Plan] or because I never used to be in school because I was sick, or they didn’t really know so it was like I cried about it most of the time.
Internal Stigma
YA indicated that they often told themselves negative messages as it related to the prognosis of living with SCD, accomplishing specific goals, and expressing a sense of fatalism when considering the challenges they face with their SCD. This was coupled with a lack of opportunities for a young African American adult. A 22-year-old female shared an example of her personal challenge: Sometimes I used to look in the mirror at myself and be like you know you’re ugly; you’re never gonna get well or you’re never gonna be the girl who’s not gonna never be sick; or you’re not smart, you’re just a disappointment. I just thought I was a disappointment to my family, my friends.
Need for Greater Collaboration
While participants respected the knowledge of nurses and other health care providers, in some instances, there was a desire to be asked their opinion more often, even if it was not the best option. A 20-year-old male said, “I didn’t get to request my pain meds. They just assigned them to me. I didn’t get to say what I wanted and what I didn’t want.”
In some instances, participants indicated that asking them to share their desires regarding their future and having discussions about the possibilities was important. They did not claim to know everything and expected their nurses and other health care providers to offer something additional to consider outside of the standard care. According to a 22-year-old female, I want them to discuss; I don’t feel like they discuss with us the possibility of having not necessarily normal lives. I don’t know how they do with others maybe because when I transitioned I was already planning to go to college. I want them to talk about it all.
Participants expressed the need to further discuss certain topics. While they were not necessarily afraid to ask questions, they were aware that nurses and other health care providers may be under a time constraint and not have the capacity to discuss additional topics.
Appreciation for Caring Providers
Participants indicated that overall, they were grateful for having nurses and other health care providers who demonstrated genuine concern and provided good care. Most believed that they could talk with their nurses and other health care providers about anything related to their SCD. This was the case with their pediatric providers, who managed their care prior to health care transition, and their current adult nurses and other health care providers. Some indicated that if time allowed, they could begin discussing other issues that also affect their SCD. A 22-year-old female described her interactions with nurses and other health care providers: “Mainly the nurses because they talk to me, and they see what I’m going through, and they want to help more.”
Feeling Isolated
As mentioned previously, participants expressed a desire for more support from peers and the community. In describing their daily routines, many indicated that they have little time for interacting with current friends, establishing new friendships, and spending quality time with family. A 19-year-old female mentioned that in attempting to live a normal life, she often experienced feeling isolated from others, stating, “I mainly go to work, come home, eat . . .”
A 22-year-old female reflected on an earlier period in her life when she felt connected, during a summer camp spent with other children living with SCD: I met a lot of people that did have SCD, and I made a lot of friends, and it felt like I wasn’t alone; I guess that was another proud moment, plus, I got to go to camp, so I got to roast marshmallows and anything you do while at camp.
Discussion
In this study, YAs described their experiences during the health care transition process in relation to several contextual factors, including social (peer and community support, stigma, collaboration with health care providers), economic (adult employment, health care resources), spiritual, biological (SCD, pain), and lifestyle (self-management). Understanding contextual factors faced by YA is critical to meeting their need for support, as these factors often affect the health care transition process. There is the potential for interruption in establishing or reinforcing self-management behaviors (Berens et al., 2017; Sobota et al., 2015; Treadwell et al., 2016). Assessment of contextual factors that may present as challenges for YA when providing individualized care for those living with SCD is significant. Awareness of cultural contexts will allow nurses and other health care providers to understand their needs and facilitate access of needed resources and support. This will also allow providers to customize the health care transition plan and optimize the transition to adult health care for YA (Treadwell et al., 2016).
Having accessible support was a common desire for all the YAs in this study, but this need was not routinely met. YA described having limited time to establish and build relationships with peers early in life and limited time to currently engage in activities with their peers. Their feelings of fatigue and isolation inhibited their involvement with peers and with SCD support groups. Identifying options to assist YA in attending support group meetings, or to provide support that will allow them to remain in their home, may be ideal (Hsu et al., 2016).
