
Abstract
Introduction
In Canada, children of immigrant and refugee families face unique challenges that can affect their mental health, regardless of whether they were born in Canada or themselves arrived as immigrants along with their families. Unlike their nonimmigrant peers, immigrant and refugee youth born outside Canada often experience stress from migration journeys and leaving their home countries, as well as adapting to a new country (Hyman et al., 2000; Islam et al., 2017; Kirmayer et al., 2011; Li et al., 2016; Salami et al., 2019). Canadian census data show 303,257 immigrants and refugees moved to Canada in 2018 and of these, 38,683 settled in Alberta (Statistics Canada, 2018). Children from immigrant families who were born in Canada often also face challenges in belonging (Creese, 2018). Furthermore, many immigrants face a range of barriers to accessing mental health care, from a lack of awareness of services, to socioeconomic conditions and discrimination, to cultural barriers (Reitz & Somerville, 2004; Thomson et al., 2015).
Mental health symptoms are interpreted differently across cultures (Bieda et al., 2017). Many studies have highlighted the role stigma plays in preventing mental health care access (Alaazi et al., 2017; Alaazi et al., 2018; Gary, 2005; Kalich et al., 2016; Shakya et al., 2010; Stol et al., 2015). Notably, numerous barriers can affect children differently than adults; thus, it is imperative that mental health care providers attend to the unique needs of children from immigrant and refugee families and seek to minimize barriers to accessing services.
Several studies have investigated barriers to mental health care faced by immigrant populations (Giacco et al., 2014; O’Mahony & Donnelly, 2007; Salami et al., 2019). However, little analysis exists of barriers faced by immigrant and refugee children specifically. Furthermore, there is little qualitative data about the policy context in Canada. With a focus on Alberta, this study seeks to fill this gap by interviewing immigrant and refugee mothers of children living in Edmonton, Alberta’s capital and second largest populated city. Alberta is an important focus because it is a significant destination province for immigrants in Canada and has the fastest growing population of immigrants. This study seeks to answer the questions: What are the barriers faced by immigrant and refugee mothers in promoting and caring for their children’s mental health and well-being in Alberta? In addition, what facilitates access to mental health services for immigrant children in Alberta?
Theoretical Framework
The study uses a theoretical framework of transnational feminism to understand barriers to mental health care access faced by immigrant families in Canada. Transnational feminism focuses on the movement of capital, labor, and people across international borders, with particular attention to gender implications (Cleland Silva, 2019). We focus on mothers’ perspectives because parenting is often gendered, with women disproportionately responsible for the well-being of their children (Lyonette & Crompton, 2014). Transnational feminism attends to the connections people have to both countries of origin and countries of settlement (Grewal et al., 1999). The framework resists ideas that universalize experiences or processes of oppression and empowerment or flatten differences across individuals’ experiences, as well as cultures and viewpoints (Mohanty, 1988, 2013). Instead, transnational feminism seeks to understand the ways in which people may occupy membership in multiple groups at the same time. These connections to multiple countries and political communities may challenge traditional definitions of citizenship (Faist, 2000).
Method
Design
This is a qualitative descriptive study. Ethics approval was obtained from the University of Alberta Research Ethics Board. Eighteen participants took part in semistructured interviews that included questions such as “What has been your experience with access to mental health services for your child?”; “What are the barriers you faced in accessing mental health care for your children?” and “What makes it easier to access these services?” Researchers sought to understand the barriers facing immigrant and refugee children’s access to mental health care in Canada though narrative and subjective experiences of participants. Qualitative description focuses on what participants say, rather than interrogating narrative for interpretation (Carr, 1994; Colorafi & Evans, 2016; Sandelowski, 2000). The central idea within this approach is that meaning is socially constructed by individual experiences.
Setting/Sample
Participants were recruited by community organizations in Edmonton, Alberta, and all lived in Edmonton. We were connected with 30 potential participants and of those, 18 consented to be part of the study. Inclusion criteria for participation was having immigrated to Canada, self-identifying as a woman, and having children younger than 18 years who live in Canada.
