
Abstract
Introduction:
Adolescents health care brokers interpret for family and community members lacking English language proficiency in health care settings. The purpose of this study was to explore personal experiences of Burmese and Bhutanese teenagers who served as health care brokers in resettled refugee families in Northeast Ohio.
Method:
A mixed methods design using photovoice guided this study. Participants completed the Adolescent Language Brokering Survey, took photos, wrote in journals, and attended focus groups.
Results:
Eight Burmese and Bhutanese teenagers participated. Three themes became apparent: health care brokering within sociocultural contexts, mediation during health care encounters, and representations of childhood.
Discussion:
The adolescents were proud to be health care brokers yet found it disrupted their lives because they were living in both their traditional culture and the American culture. Photovoice empowered them through dissemination of findings during a photo exposition, community meeting, and health literacy class. Health care professionals must recognize benefits and prohibitions when working with adolescent health care brokers.
Adolescents or children who translate or interpret for parents, grandparents, siblings, and neighbors in immigrant or refugee communities are called language brokers (Bauer, 2016; Tse, 1996). Adolescent health care brokers are teens who navigate the health care system in a variety of ways on behalf of others lacking English proficiency in health care settings (Banas et al., 2016). They are often members of refugee families who have been forced to cross national boundaries and are unable to return home safely due to armed conflicts or persecution (Koh et al., 2013; Yang, 2016). There are over 22 million refugees worldwide and half are younger than 18 years of age (UNHCR, the UN Refugee Agency, 2017). Of the 671,000 refugees admitted to the U.S. between 2008 and 2017, more than half were from Asian countries including Burma, now known as Myanmar, and Nepal (Krogstad, 2019).
Burmese
Thousands of Burmese, ethnic Chin, Karen, Shan, and other tribal hill peoples, speaking different languages and dialects, started leaving Burma in the 1970s due to ongoing human rights violations spending decades in refugee camps in Thailand or in Malaysia. They began to arrive in the United States around 2008 and now number nearly 110,000 (Centers for Disease Control and Prevention [CDC], 2016). Traditional Burmese culture is collectively oriented, with high value placed on family and religion (Burmese Culture, n.d; CDC, 2016). Burmese are indirect during communication and limit self-expression to preserve harmony (Bower, 2008). Children and adolescents are active members of the family and are aware at a young age that they are to seek to increase the family’s well-being (Koh et al., 2013) by participating in tasks within the home and community (Ramírez Carpeñon & Feldman, 2015).
Bhutanese
Thousands of Bhutanese of Nepali origin (also known as Lhotsampas) fled Bhutan in the early 1990s to escape political and ethnic persecution. They lived in United Nations’ administered refugee camps in Nepal before resettlement in countries around the world. Many of the younger generation were born in a refugee camp. Almost 100,000 Lhotsampas have resettled in the United States (Bhatta et al., 2015). Most speak Nepali as their first or second language. The community is tightly knit and family is one of the highest values in their culture. Elders command respect and are often included in discussions of health, finances, and other family issues (Maxym, 2010). In their traditional culture, children and adolescents are considered competent to contribute to family and society (Hinton, 2000). They are not public decision makers but are important to family cohesion as well as influential in bringing information into the home (Bodapati, 2019; Hinton, 2000; Evans, 2007).
The U.S. Office for Civil Rights issued policy guidelines in 2004 stating that individuals with limited English proficiency treated in federally funded facilities must be informed that interpreter services are available. Interpreters should not be minors, family, or friends (Harjer, 2019). Despite these regulations, it is well known that adolescents continue to function as health care brokers (Banas et al., 2016; Banas et al., 2017; Katz, 2014; Martinez et al., 2017).
