
Abstract
Introduction
Research highlights that patients from ethnic minority groups often receive lower quality of care. This study contributes to the knowledge and understanding of culturally sensitive care and explores health care professionals’ definitions and perceptions of this concept and how they deliver this in practice.
Method
This qualitative study conducted a total of six focus groups (n = 34) and four in-depth interviews with six categories of health care professionals in Belgium. Thematic content analysis was used.
Results
The results indicate that the concept of culturally sensitive care is perceived quite narrowly. Professionals are likely to portray their own frame of reference and find it challenging to show empathy with patients with a different background. Othering (micro-racism by defining “the other”) is a powerful example.
Discussion
The discussion reveals the significance of increasing cultural awareness and understanding, sensitizing about current narrow perceptions, and enhancing culturally sensitive care in the Belgian health care setting.
Keywords
Background
With a total of approximately 1,208,542 inhabitants, Brussels, the capital of Belgium, comprises a very ethnically and culturally diverse population. According to the World Migration Reports, up to 182 different nationalities live in the capital region of Brussels, making it the most cosmopolitan city of Europe and second in the world (UN Migration, 2019). Other Western cities also encounter large numbers of different nationalities and ethnic backgrounds, which may translate into an increasing number of patients from diverse cultural, ethnic, and linguistic backgrounds. Scientific research highlights that patients from ethnic minority groups often receive lower quality of care and less accurate diagnosis (Hart & Mareno, 2014). In addition, it appears that there are profound inequities and disparities toward these groups when they need health care (Brondolo et al., 2009; Hart & Mareno, 2014; Luiking et al., 2019). Culturally sensitive care is expected to enhance patient satisfaction as well as to improve health outcomes (Green-Hernandez et al., 2004). This article aims to provide insight into how health care professionals define and perceive culturally sensitive care and how they (try to) deliver culturally sensitive care in daily practice.
A culturally sensitive care approach is used when patient and health care professional—from different ethnic–cultural backgrounds—are in interaction with each other to search for a connection in order to build a (better quality) care relationship (Uzun & Sevinç, 2015). This care relationship is affected by the cultural characteristics of both the patient and the health care professional. By accepting and overcoming these cultural differences, a customized concept of care begins. The latter responds to the questions and needs of the patient, regardless of their culture, religion, or origin. Although the concept of “culturally competent care” is widely used in the international scientific literature (Burchum, 2002; Markey et al., 2018; Papadopoulos & Lees, 2002), this concept is not used in daily care practice in Flanders and/or Brussels, where the concept of “culturally sensitive care” is favoured. The literature shows that the concept of culturally sensitive care is also favoured is other European countries—for example, in the Netherlands and France (Shen, 2015; Sturm et al., 2017; Uzun & Sevinç, 2015). For the purposes of this article, both strands of literature are included, and both terms appear to represent the same concept and are used interchangeably. A number of models for providing culturally competent care exist, along with a number of definitions of cultural competence. Shen (2015) differentiates between theoretical models in which cultural competence is studied from a process perspective (e.g., Campinha-Bacote, 1999; Cross et al., 1989; Sagar, 2011), and methodological models that focus on the methods that a health care professional can use to achieve cultural competence (e.g., Davidhizar et al., 1998; Leininger, 1993; Sagar, 2011). The different definitions of cultural competence by both the theoretical and methodological point are demonstrated in Figure 1. Even though different definitions and theoretical models coexist, specific attributes are repeatedly cited when describing cultural competence within the different models. Shen (2015) analysed 15 cultural competence models and assessment instruments and found that four attributes were present in 13 of the 15 cultural competence models or assessment instruments: namely, awareness, knowledge, skills, and sensitivity (Campinha-Bacote, 2002; Shen, 2015).

Theoretical and methodological models of cultural competence.
When investigating the perspective of the health care professional in practice, research among nurses confirms that knowledge, skills, and attitudes are key to develop cultural competence (Shepherd et al., 2019; Suurmond et al., 2010). It is important for health care professionals to understand and take into account how a patient experiences the world, and that carers must reflect on their own biases and prejudices toward different cultural groups (Cai et al., 2017; Turner, 2005). Cultural awareness and cultural sensitivity are mentioned less often in literature among health care professionals. This may confirm a more ethnocentric point of view of health care professionals toward cultural competence, alluded to in several studies (Almutairi et al., 2017; Hopkins et al., 2020; Markey et al., 2018; Sumpter & Carthon, 2011). In response to the aforementioned gaps, the purpose of this study is to deepen knowledge and understanding of culturally sensitive care by exploring: (1) the definition and perception of health care professionals of the concept of culturally sensitive care and (2) how culturally sensitive care is delivered by health care professionals in their daily practice.