Data Collection
Interviews were conducted by a white female graduate student under close supervision of a doctoral prepared Black African immigrant nurse with extensive experience in research with immigrant populations. On obtaining written consent from participants, interviews lasted approximately 1 hour, and took place in person at a location of the participant’s choosing, usually in their homes or in community spaces such as libraries. Interviews were conducted one-on-one, and in some cases also involved an interpreter. Each participant was interviewed once and data collection concluded when data saturation was reached. Participation was voluntary and kept confidential. The interviewer kept reflexive notes documenting nonverbal communication, her own responses to interviews, and her social positioning in the research process. These added factors provide context to what participants said in the interviews, but which may not be reflected in the transcripts; as well, they are a means to be attentive to interviewers’ social positioning.
In order to further ensure rigor of the study, interviews were audio-recorded, transcribed verbatim, and then read multiple times by researchers to identify key themes. Next, researchers formed a preliminary coding tree, which was used to organize codes and was, in turn, adapted as themes began to emerge. Interview transcripts were then entered into NVivo qualitative software for thematic analysis, a method explained by Braun and Clarke (2014) as a systematic approach by which researchers can code data and then identify patterns across the data that relate to the research question. One researcher coded the data. In addition to exercising reflexivity to improve the credibility of our findings and providing thick description to ensure transferability, we maintained an audit trail of our research process to enhance dependability and confirmability of our findings.
Results
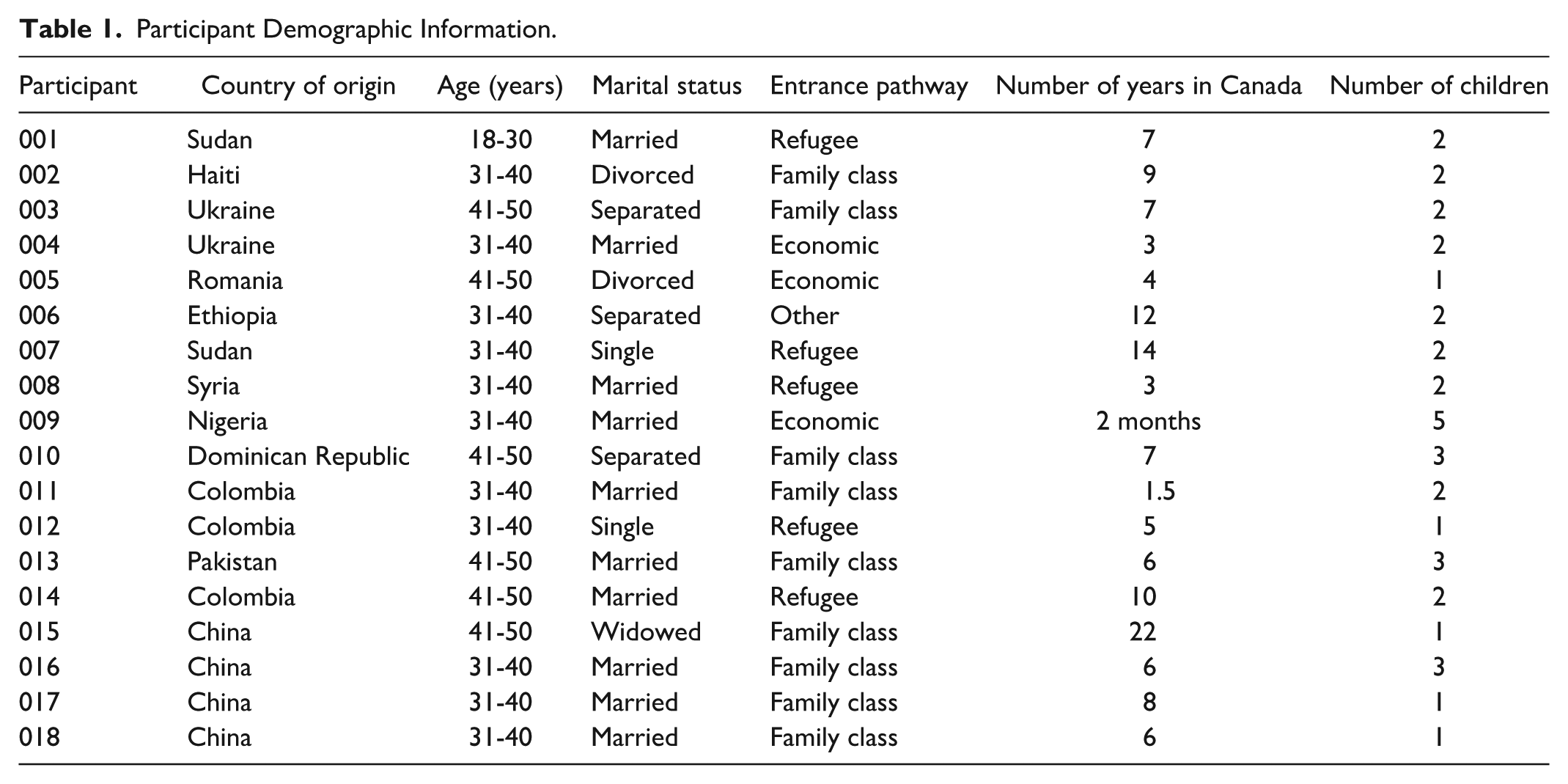
Most of the interviewees (14) had some level of postsecondary education. Only two of the women reported an annual household income over $40,000, with eight mothers reporting annual incomes of less than $20,000. The majority of participants (11) did not have children diagnosed with mental illness. However, they explained their children exhibited symptoms of poor mental health without using the language of mental illness. This is likely explained by stigma around mental illness. The length of time spent in Canada did not significantly impact differences in participants’ perceptions. Further demographic information, including cultural groups represented in the research, can be found in Table 1. In each of the 18 interviews we conducted, participants discussed barriers and facilitators they faced in accessing mental health care for their children. Below, we identify the barriers and facilitators to access to health care.