The process of health care transition was discussed and included interactions with caring nurses and other health care providers. YA indicated that their adult sickle cell providers displayed caring behaviors and that this was a strength of their care. They indicated that areas for improvement included greater collaboration between the patient, family members, pediatric providers, and adult providers around the plan and expectations for health care transition.
Communication between nurses and other health care providers and those living with SCD is more likely to be reported as being inadequate (Haywood et al., 2014). While this was not a major finding for the current study, periodically assessing and reassessing goals in specific domains such as vocational and family planning will likely lead to greater overall satisfaction of YA; specifically, patient–provider satisfaction (Schaeuble, Haglund, & Vukovich, 2010).
In this study, most participants were able to identify at least one instance when they experienced general stigma and internal stigma. Encouraging more communication of negative social characterizations related to SCD will increase awareness and may empower YA to engage in critical conversations about stigma (Jenerette, Brewer, Edwards, Mishel, & Gil, 2014). They will be better prepared to develop their capacity to recognize and address incidents of stigma while potentially enhancing their health care transition experiences and outcomes. YA described moments of spiritual distress as well as readiness for enhanced spiritual coping. This further emphasizes the need for psychosocial and spiritual support as needed before, during, and after the critical health care transition period (Clayton-Jones, Haglund, Belknap, Schaefer, & Thompson, 2016). This will likely affect the health care transition experience of YA and their response to those experiences.
Implications for Research and Practice
Results from this study offer insight for improving the health care transition experiences of YA. Consideration of the level of social networks and support from peers, family, and community members is significant when assessing and planning care. While the intersectionality framework was not used throughout the research process for this study, the framework may be useful for research plan development and analysis. An intersectionality framework posits that the experiences of others, YA in this case, are multidimensional and the intersection of age, ethnicity, gender, race, socioeconomic status, current context, and other factors should be considered when conducting research with populations. Future research can be directed toward greater understanding of intersectionality on the health care transition process.
Stigma is a construct that has been presented within sickle cell research literature (Bediako et al., 2016; Ezenwa et al., 2016; Haywood et al., 2014; Jenerette et al., 2012). Future research to understand the social and psychological conditions around general and internal stigma, as well as familial and health care provider influences, is warranted. Interventions to promote awareness of the impact of stigma and methods to support coping for adults living with SCD is warranted.
Less than favorable opportunities to develop relationships with peers, feeling isolated, and experiencing fatigue affect the capacity of those living with SCD to develop relationships across the lifespan. This continues to be critical during late adolescence when social development and serious relationships are significant. Recognizing the challenges and barriers to developing relationships and identifying strategies to address these issues is needed. A program that creates an environment for relationship building could affect self-management behaviors and health care transition outcomes for YA. Identifying mutual goals to facilitate health care transition between pediatric and adult programs further support the overall experiences of YA.
There were a few study limitations. YA participating in this study all had SCD, were African American, and were close in age. They all receive specialized care at an adult comprehensive SCD clinic in a city where high rates of poverty exist. Thus, participants were representative of a fairly homogenous group and findings may not fit other populations of YA living with SCD. The number of participants was small; while they provided detailed and rich data, their experiences represent a small proportion of people with SCD. Future studies are needed with adolescents to compare experiences and better understand the dynamics around health care transition for both adolescents and YA within a similar geographical and socioeconomic setting.
For transcultural nursing, results provide insight into factors that affect health care transition for YA living with SCD and identify their unique health care needs. This knowledge provides leverage in advocating for YA and influencing other nurses and health care providers to deliver meaningful and culturally congruent care. Few studies have focused on developing culturally relevant interventions to promote self-management and transition readiness. These interventions should also include consideration of social and psychological factors that may be unique for YA living with SCD. Attending to the needs of YA around health care transition will not be adequately addressed without being aware of and directing attention to their social, psychological, and cultural contexts.
Footnotes
Acknowledgements
The authors would like to thank the adults who participated in this study and shared their experiences with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this study was provided by Chi Eta Phi Nursing Sorority, Incorporated and the University of Wisconsin-Milwaukee (Harriet H. Werley Research Grant). Research assistance for data analysis and article development was supported by research funds from the Marquette University College of Nursing.