Method
This qualitative study is part of the larger Diverse Elderly Care research project, which examines culturally sensitive dementia care for older migrants in Brussels, from the perspectives of elders, family carers, and health care professionals. This article focuses on the perspective of the health care professional. A qualitative research method was used because it is most suitable when exploring definitions, perspectives, and practices in health care, as is the case in this study (Bernard & Bernard, 2000; Polit & Beck, 2014). The COREQ checklist was used to report the method of our study (Tong et al., 2007). Ethics approval was granted by the ethics committee of the university hospital in Brussels (CE 2016-105).
Research Team and Reflexivity
The first and second authors conducted the focus groups (FGs) and interviews. Both are researchers and have experience in the field of health care, culturally sensitive care, and qualitative research. All authors have experience in qualitative research and content analysis, and all are lecturers in a health care programme. Both interviewers reflected comprehensively on their role and potential introduction of bias in this study and it was controlled as much as possible. Before each session, the researchers were introduced, jointly with the project purpose, the logic of the FG sessions, and the ethical and privacy terms.
Study Design
FG interviews were conducted with health care professionals (nurses, midwives) and students (nursing, midwife, and medicine students), selected by using consecutive sampling. The participants were invited face-to-face during a seminar or during class. For certain participants (general practitioners [GPs]), individual interviews were organised because it was difficult to accommodate the FG sessions for this group of professionals. GPs were selected by purposive sampling for the same reason. They were invited by email and telephone by the first or second author. They were recruited from a network of health care providers in Brussels. All respondents participated in FG interviews or individual interviews on a voluntary basis. Having experience in health care (as a job or from an internship) in a diverse city (e.g., Brussels) was an inclusion criterium for all participants. Data collection took place between November 2017 and September 2018. The 2-hour FG sessions were scheduled at a convenient time for the participants. Sessions were audiotaped after obtaining verbal informed consent at the beginning of each group session. The FG interviews took place in a meeting room at a university college in Brussels. The individual interviews took place at the GPs’ individual offices. All interviews were conducted in Dutch. A total of six FG interviews (n = 34) and four in-depth interviews were conducted. In total, 23 students participated in four FG interviews; and 11 health care professionals participated in two FGs. Table 1 provides an overview of basic demographic information of the study participants. Data saturation was obtained. All FG interviews and one individual interview were conducted by the first author. The second author assisted in conducting FG five and performed three individual interviews. Participants were reassured that, although the sessions were being audiotaped, anonymity and confidentiality was guaranteed. No names were traceable in the transcriptions, as numbers were used as substitutes. All interviews were audiotaped and transcribed verbatim by an official transcription office. An interview guide, based on the literature review, was used to structure the interviews. The literature review focused on cultural competence models and definitions. The interview started with the question: “What is good (quality of) care?” as an ice breaker to stimulate discussion among the participants. Thereafter, participants were asked about the following topics: (1) How do you define and perceive culturally sensitive care (in theory and in practice)? (2) How do you (try to) provide culturally sensitive care in practice? (3) What are facilitators for and barriers to culturally sensitive care? (4) What is the role of the patient and the health care organisation in culturally sensitive care? This article will only discuss the results of the main topics 1 and 2. In order to not influence the perception of the participants regarding the topic, no a priori definition or description of culturally sensitive care was provided. After each session, a debriefing report was made, including observational notes and comments about the process.
Overview of the Sample.