Participant Demographic Information.
Barriers in Accessing Mental Health Care
The most commonly identified barriers included financial strain surrounding expensive programs or costs associated with them, a lack of information about the Canadian health care system, feeling unheard by service providers, perceived racism and discrimination, language barriers, stigma surrounding mental health, and feelings of isolation.
Financial Strain
Nine participants explained financial strain made it difficult to access services for their children. These services were not only limited to counseling but also included sports and recreation that promote child mental health and well-being. Many discussed how they were especially limited by the high costs of programs and services due to low incomes. Caring for their children also prevented them from working outside the home, creating even greater financial pressure. One participant explained through an interpreter how financial strain was related to lack of family in Canada and the loss of her credentials when she arrived.
T (translator): In Romania I was with my parents, my family. Even if I—it was difficult with my ex-husband—I could find . . . salvation [from] my parents’ [support]. Here, it’s totally different. In Romania I had my own apartment. My financial situation was very good. I fed my family as if I was married, [like] I was a husband, the head of the family. But here I have nothing. I don’t have education. (005)
Her standard of living had decreased in Canada because she could not work in the profession in which she was trained. Loss of income meant she was no longer able to provide the lifestyle her child was used to. This led to his behavioral and mental health problems, as well as affecting her ability to seek care for him.
Lack of Information
Eight participants said lack of information about the health care system and available services was a key barrier for them, reporting frustration about not knowing where to find resources and feeling unsupported by policy makers and service providers. Even some who had been in the country for many years found accessing information to be a challenge. Participants who had entered Canada as refugees also said that they missed accessing free support that would have been useful to them, simply because they did not know about them: P (participant): They don’t know it . . . Nobody tell[s] them. How they will know? And that’s why they have trouble with the kids. If they know, they are going to ask help. But they don’t know. (001)
Settling in a new country means that immigrants often leave both formal and informal support systems and sources of knowledge (such as family) in their country of origin. This creates emotional and practical implications as they lack their usual networks from which to seek advice.