Literature Review
Health care brokering has been perceived by some as adolescents functioning in adult or parental roles, thus unethical or detrimental to the child (Katz, 2014). To others, it is viewed as a transformative role in which adolescents serve their families as they mature into adulthood (Bauer, 2016). Adolescents themselves have perceived health care brokering as a negative experience, describing it as stressful (Anguiano, 2018; Banas et al., 2017; Crafter et al., 2017; Kam & Lazarevic, 2014); burdensome (Kim et al., 2017; Weisskirch, 2013; Wu & Kim, 2009); embarrassing because of sensitive information (Free et al., 2003; Katz, 2014; Kim et al., 2017); and resulting in absences from school and teen activities (Ball et al., 2016; Banas et al., 2017; Kim et al., 2017). On the other hand, teens have reported health care brokering as a positive experience when they felt needed, important, or gave voice to their parents (Bauer, 2016; Katz, 2014; Orellana & Phoenix, 2017). They felt proud (Banas et al., 2017; Bauer, 2016; Dixit et al., 2017); dutiful or loyal (Crafter et al., 2017; Katz, 2014); and had a greater sense of self-efficacy (Wu & Kim, 2009).
Since young people often acculturate faster than resettled adults (Bodapati, 2019), a debate continues as to whether adolescent health care brokering is an unhealthy role-reversal or a healthy way of relationship building (Garcia-Sanchez, 2018; Titzmann, 2012). Roche et al. (2017) found that language brokering correlated with lower parent–child closeness and less parental regulation of teen behaviors, akin to a role reversal termed parentification (Titzmann, 2012). Bodapati (2019) found that parental illiteracy in the new country’s language pushed Bhutanese teens into what that author called, premature adulthood. On the other hand, Corono et al. (2012) and Guntzviller et al. (2017) found that working through the challenges of a multilingual health care setting could be a shared parent–child experience. Though research has investigated adolescent language and health care brokers in various countries and among a variety of ethnic groups, little is known about adolescent health care brokers in resettled refugee families. The purpose of this study was to explore experiences and perceptions, through photovoice, of Burmese and Bhutanese adolescents who served as health care brokers in resettled refugee families in Northeast Ohio.
Photovoice
Photovoice is a visual research method developed for the purpose of going beyond conventional community assessment to empower people to reflect on their community’s strengths and concerns (Wang & Burris, 1994). Using photographs and focus group follow-up, photovoice is meant to reach, inform, and organize community members, enabling them to discuss and prioritize problems and solutions. This method has been used to study adolescent immigrants (Adekeye et al., 2014; Roxas et al., 2017), children in refugee camps (Oh, 2011), migrants (Moskal, 2017), and resettled refugees (Dixit et al., 2017; Vecchio et al., 2017).
Theoretical Framework
In this study, de Abreu and O’Dell’s (2017) theory on child language brokering in health care settings was used. Their metasynthesis of previous research of children and young people as language brokers was linked to critical developmental psychology and sociocultural theory. They conceptualized language brokering into three main areas: (a) adolescents as language brokers in sociocultural settings, (b) the mediation during health care encounters, and (c) representations of childhood while language brokering. Health care situations include every day family activities (Anguiano, 2018), formal health care settings (Banas et al., 2016; Banas et al., 2017), and emergency or unfamiliar circumstances (Katz, 2014). Mediation may occur in routine encounters involving family support or advocacy (Cline et al., 2010); complex encounters in which young language brokers have had little or no previous exposure to medical vocabulary, diagnoses, or concepts (Antonini, 2016); or to sensitive, even taboo situations (Nielsen et al., 2019). Portrayals of adolescent language brokering include examples of role confusion and distortion (Antonini, 2016; Titzmann, 2012); a shared family life (Corona et al., 2012; Guntzviller et al., 2017), and normal maturation toward adulthood (Bauer, 2016).
Method
Design
A mixed methods design guided this study. For the quantitative arm, participants completed a 19-item survey. For the qualitative arm, photovoice techniques were incorporated. Approval was obtained from a university’s human research committee after receiving endorsement letters for this study from agencies that worked within the refugee community where participants were recruited.