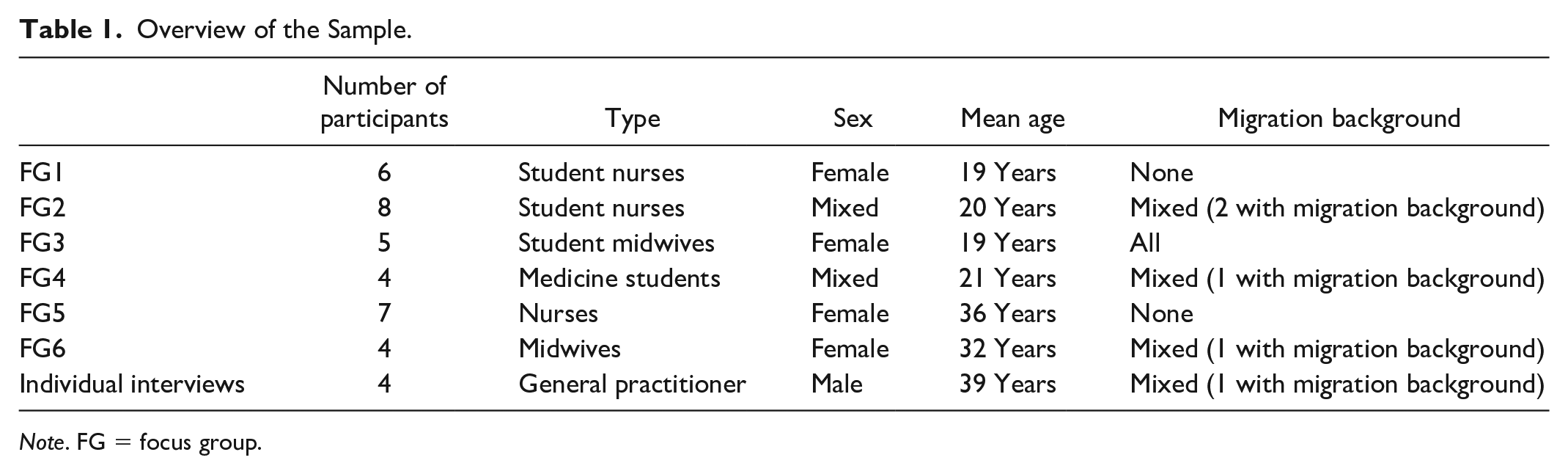
Note. FG = focus group.
Analysis
Thematic content analysis was used to analyse the data, and our analysis was coded and elaborated according to Burnard’s model (Bengtsson, 2016; Burnard, 1991; Burnard et al., 2008; Polit & Beck, 2014). The central aim of content analysis is to classify the data into more relevant and manageable parts or themes, which makes this methodological framework suitable for exploring definitions, perceptions, and practices (Graneheim & Lundman, 2004; Weber, 1990). The data was coded by the main author, using the qualitative data analysis software MAXQDA©. The coding tree was built following the main themes used by the interview guide. After initial coding, the data were explored in-depth. After a first analysis round, the authors discussed the coding of the data. A second analysis round led to five major emerging themes, which were again discussed by the research team. A third round of analysis led to the findings presented next.
Findings
The main emerging findings for the two first research topics are reviewed. Results are presented as a unit for the different types of participants (students, professionals) and the different disciplines (nurse, midwife, doctor) together, because the topic is explored from the perspective of the health care professional in general.
A Narrow Definition and Perception of Culturally Sensitive Care
Although the respondents agreed with each other that all patients should be treated equally and with respect, the respondents often had a narrow definition of culturally sensitive care. First, culturally sensitive care meant caring for “the other.” The other is different—and that is at the centre of the challenge of culturally sensitive care. In defining “the other,” the participants mentioned certain groups of immigrants very frequently, whereas other groups were not mentioned at all. When talking about culturally sensitive care, native Belgian respondents very often defined the other “culture” as “religion,” and, more specifically, as “Islamic religion.” In general, there was a strong focus on Muslim patients and on patients with roots in the Northern Africa and Middle East countries, as the following quote illustrates: In Muslim countries, the relationship with the doctor is different. . . . I cannot exactly say which countries, but there certainly are countries like that. (Nurse, FG5)
Conversely, respondents with roots in Southeast Europe or North Africa did not make this link with religion, and they saw “other cultures” as different ethnic groups, for example, patients from Eastern Europe or from Central Africa. None of the native Belgian respondents mentioned patients from Eastern or Southern Europe as an example of patients with a different culture.