Feeling Unheard During Service Intake and Assessment
Eight participants said they did not feel listened to by either schools or service providers. Participants who felt ignored by service providers said their children were evaluated based on questionnaires, rather than taking into consideration the mother’s knowledge about her children: T: Maybe it’s better to believe what mothers say, because she [the participant] knows better her child, she helps him to grow up and everything. . . . In order to go to see a specialist, she has to fill out 8[hundred], 900 questions. (003)
The participant (through a translator) reported that she struggled through system bureaucracy and unnecessary (in her view) paperwork to access mental health services for her children. Such paperwork creates delays and may discourage or prevent parents from seeking care at all, particularly if language barriers, a lack of knowledge, or stigma are also involved.
Racism and Discrimination
Seven mothers reported racism and discrimination as causes of mental health problems for their children and a barrier to accessing services. This included racism and bullying from teachers and other children at school. In one case, the mother was not allowed to go on school field trips since she speaks limited English. Such disconnection from their children hindered these mothers’ ability to seek care for their children, thus contributing to their mental health issues. One said that she felt afraid of family services, schools, and the police: P: Here, it’s different things. Kids misbehave for a lot of things, from mental illness or just bad behaviour and so—and if you go to the hospital with a kid, first thing, they start asking you all these weird questions, “How do you discipline your kids? How . . .?” All these things. Now, if you’re dealing with a foreign doctor, they will tell you, “This is how it works in Canada.” If you’re dealing with a doctor born and raised here, before you know it you see the police . . . police come to my house at three o’clock in the morning asking me for my three-year-old . . . the police was like really mean and very rude, and, “How many black kids live in this house? (002)
She reported fearing police violence against her child based on race, especially as he gets older, and if she cannot provide the care to address his mental health needs. Fear of police or family services reprisals made it even more difficult for her to access mental health care.
Two participants felt discriminated against as immigrants, noting that they lack the support that is offered to refugees. In fact, they felt they were competing with refugees for government resources and were left unsupported because they did not receive economic support: T: It’s not fair when [we] come here—when we come here as immigrants, and there are refugee people. Government supports refugees very much, because they need [help]. But for us, they don’t pay attention. It’s unfair. (003)
These participants were Eastern European and reported feeling discriminated against as immigrants because they did not receive the same support given to visibly racialized immigrants.
Language Barriers
Language barriers were another key theme and were often connected to both issues of racism and discrimination and a lack of information. Seven participants specifically discussed the impact of language barriers on accessing care. Participants cited having difficulty communicating with their child’s pediatrician, having to depend on family members for communication (including in some cases the child receiving care). Even when participants were able to access services, they could often not understand medical terminology. Many reported that this created feelings of dependency, isolation, and powerlessness, negatively affecting their relationships with their child or spouse (whoever was translating for them): T: When they went to the therapist, the therapist and him, they started talking, but I was totally isolated. . . . He didn’t translate so I was totally blocked. (013)
Several spoke of the benefit of translators. However, they also brought up issues of confidentiality and difficulties in translating medical terminology. Parents who had access to health care professionals who spoke their own language reported that they could communicate with them directly, which made them feel involved and informed throughout their child’s care.
Stigma
Seven participants said stigma around mental health and the fear of having their child labelled was a factor that made it hard for them to seek mental health services. Still, they all said this would not and did not prevent them from doing so: P: Well, speaking from my own family . . . [they] would not be happy to know that there’s mental health issues. But they would rather that we got it solved . . . than just be focused on trying to keep it quiet and we don’t want others to know. That’s my own family. So, the family stigma is not so much of a bother for me. (010)
Many mothers explained they felt stigma from their community but wanted to undo that stigma. Others said that despite the stigma, their main priority was providing care to their children. The main issue related to stigma was how it made them feel isolated because they felt they could not talk about their children’s needs or ask for information from their community.
Feelings of Isolation
Six mothers explained their own isolation, from both the general community in Canada and from their family in their country of origin, which influenced their capacity to access mental health services for their children. This isolation meant they were less able to learn about services, were unable to talk to other parents for comfort and information, and were less mentally and emotionally well themselves, undermining their parenting abilities: P: It was a complete mess . . . I was here and I am here in this country with just me and the kids. . . . From the first two years . . . [ and] from three through five years old he was like—he was like—it was hell. All I got was the runaround. (002)
This participant reported feeling as though no one would take responsibility for helping her access services. The “runaround” she refers to was being repeatedly sent from one person to another for support. Such isolation can arise, then, when immigrants lose networks and support systems, which can exacerbate stress in caring for a child with poor mental health.