Setting
About 9,000 Asian immigrants and resettled refugees live in Akron Ohio and the surrounding communities (World Population Review, 2020). This includes many Burmese and Bhutanese adolescents; approximately 50% of the students attending a local high school are of Asian descent (Harper, 2015).
Sampling/Recruitment
Burmese and Bhutanese teens were purposively sampled for this study. They had to be between the ages of 15 and 18, with experience as a language broker. Since none of the researchers were of Burmese or Bhutanese ethnicity, they sought community liaisons through three local agencies working with resettled refugees. The lead author had previously conducted research in this community so was known at those agencies; they introduced her to community contacts. A Burmese woman serving as an intern in one of the community organizations was the liaison to Burmese teens. A Bhutanese community leader who had contact with teens through families involved in community activities was the liaison to Bhutanese teens. The coauthors gave recruitment letters with consent forms to the liaisons who in turn spoke with adolescents and their parents in their native language. The liaisons helped organize meetings with teens at a local high school through contact with school administration. Each teen participant signed an assent form and one of their parents signed a consent form. Liaisons collected consent forms to return them to the research team.
Measurements
The Adolescent Language Brokering Survey used in this study was a 19-item questionnaire constructed with eight demographic questions and 11 items about language brokering. The questionnaire was based on surveys used in earlier research. Permission was granted to modify those surveys for the study. Six items from the Student Survey (Banas et al., 2016), including a question on emotions experienced during brokering situations, and six items from the Language Broker Survey (Tse, 1996), including a question asking the teens to evaluate their overall personal experience of health care brokering, were incorporated into the survey used in this study.
Data Collection
On a prearranged date the researchers and participants met to complete the survey. Then single-use cameras were distributed. The researchers provided verbal and written instructions, and a demonstration of camera use since the teens were not familiar with this type of camera. Single-use cameras were used rather than personal cell phone cameras because of ethical considerations. The teens had opportunity to ask questions about the camera and to correctly demonstrate its use. They were instructed to take photos over a period of 2 weeks, of objects, situations, or encounters related to language brokering in health care settings. Instructions included no photos of individuals’ faces or of objects that could reveal someone’s personal information. Each participant also received a notebook in which they were to write a brief description of each photo and the emotion felt related to the photo. On a designated day they returned the cameras and journals. The cameras were mailed to an independent company for film development. Next, the coauthors facilitated a focus group with the teens during which each teen chose five of their own photos to share with the group. They took turns presenting a photo of their choice to the group and explaining the significance of the image. They were also given time to comment on other participants’ photos as a way to compare and contrast their own experiences. The sessions were audio-recorded to collect additional narrative data; one coauthor took extensive notes during the discussions. Each participant received a $10 gift card as a token of appreciation. The researchers debriefed after the focus group sessions.
Data Analysis
The survey data was analyzed with descriptive statistics for response frequencies. Key words, phrases, objects, places, and other items from the journal entries and photos were also quantified. Using a manual process, content thematic analysis was used to organize the qualitative data. The authors each read through the journal entries several times highlighting key words and phrases which they wrote on note cards. Participants’ narratives explaining the photos, and the photos themselves, were compared with the journal entries. Categories were developed and then coded into three priori themes (Chapman et al., 2017), using de Abreu and O’Dell’s (2017) theory of child language brokering.
Results
Description of Sample
Eight teenagers, three males and five females, participated in this study. Four were Burmese (born in Thailand) and four were Bhutanese (born in Nepal). Their age at arrival in the United States ranged from 6 to 12 years. They were 15 and 17 years of age, and in Grades 10, 11, and 12. Seven were bilingual; one was trilingual.