Second, the respondents gave a list of practical actions as examples of how culturally sensitive care is implemented in their daily care provision. The practical actions were based often on the stereotypes that the respondents associated with immigrants from other cultures, and with Muslim immigrants in particular, like providing halal-food. A preference for the health care professional’s gender, specific food requests, and translation support were most often mentioned as examples. The respondents did not always facilitate examples from their own experience about these practical actions. Often these examples were based on stories from other health care professionals or from mentors to the student–respondents. The latter experiences were called difficult, unnecessary, or practically impossible. Almost all examples were about problems, negative experiences, or an extra effort that the respondents gave to meet the needs of the patient, as the following quote shows: INTERVIEWER: “You say: ‘I think that it is (more difficult) because of the cultural difference.’ Why do you say that?” RESPONDENT: “Because I hear from other colleagues that that is the case.” (Physician, INT2)
Third, as a solution to the fact they have experienced culturally sensitive care to be difficult, the respondents stressed that they needed more (cultural) knowledge in order to feel able to provide culturally sensitive care, but they did not discriminate between culture and religion. The examples they gave showed that they wanted more specific information about Islam. Some respondents mentioned that it is also important to have an open and inquiring attitude toward patients, that years of working experience can also increase knowledge about different cultures and that supervision could be supportive in acquiring cultural competences.
Providing Culturally Sensitive Care Is Difficult
The participants perceived culturally sensitive care to be difficult and a situation out of their comfort zone. First, the respondents were eager to gain knowledge in order to feel prepared in situations with patients that are perceived as “other” or different. They wanted to learn more about the characteristics of different ethnic–cultural groups and expected a third party (the universities, their employers) to provide this knowledge. They were unlikely to take actions themselves to broaden their knowledge and felt insecure about their own (cultural) knowledge.
If you have some idea about how to act, it seems to go a bit easier. If you have a broader knowledge—for example, of communication skills—then it is easier to act and to handle—for example, knowing that you don’t extend your hand to women from Saudi-Arabia. (Medical student, FG4)
Second, respondents were anxious about being regarded as racist, and so they hesitated to communicate and act in a spontaneous way. The reluctance to work in a spontaneous way led to feelings of exhaustion. The perception that culturally sensitive care is difficult can be caused by the idea that the respondents had about culturally sensitive care: namely, that patients expect you to do something different. So, this supposed expectation was caused by “the other.” And because the other is perceived to be different, participants expected such patients to have other needs. As a consequence of these other needs, they presumed they were expected to act differently and exert more effort, as this quote shows: For example, closing the door while having a conversation. I do that with every mother, but especially with mothers with a head scarf. (Midwife, FG6)
The respondents did not like this feeling of uncertainty and tried to find ways to handle these feelings—by using certain assumptions, acting shy and low-profile, or, at times, by overacting.
They come from God-knows-where, and with the Berber and all . . . I always have an extremely good connection with those people. I give them a hug, and those mothers aren’t embarrassed, they do their thing . . . that’s no problem. (Nurse, FG5)
Respondents think that broader knowledge and being more experienced as a health care professional was reassuring and provided the feeling of being more confident, mastering better communication, and providing better caring skills.
Third, participants mentioned a lack of time as an additional factor toward perceiving culturally sensitive care as being challenging. The respondents indicated that time is an important condition for providing good quality of care for every patient. In the current cost-savings climate, professionals have less time to do what is considered to be more work. As previously mentioned, the respondents expected other needs, and acted differently or exerted more effort toward patients with a different cultural background. Too little time, too much work, and the idea that certain types of patients require even more time, lead to conflicting demands which are difficult for the health care professional to handle in daily practice.
During my last internship, I was on my way to the waiting room to get a patient. A nurse took my arm and said: “you don’t have to invest too much time in her, that black woman” and then she let go of my arm. I thought “what just happened?” but I went to the patient and did what I was supposed to do. Afterwards, I was typing my report, and she (the nurse) came back to me and said, “that was a typical black one, wasn’t she?” . . . “I was really shocked by that.” (Medical student, FG4)
This last quote also shows a particular challenge, mentioned by the respondents with regard to working with different ethnic–cultural groups: a perceived lack of competence to oppose racism toward patients. Several respondents reported that they felt unprepared and insecure about responding to racist comments by colleagues or (in the case of students) mentors.
Care Is Delivered to “the Other,” Starting From Their Own Frame of Reference
Participants centralise themselves as the norm, and they start from this frame of reference to compare how alike or different patients are. The frame of reference is a construction of values, norms, knowledge, and experience. It is dynamic and individually set, but there are also important structural influencers from the society, such as educational and governmental systems. First, most of the respondents made it very clear that there was a difference between “us” and “them,” and they keep seeing some people as “the other.” This was expressed during the entire discourse with the health care professionals. The next citation shows that there is also an imbalance of power between “us” and “them,” which needs to be considered: Look, that doesn’t mean that there are people that receive less quality of care. . . . Not at all. But they don’t have to start acting difficult. They have to adapt (to our system), that is the rule. (Nurse, FG5)
Additionally, the use of words such as “regular people” and “normal people” to indicates people “like us” shows that a distinction is being made between different types of people.