Facilitators
Parents also discussed what factors facilitated their accessing of services for their children. Three areas emerged: being offered mental health services for their children through schools, having a high level of education, and provision of free services provided.
Services Offered by the Schools
Twelve participants talked about schools offering services or coordinating the provision of services—usually organized by teachers or principals—making this factor the most commonly cited facilitator of access to mental health services. Because many immigrant parents do not know where to access information or how to navigate the Canadian health care system, schools are critical sites of support and transmission of information, offering parents ways to be involved, network, and learn about resources: T: For me, there was [a] very difficult time in my life. In Ukrainian school, they help us a lot. They give us [assistance], refer us to go to the agencies, [provide] good direction. (004)
While many mothers reported feeling frustrated, unsupported, and isolated when schools did not provide effective support, those who had positive experiences with schools reported being well-equipped to access care for their children.
Having a High Level of Education
Six mothers had university or postgraduate degrees, and all said this level of education helped them to promote their children’s mental health and access services when needed. Their educational backgrounds included health care, education, and psychology, which are especially pertinent to child mental health. These specific educational backgrounds prepared them to better manage their children’s mental health challenges on their own. High levels of education also enabled them to seek outside help when needed. One mother discussed how when her son faced discrimination at school, she was able to support him because she knew how the school board system worked and what she was entitled to P: I was just like pissed off with the principal, so I just said that, “If . . . you will not take any action, then definitely I will write a letter to the board . . . because then I don’t have any other choice. But I will not keep my mouth shut, because I am an educated Canadian woman.” . . . Yeah, this was my, you know—I still remember my sentence, that I am an educated Canadian woman. I know my rights as well as my responsibilities. (015)
Education was thus helpful for these mothers: they had training to care for their children themselves and were better positioned to know their rights in Canada, to resist discrimination, and to access services.
Availability of Free Services
Four participants said that because they were able to access free services, such as sports and recreation, speech language pathologists, occupational therapists, psychologists, and libraries, they were able to promote their children’s mental well-being or better treat their mental illness issues: T: After assessment if they are eligible for FSCD [Family Support for Children with Disabilities], specialized services, then they will get the funding from government . . . the family can hire the professionals, come into the family to support the parents and the children. (018)
That these services were free greatly enhanced participants’ ability to access them. They also afforded them the time or resources to more effectively take on other barriers, like lack of information and isolation.
Discussion
In this research, we sought to understand immigrant and refugee mothers’ perspectives about the barriers they face in accessing mental health services for their children in Alberta, Canada, as well as factors that facilitate that access. Our findings corroborate prior research around mental health care access but shed new light on the concerns and challenges of immigrant mothers’. For example, consistent with Salami et al. (2019), we found language barriers featured as a key theme, connected to learning information. Language barriers often meant mothers felt disconnected from their children’s schools and out of the loop about their lives outside the home, consistent with findings by Beiser et al. (2015) and Ying and Han (2008), concerning parent’s participation in children’s lives after settlement. Participants also noted how this changed power dynamics within the family, consistent with findings in Mesch (2003). As noted above, one participant described how helpful it was to be able to directly communicate with her child’s bilingual doctor. Others said it was important to have a translator, but this also can pose problems in terms of confidentiality, power sharing, and the service provider’s skill with a translator (Zendedel et al., 2018). Our study added to these findings by exploring how language barriers create increased stress for parents when a child needs care because they feel there is pressure to address children’s’ needs early in development.
Stigma was also a concern for participants in our study, corroborating other finding on immigrant’s access to mental health care (Saechao et al., 2012; Salami et al., 2019; Thomson et al., 2015). Building on this work, we found that parents often downplayed the role of stigma, because their main concern was to provide care for their children. Likewise, our findings show that the fear of repercussion was present but did not feature heavily in participants’ concerns. However, participants did discuss fear and stigma in transnational ways. For instance, they highlighted simultaneous connections to Canada, which most saw as open and accepting of mental health concerns—but they also made links to their countries of origin, families in their home country, and immigrant communities in Alberta to which they belong. However, in those contexts they felt pressure to keep mental health challenges hidden.