Survey Results
All eight teens were health care brokers in the hospital and in an emergency department; seven at a pharmacy, six in a clinic, and six on the phone. Four teens said that they had been asked by a health care professional to be a translator in a health care setting. All had translated for a parent, six for a grandparent, and four for a nonfamily member. Four teens indicated they were health brokers at least once a week; five said they had missed school to translate. In response to feelings about being a health care broker, the participants admitted to a gamut of emotions: from pride (n = 8), nervous (n = 7) to calm and determined (n = 4). Five teens felt that they were expected to be language brokers rather than volunteers. Only one teen indicated being ashamed to translate and two recorded that brokering was a burden. Seven participants reported that language brokering helped them learn English; half believed translating made them more independent and mature. When asked about things they would like to learn to help others while language brokering, the majority wanted to learn to fill out medical forms, to read medical bills and legal health care documents, to learn medical vocabulary, and how to talk to a physician or nurse. They indicated they would like resources about bilingual health-related websites and question and answer web chat sessions. Detailed results of the survey are described in Table 1.
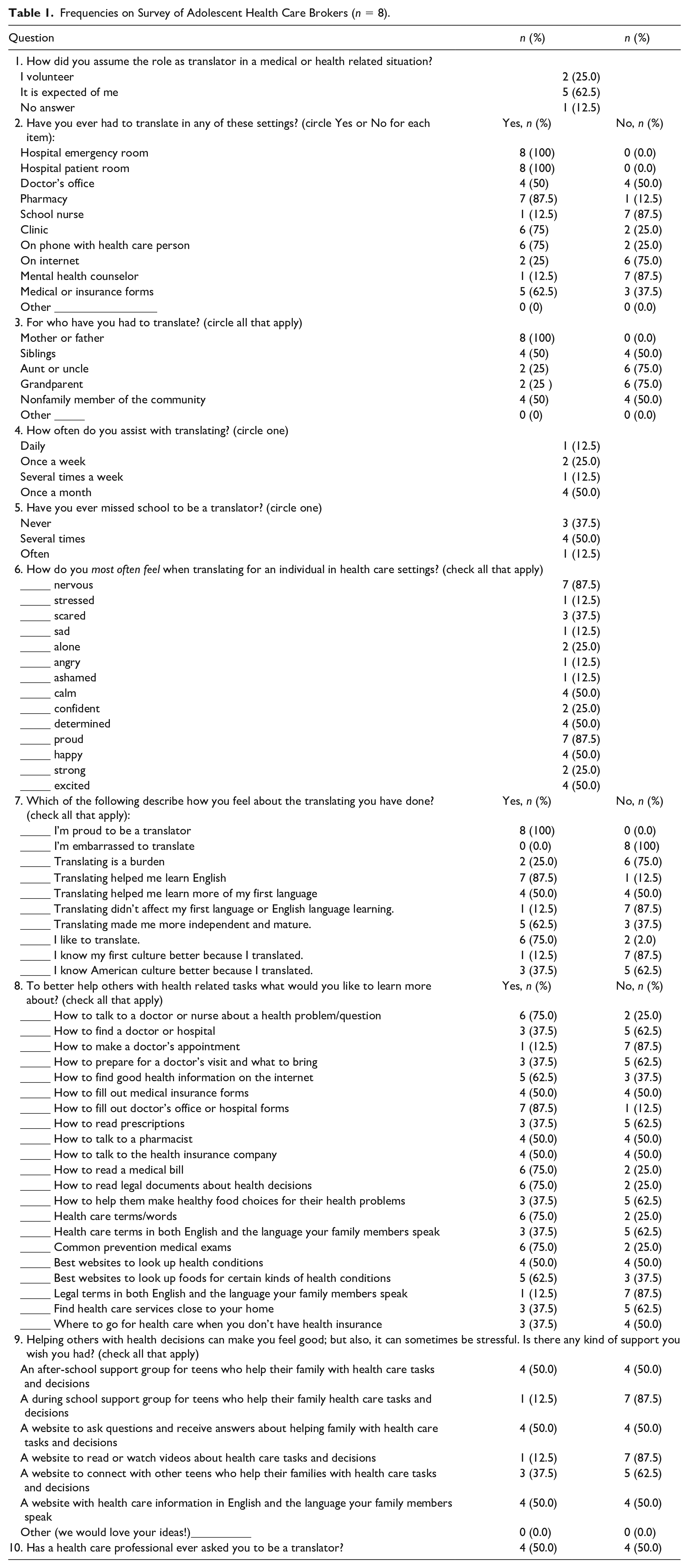
Frequencies on Survey of Adolescent Health Care Brokers (n = 8).