In winter, when it snows, I automatically remove my shoes . . . then I don’t ask, I also do that in normal people’s houses. (Nurse, FG5)
Second, communication skills and asking genuinely open questions are often presented by the respondents as good practices in order to get to know the patient and their habits. But even when the respondents asked their patients open and sincere questions, the othering continued, as this example shows: So, I ask them: “How do they do that with you (meaning: with your kind of people)?” (Nurse, FG5)
This example demonstrates that the respondent saw the daughter and the patient as a part of a larger group, namely Muslims. And in that perception all Muslims have similar habits and traditions. It is important to note that the respondents were not aware of this othering during their discourse.
Third, this “othering” mentality became noticeable in how behaviour or relationships were described by the participants. The participants shared situations and examples simply from their own point of view and from their own frame of reference.
The respondents usually showed little awareness of, or sensitivity toward, the diversity of frames of reference among people. There were several similar examples given, where the pattern was common: we (health care professionals) respect you (the patient) and we will listen to you, but eventually it will be “our” way and within “our” boundaries. There is a fear in the respondents’ statements about adapting too much to the needs of the patients. Clear communication was perceived as saying what they find possible or not, and in which circumstances. For the respondents with a migration background, it was easier to empathize toward the patient’s frame of reference. They found it easier to consider that there are different ways of thinking. White Belgian respondents who showed some awareness toward people with another frame of reference confirmed that their point of view on the world played a role in how they provided care. That point of view was influenced by how they were raised and educated, by travelling, or by years of experience as a health care professional in a diverse setting. During the interviews and FGs, the respondents showed their good intentions and presented themselves as truly committed to their patients. They were neither aware of this “othering” nor that it could be a potential barrier toward the patient.
Discussion
Health care professionals and students were interviewed to understand their perspectives on culturally sensitive care. First of all, the findings suggest that the definition, perception, and practices of culturally sensitive care by health care professionals and future professionals are often narrow, focused on daily care practice and with a specific focus on the Islamic religion and/or Arabic culture. In previous research conducted by Torres, it is underlined how the “elder immigrants” group is created as a social construct and is categorised as a “homogeneous problematic group with special needs.” A similar pattern applies to the perception of Muslim patients (Torres, 2006). This can be a result of the current framing in society in Western countries, where Islam is often presented in media, social media, and policy in a negative and stereotypical way. Fadil (2019) confirms this narrow point of view, on the societal level, where “culture” equals “migrants,” and that “migrants” equal “Muslims” (Fadil, 2019). Conversely, the findings show that the perception of Muslim health care professionals with a migration background is different. Here a different type of perception of culturally sensitive care is noted, which is based more on ethnicity and less on religion. Moreover, health care providers with a migration background have a wider range of populations and nationalities in mind when defining culturally sensitive care.
Second, the analysis shows that health care providers perceive culturally sensitive care as difficult—they feel mostly insecure, and they search for solutions in the domain of (cultural) knowledge to comfort themselves and to limit those insecurities. This is also confirmed in other research, which notes that cultural knowledge does not improve the quality of care for the patient (Berdai Chaouni et al., 2020). Another important remark is that “one type of immigrant” does not exist. Migrants are very diverse in the areas of origin, age, current socioeconomic status, culture, motive for migration, socioeconomic status before migration, educational level and literacy, among others. For all these attributes, Torres (2006) states that “immigrantness” holds certain characteristics such as foreign, culturally different, less developed, more traditional and less modern. This “immigrantness” or otherness creates feelings of uncertainty (Markey et al., 2018; Roberts et al., 2008; Torres et al., 2016). The key is to question why health care professionals are often afraid of a spontaneous or impulsive reaction they may have when working with patients of a different background. Roberts et al. (2008) calls this “White fears”; and in this research, medical students fear unintentionally offending someone during a discussion about race. DiAngelo (2011) explains this “White fragility” in White people in North America as a state in which even a minimum amount of racial stress becomes intolerable, triggering a range of defensive moves. These moves include the outward display of emotions such as anger, fear, and guilt, and behaviours such as argumentation, silence, and leaving the stress-inducing situation. (p. 54).