When immigrants leave their country of origin, feelings of being ignored, unsupported, and disempowered in Canada are largely tied to a loss of familial support. Several mothers explained that their own education helped them not only to parent their children more effectively but also to know their rights and feel more confident engaging with service providers and schools. These mothers explained that their education reduced their own self-stigma around mental health as well. These outcomes align with findings showing that increased social capital plays a large role in access to services post-migration (Sime & Fox, 2015) and that education increases health care access regardless of immigration status (Mirowsky & Ross, 2003/2017).
Participants explained they often found it difficult to afford all costs associated with accessing care for their children. Many reported not having financial, emotional, or practical support from extended family, which they counted on in their country of origin. Some participants were also responsible for sending money to their families in other countries and therefore felt the burden of such costs affecting their access to mental health services in Canada. Studies have shown that immigrants are more likely to face poverty and poor economic outcomes than nonimmigrants in Canada (Guo, 2009; Nakhaie & Kazemipur, 2013). Income, alongside education, is an important social determinant of health, with studies showing that higher income is connected to better health outcomes and access to services (Adler et al., 2016; Pickett & Wilkinson, 2015). Most participants fell below the poverty line, despite many of them having high levels of education.
Implications
This study found opportunities for transcultural practice in mental health care delivery. In terms of research and practice, mental health care provision can incorporate family-centered care by inquiring into the values (including cultural) of immigrant families and integrating them into care delivery. Furthermore, it is important to provide trained interpreters to help bridge barriers in communication. The use of trained interpreters who are well grounded in the cultural nuances of the patient population can help enhance culturally congruent care. Nursing education can also help ensure culturally congruent care by incorporating self-awareness, including of how nurses’ values, beliefs, and culture influence the care they provide.
Mental health care interventions can operate in schools, specifically through the creation of support groups and mental health champions in schools. For example, nurses can be proactive by integrating assessments and mental health education into their patient care with such populations. They can also educate teachers and other personnel working with children on strategies to improve child mental health. Creating opportunities for parents and children to connect with others (e.g., through parenting programs) can help foster community belonging, decrease isolation, and improve mental health. As family income levels are also critical to children’s mental health—for example, the ability to pay for children’s participation in sports, nurses can support the mental health of immigrant children by connecting their parents to vital community resources and to social services to address poverty.
In addition to mental health care practice, our study raised implications for immigration policy makers, who can bridge access to mental health by funding programs that incorporate mental health promotion in both pre- and postmigration counseling. Addressing the systemic and racialized barriers immigrants face in accessing mental health services can also improve their mental health. Policy makers can enforce antiracism programs and create broader comprehensive strategies to address deskilling of immigrant parents and subsequently address issues related to poverty in immigrant communities. Policies targeted at improving access to sports for low-income families, including immigrant families, can help improve this population’s mental health status. Also, policy that supports the provision of affordable mental health services in schools and community settings can improve population health outcomes.
Limitations
Due to the relatively small sample size of participants involved in qualitative research and the fact that our study was conducted in just one Canadian city (Edmonton), findings may not be generalizable to a large population (Carr, 1994). In this study, we seek the transferability of our findings by providing contextual information and quotes.
Conclusion
Findings show immigrant and refugee mothers face an array of barriers in providing care for their children’s mental health, from financial to language to isolation and exclusion from participation in their child’s mental health care. Financial strain, fear of stigma, and experiences of discrimination all posed significant barriers to their children’s access to important services and were often interrelated. Parent-centered knowledge and culturally appropriate care delivery, as well as more effective information transmission and bridging between immigrant and health care policy realms are important to dissolve immigrant children’s barriers to access. Further research to determine the effectiveness of increased funding for recreation and sports in preventing poor mental health outcomes for this population is also needed.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research has been funded by the generous support of the Stollery Children’s Hospital Foundation through the Women and Children’s Health Research Institute.