Photos and Journals
The eight teens took a total of 32 usable photos. (Several other photos were unusable because they were out of focus; some were damaged by the film developing company.) Indeed, 21 of the 32 (65%) photos were pictures of health-related objects such as a toothbrush, pill bottles, medications, phones, medical forms, and pharmacy signs. Eleven photos (33%) were symbolic objects including: wind chimes, the night sky, flags of different countries, a blanket, and a notebook. About 70% of the photos were taken within the participant’s home. The types of brokering situations included reading letters, mail, and medical forms; interpreting in doctors’ offices and pharmacies; and mediating with a landlord, a 911 operator, and pharmacy employees. Most interactions were either in person or on the phone. Common emotions mentioned in the journals included feeling irritated, frustrated, and conflicted. Table 2 includes details about the photos and journal entries.
Synopsis of Journal Entries Related to Photos (n = 32).
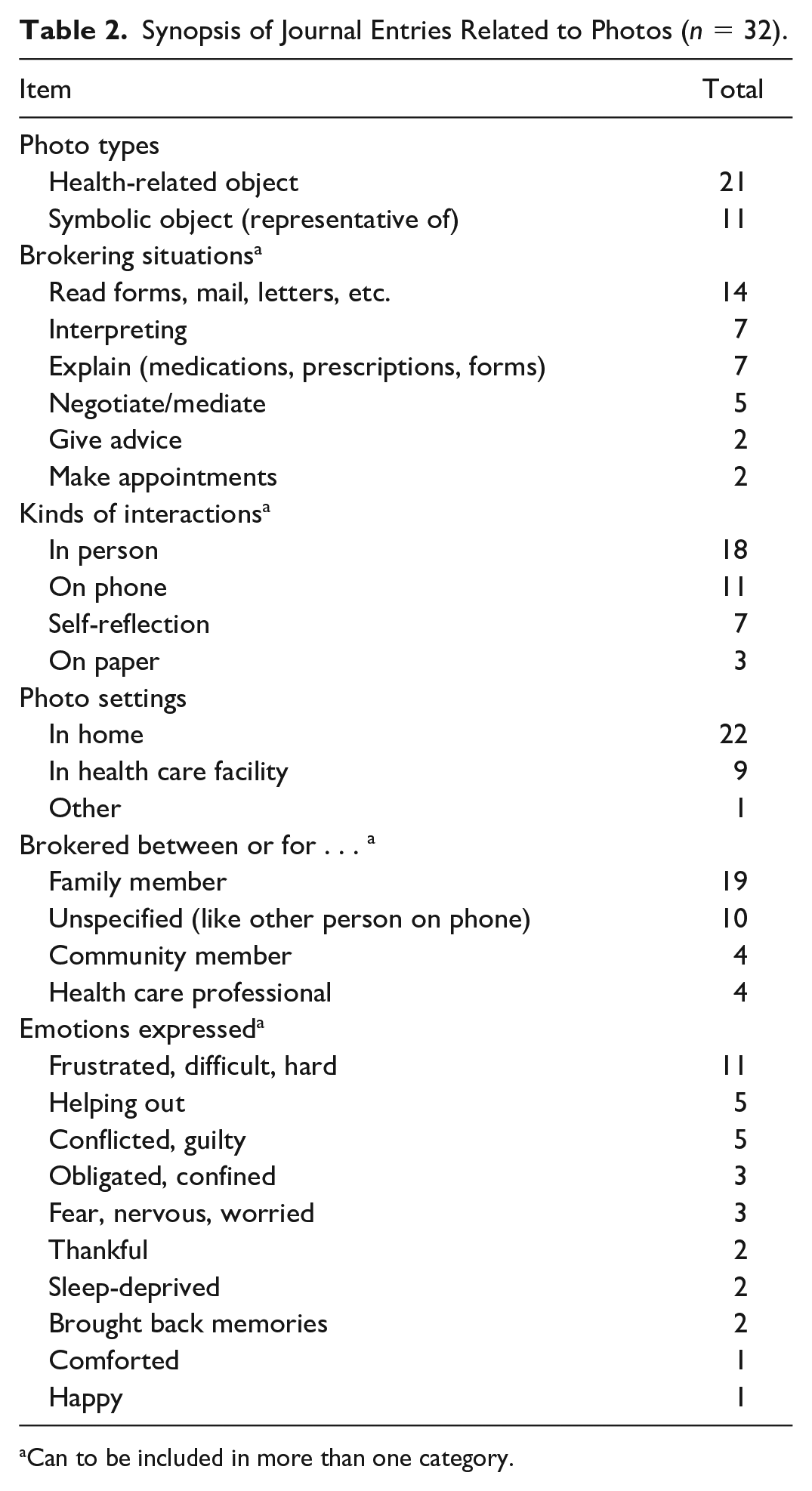
Can to be included in more than one category.