Third, “othering” seems very present, in the definition and implementation of culturally sensitive care, as results show that the health care professionals keep looking at the other. This othering could be considered to be unintended micro-racism by the health care professional. As Torres (2006) notes, the health care professional is not conscious that this is racism and that it raises a barrier toward the patient and his family. If health care professionals can overcome othering, it can help them better understand their own biases and assumptions that might hamper intercultural interaction and reciprocal trust (Alpers, 2018; Guttormsen, 2018). This point is also confirmed in other research, where it is stated that a patient’s needs can go unmet as a result of misunderstandings caused by otherness (Berdai Chaouni et al., 2020; Berdai Chaouni & De Donder, 2019; Torres et al., 2016). The fact that the balance of power plays a role should also be considered. This can be the relationship between White Western health care professionals and non-Western immigrant patients, where certain assumptions are present (e.g., the expectation that patients and families with a migration background lack knowledge; Milberg et al., 2016). This also plays a role in the frame of reference of all parties involved, and as a consequence in the communication between the health care provider and the patient, in which there is apparently room for debate, but ultimately the rules of the health care professional or organisation determine the flow. This was also confirmed by a research on ethnic minority medical students conducted by Roberts et al. (2008), where the “us and them” feelings made the students uncomfortable toward White patients and White fellow students. Being more aware of one’s own frame of reference and that of the patient leads to other actions and other skills.
The findings raise issues for practice and education. The offer of courses on culturally sensitive care using the learning method of knowledge transfer will not sufficient to actively work on the frame of reference of students and professionals. Interactive learning methods like supervision and coaching, reflective exercises, peer learning or simulations could be helpful to achieve this goal (Kılıç & Sevinç, 2018; Leung et al., 2020; Oikarainen et al., 2019). This could be explored in future research.
Limitations
A number of limitations can be identified in this study. First of all, a combination of FGs and individual interviews was used in the study. It would have been preferable to have all participants participate in a FG session. Because of organisational reasons the GP’s participated in individual interviews, in which the group dynamics of a FG were missing. This might have modulated responses (Polit & Beck, 2014). However, the interviews gave rich accounts and, it should be noted, the discourses were rather coherent with the FGs data. It is acknowledged that transferability is a challenge, but that is not the ultimate goal of this qualitative study (Bernard & Bernard, 2000). Few disagreements emerged during this FGs, and in general the participants had rather similar opinions and experiences. Second, all participants voluntarily participated in a FG on the theme of culturally sensitive care, which may involve a selection bias for participants already having an interest on the topic. Even acknowledging this selection bias, it is interesting to see the rather narrow focus of the concept and the emergence of othering and racial expressions throughout the FGs and interviews. Sorensen et al. (2017) suggests that—to achieve culturally competent care—it is essential to engage all stakeholders and ensure diversity among the stakeholders in order to set up a process with both a bottom–up and a top–down approach. Further study could provide further insight in this process and could focus on including health care professionals and students who do not have a particular interest in the topic of culturally sensitive care.
Finally, our sample included a combination of students and professionals. This could mean that not all voices in health care are heard. However, we intend to use this research to plan a more thorough study that can include a more diverse sample.
Conclusions
Achieving cultural competence for health care professionals is of utmost importance in order to guarantee the quality of care provided to patients worldwide. This study underlines the fact that health care professionals as well as students share a rather narrow definition and perception of the concept of culturally sensitive care.
A key point in our research is that health care professionals primarily use their own frame of reference to plan their work and care, finding it a challenge to empathise with other frames of reference, which is sometimes the case with patients. “Othering” is a key specific example of our findings, which opens the door to difficult communication and potential conflict during the caring process. Cultural awareness and sensitivity are needed to reflect on implicit biases and their impact on the provision of care in practice. This is essential to overcoming narrow definitions and obstinate stereotypes that may be associated with specific groups and prevent professionals toward a real implementation of proper culturally sensitive care. A number of solutions need to be envisaged. We propose interactive learning methods to facilitate developing specific awareness for health care providers in the topic explored. Aspects such as othering and its potential consequences, particularly for their patients with an ethnic-minority background should be considered. Following the above, we recommend further research in that field. Measuring the impact of an educational initiative would be interesting. In spite of health care providers’ best intentions, unintended stereotyping and othering appear present in our setting, which creates barriers in the provision of care. This should be carefully considered to deliver adjusted and appropriate culturally sensitive care.
Footnotes
Acknowledgements
We would like to express our gratitude to the respondents for their willingness to share their time and opinions with us.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the European Fund for Regional Development Brussels (Grant Number F11-06].