Themes
Focus group sessions gave the teens opportunity to share personal perspectives on their photos, which led them to open up about experiences and feelings that were not captured in the photos or journals. The qualitative data produced three themes that aligned well with those conceptualized by de Abreu and O’Dell (2017).
Brokering Within Health Care Settings
The adolescent participants described health care brokering during everyday family activities, in formal health care settings, and in emergencies. Their descriptions of these situations included translating instructions on forms, prescriptions and medicine bottles, describing healthy foods, explaining the dangers of air fresheners to an asthmatic family member, and advising the elderly to keep appointments. Brokering tasks in formal health care settings included interpreting for hospitalized patients, in the dentist office, and at the pharmacy; also using the phone to make appointments. One young lady described an emergency situation. “I had to call 9-1-1 when my little brother fell and cracked his head. It was my first time translating. I was nervous” (Figure 1).

Phone represents call to 9-1-1 in emergency situation.
Mediation During Health Care Encounters
The teenage health care brokers in this study acted as mediators or negotiators during routine and complex brokering encounters. Several young people described incidents of mediating situations that could be considered routine. One teen filmed a pharmacy sign to explain helping a family member. “I refilled my sister-in-law’s medication [at the pharmacy]” (Figure 2). One young man went to a physician for a physical exam accompanied by his father. The boy explained the questions on the medical form to his father and the father provided the necessary answers for the doctor.

Sign represents trip to pharmacy for prescription.
Several teens described complex mediation situations, explaining that it was not easy to translate when they themselves did not understand the words. One teen explained his photo, “I took a picture of a pill bottle. It’s really hard to translate prescriptions. I really hated those. Some medical terminology is very hard to translate.” Another wrote, “It’s a photo of a closed notebook and a pen. When you don’t understand big words they use, everything goes blank in your head. It’s hard” (Figure 3). One girl described a difficult mediation experience during which physicians asked her questions and relayed medical information through her to her family.
I did not know the word for liver. They didn’t know I wasn’t 18 years old. They thought I was the representative of [my grandmother], and told me she had a really high ammonia level and that her liver has failed. When they told me her liver failed, I didn’t know what liver was . . . or how to explain it in [my language]. So my parents like, call and ask me and I searched it up and showed it to them. But I translated the wrong words to my parents. So the doctors said it was a very serious condition but I didn’t use the right words to explain to my parents. They thought that my grandma just had an old age thing so because of that miscommunication thing, my parents thought, yeah she will be better. The second time I met with the doctors they asked my age and they were like “We had no idea you were so young.” They said we should be talking to someone else, her guardian. So then like, when they knew I was young, I could ask for like a real translator for my parents to talk to so they know the condition well. The next day they met with the translator and everybody together and I was at home then. They came back after and they didn’t tell me anything except they said, “Your grandma only has a month left to live.” I was shocked. I had no idea she would only live a month. My parents didn’t say anything because they know I was hurt but they kind’ve blame me because I could not translate the right words. I told them it was not serious. I hate the word “liver.” I felt useless.
Notebook and pen represent big words hard to understand.
Another teen described his experience as a mediating language broker with a photo of a can of Raid insect spray (Figure 4).
My mom wanted me to talk to the landlord about all the roach-like bugs in our house, especially during the night. She wanted me to ask him if he could spray the entire house with the bug killer chemicals. Sometime I worry about our health because bugs are everywhere and you never know when my baby brother will touch them.

Can of insecticide represents mediating with landlord.
One of the girls shared a difficult situation that happened while her mother was hospitalized. A physician was using a professional interpreter to speak with her mother. The teen noticed that the interpreter did not speak the same dialect and was using words the teen’s mother did not understand. The teen pointed this out to the interpreter who subsequently shamed the girl for interfering. The young woman told us that she was initially hesitant to intervene but on further reflection was proud of herself for having the courage to step in.
Adolescent Health Care Brokers’ Representations of Childhood
All participants stated they took on responsibilities for family members who could not speak English well inside and outside of the health care setting that may be perceived by Western culture as adult-like roles. They found themselves conflicted between adhering to traditional family expectations and adopting the social norms of American teenagers. As revealed in the survey results, some participants were proud to be helpful to their families but also felt guilty for wishing they were not relied on as much. Several participants described brokering like entrapment due to missing school, being held back from higher education, from getting married or following career paths of their choice. One teen said, “I had to explain what happened to [his] feet, and what to do so it doesn’t happen again. Most parents are busy with work or don’t know how to drive so you have to stay home until [we] find someone to go see the doctor.” (Figure 5)
Another participant journaled this statement, describing her sense of obligation; “I took a pic of the wind chimes representing how I wanted to float freely outside. I always miss the outside, especially when we have to stay a long time in the hospital [to be an interpreter]” (Figure 6).

Wind chimes symbolize desire for freedom.
Photo of feet reminded him of being the one relied on to explain the problem.
Some teens indicated they put their future plans on hold because they respected their family. One girl’s comments were very insightful.
You know, we have to think about family. It’s because of us they came to America. Knowing that they are depending on us, just to move or go away from them, we couldn’t. Being considerate, it’s being with them; leaving would be disrespectful. We would have to bring them with us.”
Another young lady, though not the oldest child in the household, explained why she shouldered the responsibility for health care brokering.
I want to help them. I feel like I was born to help them; because my sister got married early and my brother also got married, and they’re useless now. They’re older. When my parents asked them, I don’t know why, they never like, cared. They don’t like doing those things. It’s not like I like doing it, but I try to learn about those things because I want to be useful for them. Because I became useful, they keep using me. They say, “You know how to do it; you should do it.”
Discussion
This photovoice study empowered eight teens to share their experiences as health care brokers. Their survey responses, photos, journal entries, and focus group comments made it clear that they were active in their homes and community in multiple settings involving physical, mental, and environmental health. Half had been asked by health care professionals to be interpreters in situations where a professional interpreter should have been engaged. They were challenged by limited health literacy, time constraints, and responsibilities for interpreting in families where cultural traditions were changing.
The most poignant finding of this study was the tension the role of health care brokering generated in these teens. The adolescents were proud to be health care brokers yet found interpreting disrupted their lives because they were living in both their traditional culture and the American culture. Their elders expected them to contribute to the family’s well-being. They were required to miss school if needed for a brokering task. These findings were confirmed by research in other cultures (Anguiano, 2018; Ball et al., 2016; Banas et al., 2017; Cline et al., 2011). In Western culture, this may appear to be a role-reversal, termed parentification (Kam, 2011; Titzmann & Gniewosz, 2018) or premature adulthood (Bodapati, 2019). It is perceived by some as damaging to teenagers because of the potential for a negative impact on family dynamics (Katz, 2014). But for people from a traditional culture in a new country it may be more important for the family’s adjustment and eventual integration that adolescents serve as health care brokers.
To the contrary, the teens also experienced positive feelings toward brokering and were willing to continue involvement in such activities because Burmese and Bhutanese adolescents are expected to contribute to family and society (Hinton, 2000). Bauer (2016) terms this “kinship care,” a way to support the resettlement and functioning of the family. Teens are not public decision makers but may be trusted to inform the family about health issues (Evans, 2007; Hinton, 2000). In the present study, the teens used words such as “helping out,” “she needed me,” and “happy I could help.” Their attitude was part of a culture of caring, helping others solve problems particularly when mediating a situation, exemplifying an interdependent relationship (Bauer, 2016; Crafter & Iqbal, 2020; Garcia-Sanchez, 2018).
A second point of tension revealed in this study was felt by adolescents when asked to interpret by health care professionals or by family members in situations where professional interpreters should be used. On one hand, teens were expected to help their family and on the other, would not refuse an authority figure such as a nurse or physician. Other studies revealed similar results (Banas et al., 2017; Guntzviller et al., 2017; Gustafsson et al., 2019). Health care providers are to use professional interpreters rather than family members, however, adolescent health care brokers are being used despite regulations to the contrary. Interpreters are not always readily available, and resources for translating are not always provided at facilities such as pharmacies. Parents may prefer their own children because they trust them, know their dialect, understand family dynamics, and know their medical history better than a professional interpreter (Green et al., 2005; Hsieh, 2015; Padilla, 2015). Adults may worry about confidentiality if the professional interpreter is from the same community (Smith, 2018).
Photovoice Empowers Teens in their New Culture
One objective of the photovoice strategy is to promote dialogue of the issue under investigation (Budig et al., 2018; Wang & Burris, 1997). To reach this objective, this study’s findings were promptly and jointly disseminated by the researchers and teen participants so that the teens’ voices could be heard by the community and beyond. A community meeting house was the site for a 2-month exposition of a selection of the participants’ photos. Each photo was accompanied by an anonymous quote from a teen’s journal. This photo exposition alerted a reporter from a local music, art and culture newspaper who wrote an article for its monthly publication. It included quotes from the teens and researchers along with several photos. The lead author and teen participants also collaborated in a panel discussion during a town hall type community meeting in the teens’ neighborhood during which they were again able to publically verbalize their experiences. In response to a need teens expressed in the survey, the researchers organized a health literacy session on medical vocabulary. Using a participatory format, a nurse taught English words for medical conditions, human anatomy, and the titles and roles of health care personnel.
Limitations and Strengths
This study had a few limitations. The sample size was small, all the participants were from the same geographic location, and they were volunteers. The number of photos was limited because teens had difficulty focusing the cameras and the development company accidently destroyed some photos. Therefore, these participants’ experiences and perspectives may not reflect those of other adolescent health care brokers from the same or different cultural backgrounds. Notwithstanding these limitations, this study adds to the understanding of the culture of Burmese and Bhutanese resettled refugees in health care settings. The use of multiple methods to gather and analyze data increases the trustworthiness of the findings. And health care providers who encounter adolescent health care brokers during clinical care of patients with limited English proficiency should recognize the inherent challenges.
Implications for Future Research
Photovoice could be used again in this community to learn about other issues confronting teens, such as racial, environmental, scholastic, and academic topics; and more about the challenges of acculturation faced by resettled refugees. Additional research among youth in resettled refugee families in other U.S. settings could further explore the findings of this study. More research is needed to determine if adolescent health care brokers living with the tug and pull of acculturation are affected emotionally. Research is needed to learn why nurses rely on adolescent interpreters instead of professional ones. Health care professionals and community members can learn from each other in sessions where teens and adults have opportunities to speak with each other and gain confidence and understanding of health care issues. In summary, photovoice is a valuable way to empower youth to express themselves and for health care providers to learn from them.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.